Contents lists available atScienceDirect
Collegian
j o u r n a l h o m e p a g e :w w w . e l s e v i e r . c o m / l o c a t e / c o l l
Medication
administration
evaluation
tool
design:
An
expert
panel
review
Karen
M.
Davies
a,b,c,∗,1,
Ian
D.
Coombes
c,d,2,
Samantha
Keogh
e,f,g,3,4,
Karen
M.
Whitfield
c,d,5,6aDepartmentofClinicalPharmacology,RoyalBrisbaneandWomen’sHospital,Brisbane,Queensland,Australia bFacultyofMedicine,UniversityofQueensland,Brisbane,Queensland,Australia
cSchoolofPharmacy,UniversityofQueensland,Brisbane,Queensland,Australia
dPharmacyDepartment,RoyalBrisbaneandWomen’sHospital,Brisbane,Queensland,Australia
eSchoolofNursing,InstituteofHealthandBiomedicalInnovation,QueenslandUniversityofTechnology,Brisbane,Queensland,Australia fCentreforClinicalNursing,RoyalBrisbaneandWomen’sHospital,Brisbane,Queensland,Australia
gAllianceforVascularAccessTeachingandResearchGroup,GriffithUniversity,Brisbane,Queensland,Australia
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26September2017 Receivedinrevisedform17April2018 Accepted9May2018 Availableonlinexxx Keywords: Nurses Medicationadministration Self-assessment Feedback Evaluationtool
a
b
s
t
r
a
c
t
Background:Toolscurrentlyavailabletoevaluatenursemedicationadministrationpracticeshave limi-tationsandareeithernotvalidatedorhavepoorreliability.
Aim:Toidentifycriteriaandcontentforinclusioninatooltoevaluatemedicationadministrationby nursesintheclinicalsetting,usinganexpertpanel.
Methods:Apeerreviewprocessusinganexpertmultidisciplinarypanelratedtherelevanceofthecontent onthreetools;MedicationAdministrationSafetyAssessmentTool,MedicationwithRespectTooland ClinicalSkillsAssessmentTool,usingafour-pointratingscale.Expertopinionwasprovidedonrelevance ofcontent,ratingscalesandfrequencyofnurseevaluation.Thelevelofagreementwasanalysedby itemcontentvalidityindex,meanitemcontentvalidityindex,meanexpertproportion,scalecontent validityindexwithuniversalagreement,probabilityofchanceagreementandamodifiedkapparating. Qualitativethemeswerealsoreviewed.
Findings:TheitemandscalecontentvalidityindexandthekappaindexbothratedtheMedication Admin-istrationSafetyAssessmentToolandClinicalSkillsAssessmentToolasexcellent.FortheMedicationwith RespectToollessthanhalfoftheitemcontentvalidityindexratingsratedasgoodandthekappaindex ratedasexcellent,thereforethescalecontentvaliditydidnotachieveagoodrating.
Conclusions:Theexpertpanelreviewidentifieditemsofhighlevelofagreementforrelevanceand deter-minedthatcontentneededtobeclear,concise,observable,genericandpracticaltobeusefulforallnurses. Self-evaluation,feedbackandadevelopmentalplanwerealsokeycriteria.
CrownCopyright©2018PublishedbyElsevierLtdonbehalfofAustralianCollegeofNursingLtd.
∗Correspondingauthorat:DepartmentofClinicalPharmacology,RoyalBrisbane
andWomen’sHospital,Brisbane,Queensland,Australia.
E-mailaddresses:[email protected](K.M.Davies),
[email protected](I.D.Coombes),[email protected](S.Keogh), karen.whitfi[email protected](K.M.Whitfield).
1 Clinical Pharmacology, Level1, Ned Hanlon Building, Royal Brisbaneand
Women’sHospital,ButterfieldSt.,Herston,Brisbane,Queensland4029,Australia.
2 Pharmacy Department,Level 1,Ned Hanlon Building,Royal Brisbaneand
Women’sHospitalButterfieldSt.,Herston,Brisbane,Queensland4029,Australia.
3 QUT,Rm338,NBlock,KelvinGroveQld4059,Australia.
4 CentreforClinicalNursing,RoyalBrisbaneandWomen’sHospital,Level2,
Build-ing34,Herston,Brisbane,Queensland4029,Australia.
5 SchoolofPharmacy,PACEPrecinct,Building870,TheUniversityofQueensland
QLD4072,Australia.
Summaryofrelevance Problem:
Therearefewvalidatedandreliablenursemedication admin-istrationevaluationtoolscurrentlyavailableforuseintheclinical setting.
Whatisalreadyknown:
Avoidablemedicationadministrationerrorsarewidelyreported in nursing literature. Compliance to safe medication practice reducesthepotentialforerrorandunintentionalpatientharm.
6PharmacyDepartment,RoyalBrisbaneandWomen’sHospital,Level1,Ned
Han-lonBuilding,RoyalBrisbaneandWomen’sHospital,ButterfieldSt,Herston,Brisbane, Queensland4029,Australia.
https://doi.org/10.1016/j.colegn.2018.05.001
WhatthisPaperAdds:
Developmentofarelevantandpracticalmedication adminis-trationevaluationtoolthatincorporatesself-evaluation,feedback andadevelopmentalplanaskeycriterion.
1. Introduction
Medicationadministrationisakeycomponentofthe medica-tionmanagementprocessandcomprisesasignificantcomponent ofnursingpatientcare (Jennings etal., 2011; Westbrooket al., 2011). Basic coreclinicalskills are required tounderstand and ensure the safe, effective and efficient administration of med-ications to patients and avoid unintentional harm (Australian CommissiononSafetyandQualityinHealthCare,2012b;Coyne etal.,2013;Härkänenetal.,2016;Sinclairetal.,2014;Stolic,2014). TheWorld HealthOrganisation (WHO) aimstohalve avoidable medication-relatederroroverfiveyearsbyaddressingweaknesses inhealthsystemsandimprovingthewaymedicationsare man-aged(WorldHealth Organisation,2017).Examplesof theWHO strategiestoachievethisare:1)theuseoftoolstohelphealthcare professionals,especiallywhenusingmedicationswithahighrisk ofharmifusedimproperlyandenhancingpatientsunderstanding ofthesemedications,2)tostrengthenleadershipdevelopmentand skill-buildingand,3)topromotepatientsafetyresearchinthisarea. Therearemanystudiesdemonstratingthepotentialfor medi-cationadministrationerrorthatcanleadtopatientharm(Popescu et al., 2011), (Gunningberg et al., 2014). Observational studies undertakeninternationally,andlocallywithinAustraliaandNew Zealandhaveidentified factorsthatareknowntocontributeto increasedpotentialfor errorand harmtopatients. Distractions caused by external environmental factors such as monitoring alarms, interruptions by nurses, doctors, other staff members, patientsandfamilymembershavebeenshowntoincreaseerrors (Daviesetal.,2015;Härkänenetal.,2015;Westbrooketal.,2010). Simulated scenario-based training of 591 nurses has shown a thirdofnursesidentifiedallknownerrors(Coombesetal.,2005). Examplesoftheseerrorswere1)incorrectintravenouspotassium concentration2)re-exposuretoasevereadversedrugreaction3) incorrectformulationofamedication4)nodosedocumentedon theprescription5)incorrectfrequencydocumented6)incorrect medicationssuppliedondischarge.Lackofknowledgeand devia-tionfromnationalstandards,statelegislationandlocalprocedures andpoliciesthatunderpinsafemedicationpracticehavealsobeen showntocontributetoincongruencefromacceptedsafepractice (Westbrooketal.,2011).Thisleadstoperpetuationofpoor med-icationpracticethroughlearnedanddemonstratedbehavioursto newstaff(Popescuetal.,2011).
Whengapsinpracticeareidentified,feedbackisrequiredto enable the nurse to implement strategies to improve practice (Spector,2014).Forfeedbacktobeeffectivemultiplefactorsneed tobeconsidered; whetherthenurse is willingand engagedto receivefeedback,theenvironmentinwhichfeedbacktakesplace, thetimingoffeedbackand ifthetaskissomethingthenurseis requiredtodoorwantstodo,aswellastherelationshipbetween thenurseandthereviewer.Feedbackneedstobeformative,not summative,withinformationabouttheirperformance communi-catedtothelearnerthatisintendedtomodifytheirthinkingor behaviourforthepurposeofimprovinglearningandpatient out-comes.Summativefeedbackisusuallycumulativefeedbackover timefrommultipleassessmentsandisoftengradedwithamark. Thistypeoffeedbackisoftenlessdescriptiveinprovidingexamples ofindividualperformanceopportunitiesforimprovement(Butler &Winne,1995;Molloy&Boud,2013;Wikander&Bouchoucha, 2018).Localobservationalauditstudieshavedemonstratedthat combiningintermittentnurseobservationofmedication
adminis-trationaswellasprovidingdirectindividualfeedbackcanimprove practice.Examplesinclude:increasedcheckingofpatient identi-ficationandadverse drugreactions,decreased medicationerror selection,decreasedwrongrateadministrations,decreased omis-sionsofmedications,decreasedforgettingtosignmedicationcharts afteradministration,decreasedinterruptions(Daviesetal.,2015). Other professions including Pharmacy have demonstrated improvement in pharmacist’s performance facilitated by an adaptedcompetency-basedgenerallevelframework(GLF).TheGLF isatoolusedtoevaluatepharmacist’sperformanceand incorpo-ratestailoredfeedbackandindividualisedtrainingplantoguide professional development (Coombes et al., 2010; Stacey et al., 2014).However,thereisalackofvalidatedandreliabletoolsto conductself-evaluation,observationandprovideformative
feed-backofnursingmedicationadministrationpracticeintheclinical
setting,suchas:thehospitalinpatientsetting,residentialagedcare facility,communityorgeneralpractice.
2. Literaturereview
Theliteraturereviewofmedicationadministrationassessment toolssynthesisesthe variousmethods and toolsused toassess nursesmedicationadministrationpracticeandhasidentifiedalack ofvalidatedandreliablecompetencymeasuresintheclinical set-ting(Liˇcen&Plazar,2015).Tools identifiedwere either: a)not specifictomedicationadministration,b)developedforstudents, newgraduatesornursingspecialtiesonly,c)medicationcalculation focused,d)lackedself-assessment,e)hadnodevelopmentalplan,f) werenotvalidatedorg)hadpoorreliability(Bulletal.,2017;Coates &Chambers,1992;Fisher&Parolin,2000;Longetal.,2013;Sinclair etal.,2014).Threetoolswereidentifiedthatcontainedmanyof thesecriteriaandwereusedtoassessnursemedication adminis-tration.Therefore,thesethreetoolswerechosentobeincludedin thisstudy.
ThetoolfromtheUnitedKingdomwasamedication adminis-trationcompetencytool,MedicationwithRespectTool(MwRT), adaptedfromanestablishedassessmentframeworkusedto eval-uateorallyadministeredmedicationsin thementalhealth area. (Hemingway etal.,2011;Turneret al.,2007,2008).Theformat usedevidence-basedstructuredcriteriaaimingtominimisethe riskofmedicationerrors bydefining andsettingproceduresfor safe administration. Two assessments were used (1) Observed StructuredClinicalExamination(OSCE)and(2),anassessmentof Administrationof Medicine CompetencyFrameworks(Oral and Intramuscular). Only the Oral tool was reviewed in this study. Thecontentwascomprehensiveincludingadditional environmen-talcomponentssuchascleaning,restockingandsecurelockingof medicationstorage,aswellastheadministrationofthemedication. However,theresearchwasundertakenwithmentalhealthnurses onlyandfurtherworkwouldberequiredtovalidateinother clin-icalareassuchasthegeneralhospitalinpatientsetting,specialty fieldssuchasintensivecareandpaediatric,aswellascommunity andagedcarefacilities.
Themedicationadministrationsafetyassessmenttool(MASAT) from the United States of America (US) is a binomial scale usedtoevaluateaccuratemedicationadministrationperformance (Goodstone&Goodstone,2013).Theresearchersconducteda lit-eraturesearchofthe“6rights”ofmedicationadministrationto develop thecontent and identifyspecific behavioursrelated to performingthem.Reliabilityofthetoolwasconductedusing sim-ulationscenarios and a simple five-point anchoredlikertscale. Thecontentwasachecklistformatof8rightsforsafemedication administration.Threewereforcheckingthecorrectpatientandone eachforcheckingtherightdrug,dose,route,timeand documen-tation.TheauthorsconcludedtheMASATchecklistformedication
administrationassessmentwasreliable(Cronbach’salpha0.90)ina simulatedandclinicalhospitalwardsettingwithanundergraduate nursingstudentcohort.Itwasnothowever,usedwithRegistered Nurses.
TheAustralianClinicalSkillsAssessmentTool(CSAT)was devel-opedbynurseeducatorsforthepurposeofsupportingnewstaff, postinductionaspartofamedicationresourcepackage(O’Brien, 2015).Themaincomponentsidentifykeymedicationprocedures toinformstandards ofpractice,assesses foundationknowledge bycasescenarioexamples,thenobservesthenurseinpracticeto ensurethatthestepsforsafeadministrationareadheredto.The contentincludedcheckingthecorrectrightsofthemedicationas wellasthevalidityoftheprescription,knowledgeofthe medica-tionandassessmentofthepatientpreand postadministration. Formativefeedbackisprovided,andanyknowledgepracticegaps arediscussedforfurtherimprovement.TheCSAThasnothowever beenvalidatedtodeterminereliability,reproducibility,usefulness andefficacy.Thepackagehas5hoursofContinuingProfessional Development(CPD)allocatedtocompletethemoduleknowledge componentandthreeassessments.Importantly,thetimerequired tocompletethepackagelimitsitsbroaderuse,precludingallnurses fromtheopportunitytobenefit.
Thereisaneedforapractical,userfriendlymedication admin-istrationevaluationtoolforallnursesthatallowsself-evaluation, observationinclinicalpractice,provisionofformativefeedbackand developmentofamutuallyagreedplanforimprovingperformance. 3. Methods
3.1. Aim
Toidentifycriteriaandcontentforinclusioninatooltoevaluate safe,effectiveandefficientmedicationadministrationbynurses intheclinicalsettingtoensureallproceduresarebeingfollowed, usinganexpertpanel.
3.2. Studydesign
Apeerreviewprocesswasemployedusinganexpert multidisci-plinarypaneltoreviewthecontentofthreetoolsidentifiedinthe literatureusedtoevaluatemedicationadministrationbynurses. Theexpertreviewwasconductedasdescribedby(Polit&Beck, 2008)byinvitedmedicationexpertsaskedtoratethecontentof itemsandoverallscalesforrelevanceinthedevelopmentofa med-icationadministrationevaluationtool.Thisstudyreceivedawaiver ofHumanResearchEthicsCommittee(HREC)reviewfromthe Hos-pitalandHealthServiceHREC(HREC/16/QRBW/351).Thefunder forthestudydidnotcontributetothestudyprotocol,design,data collection,analysisofresultsorthemanuscript.
3.3. Studysettings
The expert panel review was held at a tertiary metropoli-tanhospitalinJuly2016overtwohours.Expertpanelmembers eitherattendedfacetoface,viavideoconferenceorteleconference. Expertsunabletoattendwereofferedtheopportunityforoneon oneinterviewwiththesameagendaquestionsastheexpertpanel meeting.
3.4. Datacollection
Invitationsfor thepanelweresent viaemailto22potential expertsthatmetthecriteria asexpertsinmedication adminis-trationorhadevaluatedmedicationassessmenttoolspreviously. Sixteenofthetwenty-twoinvitedexpertswhowerefromarange ofmultidisciplinary(nursing,pharmacyandmedical)backgrounds
and roles including clinical, academic, research, education and safetyandqualityprofessionsparticipated.Consentwasprovided byacceptanceoftheinvitation.
Theexpertpanelmemberswereprovidedfourquestionnaires viaemailpriortothemeeting.Abriefdemographicquestionnaire included data abouttheir profession,role, years of experience, whethertheymanagedmedicationsorwhetherornottheyhad validated anassessment tool previously. Therewere alsothree structuredquestionnairesofthechosentoolstocompletepriorto thediscussionpanel:
•MwRT(Hemingwayetal.,2011), •MASAT(Goodstone&Goodstone,2013) •CSAT(O’Brien,2015)
Thequestionnairesaskedthepaneltoratetheindividual con-tentforrelevancytosafemedicationadministrationpracticeusing thefollowingscale:
1notrelevant, 2somewhatrelevant, 3quiterelevantto 4highlyrelevant.
Thequestionnairesalsoaskedthepaneltoratetheindividual contentonafour-pointratingscalefrom:
•deleteitem, •reviseitem(major), •reviseitem(minor) •keepitemasis.
(Polit&Beck,2008)
Thefacilitatorwasasenioracademicpharmacistwithover10 years’experienceinfacilitatinglargegroupsofhealth profession-als.Thepanelmeetingwasrunbythefacilitatorusinganagenda toguidethediscussion.Minutesweretakenaswellasanaudio recording tocapturecontentof thediscussion. Thepanel were dividedintothreegroupsoffourparticipantstoallowconstructive discussionaroundtheeightagendaquestions.Thepaneldiscussion focusedonthefollowingareas:
•typeofcontenttobeincludedsuchas:checkingtheright medi-cationandproceduralstepsinmedicationadministration. •theformatofthetool,whetherbinomialorlikertscalesshouldbe
usedforevaluation;whetherallroutesandtypesofmedication suchas:oral,intravenous(IV),intramuscular(IM)andcontrolled schedule8drugs(CD)shouldbeincludedinonetoolorshould therebemultipletools.
•numberofpatientstoadequatelyassesseachnurse. •numberofmedicationstoadequatelyassesseachnurse •numberofroutesofmedicationstoadequatelyassesseachnurse •lengthoftimetoadequatelyassesseachnurseandallowthetool
tobepracticalanduseful •frequencyofobservations
Based onthe resultsof therecommended contentfrom the expertpanelamedicationadministrationtoolwasdesigned.The designedtoolwasthensenttotheexpertpanelforfacevalidity evaluation.
3.5. Dataanalysis
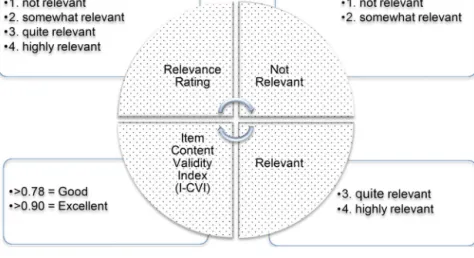
DatawerecollatedusingMicrosoftExcelandtheitemcontent validityindex(I-CVI)wascalculatedbytheproportionofitems ratedrelevantbyeachexpert.ThedescriptionforcalculatingI-CVI
Fig.1. DataAnalysis. (Polit&Beck,2006)
Table1
DataAnalysisMeasuresofAgreementandAcceptableRatings.
Measure Calculation ValidityRating
I-CVI=Itemcontentvalidityindex Numberofitemsratedrelevant(3or4)/numberofexpert
responders
Good=>0.78; Excellent=>0.90
S-CVI/Ave=Scalecontentvalidityindexaverage AverageofallI-CVI Excellent=>0.90
MeanExpertProportion Averageofexpertproportionratedrelevantbyallexperts Excellent=>0.90
S-CVI/AU=Scalecontentvalidityindexuniversal agreement
Numberofitemsratedrelevant(3or4)byALLexperts /numberofitems
Good=>0.70 Pc=Probabilityofchanceagreementonrelevance N=numberofexpertsandA=numberagreeingon
relevance[N!/A!(N-A)]x0.5N
Good=<0.070
k*=Kappachancecorrectedforagreementonrelevance (I-CVI-Pc)/(1-Pc) Poor=k*<0.40;
Fair=k*0.40-0.59; Good=k*0.60-0.74; Excellent=k*>0.74
isinFig.1.Thevalidityofeachscaleoverall,themeanitem con-tentvalidityindex(S-CVI/Ave),themeanoftheexpertproportion relevantbyallexpertsandthescalecontentvalidityindexwith universalagreement(S-CVI/UA)byallexpertswereallcalculated. Inordertoaccountforthepossibilityofagreementor disagree-mentonrelevancebeingbychancetheProbabilityofChance(Pc) wascalculated.Thenamodifiedkappa,forusewithmultipleraters, astatisticalindexadjustingforchanceagreementwascalculated. Dataanalysismeasuresofagreementandacceptableratingsare detailedinTable1.
Fig.1.Itemcontentvalidityindex(I-CVI)forratingrelevance (Polit&Beck,2006)
Thecontentsratedasrelevant(3.quiterelevantand4.highly relevant)andrecommendedtokeepitemasis,wereconsideredfor useinthedesignedtool.Contentsratedasrelevant,andreviseitem wereconsideredformodifying.Contentsratedasnotrelevantwere notconsideredforuseinthetooldesign.Duringtheexpertpanel meetingallresponsestotheagendaquestionsweredocumented andthemajorityresponsewasusedinthedesignofthetool.
Qualitativethematicanalysisofcommentswasconductedby collatingintocommonwordstodeterminethemes.Thesethemes wereusedasreasonstoaltercontentorincludeintheproposed tooldesign.
4. Findings
4.1. Quantitative
Fourteenofthe16expertpanelcompletedthedemographic questionnaire.Theyconsistedof5nurses,6pharmacists,2medical officersand1publichealthresearcher.Allhadbetween10and40 years’experienceintheirprofessionalpracticewiththemajority
having20–30years’experience.Overhalfofparticipantscurrently managemedicineseitherprescribing,dispensingoradministering. Justunderhalf(6/14)havingpreviousexperiencewithvalidating acompetencytool,ofwhich67%weremedicationrelated.
Thedataanalysisresultsforrelevanceandcontentvalidityfor eachof thethree medicationadministrationtoolsare shownin Table2.Allcontentitemsratedasexcellentinthethreetoolswere considerforuseintheproposedtooldesign.
4.2. MwRT
TheMwRThad45questionswithlessthanhalf(22)scoringan I-CVIgreaterthan0.78ratingthecontentrelevanceasgood.The S-CVI/Avedidnotmeettherecommended0.9ratingandthe S-CVI/UAratingofagreementbyallexpertswasonly0.27.Therefore, thekappaindexcorrectedforchanceagreementratedonly22/45 itemsforthescaleasexcellent.
4.3. MASAT
TheMASAThadonlyeightquestionsandtheI-CVIratingforall eightquestionswas100%agreeingonrelevance.Therefore,the S-CVI/Ave,meanexpertproportion,S-CVI/UAandkappadesignating agreementonrelevanceallratedthescaleasexcellent.
4.4. CSAT
TheI-CVIforall25questionsintheCSATratedover0.78rating theitemsrelevanceasgood.Thescalecontentvalidityratedas excellentforallcalculationsofS-CVI/Ave,meanexpertproportion, S-CVI/UAandkappa.
Table2
CombinedSummaryofToolExpertPanelEvaluationofContentValidity.
Tool Number ofItems Numberof Experts Numberof I-CVI>0.78 Meanexpert proportion>0.90 MeanI-CVI (S-CVI/Ave)>0.90 S-CVI/UA >0.70 Pc<0.069 Numberof k*>0.74 KappaEvaluation Rating MwRT 45 10 22 (0.30-1.00) 0.68 (0.21-0.98) 0.73 0.27 0.001-0.273 22 (0.20-1.00) 22/45Excellent MASAT 8 10 8 (1.00) 1.00 (1.00) 1.00 1.00 0.001-0.002 8 (1.00) 8/8Excellent CSAT 25 12 25 (0.89-1.00) 1.00 (1.00) 0.97 0.72 0.00-0.018 25 (0.90-1.00) 25/25Excellent Table3
QualitativeThemesfromToolsReviewed.
Tool Theme Description
MwRT “wordingneedstoberevised”
“clarification”“notpracticalbecauseitwastoo long”“notrelevanttogeneralnursing medicationsafety”inAustralia
Clarificationrequiredaroundquestionsmeaning.Itwaslongwith45questions. ItwasspecificallyformentalhealthnursesandnotgeneralnursinginAustralia.
MASAT “student”“allergies”“acronyms”“outcome” Specifictostudentnurses,notgenericforallnurses. Therewasnocheckofpatientallergies.
Acronymsusedwerenotclearorgeneric.
Havingcheckeditwasnotcleariftheoutcomewas“correct”.
CSAT “checking”“correct”“add”“how”“duplication” Patientidentificationandallergieswerenotseparatequestionstobeabletodetermineifthey werecorrect.
Moredetailneededtobeclearonspecificcomponents. Howisitdonetobeobservable,measurableandconcise. Duplicationofquestionsandcomponentsintool.
4.5. Qualitative
Therewasgeneralagreementbytheexpertpanelthatthere shouldbe“rights” ofmedicationadministration included;right patient,medication,dose,route,time.Commentswerethat word-ingneededtobeclearanddefinedasobservabletasksbysuccinctly describingthesteps.Itwasalsoagreedthatthereareprocedural stepsassociatedwithmedicationadministrationthatneedtobe included.Suchas:
•Appropriatehandhygiene
•Aseptictechniquewhenpreparingmedication
•Conductingassessmentandobservationsofthepatientto deter-mineifitisappropriateandsafetoadministerthemedication. •Engage the patient in the administration to determine their
knowledgeandunderstandingofthemedications.
•Appropriatelydocumentadministrationofthemedicationafterit hasbeenadministered,orifnot,whynot,andwhowasinformed andendorsedthedecision.
Thepanelconcurredthatideallythereshouldbeoneratingscale forbothcomponentsofthetoolandthatabinomialyes/noscale, waspreferableandpractical.Itwasagreedthatonetoolshould coverallroutesandtypesofmedicationadministeredandtherefore somequestionswouldnotbeapplicableinallscenarios.An exam-pleofthiswouldbeoralmedicationwhichrequiresonenurseto administerandwouldnotrequirelabellingofanintravenousline. Thequestionofhowmanyobservationsormedicationswouldbe adequatetoevaluateeach nurses’practiceremainedunclear,as itwouldbedependentontheoutcomeoftheobservation. Rigor-ousdiscussionwasaroundhowthiswouldbedeterminedwithall agreeingthatitwouldbedependentonmanyvariablesi.e.Howsafe thenurse’spracticewas;andwhethertheobserver’sexpertopinion wasthattheyrequiredmoreinformationtodetermineconsistency ofpractice.Mostsaidtheywouldrequireatleastoneobservation, withoneexpertrecommendingmorethantwopatients,andone recommendingfivetotenpatients.Butitwasagreedthatsome nursesmayneeda repeatevaluation. Thepanelagreedthatan annualassessmentwouldbebeneficial.Theconsensuswasthata
toolneededtobeameaningfullearningtool,thatincludednurse’s self-assessment to enablereflection ontheirown practice.The panelagreed thatarticulated feedback inwhich a plan for any improvementcanbediscussedandagreeduponwasimperative. Overallthetoolandprocessneedtobepracticalandworkable,so itwillbeappliedandbecomepartofthenormalpractice.
Individualqualitativethemesforthethreetoolsreviewedare summarisedinTable3.Thethemeswerepredominantlyaround addingitemsdeemedimportantsuchascheckingpatientallergies andclarificationtoensurecontentwasconciseandnotduplicated. Examplesofquestionsdeemednotrelevantincludedthosethat werelongandusedmultiplecriteriatomakeanevaluation, mak-ingitunclearonwhatwasbeingchecked.TheMwRTcontentwas specifictoUKmentalhealthnurses.Halfofthecontentwasratedas irrelevanttothegeneralnursepopulationandwouldrequiremajor revision.Howitemsweremeasuredwasnotalwaysobservable,and whatwastheoutcomeonceitwaschecked,wasitcorrect?
Usingtheresultsofthefeedbackfromthefacevaliditysurvey thetool wasrevisedfor furtherevaluation withintra-raterand inter-ratertesting(Table4).
5. Discussion
Theaimofthisstudywastoidentifysuitableandrelevant con-tentrequiredforinclusioninanevaluationtoolfornursingstaff undertakingmedicationadministrationintheclinicalsettingby reviewingthecontentofthreeexistingtools.
The MwRT was very long containing 45 questions and was specifictomentalhealthnursesintheUK.Thecontentwas compre-hensiveincludingproceduralstepsforappropriatehandhygiene, considerationofwhetheritisapplicableforthepatientconditionas wellasengagingthepatientinthemedicationadministration.Only halfofthecontentwasratedasrelevantandwouldthereforeneed revisionforuseinthegeneralnursepopulation.Thetool there-forewasdeemednotpracticalorrelevanttothegeneralnursing medicationsafetysetting.
TheMASAThadthefewestquestionsandratedthehighest rele-vanceforallthreetools.Thisensureditwasconciseandeasytouse. Thestudywasdesignedspecificallyforstudentnurses.Although
Table4
ExampleofContentinDesignedMAEFT.
RightMedication
1 Checkedthemedicationagainstthemedicationorderandconfirmedthe medicationnameandformulationiscorrect.
2 Confirmedthemedicationisindicatedforthepatientdiagnosisandchecked therearenoduplicateordersofthemedicineorofsimilarclassofmedicine. 3 Checkedthemedicationexpiryiswithindate.
RightProcedure
1 Nurseconductspatientobservationspriortoadministeringthemedication asrequired.
2 Nurseconductshandhygieneandusesappropriatepersonalprotective equipmentasrequiredwhenadministeringthemedication.
3 Nurseusesstandardnon-touchoraseptictechniquewhenpreparingand administeringmedication.
4 Nurseconfirmsifmedicationrequires2nursestocheck.Ifso,bothnurses performanindependentcheckandcalculation.
thiscouldbeextrapolatedtothegeneralnursepopulation. The expertpanelidentifiedanumberofgaps–suchasnocheckingof thepatient“allergies”whichiscrucialtoavertre-exposureofthe patienttoknownadversedrugreactions(ADR)and preventable harmandakeycomponentinAustralianMedicationSafety Stan-dard4 (AustralianCommissiononSafety andQualityin Health Care,2012b).Inaddition,therewereonlytwopatientidentifiers andinAustralia,Standard5.PatientIdentificationandProcedure Matchingrequiresatleastthreeidentifierstoconfirmthecorrect patient;patientname, dateofbirth anduniquehospital record number(AustralianCommissiononSafetyandQualityinHealth Care,2012a).Thepanelidentifiedthatanumberofthequestions withinthetoolwereunclearandambiguous.
TheCSATratedashavingexcellentcontentvalidity.Thepanel didhighlightsomedisadvantages however.Notallcomponents werewrittenasobservableandmeasurabletasks.Anexamplewas thecheckingofthepatientidentificationwherethepatientchart label,hospitalrecordnumber,dateofbirthandallergieswereall onequestion.Thesewouldneedtobeseparatecriteriainthetool. Thetoolwasfoundtobecomprehensivebutsomeofthecontent wasduplicatedsuchasrequirementsforsinglenursecheckandtwo nursecheckwhichwerethesame.Onlythetoolfororal, subcuta-neousandintramuscularmedicationadministrationofthepackage wasreviewedhowever,thepackageincludedtwootherseparate toolsfordifferentroutesandtypesofmedicationsthatwerenot reviewed.
Therefore,theliteraturehasidentifiedadearthofappropriate toolsforevaluationofallnurses’medicationadministrationclinical practicethatarereliableandvalidated.
Itisimportantthatthedesignofanevaluationtoolisgenericto theadministrationprocesswithgenericterms,soitisnot coun-tryspecificto make it as universalas possible.Although there aredifferencesininternationalpracticese.g.USApre-madeand automateddispensedmedications,thecorecheckingrequirements shouldremainthesame.Norshouldthedifferencebetweenthe typesofmedicationadministration(e.g.fromtheoriginal pack-age,adoseadministrationaidorautomateddispensingsystem) impacttheuniversalityofamedicationadministrationevaluation tool.Itshouldalsobegenericforanymedicationadministration setting,suchas;inahospitalwardenvironment,proceduralarea, nursinghomeorcommunity.Medicationadministrationstandards ofpracticeshouldremainthesameregardlessofprofessione.g. Nursing,medicalofficersandalliedhealthstaffsuchas
physiother-apists.Hencethereisaneedfordesigningagenericmedication administrationtoolsuitableforusebyallclinicians.
6. Conclusion
The expert panel identified that the content of a medica-tionadministrationself-evaluation,observationandfeedbacktool neededtobeclear,conciseandobservableinordertobeuseful. Specificcriteriawereestablishedbasedonthreetoolsidentified in the literature. Such a tool needed to be generic for use by allnursesregardlessofexperience,specialtyandclinicalsetting. Nursesneededtoself-evaluatefirsttoenablereflectionontheir ownpractice.Formative,notsummative,feedbackbytheobservers wasidentifiedaskey,aswasanagreeddevelopmentalplanforthe tooltobeutilisedasalearningtool.Importantly,self-awareness andfeedbackofclinicalpracticemayprovidemotivationto main-tain and improvestandards of care,potentially reducing errors andprovidingsafermedicationadministrationpracticeandbetter patientoutcomes.Futurestudieswillinvolvevalidatingfor inter-raterandintra-raterreliabilityandfurthertestingintheclinical setting.
Ethicalapprovalstatement
Thisstudydidnotinvolvehumanoranimalresearchandwas grantedan exemptionfromHighRiskEthics bytheRoyal Bris-baneandWomen’sHospitalHumanResearchEthics Committee HREC/16/QRBW/351on11thJuly2016.
ExpertPanelReviewArticle Conflictofintereststatement
Therewasnoconflictofinterestsinconductingthisstudyfor anyoftheauthors.
Acknowledgments
Theauthorsaregratefultotheexpertpanelwhotookthetime tocompletethequestionnairesandparticipateinthereviewofthe contentanddesignoftheMAEFT.Theauthorswouldliketothank QIMRBerghoferMedicalResearchInstitutestatisticiansfortheir expertiseandadvice.
ThisworkwassupportedandfundedbytheQueenslandHealth, Metro North Hospital and Health Services, Royal Brisbane & Women’sHospital,ResearchPostgraduateScholarships2017for thefirstauthorPhDcandidatethroughtheUniversityof Queens-land.
References
AustralianCommissiononSafetyandQualityinHealthCare.(2012a).National safetyandqualityhealthservicestandardsSydneyRetrievedfrom.ACSQHC. https://www.safetyandquality.gov.au/wp-content/uploads/2011/09/NSQHS-Standards-Sept-2012.pdf
AustralianCommissiononSafetyandQualityinHealthCare.(2012b).safetyand qualityimprovementGuidestandard4:Medicationsafety(october2012).Sydney AustralianCommissiononSafetyandQualityinHealthCare.
Bull,E.R.,Mason,C.,Junior,F.D.,Santos,L.V.,Scott,A.,Ademokun,D.,&Cavanagh, S.M.(2017).Developingnursemedicationsafetytraininginahealth partnershipinMozambiqueusingbehaviouralscience.Globalizationand Health,13,45.http://dx.doi.org/10.1186/s12992-017-0265-1
Butler,D.L.,&Winne,P.H.(1995).Feedbackandself-regulatedlearning:A theoreticalsynthesis.ReviewofEducationalResearch,65(3),245. Coates,V.E.,&Chambers,M.(1992).Evaluationoftoolstoassessclinical
competence.NurseEducationToday,12(2),122–129.http://dx.doi.org/10.1016/ 0260-6917(92)90038-P
Coombes,I.,Avent,M.,Cardiff,L.,Bettenay,K.,Coombes,J.,Whitfield,K.,&Bates,I. (2010).Improvementinpharmacist’sperformancefacilitatedbyanadapted competency-basedGenerallevelframework.JournalofPharmacyPracticeand
Research,40(2),111–118.http://dx.doi.org/10.1002/j.2055-2335.2010. tb00517.x
Coombes,I.D.,Heel,A.C.,Stowasser,D.A.,Reid,C.M.,Henderson,A.,&Mitchell,C. A.(2005).Identificationofmedicationerrorsbynursesduringasimulated ward,medicationsafetyorientationprogram.JournalofPharmacyPracticeand Research,35(3),190–194.http://dx.doi.org/10.1002/j.2055-2335.2005. tb00336.x
Coyne,E.,Needham,J.,&Rands,H.(2013).Enhancingstudentnurses’medication calculationknowledge;Integratingtheoreticalknowledgeintopractice.Nurse EducationToday,33(9),1014–1019.http://dx.doi.org/10.1016/j.nedt.2012.04. 006
Davies,K.,Mitchell,C.,&Coombes,I.(2015).TheRoleOfObservationAnd FeedbackInEnhancingPerformanceWithMedicationAdministration.Journal ofLawandMedicine,23(2),316.
Fisher,M.,&Parolin,M.(2000).Thereliabilityofmeasuringnursingclinical performanceusingAcompetencybasedassessmenttool:Apilotstudy. Collegian,7(3),21–27.
Goodstone,L.,&Goodstone,M.S.(2013).Useofsimulationtodevelopa medicationadministrationsafetyassessmenttool.ClinicalSimulationin Nursing,9(12),e609–e615.http://dx.doi.org/10.1016/j.ecns.2013.04.017,601p. Gunningberg,L.,Pöder,U.,Donaldson,N.,&LeoSwenne,C.(2014).Medication
administrationaccuracy:Usingclinicalobservationandreviewofpatient recordstoassesssafetyandguideperformanceimprovement.Journalof EvaluationinClinicalPractice,20(4),411–416.http://dx.doi.org/10.1111/jep. 12150
Härkänen,M.,Ahonen,J.,Kervinen,M.,Turunen,H.,&Vehviläinen-Julkunen,K. (2015).Thefactorsassociatedwithmedicationerrorsinadultmedicaland surgicalinpatients:Adirectobservationapproachwithmedicationrecord reviews.ScandinavianJournalofCaringSciences,29(2),297–306.http://dx.doi. org/10.1111/scs.12163
Härkänen,M.,Voutilainen,A.,Turunen,E.,&Vehviläinen-Julkunen,K.(2016). Systematicreviewandmeta-analysisofeducationalinterventionsdesignedto improvemedicationadministrationskillsandsafetyofregisterednurses. NurseEducationToday,41,36–43.http://dx.doi.org/10.1016/j.nedt.2016.03.017 Hemingway,S.,Baxter,H.,Smith,G.,Burgess-Dawson,R.,&Dewhirst,K.(2011).
Collaborativelyplanningformedicinesadministrationcompetency:Asurvey evaluation.JournalofNursingManagement,19(3),366–376.http://dx.doi.org/ 10.1111/j.1365-2834.2011.01245.x,311p.
Jennings,B.M.,Sandelowski,M.,&Mark,B.(2011).Thenurse’smedicationday. QualitativeHealthResearch,21(10),1441–1451.http://dx.doi.org/10.1177/ 1049732311411927
Liˇcen,S.,&Plazar,N.(2015).Identificationofnursingcompetencyassessmenttools aspossibilityoftheiruseinnursingeducationinSlovenia;Asystematic literaturereview.NurseEducationToday,35(4),602–608.http://dx.doi.org/10. 1016/j.nedt.2014.12.023
Long,D.,Young,J.,Rickard,C.M.,&Mitchell,M.L.(2013).Measuringpaediatric intensivecarenursingknowledgeinAustraliaandNewZealand:Howthe basicknowledgeassessmenttoolforpediatriccriticalcarenurses (PEDS-BKAT4)performs.AustralianCriticalCare,26(1),36–42.http://dx.doi. org/10.1016/j.aucc.2012.02.004
Molloy,E.,&Boud,D.(2013).Seekingadifferentangleonfeedbackinclinical education:Thelearnerasseeker,judgeanduserofperformanceinformation. MedicalEducation,47(3),227–229.http://dx.doi.org/10.1111/medu.12116 O’Brien,E.(2015).MedicationresourcepackageRetrievedfrom.RBWHintranet:
RoyalBrisbaneandWomen’sHospital(RBWH).http://hi.bns.health.qld.gov.au/ nursing/education.htm#workforcedevelopment
Polit,D.F.,&Beck,C.T.(2006).Thecontentvalidityindex:Areyousureyouknow what’sbeingreported?Critiqueandrecommendations.ResearchinNursing& Health,29(5),489–497.http://dx.doi.org/10.1002/nur.20147
Polit,D.F.,&Beck,C.T.(2008).InDeniseF.Polit,&CherylTatanoBeck(Eds.), Nursingresearch:Generatingandassessingevidencefornursingpractice. Philadelphia:Philadelphia:WoltersKluwerHealth/lippincottWilliams& Wilkins.
Popescu,A.,Currey,J.,&Botti,M.(2011).Multifactorialinfluencesonand deviationsfrommedicationadministrationsafetyandqualityintheacute Medical/Surgicalcontext.WorldviewsonEvidence-BasedNursing,8(1),15–24. http://dx.doi.org/10.1111/j.1741-6787.2010.00212.x
Sinclair,P.M.C.,Shanahan,M.,&Monica,B.S.(2014).Thedevelopmentofa medicationcalculationcompetencyandqualityuseofrenalmedicine e-learningprogram.RenalSocietyofAustralasiaJournal,10(2),58–60. Spector,J.M.(2014).Handbookofresearchoneducationalcommunicationsand
technology.InFeedbackmodelsforlearning,teachingandperformance.pp. 413–424.Retrievedfrom.http://download.springer.com.ezproxy.library.uq. edu.au/static/pdf/665/chp%3A10.1007%2F978-1-4614-3185-533. pdf?originUrl=http%3A%2F%2Flink.springer.com%2Fchapter%2F10. 1007%2F978-1-4614-3185-5 33&token2=exp=1474253239∼acl=%2Fstatic%2Fpdf%2F665%2Fchp%3A10. 1007%2F978-1-4614-3185-533.pdf%3ForiginUrl%3Dhttp%3A%2F%2Flink. springer.com%2Fchapter%2F10.1007%2F978-1-4614-3185-5 33*∼hmac=c0a5d32a8bd7b12e9b6235c2f9ae36a2f977b71f12a11c18c1cf 38968d34a577
Stacey,S.,Wainwright,C.,Coombes,I.,&Whitfield,K.(2014).Usingthe ¨general levelframework¨toidentifygapsinknowledgeandskillstoprioritise professionaldevelopmentactivitiesforpaediatricpharmacists.(report). ArchivesofDiseaseinChildhood,99(8).
Stolic,S.(2014).Educationalstrategiesaimedatimprovingstudentnurse’s medicationcalculationskills:Areviewoftheresearchliterature.Nurse EducationinPractice,14(5),491–503.http://dx.doi.org/10.1016/j.nepr.2014.05. 010
Turner,J.,Gardner,B.,Staples,T.,&Chapman,J.(2007).Medicineswithrespect: Developinganintegratedcollaborativeapproachtomedicationmanagement. MentalHealthNursing,27(6),16–19.
Turner,J.,Gardner,B.,Staples,T.,&Chapman,J.(2008).Medicineswithrespect (parttwo):Implementationandevaluationofamedicationmanagement initiativeinacutein-patientsettings.MentalHealthNursing,28(1),12–15. Westbrook,J.I.,Duffield,C.,Li,L.,&Creswick,N.J.(2011).Howmuchtimedo nurseshaveforpatients?Alongitudinalstudyquantifyinghospitalnurses’ patternsoftasktimedistributionandinteractionswithhealthprofessionals. BMCHealthServicesResearch,11(319) http://dx.doi.org/10.1186/1472-6963-11-319
Westbrook,J.I.,Rob,M.I.,Woods,A.,&Parry,D.(2011).Errorsinthe
administrationofintravenousmedicationsinhospitalandtheroleofcorrect proceduresandnurseexperience.BMJQuality&Safety,20(12),1027–1034. http://dx.doi.org/10.1136/bmjqs-2011-000089
Westbrook,J.I.,Woods,A.,Rob,M.I.,&Dunsmuir,W.T.M.(2010).Associationof interruptionswithanincreasedriskandseverityofmedicationadministration errors.ArchivesofInternalMedicine(1960),170(8),683–690.http://dx.doi.org/ 10.1001/archinternmed.2010.65
Wikander,L.,&Bouchoucha,S.L.(2018).Facilitatingpeerbasedlearningthrough summativeassessment–Anadaptationoftheobjectivestructuredclinical assessmenttoolfortheblendedlearningenvironment.NurseEducationin Practice,28(SupplementC),40–45.http://dx.doi.org/10.1016/j.nepr.2017.09. 011
WorldHealthOrganisation.(2017).WHOlaunchesglobalefforttohalve medication-relatederrorsin5yearsRetrievedfrom.http://www.who.int/ mediacentre/news/releases/2017/medication-related-errors/en/