The Relationship Between Muscle Length Imbalance and the Occurrence of Scoliosis and Back Pain in Collegiate Female Gymnasts
Caroline Campbell
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for graduation with honors in the
Department of Exercise and Sport Science 2015
Approved by:
______________________________________ Advisor: Meredith Petschauer, PhD, LAT, ATC
______________________________________ Reader: Abbie Smith-Ryan, PhD, CSCS, CISSN
ABSTRACT
Caroline Campbell: The Relationship Between Muscle Length Imbalance and the Occurrence of Scoliosis and Back Pain in Collegiate Female Gymnasts
(Under the direction of Dr. Meredith Petschauer)
Gymnastics at the collegiate level is unique in that these elite athletes begin high volume and high intensity training at a very young age. The sport is unilateral meaning each gymnast has a dominant leg that always leads in split leaps and a dominant side to which they always twist. The combination of these factors puts the gymnast at risk for developing muscle length
imbalances between their dominant and non-dominant sides. With such a high incidence of back pain in this population, more research was needed to investigate any relationships with potential muscle length imbalances. The purpose of this study was to determine if collegiate women gymnasts exhibit muscle length imbalances in the lower extremity and if these imbalances were related to back pain, the amount of spinal curvature, or both. Muscle length measurements of the iliopsoas, rectus femoris, hamstrings, and quadratus lumborum were taken on 13 UNC female varsity gymnasts. Participants completed a Modified Oswestry Disability Index if they
experienced back pain. Using the angle tool on Image J software, the amount of spinal curvature for each gymnast was measured from a dual energy x-ray absorptiometry (DXA) scan. A
ACKNOWLEDGMENTS
Thank you to Dr. Meredith Petschauer, for your constant guidance from this project’s inception until the final round of editing. You’ve taught me more than you can imagine and I have truly enjoyed working with you this year.
Thank you to my best friend, for believing in me before I believed in myself. I probably would have talked myself out of doing this project if it weren’t for your encouragement and support from the moment I first thought about writing an honors thesis.
TABLE OF CONTENTS
Page
LIST OF TABLES………...v
LIST OF FIGURES………...v
CHAPTER 1. INTRODUCTION………..1
1.1. A Statement of the Problem………1
1.2. Research Questions……….4
1.3. Research Hypothesis………...6
1.4. Operational Definitions………...7
1.5. Limitations………..7
1.6. Assumptions………7
1.7. Independent Variables………8
1.8. Dependent Variables………...8
CHAPTER 2. REVIEW OF THE LITERATURE………9
2.1. Epidemiology of Injuries in Gymnastics………9
2.2. Muscular Flexibility Imbalance and Unilateral Issue in Sports………11
2.3. Muscular Strength Imbalance………...15
2.4. Instrumentation……….17
CHAPTER 3. METHODOLOGY………...22
3.1. Subjects……….22
3.2. Procedure………..22
3.2.1. Thomas Test: Iliopsoas………...23
3.2.2. Modified Thomas Test: Rectus Femoris……….24
3.2.3. Straight Leg Raise Test: Hamstrings………..25
3.2.4. Side Bending Test: Quadratus Lumborum……….26
3.2.5. Back Pain Questionnaire……….27
3.2.6. Determining Spinal Curvature………27
3.3. Statistical Analysis………27
CHAPTER 4. RESULTS……….31
4.1. Subject Characteristics………..31
4.2. Muscle Length Imbalances………...31
4.3. Back Pain and Muscle Length Imbalances………...32
CHAPTER 5. DISCUSSION………...40
5.1. Muscle Lengths……….40
5.2. Muscle Length Imbalances and Back Pain………...41
5.3. Muscle Length Imbalances and Spinal Curvature………44
5.4. Sample Size………...46
5.5. Future Research………47
5.5. Conclusions………...48
6. APPENDIX A………..49
LIST OF TABLES
Table 1: Subject Characteristics………...34
Table 2: Average Muscle Lengths………...34
Table 3. Paired Samples T Test Results………...34
Table 4. Pearson Correlations: Back Pain………34
Table 5. Pearson Correlations: Curvatures………..34
LIST OF FIGURES Figure 1. Back Pain vs. Iliopsoas Imbalance………...35
Figure 2. Back Pain vs. Rectus Femoris Imbalance……….35
Figure 3. Back Pain vs. Hamstring Imbalance……….36
Figure 4. Back Pain vs. Quadratus Lumborum Imbalance………..36
Figure 5. Curvature vs. Iliopsoas Imbalance………...37
Figure 6. Curvature vs. Rectus Femoris Imbalance……….37
Figure 7. Curvature vs. Hamstring Imbalance……….38
Figure 8. Curvature vs. Quadratus Lumborum Imbalance………...38
Chapter I: Introduction
A Statement of the Problem
There are over 1,650 student-athletes participating in 83 different collegiate women’s gymnastics programs across the United States [1].While this may seem like a small number, there are over 1.8 million people over the age of six that participate in gymnastics over 50 times per year in the US [2]. Many of the elite gymnasts participating at the high school and collegiate level have been training intensely for the majority of their lives. This intense training throughout periods of rapid growth, such as during puberty, puts the spine at an increased risk for injury [3]. The NCAA Injury Surveillance System reports that low back strains account for 6.1% of injuries during practice and 3.2% of injuries during competition [4]. However, a study collecting injury incidence data on collegiate gymnasts at the
University of Utah used a more inclusive definition of injury found that low back pain and injuries accounted for 11.6% of total injuries by body part [5]. For many gymnasts, back pain becomes a chronic issue with one in four injuries presenting as a re-injury [3]. This has important implications for the athlete even after retirement, as back pain tends to persist for long periods of time [3].
tightness was the only factor associated with low back pain [7]. In contrast, Nadler found that inflexibility of the lower extremity was not associated with low back pain [8]. Since
gymnasts are unilateral athletes and tend to exhibit extreme flexibility, they are an interesting population in terms of how they relate to many of the existing studies on low back pain and muscle imbalance.
In addition to the incidence of low back pain, muscle imbalances may also be related to the development of scoliosis. While the etiology for adolescent idiopathic scoliosis isn’t completely understood, many theories include persistent asymmetric loading of the spine that disturbs the balance of muscles [9]. This type of asymmetric loading is highly prevalent in gymnastics, as many skills involve balancing on one arm or leg and a large number of repetitions are performed daily in practice. Other theories include ligamentous laxity and delayed menarche, but in reality the etiology is most likely multi-faceted with all three mechanisms (and possibly more) playing a role in initiating scoliosis [9]. While weight-bearing exercise is important for the development of bone strength in youth, there may be a limit to how much is healthy. It is unclear if there is a point at which intense training in a unilateral sport is putting the athlete at risk for developing spinal curvatures.
Research Questions
1. Muscle Length:
a. Is there a significant difference in the length of the iliopsoas between the dominant and non-dominant side?
b. Is there a significant difference in the length of the rectus femoris between the dominant and non-dominant side?
c. Is there a significant difference in the length of the hamstrings between the dominant and non-dominant side?
d. Is there a significant difference in the length of the quadratus lumborum between the dominant and non-dominant side?
2. Imbalance and Back Pain Comparisons:
a. Is there an association between an imbalance of the length of iliopsoas and back pain?
b. Is there an association between an imbalance of the length of the rectus femoris and back pain?
c. Is there an association between an imbalance of the length of the hamstrings and back pain?
d. Is there an association between an imbalance of the length of the quadratus lumborum and back pain?
3. Imbalance and Scoliosis Comparisons:
b. Is there an association between an imbalance of the length of the rectus femoris and the degree of spinal curvature?
c. Is there an association between an imbalance of the length of the hamstrings and the degree of spinal curvature?
Research Hypothesis
1. Muscle Length:
a. The dominant side will have a shorter iliopsoas than the non-dominant side. b. The dominant side will have a shorter rectus femoris than the non-dominant side. c. The dominant side will have longer hamstrings than the non-dominant side.
d. The dominant side will have a shorter quadratus lumborum than the non-dominant side.
2. Imbalance and Back Pain Comparisons:
a. An imbalance of the length of the iliopsoas will be associated with back pain. b. An imbalance of the length of the rectus femoris will be associated with back pain. c. An imbalance of the length of the hamstrings will be associated with back pain. d. An imbalance of the length of the quadratus lumborum will be associated with back pain.
3. Imbalance and Scoliosis Comparisons:
a. An imbalance of the length of the iliopsoas will be associated with spinal curvature. b. An imbalance of the length of the rectus femoris will be associated with spinal curvature.
c. An imbalance of the length of the hamstrings will be associated with spinal curvature.
Operational Definitions
Back pain: measured as a percent score based on a modified Oswestry Disability Index
Dominant side: defined as the gymnast’s preferred lead leg and the side twisted to during routines
Non-dominant side: opposite side of the dominant side
Muscle length: the end to end measurement of a muscle, expressed in degrees based on its corresponding muscle length test
o Iliopsoas: measured using the Thomas test
o Rectus femoris: measured using the modified Thomas test
o Hamstrings: measured using the straight leg raise test
o Quadratus lumborum: measured using the side bending test
Scoliosis: Lateral curvature of the spine of 10 or more as shown by DXA scans with no apparent positioning error
Limitations
Small sample size
Only collecting data at one point in time during the season
No control over therapy or treatment that athletes are currently receiving
Assumptions
Athletes are truthful when answering the questionnaire Independent Variables
1. Non-dominant or dominant side 2. Imbalance of muscle lengths
Dependent Variables
1. Muscle Length a. Iliopsoas b. Rectus Femoris c. Hamstrings
d. Quadratus Lumborum 2. Back Pain
Chapter II: Review of the Literature
Epidemiology of Injuries in Gymnastics
Gymnasts competing at any level put a high degree of stress on their backs due to the repetitive flexion and hyperextension positions needed in skills such as vaulting and
dismounts, the high compressive forces on the spine during landings, and rotational forces needed for twists [3]. It is common for gymnasts to begin training as early as the age of six. Therefore, most collegiate level gymnasts have been putting these strains on their body for the majority of their lives. Caine and Nassar found that while a majority of gymnastics injuries are sudden onset (52.0-83.4%), chronic injuries are more prevalent as the
competitive level increases [3]. Additionally, whether an injury is acute or chronic is often related to the involved body part [3]. For example wrist and back pain tends to present more chronically, while ankles are more often injured acutely. Therefore, due to competing at a high level and training for such a long period of time, it is logical that many collegiate gymnasts experience back injuries at some point in their career.
injury [11]. Gymnastics is a skill-specific sport, so while an ankle injury may prevent an athlete from practicing on the beam, they may still be allowed to work on the bars during practice and would have a lower time loss compared to an athlete with the same injury in another sport. Sands et al. reported that gymnasts trained with an injury during 71% of all exposures (practices, competitions, and conditioning) [5], which supports the notion that gymnasts are often able to continue practicing to some extent despite an injury. Likewise, the data on low back injuries reported by the NCAA Injury Surveillance System (NCAA ISS) may not accurately represent the true incidence because athletes with chronic low back pain may be able to continue to practice while not having any time loss and would therefore not be included in the data [4].
In order to include injuries that did not cause the athlete to sit out for at least a day of practice, Sands et al. collected data on 37 gymnasts over a five year period at the University of Utah defining an injury as “any damaged body part that would interfere with training” [5]. With this more inclusive definition of injury, the lower back was the most injured body part at 11.56% of total injuries [5]. Sands et al. also recorded the side of the injury for upper and lower extremities and found that the right side of the body was injured more than the left and that this discrepancy was statistically significant [5]. This is of interest when considering that, unlike bilateral sports such as swimming or running, gymnasts have a preferred side that they always rotate to and a dominant leg that is always the lead leg.
Muscular Flexibility Imbalance and Unilateral Issue in Sports
between the right and left side or antagonist muscle groups could result in pain or injury in other parts of the lower extremity, including the low back.
In agreement with the link theory, Knapik et al. hypothesized that injury could result due to inadequate absorption of force by the weaker side [6]. This study followed 138 female collegiate athletes across eight varsity sports at a division I university for three years. These athletes were 2.6 times more likely to sustain a lower extremity injury when the right hip extensor was 15% or more flexible than the left hip extensor [6]. However, athletes with greater range of motion in the left hip extensor were only 1.7 times more likely to withstand a lower extremity injury [6]. While this relationship was not statistically significant, it does show that the imbalance correlation is present on both sides. An additional item to note with this study is that less than half of the subjects with a hip extensor imbalance had more range of motion in their left hip, therefore, a small sample size could be the reason why statistical significance was not found on that side. Another study found a positive correlation between a flexibility imbalance and injury, but with different muscle groups. Kujala et al. studied the relationship between a number of subject characteristics and a lifetime cumulative incidence of low back pain in 105 male and female athletes with an average age of 12 across a
multitude of sports [7]. Tightness of the hip flexors was the only measure that was statistically significant in relationship with an increased frequency of low back pain [7]. While it’s evident that hip musculature affects the low back and that imbalances between muscle groups can increase the potential for injury, there are many factors that remain unclear.
low back pain [15]. For example, increased right hip symptoms were associated with increased shoulder horizontal abduction range, while increased left hip symptoms were associated with decreased hip extension and spinal flexion [15]. However, gymnasts that experienced low back pain only had greater toe touching ability (finger to heel distance) than those without symptoms. This study suggests that pain or injury could be associated with area specific flexibility as opposed to overall flexibility.
In a study measuring flexibility, joint laxity, leg length discrepancy, and presence of overuse syndromes (determined by a history of ongoing discomfort and tenderness with palpation) during pre-participation physicals of 257 college athletes across 9 varsity sports, Nadler followed the athletes to see if there were any associations with the development of low back pain throughout the season [16]. During that time frame 6% of men and 15% of women experienced low back pain, however only athletes with lower extremity ligamentous laxity or overuse syndromes were at a greater risk for the development of low back pain [16]. Inflexibility of the lower extremity and leg length discrepancies were not associated with low back pain, however it is important to note that flexibility was measured on a
that if the correlation with low back pain is not a flexibility imbalance then strength
discrepancies could be the issue [16]. Nadler’s later study is explained in the strength section. In addition to differing views on the role of flexibility, opposing views on the
Muscular Strength Imbalance
An alternative hypothesis for the development of low back pain is the presence of strength differences between opposing muscle groups or between right and left sides. In addition to observing increased low back pain with increased spine rigidity, Kums et al. found that rhythmic gymnasts had an imbalance in muscle tone between spinal muscles (erector spinae) and abdominals [17]. Muscle tone was defined as the tension of skeletal muscle that helps ensure balance, posture, and creates the background tension necessary for active movements [17]. The gymnasts’ spinal muscles had more tone than the abdominals, but the control group did not exhibit any imbalance. Therefore, the discrepancy was most likely due to the repeated back hyperextension movements required by the sport [17]. Hyperextension could cause a reduction of trunk flexor tone because the abdominals are continuously stretched as the spinal muscles contract. Most importantly, the imbalance between erector spinae and abdominal tone was related to an increased incidence of low back pain [17]. However, it is unclear whether this imbalance is a predisposition to low back pain or is a result of previous injury.
episode groups [18]. Therefore, this study suggests that correcting an erector spinae muscle recruitment imbalance may not be critical in the prevention of low back pain.
In terms of strength differentials in the lower extremity associated with low back pain, a few relationships have been discovered. Arab and Nourbakhsh found that there was no significant difference in abductor strength between low back pain subjects with or without IT band tightness [19]. However, subjects without low back pain had significantly stronger hip abductors compared to those experiencing low back pain [19]. Therefore, IT band tightness was not a factor in determining the presence of low back pain in patients aged 20-60. Nadler et al. measured hip strength between sides in 210 NCAA division I athletes (140 males, 70 females) and found that females with no lower extremity injury in the past year had left hip extensors that were 10.9% stronger than their right hip extensors [14]. For
comparison, female athletes with a lower extremity injury in the past year had left hip
extensors that were only 1.3% stronger than their right hip extensors [14]. It is logical that the left side is stronger because most people are right handed and therefore use their left foot for support/balance when using their right foot for gross or fine movements (such as kicking) [14]. Additionally, females that reported low back pain had greater differences in side-to-side strength. The left hip extensor was 11.7% stronger than the right in female athletes that reported low back pain, while only 5.9% stronger in those that did not report low back pain, and there was no significant difference between sides for hip abductors in either group [14]. Nadler offers two possible explanations for the differences in strength between athletes with prior lower extremity injury and low back pain. Prior low back pain could stimulate
development of low back pain [14]. As there were no significant correlations for muscular imbalances and lower extremity injury or low back pain for males, this study sheds light on possible factors in the discussion of how men and women’s bodies may respond differently to injury.
Taking into consideration all the conflicting evidence on how, or if, imbalances in flexibility, spinal configuration, or strength play a role in the presence of injury or low back pain, it is clear that more research needs to be done to clarify and expand upon this
relationship. With such a high prevalence of low back pain in sports, and particularly
gymnastics, this research could lead towards finding ways to prevent the development of low back pain and could therefore help improve athlete performance.
Instrumentation
section, both scoliosis and degree of lumbar lordosis have implications for low back pain. Therefore, it is critical that these three characteristics can be measured reliably and accurately.
One of the greatest issues with measuring lumbar lordosis in a clinical setting is that goniometers cannot be used. The bubble inclinometer, similar to the tool used in Ohlen’s study to measure lumbar mobility, is an effective instrument in measuring lumbar lordosis. However, it tends to not be as accessible or familiar to clinicians in comparison to the goniometer [22]. Due to the widespread use of smartphones and their wide variety of applications, Salamh and Kolber studied whether the iHandy® Level application on an IPhone 4 could be used to accurately and reliably measure lumbar lordosis. The iHandy® Level application is a free product that uses the iPhone’s built in accelerometer to measure angles, generally used for leveling pictures on walls or for construction projects. To measure lumbar lordosis in this study, each subject was marked at the T12 and S1 spinous processes, using the iliac crest as a baseline landmark for L4-L5 [22]. To obtain the measurement, the instrument was placed at the T12-L1 and S1-S2 landmarks; angles were recorded and then added together. The measurement was repeated and the mean of the two values from each instrument were used in the analysis. The results of the study showed good inter-rater and intra-rater reliability for the inclinometer and IPhone application when measuring
level application is a feasible way for both researchers and clinicians to measure lumbar lordosis.
The preferred method for diagnosing scoliosis is through measuring spinal curvature by either the Cobb or Ferguson angle on an X-ray. Due to the high levels of radiation from an X-ray, it would be unethical to require research subjects to be unnecessarily exposed to this radiation, which may limit the accuracy of scoliosis prevalence data due to false negatives on tests such as the Adams forward bend. Dual energy x-ray absorptiometry (DXA) scans use less than one percent of the radiation of that of an X-ray, however subjects lay flat during the scanning which could prevent accurate scoliotic diagnosis [23]. Taylor et al. created a
Standard tests for measuring muscle length of muscles in the lower extremity were conducted on 72 college-aged students (47 females, 25 males), excluding elite athletes, those with previous lower extremity or low back surgery, and those with severe postural issues [24]. The Thomas test was used to measure the length of the iliopsoas, where the subject’s low back and sacrum was on the table with their knees just hanging off the edge. The subject was instructed to bring their contralateral knee towards their chest as far as they can without their back leaving the table. If the iliopsoas was shortened, the thigh came off the table and measurements were taken by aligning the goniometer with the axis over the greater
trochanter, the stationary arm over the lateral midline of the trunk, and the moving arm in line with the lateral epicondyle of the femur [20]. In Corkery’s study the mean angle of hip flexion in the females was 2.2°± 2.3° on the right side and 2.0°±1.8° on the left, with a mean total of 2.3° ±1.9° [24].
The Modified Thomas test was used to measure the length of the rectus femoris. This test was set up similar to the Thomas test, however instead, the goniometer’s axis was aligned at the lateral epicondyle of the femur, the stationary arm in line with the greater trochanter of the femur, and the moving arm at the lateral malleolus and knee flexion is recorded [20]. Corkery found that the mean angle of knee flexion for females was
Chapter III: Methodology
Subjects
Fifteen female varsity gymnasts at the University of North Carolina at Chapel Hill participated in this research study. Participants were excluded if they had surgery in the past 3 months on the date of testing. There were no limitations to inclusion regarding current pain or injury. Participants were recruited by the women’s gymnastics head athletic trainer. Prior to testing, all participants signed consent forms approved by the Institutional Review Board. Demographic information, including age, height, weight, lead leg, side twisted to, and length of time training as a gymnast, was collected on each participant.
Procedure
Participants came into the Sports Medicine Research Lab one time to test the length of their iliopsoas, rectus femoris, hamstrings, and quadratus lumborum and answer a
Thomas Test: Iliopsoas
The participant laid supine with the buttock on the edge of the table so that the legs are hanging off the edge. The examiner flexed the contralateral hip, bringing the knee to the chest, far enough to flatten the lumbar spine against the table. The participant was asked to hold their knee in this position. The inclinometer was aligned along the midpoint of the top of the thigh and the measurement was recorded. It was critical that the participant did not pull their knee to their chest beyond what was needed to allow the spine to flatten against the table, as this could cause excessive rotation of the pelvis and an inaccurate measurement [20]. For the iliopsoas, the angle represents the degrees below the horizontal of the thigh during the Thomas Test.
Modified Thomas Test: Rectus Femoris
The starting position for the modified Thomas test was the same as for the original Thomas test. The participant was supine, with the knees extended just past the edge of the table. The examiner flexed the contralateral hip, bringing the knee towards the chest just far enough to flatten the lumbar spine. The participant as instructed to hold their knee in this position during the measurement. If the rectus femoris was shortened, the knee extended slightly [20]. The inclinometer was placed at the midpoint along the shin and the
measurement was recorded. The angles for the rectus femoris represented the degrees away from the vertical of the shin during the Modified Thomas Test. Therefore, the more negative the measurement, the shorter the muscle; whereas, positive values represented longer muscle length.
Figure 3: Modified Thomas test resting position [20]
Straight Leg Raise Test: Hamstrings
The participant started lying supine with both their hips and knees extended. The examiner then flexed the participant’s hip through its full range of motion, while maintaining full knee extension. The contralateral leg maintained a fully extended position throughout the test. The inclinometer was aligned along the midline of the back of the thigh, halfway
between the greater trochanter and the lateral epicondyle and the measurement was recorded. Due to the flexibility of the gymnasts, the hamstrings were measured in terms of degrees away from the vertical.
Figure 5: Resting position for straight leg raise test [20]
Side Bending Test: Quadratus Lumborum
The participant stood with their weight evenly distributed across both feet and arms relaxed at their sides. While in this resting position, a dot was marked on the thigh directly below the tip of the middle finger. The participant was then asked to lean as far as they could to one side, keeping the hips level, and another dot was marked below the tip of the middle finger. A tape measure was used to measure the distance in centimeters between the two dots. This procedure was repeated three times on each side, removing the dots in between each measurement.
Back Pain Questionnaire
First, each participant was asked if they currently experience any back pain. If the participant answered yes, they filled out a Modified Oswestry Disability Index in order to measure the functional impairment of her back pain. Those participants who answered that they had no back pain were given a score of zero. The version used is listed in Appendix A and includes a section relevant to the athlete’s ability to participate in gymnastics. The Modified Oswestry Disability Index used in this study has 11 sections, each with six possible answer choices. The choices are assigned points in order from zero to six. The total number of points was added across all sections and divided by 66 to obtain a raw score. The raw score was used in the data analysis. The higher the score on the Modified Oswestry Disability index, the greater the disability that was caused by the athlete’s back pain.
Determining Spinal Curvature
aligned with the center line. Lateral curvature was measured on the remaining scans that did not have an apparent positioning error using a modified Ferguson method [26]. This method entails drawing a normal line through the center of the spine, another line through the apex of the curve, and then using the angle tool of the ImageJ software to measure the angle at the intersection of the two lines. Any angle of 10° or greater was considered a scoliotic curve [23]. The degree value of the amount of curvature was used in the analysis.
Statistical Analysis
Statistical Analysis Table
Research Question Variables Statistical Test
1a. Is there a significant difference in the length of the iliopsoas between the dominant and non-dominant side?
IV: Side
DV: Length of iliopsoas
Paired Samples T-Test
1b. Is there a significant difference in the length of the rectus femoris between the dominant and non-dominant side?
IV: Side
DV: Length of rectus femoris
Paired Samples T-Test
1c. Is there a significant difference in the length of the hamstrings between the dominant and non-dominant side?
IV: Side
DV: Length of hamstrings
Paired Samples T-Test
1d. Is there a significant difference in the length of the quadratus lumborum between the dominant and non-dominant side?
IV: Side
DV: Length of quadratus lumborum
Paired Samples T-Test
2a. Is there an association between an imbalance of the length of iliopsoas and back pain?
IV: Iliopsoas length imbalance
DV: Back pain
Regression Analysis/ Pearson Correlation
2b. Is there an association between an imbalance of the length of the rectus femoris and back pain?
IV: Rectus femoris length imbalance
DV: Back pain
Regression Analysis/ Pearson Correlation
2c. Is there an association between an imbalance of the length of the hamstrings and back pain?
IV: Hamstrings length imbalance
DV: Back pain
Regression Analysis/ Pearson Correlation
2d. Is there an association between an imbalance of the length of the quadratus lumborum and back pain?
IV: QL length imbalance DV: Back pain
Regression Analysis/ Pearson Correlation
3a. Is there an association between an imbalance of the length of the iliopsoas and the presence of a scoliotic curve?
IV: Iliopsoas length imbalance
DV: Amount of curvature
Regression Analysis/ Pearson Correlation
3b. Is there an association between an imbalance of the length of the rectus femoris and
IV: Rectus femoris length imbalance
the presence of a scoliotic
curve? DV: Amount of curvature
3c. Is there an association between an imbalance of the length of the hamstrings and the presence of a scoliotic curve?
IV: Hamstrings length imbalance
DV: Amount of curvature
Regression Analysis/ Pearson Correlation
3d. Is there an association between an imbalance of the length of the quadratus
lumborum and the presence of a scoliotic curve?
IV: QL length imbalance DV: Amount of curvature
Regression Analysis/ Pearson Correlation
Chapter IV: Results
Data was collected for 13 subjects. The average age of the subjects was 20 years and they have been training as a gymnast for about three quarters of their lives, an average of 15 years. The gymnasts were all of similar height and weight with an average of 62.3 inches and 122.5 pounds. Subject characteristics can be found in Table 1. Dominance was defined as the lead leg for the iliopsoas, rectus femoris, and hamstrings, and the side twisted to for the quadratus lumborum. There were eight gymnasts with left leg dominance and five with right leg dominance. However, there were nine gymnasts with left side dominance and four with right side dominance, due to four gymnasts that twist to one side while their opposite leg leads. The average muscle lengths and standard deviations for each side are listed in Table 2.
Muscle Length Imbalances
In order to address research question 1a-d, paired samples T-tests were conducted to compare the length of each muscle for the dominant and non-dominant sides. There was no significant difference between the dominant and non-dominant sides for the iliopsoas
(p=0.09), rectus femoris (p=0.21), and the quadratus lumborum (p=0.07). However, 11 out of the 13 gymnasts exhibited a shorter iliopsoas on the dominant side. Additionally, eight out of 13 gymnasts exhibited a shorter rectus femoris and quadratus lumborum on their dominant side. There was a significant difference between the dominant and non-dominant sides for the hamstrings (p=0.001), for which 11 of the 13 exhibited more length on their dominant side. These results are summarized in Table 3.
Nine of the 13 gymnasts experienced back pain, which ranged from as little as 4% to 40% impairment across this sample. The Modified Oswestry Disability Index considers 0-20% scores as minimal disability and 20-40% as moderate disability. Four gymnasts were in the minimal disability range and five were in the moderate disability range. Pearson
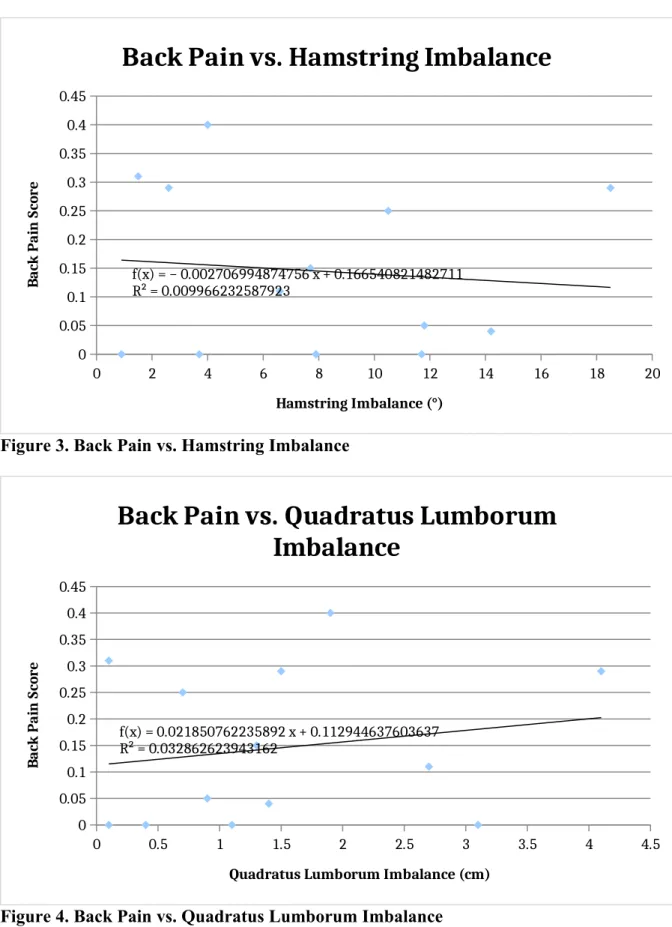
correlations were conducted between the difference in length for each of the muscles and the back pain score to address research question 2a-d. The results of this analysis are listed in Table 4 along with graphs of the back pain score versus each muscle imbalance. There was not a significant relationship between the back pain score and muscle imbalance for the iliopsoas (p=0.14), hamstring (p=0.76), or quadratus lumborum (p=0.56) (Figure 1, 3, 4). There was a significant linear relationship between the rectus femoris imbalance and the degree of back pain (p=0.001) (Figure 2).
Spinal Curvature and Muscle Length Imbalances
Of the 13 gymnasts studied, five had curves of over 10° and according to the
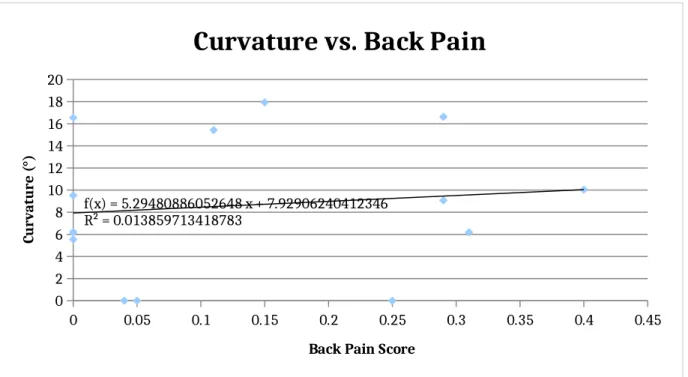
Finally, the direction of the curve, if any, was compared to the side twisted to for each gymnast. Four gymnasts twisted to the right, two of which had lumbar curves to the left, one had a thoracic curve to the left, and one had zero curvature. Nine gymnasts twisted to the left, five of which had thoracic curves to the right, one had a thoracic curve to the left, one had a lumbar curve to the left, and two had zero curvature. There was no significant relationship between the amount of back pain and the degree of curvature (R=0.110; p=0.72) (Figure 9).
Table 1. Subject Characteristics
Age (years) 20.23 ± 1.59 Height (inches) 62.31 ± 2.02 Weight (lbs) 122.54 ± 10.93 Training Time
(years)
15.15 ± 2.88
Table 2. Average Muscle Lengths
Muscle Dominant Side Non-Dominant Side
Iliopsoas (°) 29.25±10.55 33.25±7.01
Rectus Femoris (°) -4.05±7.45 -1.74±9.50
Hamstrings (°) 58.46±11.75 51.28±12.07
Quadratus Lumborum (cm) 20.72±4.63 21.62±4.08
Table 3. Paired Samples T Test Results (n=13) Muscle (dominant vs.
non-dominant) Mean± SD Standard Error ofthe Mean Sig (2-tailed)
Iliopsoas (°) 4.00±7.93 2.20 0.094
Rectus Femoris (°) 2.23±6.31 1.75 0.210
Hamstrings (°) 7.18±6.24 1.73 0.001
Quadratus Lumborum (cm)
0.908±1.67 0.463 0.074
Table 4. Pearson Correlations: Back Pain (n=13) Muscle Imbalance & Back
Pain Score
Correlation Sig (2-tailed)
Iliopsoas -0.436 0.136
Rectus Femoris 0.797 0.001
Hamstrings -0.095 0.758
Quadratus Lumborum 0.179 0.559
Table 5. Pearson Correlations: Curvatures (n=13) Muscle Imbalance &
Curvature
Correlation Sig (2-tailed)
Iliopsoas 0.151 0.792
Rectus Femoris 0.142 0.645
Hamstrings -0.191 0.532
0 1 2 3 4 5 6 7 8 0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4 0.45
f(x) = − 0.027322056290844 x + 0.250259277608701 R² = 0.19415642995905
Back Pain vs. Iliopsoas Imbalance
Iliopsoas Imbalance (°)
B ac k P ai n S co re
Figure 1. Back Pain vs. Iliopsoas Imbalance
0 2 4 6 8 10 12 14 16 18
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4 0.45
f(x) = 0.02636471064893 x + 0.014575089472618 R² = 0.631631944665574
Back Pain vs. Rectus Femoris Imbalance
Rectus Femoris Imbalance (°)
B ac k P ai n S co re
0 2 4 6 8 10 12 14 16 18 20 0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4 0.45
f(x) = − 0.002706994874756 x + 0.166540821482711 R² = 0.009966232587923
Back Pain vs. Hamstring Imbalance
Hamstring Imbalance (°)
B ac k P ai n S co re
Figure 3. Back Pain vs. Hamstring Imbalance
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4 0.45
f(x) = 0.021850762235892 x + 0.112944637603637 R² = 0.032862623943162
Back Pain vs. Quadratus Lumborum
Imbalance
Quadratus Lumborum Imbalance (cm)
B ac k P ai n S co re
0 1 2 3 4 5 6 7 8 0 2 4 6 8 10 12 14 16 18 20
f(x) = 0.239723854011843 x + 7.77867536036992 R² = 0.00738926417017
Curvature vs. Iliopsoas Imbalance
Iliopsoas Imbalance (°)
Cu rv at u re ( °)
Figure 5. Curvature vs. Iliopsoas Imbalance
0 2 4 6 8 10 12 14 16 18
0 2 4 6 8 10 12 14 16 18 20
f(x) = 0.214349550948747 x + 7.63534261260045 R² = 0.020640342522884
Curvature vs. Rectus Femoris Imbalance
Rectus Femoris Imbalance (°)
Cr u va tu re ( °)
0 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20
f(x) = − 0.233680317440265 x + 10.525147711687 R² = 0.036715893007071
Curvature vs. Hamstring Imbalance
Hamstring Imbalance (°)
Cu rv at u re ( °)
Figure 7. Curvature vs. Hamstring Imbalance
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
0 2 4 6 8 10 12 14 16 18 20
f(x) = 3.6703396630115 x + 3.24980342337523 R² = 0.458390115895453
Curvature vs. Quadratus Lumborum
Imbalance
Quadratus Lumborum Imbalance (cm)
Cu rv at u re ( °)
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4 0.45 0
2 4 6 8 10 12 14 16 18 20
f(x) = 5.29480886052648 x + 7.92906240412346 R² = 0.013859713418783
Curvature vs. Back Pain
Back Pain Score
Cu
rv
at
u
re
(
°)
Chapter V: Discussion
Muscle Lengths
For all four of the muscle lengths measured in this study, the results were what were expected due to the biomechanical nature of the sport. All except for two of the gymnasts had a shorter iliopsoas on their dominant side. Also, eight of the thirteen gymnasts exhibited a shorter rectus femoris on their dominant side. With one exception, all of the gymnasts had either a short iliopsoas or a short rectus femoris on their dominant side and some had shorter lengths for both muscles. This supports the hypothesis that the repeated hip flexion of the dominant/lead leg during split leaps may cause a shortening in both the iliopsoas and the rectus femoris. Meanwhile, the simultaneous hip extension of the non-dominant leg in the split leaps may cause a lengthening of the rectus femoris and iliopsoas. In the same regard, eleven of the thirteen gymnasts had longer hamstrings on their dominant side. This is also in support of the hypothesis that the repeated hip extension of the non-dominant leg during split leaps would result in a shortening over time while the hamstring of the dominant leg
lengthens. Eight of the thirteen gymnasts exhibited a shorter quadratus lumborum on their dominant side, which supports the hypothesis that repeated twisting to one side would result in a shortening over time. It is not possible to know from this study whether the lengthening of one side and the shortening of the other are occurring independently or in combination. However, in the trunk musculature it is more likely that only the dominant quadratus
to the fact that during a twist, the non-dominant quadratus lumborum is not stretched significantly.
Despite the similar heights and weights of the gymnasts, there was large variability in their muscle lengths. Genetics play a major role in the determination of muscle fiber ratios and fiber size [27]. However, research has supported that training can alter not only fiber size, but also fiber type proportions [28]. Unfortunately, there is minimal literature regarding the determination of genetic influence versus training on muscle length. More research is necessary in this area to explore why so much variability exists in populations of athletes of similar height, weight, and activity level.
Muscle Length Imbalances and Back Pain
cartilage [29]. For young athletes, arthritis can be a debilitating chronic injury that negatively affects their quality of life for years after the end of their sports career [30].
The only statistically significant correlation found with the degree of back pain was with the amount of rectus femoris imbalance. However, there are some potential reasons for why the imbalances in the other muscles tested were not related to back pain. Overall, there were few subjects that had large imbalances in both the rectus femoris and the iliopsoas. Seeing as these muscles are synergistic in performing hip flexion, it makes sense that there would not be large discrepancies in both muscles. This is evident in the fact that 12 of the 13 subjects had either a short iliopsoas or a short rectus femoris in their dominant leg. The iliopsoas actually had a greater difference between sides (4.00°±7.93°) than the rectus femoris (2.23°±6.31°), but only the rectus femoris imbalance was statistically correlated with back pain. Perhaps the amount of the imbalance is not as important as just the existence of some degree of imbalance. We would assume that a greater imbalance would result in more anterior pelvic tilt and therefore even more back pain. However, it may be possible that once enough of a pelvic tilt is present, back pain occurs and the degree of that pain becomes more of an individual factor.
Despite a statistically significant imbalance of the hamstrings, there was no correlation found between the amount of imbalance and the degree of back pain. The
pelvic tilt, they are not the sole determining factor. There needs to be an imbalance between the lengths of the rectus femoris and/or the iliopsoas and the hamstrings in order for the tilt to occur. Seeing as the anterior pelvic tilt is the most probable cause of back pain, an imbalance in the hamstrings may not be the primary issue when it comes to the development of this tilt. With that said, it is also possible that the sample size for this study may have been too small to establish a relationship between hamstring length imbalance and back pain.
There was no statistically significant relationship found between the imbalance in the quadratus lumborum and back pain or the degree of spinal curvature and back pain.
Potentially, the anterior pelvic tilt is the main factor when determining the amount of back pain. However, a curve in the spine could increase facet joint pressure and friction, especially when combined with the twisting and back extension movements that gymnasts perform routinely. It is possible that the sample size was too small to see any correlation between these factors. With that said, a curvature in the spine does not always coincide with back pain. If the curve were in a position in which the vertebrae were not loaded, pain would not occur. There were four gymnasts that had curvature but no back pain. There was no pattern in this sample for the type or amount of curvature that was not related to back pain. The degrees of curvature for these four subjects ranged from 5.55° to 16.62° and there were two thoracic, one lumbar, and one ‘S’ shaped curve.
across a sample because the answers to the survey rely on the individual’s perception of pain and their definitions of key words (i.e. ‘some pain’, ‘heavy weights’, ‘moderate vs. severe’, etc.). Unfortunately, there is no clear way to ameliorate this issue in survey research,
especially when only obtaining scores at one point in time. The Oswestry Disability Index is best suited for tracking an individual’s impairment due to pain over a period of time.
However, for this study it was the best-known survey to obtain a general gauge of the degree of each subject’s back pain.
Muscle Length Imbalances and Spinal Curvature
The results revealed a correlation between the amount of imbalance in the quadratus lumborum and the degree of curvature in the spine. The quadratus lumborum originates on the posterior third of the iliac crest and inserts on the transverse processes of the L1-L4 vertebrae and the 12th rib. When the QL is shortened on one side, the lumbar vertebrae are pulled in the ipsilateral direction creating a lateral curve in the spine. These curvatures have become so extreme in some cases that they can be considered scoliotic. Therefore, despite the lack of a statistical difference between the dominant and non-dominant sides of the quadratus lumborum, there is clear clinical significance in relation to the development of spinal
curvature.
lumborum is shorter on one side the vertebrae are pulled closer to the iliac crest, creating a curve in the lumbar portion of the spine. There was a statistically significant correlation found between the amount of quadratus lumborum imbalance and the amount of curvature. If an ‘S’ shaped curve was present, the lumbar angle was used in the analysis.
However, with such a high percentage of gymnasts exhibiting a thoracic curve, it is hard to make sense of how a quadratus lumborum imbalance could be playing a role in the development of this curvature. Perhaps the obliques are more of a contributing factor in the rotation movements so often performed by the gymnasts. The internal obliques are synergists with the quadratus lumborum in performing lateral trunk flexion. Therefore, an imbalance in the internal obliques could be altering the quadratus lumborum measurements. It is also possible that there is an imbalance in the obliques that could be contributing to the amount of curvature present in the gymnasts. The internal obliques originate on the iliac crest and inguinal ligament and attach onto ribs 10-12 and the linea alba. Therefore, a shortening of the internal oblique on the dominant side could be contributing to spinal curvature by bringing the ribs closer to the iliac crest. Another factor that would be interesting to measure is the amount of rotation of the ribs. Rib rotation could be playing a role in creating the thoracic curvatures of the spine. Since the DXA scan is a 2D image, it was not possible to measure the amount of rib rotation in this study.
amount of hip and leg imbalances were not correlated with the amount curvature due to the fact that they are sagittal plane movers. Unlike the quadratus lumborum, the rectus femoris, iliopsoas, and hamstrings do not create any lateral forces that would pull the spine to one side over time.
The statistical analysis only revealed a correlation between the amount of quadratus lumborum imbalance and the amount of curvature. Therefore, it is unclear as to which is the cause of the other. Due to the tremendous length of time the gymnasts have been training, it would follow that the repeated movement patterns cause the biomechanical imbalances, which then creates the curvatures. Additionally, the high incidence of scoliosis in this sample (38%) compared to 2-3% in the normal population suggests that the nature of the sport is responsible for these changes.
Sample Size
A potential reason for only approaching statistical significance for an imbalance in the iliopsoas and the quadratus lumborum is that the sample size of 13 was too small. A larger number of participants is needed in order to make such small differences in a
population apparent. Due to the larger imbalance between the dominant and non-dominant hamstrings, the sample size was sufficient to distinguish this difference as statistically significant. However, for the other muscles, the imbalances were not as sizeable and
0.8) to find any statistically significant imbalances in the iliopsoas. The power for the imbalance in the rectus femoris was 0.230 and the power for the imbalance in the quadratus lumborum was 0.428, meaning at least 45 gymnasts would be needed to get a strong enough power to compare all variables.
Future Research
First, this study could be repeated with a larger sample in order to increase the power and potentially draw more concrete conclusions. Also, due to the large number of curvatures in the thoracic region of the spine, it would be insightful to measure the amount of rib rotation. While it is never good to unnecessarily expose individuals to radiation, X-rays would be necessary to measure rib rotation since this is not possible on the DXA scans. Finally, it would be interesting to include a measurement of the obliques, however there is not a good measurement tool available at this time.
they are able to return to a normal amount of imbalance. This amount of imbalance would most likely be minimal, although there is no data in the literature to support this idea.
Conclusions
It is evident from these findings that there is a statistically significant difference in the length of the dominant and non-dominant hamstrings in collegiate female gymnasts. Also, despite having no statistically significant imbalance in the rectus femoris or the quadratus lumborum, these imbalances are clinically significant. The correlation between the amount of back pain and the amount of rectus femoris imbalance supports the hypothesis that an
anterior pelvic tilt is to blame for back pain. Also, the correlation between the amount of spinal curvature and the amount of quadratus lumborum imbalance supports the hypothesis that a shortened quadratus lumborum on the dominant side creates a curve in the opposite direction. There was no relation between back pain and spinal curvature, which pulls in to question the importance of the quadratus lumborum imbalance. However, scoliosis can have negative effects on one’s quality of life with pain being caused by the curve itself or
Appendix A
Modified Oswestry Disability Index
SECTION 1-PAIN INTENSITY
☐ The pain comes and goes and is very mild. ☐ The pain is mild and does not vary much. ☐ The pain comes and goes and is moderate. ☐ The pain is moderate and does not vary much. ☐ The pain comes and goes and is very severe. ☐ The pain is severe and does not vary much.
SECTION 2-PERSONAL CARE
☐ I would not have to change my way of washing or dressing in order to avoid pain.
☐ I do not normally change my way of washing or dressing even though it causes some pain. ☐ Washing and dressing increases the pain, but I manage not to change my way of doing it. ☐ Washing and dressing increases the pain and I find it necessary to change my way of doing it. ☐ Because of the pain, I am unable to do some washing and dressing without help.
☐ Because of the pain, I am unable to do any washing and dressing without help.
SECTION 3-LIFTING
☐ I can lift heavy weights without extra pain. ☐ I can lift heavy weights, but it causes extra pain.
☐ Pain prevents me from lifting heavy weights off the floor, but I manage if they are conveniently positioned (e.g., on a table).
☐ Pain prevents me from lifting heavy weights off the floor.
☐ Pain prevents me from lifting heavy weights, but I can manage light to medium weights if they are conveniently positioned.
☐ I can only lift very light weights at the most.
SECTION 4-WALKING ☐ I have no pain on walking.
☐ I have some pain on walking, but it does not increase with distance. ☐ I cannot walk more than one mile without increasing pain.
☐ I cannot walk at all without increasing pain.
SECTION 5-SITTING
☐ I can sit in any chair as long as I like.
☐ I can only sit in my favorite chair as long as I like. ☐ Pain prevents me from sitting more than one hour. ☐ Pain prevents me from sitting more than 1/2 hour. ☐ Pain prevents me from sitting more 10 minutes. ☐ I avoid sitting because it increases pain right away.
SECTION 6-STANDING
☐ I can stand as long as I want without pain.
☐ I have some pain on standing, but it does not increase with time. ☐ I cannot stand for longer than one hour without increasing pain. ☐ I cannot stand for longer than 1/2 hour without increasing pain. ☐ I cannot stand for longer than 10 minutes without increasing pain. ☐ I avoid standing because it increases the pain right away.
SECTION 7-SLEEPING ☐ I get no pain in bed.
☐ I get pain in bed, but it does not prevent me from sleeping well. ☐ Because of pain, my normal night’s sleep is reduced by less than 1/4. ☐ Because of pain, my normal night’s sleep is reduced by less than 1/2. ☐ Because of pain, my normal night’s sleep is reduced by less than 3/4. ☐ Pain prevents me from sleeping at all.
SECTION 8-SOCIAL LIFE
☐ My social life is normal and gives me no pain.
☐ My social life is normal, but increases the degree of pain.
☐ Pain has no significant effect on my social life apart from limiting my more energetic interests
☐ Pain has restricted my social life and I do not go out very often. ☐ Pain has restricted my social life to my home.
☐ I have hardly any social life because of the pain.
SECTION 9-TRAVELLING ☐ I get no pain while travelling.
☐ I get extra pain while travelling, which compels me to seek alternative forms of travel. ☐ Pain restricts all forms of travel.
☐ Pain prevents all forms of travel except that done lying down.
SECTION 10-CHANGING DEGREE OF PAIN ☐ My pain is rapidly getting better.
☐ My pain fluctuates, but is definitively getting better.
☐ My pain seems to be getting better, but improvement is slow at present. ☐ My pain is neither getting better nor worse.
☐ My pain is gradually worsening. ☐ My pain is rapidly worsening.
SECTION 11-GYMNASTICS PARTICIPATION
☐ I have no pain when doing gymnastics.
☐ I have pain with one skill and then it goes away.
☐ I have pain with one skill and it persists.
☐I have pain with multiple skills and it goes away.
☐ I have pain with multiple skills and it persists.
☐ I have changed my routine because I can no longer perform a skill due to pain.
References
1. School's That Sponsor Women's Gymnastics. 2014 [cited 2014 November 11]; Available from: https://usagym.org/pages/home/college/womeninfo.html.
2. Sports, Fitness, and Leisure Activities Topline Participation Report. 2013, The Sports and Fitness Industry Association: Silver Spring, Maryland. p. 1-28.
3. Caine, D.J. and L. Nassar, Gymnastics injuries. Med Sport Sci, 2005. 48: p. 18-58. 4. Marshall, S.W., et al., Descriptive epidemiology of collegiate women's gymnastics injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. J Athl Train, 2007. 42(2): p. 234-40.
5. Sands, W.A., B.B. Shultz, and A.P. Newman, Women's gymnastics injuries. A 5-year study. Am J Sports Med, 1993. 21(2): p. 271-6.
6. Knapik, J.J., et al., Preseason strength and flexibility imbalances associated with athletic injuries in female collegiate athletes. Am J Sports Med, 1991. 19(1): p. 76-81.
8. Nadler, S.F., et al., Relationship between hip muscle imbalance and ocurrence of low back pain in collegiate athletes: a prospective study. American Journal of Physical Medicine & Rehabilitation, 2001. 80(8): p. 572-577.
9. Modi, H., et al., Muscle imbalance in volleyball players initiates scoliosis in immature spines: a screening analysis. Asian Spine J, 2008. 2(1): p. 38-43.
10. Keene, J.S., et al., Back injuries in college athletes. J Spinal Disord, 1989. 2(3): p. 190-5.
11. Dick, R., J. Agel, and S.W. Marshall, National Collegiate Athletic Association Injury Surveillance System commentaries: introduction and methods. J Athl Train, 2007. 42(2): p. 173-82.
12. Bono, C.M., Low-back pain in athletes. J Bone Joint Surg Am, 2004. 86-a(2): p. 382-96.
13. Ohlen, G., T. Wredmark, and E. Spangfort, Spinal sagittal configuration and mobility related to low-back pain in the female gymnast. Spine (Phila Pa 1976), 1989. 14(8): p. 847-50.
14. Nadler, S.F., et al., The relationship between lower extremity injury, low back pain, and hip muscle strength in male and female collegiate athletes. Clinical Journal of Sport Medicine, 2000. 10(2): p. 89-97.
15. Kirby, R.L., et al., Flexibility and musculoskeletal symptomatology in female gymnasts and age-matched controls. Am J Sports Med, 1981. 9(3): p. 160-4.
16. Nadler, S.F., et al., Low back pain in college athletes. A prospective study correlating lower extremity overuse or acquired ligamentous laxity with low back pain. Spine (Phila Pa 1976), 1998. 23(7): p. 828-33.
17. Kums, T., et al., Spinal curvature and trunk muscle tone in rhythmic gymnasts and untrained girls. Journal of Back and Musculoskeletal Rehabilitation, 2007. 20(2-3): p. 87-95.
18. Reeves, N.P., J. Cholewicki, and S.P. Silfies, Muscle activation imbalance and low-back injury in varsity athletes. J Electromyogr Kinesiol, 2006. 16(3): p. 264-72. 19. Arab, A.M. and M.R. Nourbakhsh, The relationship between hip abductor muscle
strength and iliotibial band tightness in individuals with low back pain. Chiropr Osteopat, 2010. 18: p. 1.
21. Kendall, F.P.M., Elizabeth Kendall; Provance, Patricia Geise, Muscles: Testing and Function. 4th ed. 1993, Baltimore, MD: Williams & Wilkins.
22. Salamh, P.A. and M. Kolber, The reliability, minimal detectable change and
concurrent validity of a gravity-based bubble inclinometer and iphone application for measuring standing lumbar lordosis. Physiother Theory Pract, 2014. 30(1): p. 62-7. 23. Taylor, H.J., et al., Identifying scoliosis in population-based cohorts: development
and validation of a novel method based on total-body dual-energy x-ray absorptiometric scans. Calcif Tissue Int, 2013. 92(6): p. 539-47.
24. Corkery, M., Briscoe, H., Ciccone, N., Foglia, G., Johnson, P., Kinsman, S., Legere, L., Lum, B., Canavan, P.K., Establishing normal values for lower extremity muscle length in college-aged students. Physical Therapy in Sport, 2007. 8: p. 66-74. 25. Waddell, G., et al., Objective clinical evaluation of physical impairment in chronic
low back pain. Spine (Phila Pa 1976), 1992. 17(6): p. 617-28.
26. Ferguson, A., The study and treatment of scoliosis. Southern Medical Journal, 1930. 23(2): p. 116-120.
27. Tesch, P.A. and J. Karlsson, Muscle fiber types and size in trained and untrained muscles of elite athletes. J Appl Physiol (1985), 1985. 59(6): p. 1716-20.
28. Simoneau, J.A., et al., Human skeletal muscle fiber type alteration with high-intensity intermittent training. Eur J Appl Physiol Occup Physiol, 1985. 54(3): p. 250-3. 29. Ray, C.D. Causes of Osteoarthritis and Spinal Arthritis. 2005 [cited 2015 April 8];
Available from: http://www.spine-health.com/conditions/arthritis/causes-osteoarthritis-and-spinal-arthritis.
![Figure 1: Thomas test resting position [20] Figure 2: Participant position for measurement [20]](https://thumb-us.123doks.com/thumbv2/123dok_us/8331159.2210087/29.918.136.445.525.819/figure-thomas-resting-position-figure-participant-position-measurement.webp)
![Figure 3: Modified Thomas test resting position [20]](https://thumb-us.123doks.com/thumbv2/123dok_us/8331159.2210087/30.918.137.787.574.857/figure-modified-thomas-test-resting-position.webp)
![Figure 5: Resting position for straight leg raise test [20]](https://thumb-us.123doks.com/thumbv2/123dok_us/8331159.2210087/31.918.141.810.442.688/figure-resting-position-straight-leg-raise-test.webp)
![Figure 7: Starting and ending positions for the quadratus lumborum muscle length test [25]](https://thumb-us.123doks.com/thumbv2/123dok_us/8331159.2210087/32.918.151.429.445.776/figure-starting-ending-positions-quadratus-lumborum-muscle-length.webp)