Acknowledgements:
Abstract
Background: Patient preferences are important to consider in the decision-making process for colorectal cancer (CRC) screening. Vulnerable populations, especially, exhibit lower screening uptake. This systematic review describes studies on vulnerable populations’ preferences
regarding CRC screening.
Methods: We searched the PubMed, CINAHL, PsychInfo, Scopus, and Web of Science databases for articles published between January 1, 1996 to December 31, 2017. We screened studies for eligibility and using a standardized spreadsheet, abstracted and compared study designs and outcomes.
Results: A total of 44 articles were selected and are organized by the types of vulnerable population(s) whose preferences are reported. Of these studies, 17 report on preferences among racial/ethnic minorities, 11 among multiracial/multiethnic minorities, 7 among low-income groups, 6 among veterans, 2 among rural residents, and 1 among immigrants.
Introduction
Colorectal cancer (CRC) is the third most common type of cancer in the United States and the second leading cause of cancer deaths. In 2017, there were an estimated 135,430 new cases diagnosed (95,520 cases of colon cancer and 39,910 cases of rectal cancer) and an
estimated 50,260 CRC-specific deaths.1 CRC is expected to cost the U.S. healthcare system $14 billion per year.2 Screening has been shown to reduce the incidence and mortality of CRC by 30-60% and has the potential to save an estimated 18,800 lives per year.3,4 CRC screening is
imperative for early detection and appropriate treatment, especially since early stage CRC is asymptomatic.5 The US Preventive Services Task Force (USPSTF) has recommended CRC screening using colonoscopy, fecal occult blood testing (FOBT), or sigmoidoscopy for adults age 50 to 75 years.6 The recommended time interval between screenings depends on the modality used (e.g. colonoscopy every ten years, sigmoidoscopy every five years, FOBT annually). Of these, colonoscopy and FOBT are the most common.7
The U.S. has recently seen an increase in CRC screening, yet the 2015 national rate of 62.6% is well below the Healthy People 2020 target of 70.5% set by the U.S. Department of Health and Human Services.8,9 The national rate is also lower than breast and cervical cancer screening rates (72% and 81% respectively).8 CRC screening is even lower in many vulnerable sub-populations. Patients who are racial and ethnic minorities, foreign born, low-income, are publicly insured or uninsured, and live in rural areas are at greater risk of not being screened.10-15
optimal option, has been increasingly advocated for screening and other types of preventive care.18 There are multiple options for CRC screening modality that present unique combinations of test characteristics, such as accuracy, invasiveness, and comfort.19 Individuals weigh these characteristics in deciding their preference for CRC screening. For example, some patients may prefer FOBT, due to its non-invasive nature, and are more likely to engage in screening when presented with the choice of this option. Presenting choices of screenings that match with individuals’ preferences may increase CRC screening uptake.
Systematic reviews have assessed preferences of CRC screening within the general population.20-22 These reviews reported that the general population values accuracy and clinical effectiveness but did not exhibit an overwhelming preference for a modality. However, screening rates are lower among vulnerable patients and there is significant evidence that vulnerable
patient populations face increased barriers to preventive care.23-27 Given these unique barriers, preferences may differ between the general population and underserved patients. Thus, an understanding of preferences, specifically among underserved patient populations is critical to increasing their screening rates. To our knowledge, this is the first systematic review to address CRC screening preferences among vulnerable populations.
Problem Statement
CRC mortality rates have started to decline, largely due to improved screening rates, but many people have yet to be screened. Vulnerable populations’ preferences concerning CRC screening practices, including screening modality, test features, decision making, and methods of communication about screening options, and provides insight into how to best target
interventions aimed at improving screening rates among vulnerable populations.
Inclusion/Exclusion Criteria
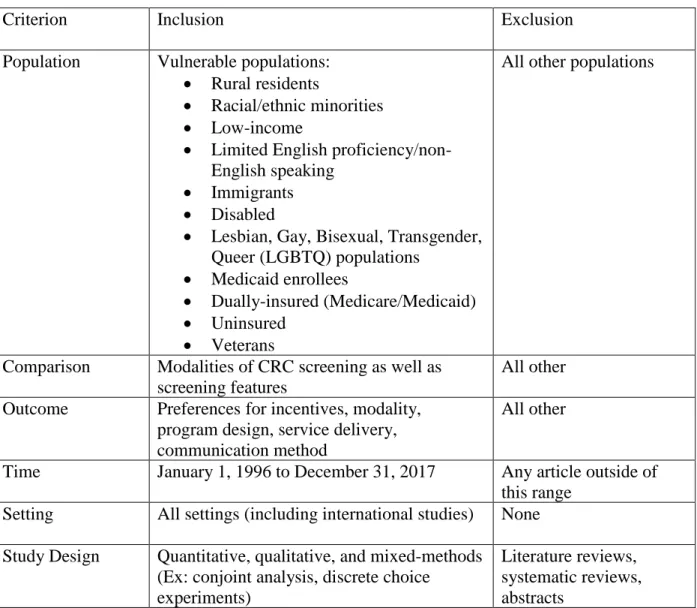
We conducted a systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.28 Studies eligible for review met specific criteria outlined below in Table 1.
Table 1: Inclusion/Exclusion criteria
Criterion Inclusion Exclusion
Population Vulnerable populations: • Rural residents
• Racial/ethnic minorities • Low-income
• Limited English proficiency/non-English speaking
• Immigrants • Disabled
• Lesbian, Gay, Bisexual, Transgender, Queer (LGBTQ) populations
• Medicaid enrollees
• Dually-insured (Medicare/Medicaid) • Uninsured
• Veterans
All other populations
Comparison Modalities of CRC screening as well as screening features
All other Outcome Preferences for incentives, modality,
program design, service delivery, communication method
All other
Time January 1, 1996 to December 31, 2017 Any article outside of this range
Setting All settings (including international studies) None Study Design Quantitative, qualitative, and mixed-methods
(Ex: conjoint analysis, discrete choice experiments)
Literature reviews, systematic reviews, abstracts
Search Strategy
timeframe because the USPSTF released its first guidelines on CRC screening in December 1995.29 The following search string was used to search for relevant articles:
((“colorectal” AND “cancer” OR “colon” AND “cancer”) AND (“screening” OR “detection” OR “testing” OR “test”) AND ((“preference” OR “preferences” OR “perception” OR “perceptions”) OR (“discrete” AND “choice”) OR (discrete AND choices))) AND PUBYEAR > 1995
The specific vulnerable populations identified in the inclusion criteria were not included in this search string. While our focus was on underserved populations, we did not exclude studies outright if they were not specifically about vulnerable populations. Instead, we included the studies that contained subgroup analyses regarding screening preferences for one or more vulnerable populations and excluded those without a subgroup analysis.
In total, 4,269 articles were found and imported into F1000, a reference manager, where articles were de-duplicated. The remaining 2,153 articles were then transferred to Covidence and then further deduplicated, leaving 2,106 articles to be screened.
Using Covidence, two reviewers independently screened the study titles and abstracts according to the predetermined inclusion/exclusion criteria. The two reviewers started with a small pool of 20 articles to ensure consistency and to further refine the inclusion/exclusion criteria. Following the title and abstract screening process, the two reviewers resolved
discrepancies in their ratings. If a consensus could not be reached, a third reader made the final decision. The two reviewers then engaged in a full-text review of the remaining 154 articles to assess whether each article should be included or excluded and to categorize the excluded
articles by reason of exclusion. Discrepancies regarding whether the article should be included or excluded, as well as the reason for exclusion, were resolved by the two reviewers with the third reader making the final decision about any remaining discrepancies.
The two reviewers abstracted the data from the remaining articles into a literature matrix using Microsoft Excel 2010. The literature matrix included fields such as title, sample size, study design, vulnerable population studied, baseline population characteristics, outcome measure, and risk of bias.
Results
these categories are not necessarily mutually exclusive. For example, studies often included racial or ethnic minorities as well as low-income individuals. For this analysis, studies were categorized based on the vulnerable population prioritized during sampling and in the analysis.
The multiracial/multiethnic minorities category was created because some studies did not focus on or have an overwhelming majority of participants from a single racial group. Other studies focused on assessing the preferences of a specific racial group or had a large portion of a racial group in their study population due to their sampling.
Grouping by outcomes and study design were considered but categorizing by vulnerable population will best assist public health officials designing interventions for these underserved populations. Most of the selected articles dealt with preferences in terms of modality and testing attributes.
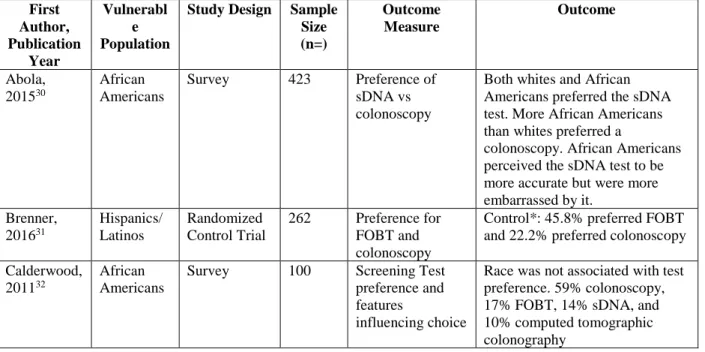
Racial/Ethnic Minorities (n=17)
Table 2: Characteristics of Studies with Racial/Ethnic Populations
First Author, Publication
Year
Vulnerabl e Population
Study Design Sample
Size (n=)
Outcome Measure
Outcome
Abola, 201530
African Americans
Survey 423 Preference of sDNA vs colonoscopy
Both whites and African Americans preferred the sDNA test. More African Americans than whites preferred a
colonoscopy. African Americans perceived the sDNA test to be more accurate but were more embarrassed by it.
Brenner, 201631
Hispanics/ Latinos
Randomized Control Trial
262 Preference for FOBT and colonoscopy
Control*: 45.8% preferred FOBT and 22.2% preferred colonoscopy
Calderwood, 201132
African Americans
Survey 100 Screening Test preference and features
influencing choice
Ellison, 201133
African Americans
Survey 395 Preference for source of information
Top four preferred sources of information: doctor/provider, health brochures, television, and from someone who speaks their language. Greiner, 200534 African Americans Focus Group Interviews
55 Preference for FOBT,
sigmoidoscopy, colonoscopy
Following the educational lecture session, 33% of the participants preferred colonoscopy and 26% preferred for FOBT. The rest would go with their doctor’s recommendation Harden, 201135 African Americans Focus Group Interviews
28 Preferences for FOBT and FIT
FIT was preferred because it requires no food restrictions Jo, 200836
Korean-Americans
In-person Interviews
151 Preference for source of information
Educational seminar (42%) was most preferred, followed by Korean media (30%) and print materials (20%). Martens, 201637 Hispanics/ Latinos Discrete Choice Experiment
38 Testing options, travel time, money paid for screening, and the portion of the cost of follow- up care paid out of pocket
Option of 2 or 3 tests was preferred over either colonoscopy or the stool test alone.Cost variables were more important than testing options or travel time
Messina, 200538 African Americans Telephone Survey
2119 Preference for decision making about CRC screening
Black versus white ethnicity was associated with greater odds of preferring to share decision making with the physician. Molokwu,
201739
Hispanics/ Latinos
Survey 780 Decision preferences (collaborative vs. active vs. passive)
The majority preferred a collaborative role (53.3%) compared to a passive (26.4%) or active role (20.3%).
Myers, 200840
Non-white Survey 154 Screening preference for FOBT and colonoscopy
122 exhibited preference for colonoscopy and 32 exhibited preference for FOBT. No racial differences found Palmer, 201041 African Americans In-person Interviews
60 Preference for FOBT, barium enema, flexible sigmoidoscopy, and colonoscopy
Preferred colonoscopy and FOBT over barium enema or flexible sigmoidoscopy Ruffin, 200942 African Americans Focus Groups; Survey
93 Preference for FOBT, flexible sigmoidoscopy, colonoscopy, and double contrast barium enema
More whites than African Americans preferred FOBT, while more African Americans than whites preferred
colonoscopy. African Americans overall preferred colonoscopy, due to viewing it as accurate Schroy, 201143 African Americans Randomized Control Trial
665 Test preferences and decision-making preferences
preferred shared decision-making approach (53%) and 28% preferred a patient-dominant approach
Schroy, 200544
Non-white Survey 3359 Preference of SB-DNA testing, FOBT, and colonoscopy
Non-white: 42.5% prefer SB-DNA, 30.5% prefer FOBT, 27.0% prefer colonoscopy
Schroy, 200745
African Americans
Survey 263 Preference for colonoscopy, FOBT,
sigmoidoscopy, sigmoidoscopy plus FOBT, barium enema, and sDNA
African Americans were more likely to prefer colonoscopy and value test accuracy
Zapatier, 201146
Hispanics/ Latinos
Survey 438 Sex and ethnicity preference for endoscopists
Hispanic women more likely to have preference for sex of endoscopist. Hispanics were more likely to prefer ethnicity of endoscopist
Ten of the seventeen studies focused on preferences among African Americans, four among Hispanics/Latinos, two among non-whites, and one among Korean-Americans. Most observed preferences in terms of modality and testing features and used a variety of outcome measures and study designs. Three articles looked at preference of decision making, two investigated preferred sources of information, and one considered preference for the sex and ethnicity of endoscopists.
Six articles reported colonoscopy as the most preferred modality, two of the articles reported sDNA as the most preferred modality, and two of the articles indicated that FOBT or FIT were the most preferred modality. All six of the articles reporting colonoscopy as the
preferred modality focused on African-Americans. One of the articles on sDNA testing, Abola et al, focused on African-Americans, while the other article on sDNA testing did not specify a racial group in its study population.
valued its accuracy. Martens et al. employed a discrete choice experiment for a Hispanic/Latino population and noted that cost attributes were more important than the testing attributes tested.
Zapatier et al. found that Hispanics overall exhibited a preference for the sex and ethnicity of endoscopist. The two articles that discussed preference for source of information focused on two different racial groups, but both indicated sources in their respective languages. Jo et al found that Korean media was one of the preferred sources of information and Ellison et al reported that someone who spoke the language was a preferred source as well. The three articles that studied preference of decision making indicated a preference for shared decision making and collaborative decision making compared to a passive and patient-dominant approach to decision making.
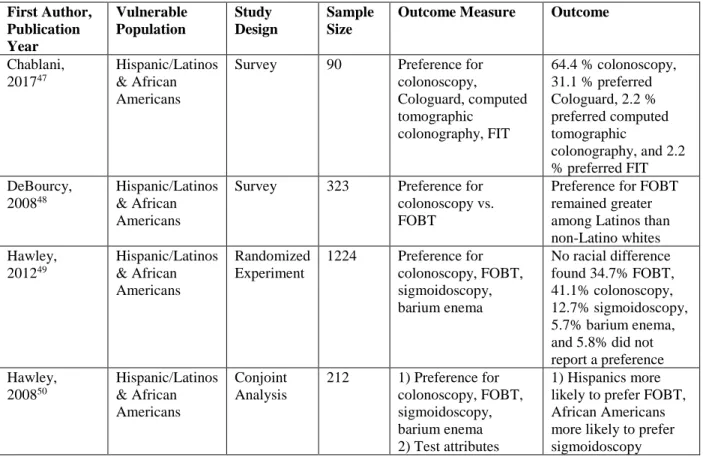
Multiracial/Multiethnic Minorities (n=11)
Table 3: Characteristics of Studies with Multiracial/Multiethnic Populations
First Author, Publication Year Vulnerable Population Study Design Sample Size
Outcome Measure Outcome
Chablani, 201747
Hispanic/Latinos & African Americans
Survey 90 Preference for colonoscopy, Cologuard, computed tomographic
colonography, FIT
64.4 % colonoscopy, 31.1 % preferred Cologuard, 2.2 % preferred computed tomographic
colonography, and 2.2 % preferred FIT DeBourcy,
200848
Hispanic/Latinos & African Americans
Survey 323 Preference for colonoscopy vs. FOBT
Preference for FOBT remained greater among Latinos than non-Latino whites Hawley, 201249 Hispanic/Latinos & African Americans Randomized Experiment
1224 Preference for colonoscopy, FOBT, sigmoidoscopy, barium enema
No racial difference found34.7% FOBT, 41.1% colonoscopy, 12.7% sigmoidoscopy, 5.7% barium enema, and 5.8% did not report a preference Hawley, 200850 Hispanic/Latinos & African Americans Conjoint Analysis
212 1) Preference for colonoscopy, FOBT, sigmoidoscopy, barium enema 2) Test attributes
2) African Americans rated accuracy as most important. More African Americans rated the frequency of test as important compared to other groups
Quick, 201351 Hispanic/Latinos & African Americans
Survey 418 Preference for colonoscopy vs. FIT
Colonoscopy was the most preferred test at baseline when compared to FIT Sheikh, 200452 Hispanic/Latinos
& African Americans
Survey 193 Preference for FOBT, sigmoidoscopy, colonoscopy
Hispanics were more likely to not want screening and preferred
sigmoidoscopy over colonoscopy Shokar, 201053 Hispanic/Latinos
& African Americans
Cognitive ranking tests
168 Preferences of 13 attributes for FOBT, sigmoidoscopy, barium enema, colonoscopy
African Americans ranked accuracy, amount of colon examined, discomfort, and complications as most important. Shokar, 200554 Hispanic/Latinos
& African Americans
In-person Interviews
30 Preference for colonoscopy, FOBT, barium enema, any test, flexible
sigmoidoscopy, none, up to doctor
African Americans (n=10): preference for FOBT (4), barium enema (2),
colonoscopy (1), any test (1), flexible sigmoidoscopy (1), up to doctor (1), none (0). Hispanics (n=10): preference for colonoscopy (3), FOBT (2), any test (2), barium enema (1), flexible sigmoidoscopy (1), none (1), up to doctor (0). Taber, 201455 Hispanic/Latinos
& African Americans
Survey 100 Preference for colonoscopy, sigmoidoscopy, FOBT, and SEPT9 (blood test)
Blacks remained less likely to prefer SEPT9 testing. Unscreened blacks were more likely to prefer colonoscopy Wolf, 200656 Hispanic/Latinos
& African Americans
Survey 216 Preference for FOBT, colonoscopy, or no preference; preference for test features
The majority preferred FOBT over
Wolf, 201657 Hispanic/Latinos & African Americans
Survey 453 Preference for colonoscopy vs. home stool test;
Whites were more likely to express a preference for home stool test (HST) than non-whites
Seven of the selected studies were executed using surveys and every study measured preference in terms of modality and test features and included African Americans and
Hispanic/Latinos in their study populations. Eight of these studies looked at only preference of modality, two of these examined test attributes as well, and one study focused on just test attributes. Five of the eleven studies indicate a preference for colonoscopy, while four of the studies suggested that a certain racial group preferred FOBT. Shokar et al, one of the four studies, exhibited very low sample sizes of African Americans and Hispanic/Latinos. Wolf et al also noted that whites were more likely to prefer home stool tests than non-whites, while Sheikh reported that Hispanics were more likely to prefer sigmoidoscopy. A range of preferences for modality have been uncovered in our findings.
It is difficult to compare studies that investigated test attributes, since each study used different test attributes and different study designs. However, the studies suggest that accuracy, frequency of test, discomfort, and convenience are all important attributes for African Americans and Hispanic/Latinos.
Low-income (n=7)
Table 3: Characteristics of Studies with Low-Income Populations
First Author, Publication Year
Study Design Sampl
e Size
Outcome Measure Outcome
Cho, 201758 Questionnaires 396 Preference for FIT vs. colonoscopy
Participants with higher income levels preferred colonoscopy.
Frew, 200159
Saengow, 201560
In-person Interview
437 Preferences and acceptance of FIT vs. colonoscopy
Low-income was not associated with preference for screening
Waller, 201561
Survey 1964 Preference for expert
recommendation
Low-income was not associated with recommendation preference
Wong, 201062
Survey 3430 Preference for FIT vs. colonoscopy
No statistical differences in choice by monthly household income.
Wong, 201263
Survey 7845 Preference for FIT vs. colonoscopy
Low-income associated with higher odds of changing preference from colonoscopy to FIT after educational session
Xu, 201564 Survey 667 Preference for FIT vs. colonoscopy
As household incomes increased, patients tended to prefer colonoscopy.
Among the seven studies on low-income patient preferences, six were conducted in an international setting. Xu et al. is the only domestic study in this group. Five out of the seven studies focused on preference of FIT vs. colonoscopy, while the other two studies focused on willingness to pay and preference for an expert recommendation. In a willingness to pay study, Frew et al found that low-income patients were less willing to pay for CRC screening as
expected. Waller et al did not find any association between being low-income and preference for expert recommendation. Xu et al, Cho et al, and Wong et al point to a possible relationship between low-income and FIT preference. Wong et al showed that low-income participants were more likely to shift preferences from colonoscopy to FIT after an educational session, while the other two studies found low-income to be associated with FIT preference. However, Saengow et al and Wong et al did not find any association with income and preference. Given that a large proportion of these studies were international, cultural and social contexts may have influenced the results of these studies making it difficult to generalize to underserved populations in the U.S.
Veterans (n=6)
First Author, Publication Year
Study Design Sample Size Outcome Measure Outcome
Akerkar, 200165 Questionnaires 295 Time-tradeoff between virtual colonoscopy and conventional colonoscopy
Willing to wait 4.9 weeks to undergo conventional colonoscopy
Friedemann-Sánchez, 200766
Focus Group Interviews
70 Preference among fecal occult blood test, flexible sigmoidoscopy, colonoscopy
Colonoscopy was preferred over all other screening modalities
Imaeda, 201067 Maximum Differences Scaling tool
92 Preference for test attributes and modalities
Colonoscopy was preferred, and subjects viewed sensitivity of the test, the risk of a perforation and the potential need for a second test as most important. Moawad, 201068 Survey 250 Preference for
colonoscopy vs. Computed tomography colonography
95% of the study population preferred CTC
Powell, 200969 Survey 2068 Preference for FOBT,
sigmoidoscopy, colonoscopy, barium enema (DCBE) or no screening
Preference: colonoscopy (37%), FOBT (29%), no preference (22%), sigmoidoscopy (5%), do not want screening (4%), barium enema (2%)
Rajapaksa, 200770
Survey 272 Preference of
computed tomographic colonography vs. optical
colonoscopy
Proportion of subjects who preferred computed tomographic colonography over optical colonoscopy was not significantly different
Six studies sampled patients exclusively from the Veterans Health Administration (VHA). These studies primarily focused on preferences of modality. Four out of six studies indicated that colonoscopy was the preferred modality for CRC screening among veterans. Rajapaksa et al found that the preference of computed tomographic colonography over
Rural (n=2)
Table 5: Characteristics of Studies with Rural Populations
First Author, Publication Year
Study Design Sample Size Outcome Measure Outcome
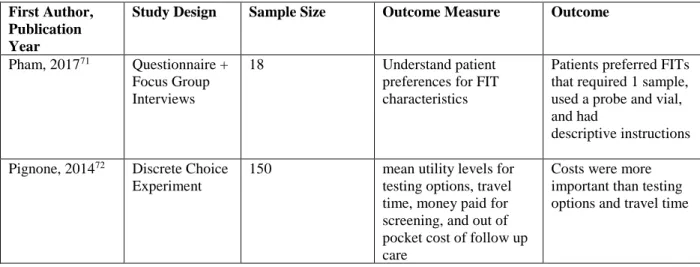
Pham, 201771 Questionnaire + Focus Group Interviews
18 Understand patient preferences for FIT characteristics
Patients preferred FITs that required 1 sample, used a probe and vial, and had
descriptive instructions
Pignone, 201472 Discrete Choice Experiment
150 mean utility levels for testing options, travel time, money paid for screening, and out of pocket cost of follow up care
Costs were more important than testing options and travel time
Two studies focused primarily on rural populations’ preferences for CRC screening. Pham et al studied a rural population that consisted of predominantly Hispanics, but a subgroup analysis to see whether preference varied by race was not conducted. Pham et al suffered from a relatively low sample size (n=18), which would have made it difficult to draw significant statistical inferences on differences in race. Pignone et al sampled from a rural setting as well and included a large percentage of uninsured and low-income individuals.
While focused on rural populations, these two articles varied in methodology and design. Pham et al studied patient preferences for characteristics of fecal immunochemical test (FIT), a specific screening modality using stool samples, while Pignone et al studied preferences for 4 test attributes. Pham et al. showed that the study population enjoyed the convenience of the FIT compared to a colonoscopy, while Pignone et al. showed that the study population favors having the option of stool testing, rather than only colonoscopy.
Immigrants (n=1)
First Author, Publication Year
Study Design
Sample Size Outcome Measure Outcome
Benning, 201473
Discrete Choice Experiment
815 1) Preference among stool, blood, and combi tests 2) How do preferences differ according to sociodemographic characteristics
3) Preference in terms of test attributes
1) Combi tests were preferred
2) Sociodemographic characteristics influence preference
3) Sensitivity, risk reduction, scientific evidence are favorable attributes
Only one article was found with information on immigrants’ preferences of CRC screening. The article was conducted in the Netherlands and collected sociodemographic variables as well as preferences regarding stool, blood, and combination tests (combination of the stool and blood tests). The study found that individuals who are higher educated, born in the Netherlands, younger, and have experienced a colonoscopy are more likely to prefer either screening test than people who are less educated, immigrants, older, and have not experienced a colonoscopy. In general, the study also found that sensitivity, risk reduction of CRC death, and scientific level of evidence were favorable attributes. However, no subgroup analysis was done to elicit whether immigrants had the same preferences in terms of testing attributes.
Discussion
screening.74,75 Many studies, especially those that focused on Hispanic/Latinos, may have captured immigrant populations, but did not record immigrant status. There also have yet to be studies assessing preferences in some of the vulnerable populations that were incorporated in the inclusion criteria.
In terms of outcomes, many studies across vulnerable groups focused on preference for modality, especially contrasting colonoscopy vs. stool tests. Many studies pointed to
colonoscopy as the preferred modality among racial/ethnic minorities and veterans, while low-income populations seemed to prefer stool tests. There was no overwhelming and conclusive evidence on this issue and may require additional focus on information on test attributes to further our understanding on what modality would be the ideal screening option. A handful of studies argued that vulnerable groups in their study populations preferred stool tests. Studies that investigated test attributes tended to find that accuracy, sensitivity, costs, frequency of test, and discomfort were all important attributes to consider. Accuracy and sensitivity were often associated with colonoscopy, while convenience and comfort were often associated with stool tests.
Limitations
The studies selected displayed a wide range of heterogeneity in study design and
outcomes across all studies, making them difficult to compare. In addition, the intersectionality of identities among the vulnerable populations made it difficult to elicit a specific preference for a singular categorization. As a result, generalizations and overarching conclusions on specific vulnerable groups could not be made, due to the variety of factors that are involved in
preferences for colorectal cancer screening. Instead, this review elicited trends and themes from the literature.
Strengths
There were many strengths of this study, including the large number of databases searched over a long study period and this being the first systematic review that addresses the preferences among underserved populations.
Implications and Future Directions
As noted before, the preferences for many traditionally vulnerable groups have yet to be assessed and may be of interest for the future. There may need to be more standardized methods to capture preferences for vulnerable group specifically, such as discrete choice experiments. There have been many discrete choice experiments done for the general population, but few have focused on vulnerable groups. To increase CRC screening overall, special attention must be paid to vulnerable populations that struggle with a lower screening uptake.
The plurality in outcomes, study design, and populations of the selected studies
demonstrate the wide spectrum of preferences of vulnerable populations. This review echoes the results of previous systematic reviews done on preferences for CRC screening of the general population in that there is no specific modality that is overwhelmingly supported by vulnerable populations and that attributes such as accuracy and sensitivity are important features to
consider. Further improvements in the CRC screening rate may be achieved through the alignment of vulnerable populations’ preferences with provider preferences through shared decision making.
Bibliography
. 1. Cancer Facts & Figures 2017. Available at:
https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2017.html.
2. Mariotto AB, Yabroff KR, Shao Y, Feuer EJ, Brown ML. Projections of the cost of cancer care in the United States: 2010-2020. J Natl Cancer Inst 2011;103(2):117-128. doi:10.1093/jnci/djq495.
3. Whitlock EP, Lin JS, Liles E, Beil TL, Fu R. Screening for colorectal cancer: a targeted, updated systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 2008;149(9):638-658.
4. Maciosek MV, Solberg LI, Coffield AB, Edwards NM, Goodman MJ. Colorectal cancer screening: health impact and cost effectiveness. Am J Prev Med 2006;31(1):80-89. doi:10.1016/j.amepre.2006.03.009.
5. Shida H, Ban K, Matsumoto M, et al. Asymptomatic colorectal cancer detected by screening. Dis Colon Rectum 1996;39(10):1130-1135.
6. U.S. Preventive Services Task Force. Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2008;149(9):627-637. 7. Centers for Disease Control and Prevention (CDC). Vital signs: colorectal cancer
screening test use--United States, 2012. MMWR Morb Mortal Wkly Rep 2013;62(44):881-888.
9. Cancer. Cancer | Healthy People 2020. https://www.healthypeople.gov/2020/topics-objectives/topic/cancer/objectives.
10. Goel MS, Wee CC, McCarthy EP, Davis RB, Ngo-Metzger Q, Phillips RS. Racial and ethnic disparities in cancer screening: the importance of foreign birth as a barrier to care. J. Gen. Intern. Med. 2003;18(12):1028-1035.
doi:10.1111/j.1525-1497.2003.20807.x.
11. Jackson CS, Oman M, Patel AM, Vega KJ. Health disparities in colorectal cancer among racial and ethnic minorities in the United States. J. Gastrointest. Oncol. 2016;7(Suppl 1):S32-43. doi:10.3978/j.issn.2078-6891.2015.039.
12. James TM, Greiner KA, Ellerbeck EF, Feng C, Ahluwalia JS. Disparities in colorectal cancer screening: a guideline-based analysis of adherence. Ethn. Dis. 2006;16(1):228-233.
13. Decker KM, Singh H. Reducing inequities in colorectal cancer screening in North America. J. Carcinog. 2014;13:12. doi:10.4103/1477-3163.144576.
14. Liss DT, Baker DW. Understanding current racial/ethnic disparities in colorectal cancer screening in the United States: the contribution of socioeconomic status and access to care. Am. J. Prev. Med. 2014;46(3):228-236. doi:10.1016/j.amepre.2013.10.023. 15. Walsh JME, Posner SF, Perez-Stable EJ. Colon cancer screening in the ambulatory
setting. Prev. Med. 2002;35(3):209-218.
16. Kiviniemi MT, Hay JL, James AS, et al. Decision making about cancer screening: an assessment of the state of the science and a suggested research agenda from the ASPO Behavioral Oncology and Cancer Communication Special Interest Group. Cancer Epidemiol. Biomarkers Prev. 2009;18(11):3133-3137. doi:10.1158/1055-9965.EPI-18-11-ASPO.
17. Nguyen TT, McPhee SJ. Patient-provider communication in cancer screening. J. Gen. Intern. Med. 2003;18(5):402-403.
18. Pignone M, Bucholtz D, Harris R. Patient preferences for colon cancer screening. J. Gen. Intern. Med. 1999;14(7):432-437. doi:10.1046/j.1525-1497.1999.00018.x.
19. Geiger TM, Ricciardi R. Screening options and recommendations for colorectal cancer. Clin. Colon Rectal Surg. 2009;22(4):209-217. doi:10.1055/s-0029-1242460.
20. Wortley S, Wong G, Kieu A, Howard K. Assessing stated preferences for colorectal cancer screening: a critical systematic review of discrete choice experiments. Patient 2014;7(3):271-282. doi:10.1007/s40271-014-0054-3.
21. Ghanouni A, Smith SG, Halligan S, et al. Public preferences for colorectal cancer screening tests: a review of conjoint analysis studies. Expert Rev. Med. Devices 2013;10(4):489-499. doi:10.1586/17434440.2013.811867.
22. Marshall D, McGregor SE, Currie G. Measuring preferences for colorectal cancer screening: what are the implications for moving forward? Patient 2010;3(2):79-89. doi:10.2165/11532250-000000000-00000.
23. Hegarty V, Burchett BM, Gold DT, Cohen HJ. Racial differences in use of cancer prevention services among older Americans. J. Am. Geriatr. Soc. 2000;48(7):735-740. doi:10.1111/j.1532-5415.2000.tb04746.x.
25. Elnicki DM, Morris DK, Shockcor WT. Patient-perceived barriers to preventive health care among indigent, rural Appalachian patients. Arch. Intern. Med. 1995;155(4):421-424. doi:10.1001/archinte.1995.00430040097012.
26. Shi L, Lebrun LA, Zhu J, Tsai J. Cancer screening among racial/ethnic and insurance groups in the United States: a comparison of disparities in 2000 and 2008. J. Health Care Poor Underserved 2011;22(3):945-961. doi:10.1353/hpu.2011.0079.
27. Solberg LI, Brekke ML, Kottke TE. Are physicians less likely to recommend preventive services to low-SES patients? Prev. Med. 1997;26(3):350-357.
doi:10.1006/pmed.1997.0150.
28. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097
29. Levin B, Bond JH. Colorectal cancer screening: Recommendations of the U.S. Preventive Services Task Force. Gastroenterology 1996;111(5):1381-1384.
doi:10.1053/gast.1996.1111381.
30. Abola MV, Fennimore TF, Chen MM, et al. Stool DNA-based versus colonoscopy-based colorectal cancer screening: patient perceptions and preferences. family med commun hlth 2015;3(3):2-8. doi:10.15212/FMCH.2015.0125.
31. Brenner AT, Hoffman R, McWilliams A, et al. Colorectal cancer screening in vulnerable patients: promoting informed and shared decisions. Am. J. Prev. Med. 2016;51(4):454-462. doi:10.1016/j.amepre.2016.03.025.
32. Calderwood AH, Wasan SK, Heeren TC, Schroy PC. Patient and provider preferences for colorectal cancer screening: how does CT colonography compare to other modalities? Int. J. Canc. Prev. 2011;4(4):307-338.
33. Ellison J, Jandorf L, DuHamel K. Colonoscopy screening information preferences among urban hispanics. J. Immigr. Minor. Health 2011;13(5):963-966. doi:10.1007/s10903-010-9368-y.
34. Greiner KA, Born W, Nollen N, Ahluwalia JS. Knowledge and perceptions of colorectal cancer screening among urban African Americans. J. Gen. Intern. Med. 2005;20(11):977-983. doi:10.1111/j.1525-1497.2005.00165.x.
35. Harden E, Moore A, Melvin C. Exploring perceptions of colorectal cancer and fecal immunochemical testing among African Americans in a North Carolina community. Prev. Chronic Dis. 2011;8(6):A134.
36. Jo AM, Maxwell AE, Wong WK, Bastani R. Colorectal cancer screening among underserved Korean Americans in Los Angeles County. J. Immigr. Minor. Health 2008;10(2):119-126. doi:10.1007/s10903-007-9066-6.
37. Martens CE, Crutchfield TM, Laping JL, et al. Why Wait Until Our Community Gets Cancer?: Exploring CRC Screening Barriers and Facilitators in the Spanish-Speaking Community in North Carolina. J. Cancer Educ. 2016;31(4):652-659. doi:10.1007/s13187-015-0890-4.
38. Messina CR, Lane DS, Grimson R. Colorectal cancer screening attitudes and practices preferences for decision making. Am. J. Prev. Med. 2005;28(5):439-446.
doi:10.1016/j.amepre.2005.02.006.
40. Myers RE, Hyslop T, Sifri R, et al. Tailored navigation in colorectal cancer screening. Med. Care 2008;46(9 Suppl 1):S123-31. doi:10.1097/MLR.0b013e31817fdf46. 41. Palmer RC, Midgette LA, Mullan ID. Colorectal cancer screening preferences among
African Americans: which screening test is preferred? J. Cancer Educ. 2010;25(4):577-581. doi:10.1007/s13187-010-0081-2.
42. Ruffin MT, Creswell JW, Jimbo M, Fetters MD. Factors influencing choices for colorectal cancer screening among previously unscreened African and Caucasian Americans: findings from a triangulation mixed methods investigation. J. Community Health 2009;34(2):79-89. doi:10.1007/s10900-008-9133-5.
43. Schroy PC, Emmons K, Peters E, et al. The impact of a novel computer-based decision aid on shared decision making for colorectal cancer screening: a randomized trial. Med. Decis. Making 2011;31(1):93-107. doi:10.1177/0272989X10369007.
44. Schroy PC, Heeren TC. Patient perceptions of stool-based DNA testing for colorectal cancer screening. Am. J. Prev. Med. 2005;28(2):208-214.
doi:10.1016/j.amepre.2004.10.008.
45. Schroy PC, Lal S, Glick JT, Robinson PA, Zamor P, Heeren TC. Patient preferences for colorectal cancer screening: how does stool DNA testing fare? Am. J. Manag. Care 2007;13(7):393-400.
46. Zapatier JA, Kumar AR, Perez A, Guevara R, Schneider A. Preferences for ethnicity and sex of endoscopists in a Hispanic population in the United States. Gastrointest. Endosc. 2011;73(1):89-97, 97.e1. doi:10.1016/j.gie.2010.09.008.
47. Chablani SV, Cohen N, White D, Itzkowitz SH, DuHamel K, Jandorf L. Colorectal Cancer Screening Preferences among Black and Latino Primary Care Patients. J. Immigr. Minor. Health 2017;19(5):1100-1108. doi:10.1007/s10903-016-0453-8.
48. DeBourcy AC, Lichtenberger S, Felton S, Butterfield KT, Ahnen DJ, Denberg TD. Community-based preferences for stool cards versus colonoscopy in colorectal cancer screening. J. Gen. Intern. Med. 2008;23(2):169-174. doi:10.1007/s11606-007-0480-1. 49. Hawley ST, McQueen A, Bartholomew LK, et al. Preferences for colorectal cancer
screening tests and screening test use in a large multispecialty primary care practice. Cancer 2012;118(10):2726-2734. doi:10.1002/cncr.26551.
50. Hawley ST, Volk RJ, Krishnamurthy P, Jibaja-Weiss M, Vernon SW, Kneuper S. Preferences for colorectal cancer screening among racially/ethnically diverse primary care patients. Med. Care 2008;46(9 Suppl 1):S10-6.
doi:10.1097/MLR.0b013e31817d932e.
51. Quick BW, Hester CM, Young KL, Greiner KA. Self-reported barriers to colorectal cancer screening in a racially diverse, low-income study population. J. Community Health 2013;38(2):285-292. doi:10.1007/s10900-012-9612-6.
52. Sheikh RA, Kapre S, Calof OM, Ward C, Raina A. Screening preferences for colorectal cancer: a patient demographic study. South. Med. J. 2004;97(3):224-230.
doi:10.1097/01.SMJ.0000078619.39604.3D.
53. Shokar NK, Carlson CA, Weller SC. Informed decision making changes test preferences for colorectal cancer screening in a diverse population. Ann. Fam. Med. 2010;8(2):141-150. doi:10.1370/afm.1054.
55. Taber JM, Aspinwall LG, Heichman KA, Kinney AY. Preferences for blood-based colon cancer screening differ by race/ethnicity. Am. J. Health Behav. 2014;38(3):351-361. doi:10.5993/AJHB.38.3.4.
56. Wolf RL, Basch CE, Brouse CH, Shmukler C, Shea S. Patient preferences and adherence to colorectal cancer screening in an urban population. Am. J. Public Health
2006;96(5):809-811. doi:10.2105/AJPH.2004.049684.
57. Wolf RL, Basch CE, Zybert P, et al. Patient test preference for colorectal cancer screening and screening uptake in an insured urban minority population. J. Community Health 2016;41(3):502-508. doi:10.1007/s10900-015-0123-0
58. Cho Y-H, Kim DH, Cha JM, et al. Patients’ preferences for primary colorectal cancer screening: A survey of the national colorectal cancer screening program in korea. Gut Liver 2017;11(6):821-827. doi:10.5009/gnl17025.
59. Frew E, Wolstenholme JL, Whynes DK. Willingness-to-pay for colorectal cancer
screening. Eur. J. Cancer 2001;37(14):1746-1751. doi:10.1016/S0959-8049(01)00200-3. 60. Saengow U, Chongsuwiwatvong V, Geater A, Birch S. Preferences and acceptance of
colorectal cancer screening in thailand. Asian Pac. J. Cancer Prev. 2015;16(6):2269-2276. doi:10.7314/APJCP.2015.16.6.2269.
61. Waller J, Macedo A, von Wagner C, et al. Communication about colorectal cancer screening in Britain: public preferences for an expert recommendation. Br. J. Cancer 2012;107(12):1938-1943. doi:10.1038/bjc.2012.512.
62. Wong MCS, Tsoi KKF, Ng SSM, et al. A comparison of the acceptance of
immunochemical faecal occult blood test and colonoscopy in colorectal cancer screening: a prospective study among Chinese. Aliment. Pharmacol. Ther. 2010;32(1):74-82.
doi:10.1111/j.1365-2036.2010.04312.x.
63. Wong MCS, John GK, Hirai HW, et al. Changes in the choice of colorectal cancer screening tests in primary care settings from 7,845 prospectively collected surveys. Cancer Causes Control 2012;23(9):1541-1548. doi:10.1007/s10552-012-0031-x. 64. Xu Y, Levy BT, Daly JM, Bergus GR, Dunkelberg JC. Comparison of patient
preferences for fecal immunochemical test or colonoscopy using the analytic hierarchy process. BMC Health Serv. Res. 2015;15:175. doi:10.1186/s12913-015-0841-0. 65. Akerkar GA, Yee J, Hung R, McQuaid K. Patient experience and preferences toward
colon cancer screening: a comparison of virtual colonoscopy and conventional
colonoscopy. Gastrointest. Endosc. 2001;54(3):310-315. doi:10.1067/mge.2001.117595. 66. Friedemann-Sánchez G, Griffin JM, Partin MR. Gender differences in colorectal cancer
screening barriers and information needs. Health Expect. 2007;10(2):148-160. doi:10.1111/j.1369-7625.2006.00430.x.
67. Imaeda A, Bender D, Fraenkel L. What is most important to patients when deciding about colorectal screening? J. Gen. Intern. Med. 2010;25(7):688-693.
doi:10.1007/s11606-010-1318-9.
68. Moawad FJ, Maydonovitch CL, Cullen PA, Barlow DS, Jenson DW, Cash BD. CT colonography may improve colorectal cancer screening compliance. AJR Am J Roentgenol 2010;195(5):1118-1123. doi:10.2214/AJR.10.4921.
70. Rajapaksa RC, Macari M, Bini EJ. Racial/ethnic differences in patient experiences with and preferences for computed tomography colonography and optical colonoscopy. Clin. Gastroenterol. Hepatol. 2007;5(11):1306-1312. doi:10.1016/j.cgh.2007.05.023.
71. Pham R, Cross S, Fernandez B, et al. “finding the right FIT”: rural patient preferences for fecal immunochemical test (FIT) characteristics. J. Am. Board Fam. Med.
2017;30(5):632-644. doi:10.3122/jabfm.2017.05.170151.
72. Pignone MP, Crutchfield TM, Brown PM, et al. Using a discrete choice experiment to inform the design of programs to promote colon cancer screening for vulnerable populations in North Carolina. BMC Health Serv. Res. 2014;14:611.
doi:10.1186/s12913-014-0611-4.
73. Benning TM, Dellaert BGC, Dirksen CD, Severens JL. Preferences for potential innovations in non-invasive colorectal cancer screening: A labeled discrete choice experiment for a Dutch screening campaign. Acta Oncol. 2014;53(7):898-908. doi:10.3109/0284186X.2013.877159.
74. Phillips CD, McLeroy KR. Health in rural America: remembering the importance of place. Am. J. Public Health 2004;94(10):1661-1663. doi:10.2105/AJPH.94.10.1661. 75. López G, Bialik K. Key findings about U.S. immigrants. Pew Research Center.