R E V I E W A R T I C L E
Journey from 2D to 3D: Implant imaging a review
Anil Kumar N.1, Gaurav Agrawal2, Anchala Agrawal1, Sreedevi1, Ankur Kakkad11Department of Oral Medicine and Radiology, Hitkarini Dental College and Hospital, Jabalpur, Madhya Pradesh, India, 2Department of Oral Pathology, SMBT Dental College and Hospital, Sangamner, Maharashtra, India
Abstract
Imaging techniques play an important role in proper treatment planning for dental implant. Conventional radiographic imaging techniques provide suffi cient information regarding suggested implant sites. But, small size, image distortion, and magnifi cation limit their use in many cases. Previously computed tomography (CT) has been employed for pre-operative planning of implant. The major disadvantages of CT are artifacts, high dose of radiation, and cost. Advanced imaging modalities like cone-beam CT produces three-dimensional images at relatively low cost and radiation dose thus making it invaluable in coordination with other techniques providing the anatomical information thus helps in proper treatment plan, good prognosis and thus relatively low risks for surgical mishaps.
Keywords: Artifacts, dental implants, imaging modalities, radiation risk
Correspondence
Dr. Anchala Gaurav Agrawal, Department of Oral Medicine and Radiology, Hitkarini Dental College and Hospital, Jabalpur - 482 001, Madhya Pradesh, India. Phone: +91-9713623860.
C/o Mrs. Ratna Sakhuja, 2/B Hemasha Apartment, Near GS College, Jabalpur, M.P, India. E-mail: [email protected]
Received 29 November 2014; Accepted 29 December 2014
doi: 10.15713/ins.ijcdmr.13
How to cite the article:
Anil Kumar N, Gaurav Agrawal, Anchala Agrawal, Sreedevi, Ankur Kakkad, “Journey from 2-D to 3-D: Implant imaging a review,” Int J Contemp Dent Med Rev, Vol. 2014. Article ID 091114, 2014. doi: 10.15713/ins.ijcdmr.13
Introduction
The use of dental implants in oral rehabilitation has become an integral part of treatment for restoring edentulous spaces. The purpose of tooth replacement with implants is to restore adequate function and esthetics without aff ecting adjacent hard and/or soft tissue structures. Diagnostic radiography is essential for implants in pre-operative, intraoperative, and post-operative assessment by use of a variety of imaging techniques.[1] In the past, periapical radiographs, occlusal
radiograph along with panoramic images were used as the sole determinants of implant diagnosis and treatment planning; as these radiographic modalities provide a two-dimensional (2D) representation of three-dimensional (3D) structures. Hence, the advancement of radiographic technology including, cephalometrics, computed tomography (CT), magnetic resonance imaging (MRI) as well as cone-beam CT (CBCT) is increasingly considered essential for optimal implant placement.[2] 3D information is essential for the implantologist
before placement of osseointegrated dental implants.[3] The
fundamental basis for radiological examination is to maximize the ratio of the benefi t/risk, as imaging for the planning of
implant placement is confusing because of the large number of modalities available. Clinicians, however, must recognize that each technique has advantages and limitations. It is essential to consider treatment objectives and patient needs carefully before performing or ordering imaging tests.
The objectives of diagnostic imaging depend on:[4]
1. Amount and type of information required (i.e., combinations of conventional dental images)
2. Least radiation risk to the patient; and
3. Appropriate clinical examination and patient’s need. The ideal imaging technique for dental implant care should have several essential characteristics including:[6,7]
1. The ability to visualize the implant site in the mesiodistal, buccolingual, and superioinferior dimensions
2. The ability to allow reliable, accurate measurements 3. Normal anatomical structures (incisive canal, nasal fl oor,
maxillary sinus, mandibular canal)
4. Capacity to evaluate trabecular bone density and cortical thickness (height, width)
7. Minimal radiation risk (as low as reasonably achievable) [Tables 1 and 2].
Periapical radiography
Long cone paralleling technique is the technique of choice for taking periapical radiographs. Among all the imaging modalities, intraoral periapical radiographs off er the best resolution (line pairs/mm), area of interest can be examined for trabecular patterns, residual roots, periodontium, as well as angulation of adjacent teeth, readily available, inexpensive, less radiation dose.
Limitations
2D perspective of 3D anatomy, thus not adequate to estimate the amount of available bone (facio-lingual dimension) in the edentulous site, their limited size makes them inadequate for evaluating large edentulous areas and associated maxillary and mandibular structures, distortion of obtained image, anatomic limitations, and image receptor fl exibility [Figure 1a-c].
Digital intraoral radiographic images
Advantage of this over conventional periapical radiography is 75-90% less exposure, instant results, contrast can be manipulated.
Limitations
It will provide the dentist the limited area for imaging, and no facio-lingual dimension can be assessed.
Bitewing
This modality helps in the assessment of the coronal structure of tooth and alveolar bone in relation to the adjacent edentulous space.
Limitations
Periapical area cannot be assessed so approximation with adjacent vital structures is a major limitation.
Occlusal radiograph
Provide us with facio-lingual dimension technique is readily available, high image defi nition, inexpensive, less radiation exposure.
Limitations
Not useful in the maxillary arch because of distortion, records only the widest portion of mandible, with limited reproducibility.
Panoramic radiograph
This outlines the bony anatomy clearly and is generally used for diagnosis of gross pathoses within the jaws as well as the relation of anatomic structures such as sinuses, canals, fossa, and foramen in the implant site.
Limitations
Decreased resolution and sharpness, no cross-sectional imaging, magnifi cation is varied, and unreliable (25-30%) especially in the vertical dimension and is more pronounced in posterior than in anterior areas. Thus may give a false sense that more bone exists between the crest of the alveolar process and the Table 1: Commonly used radiographic procedures with time
intervals for treatment planning and assessment of dental implants Stage of treatment Time
(months)
Radiographic procedures
Treatment planning −1 PA, Pan, Tomo, CT, Ceph
Surgery (placement) 0 PA, Pan, Tomo, CT, Ceph for correction of problems
Healing 0-3 PA, Pan, Tomo, CT, Ceph for correction of problems
Remodeling 4-12 PA, Pan
Maintenance (without problems)
13+ PA, Pan, (follow-up approximately every 3 years)
Complications Anytime PA, Pan, CT (as indicated)
PA: Periapical, Pan: Panoramic radiography, Tomo: Conventional tomography, CT: Reformatted computed tomography
Table 2: Imaging modalities and limitations
Analog/two dimensional Digital/three dimensional Periapical Computed tomography (CT)
Digital periapical DentaScan imaging
Bitewing ICT
Occlusal MRI
Panoramic CBCT, MDCT
Lateral cephalometric
CT: Computed tomography, ICT: Interactive computed tomography, MRI: Magnetic resonance imaging, CBCT: Cone-beam CT, MDCT: Multi-detector CT
Figure 1: (a-c) Periapical radiograph showing implant fi xtures, along with abutment
c
inferior alveolar canal, nasal fossa or maxillary sinuses. Improper patient positioning may further contribute to image distortion. Even properly positioned and exposed panoramic radiographs cannot be used for direct bony measurements (not enough for implant placement) unless the magnifi cation factor for the target area is predetermined. Predetermination of the magnifi cation factor can be accomplished using a radiographic stent with ball bearings embedded in acrylic and imaged in the patient’s mouth [Figure 2].
Lateral cephalogram
Along with soft tissue profi le of the patient, axial tooth inclination and dentoalveolar ridge relationship in the midline can be assessed.
Limitations
Provide dentist with cross-sectional dimension only at midline, image magnifi cation and also contralateral side superimposition evident [Figure 3].[8-12]
CT
3D reformatting useful in augmentation process like sinus augmentation, uniform magnifi cation, high contrast, defi nition, multiplanar views, 3D reconstruction, simultaneous study of multiple implant sites, also enables software analysis.
Limitations
Limited availability, the cost factor, high radiation risk, requires technical skill, lack of usefulness for implant- interface follow-up due to lack of metallic streak artefacts [Figure 4a and b].
Dentascan imaging
This imaging modality provides us with programmed formation, recollection, and display of the image, mandibular arch, the
maxillary arch and cross-sectional and tangential/panoramic images of the alveolus enabling accurate preprosthetic treatment planning. Diagnostic template is necessary for determining the position and orientation of dental implants.
Limitations
Magnifi cation of images, grayscale values, is limited, and the tilt of the patient’s head during the examination is critical.
Interactive CT (ICT)
It overcomes limitations of CT, also enables radiologist to transfer the image to the computer, so clinician can view the image on his own computer. Hence, 3D treatment can be planned according to patient’s anatomy and can be seen before surgery thus helping in determining the number and size of implants correctly according to density of bone at suggested sites. ICT is more relevant diagnostic technique when compared to conventional techniques for implant planning.
Limitations
Exact position of implants is diffi cult, tedious and time-consuming [Figure 5].
Figure 2: Panoramic radiograph showing fi ve implants in mandibular anterior tooth region
Figure 3: Sagittal view showing soft tissue profi le along with cross-sectional image
Figure 4: Computed tomography images, bone reconstruction showing as denta scanner (a), determination of alveolar bone height in maxillary anterior tooth region and distance from nasal fossa (b)
MRI
In MRI, cortical bone can be clearly delineated from the cancellous bone. Vital structures such as nerves, vessels, and the
fl oor and mucosa of the maxillary sinus are readily identifi ed by the implant surgeon, exceptionally safe due to the absence of ionizing radiation, high image quality.
Limitations
High capital and running costs with lack of availability have been a signifi cant barrier to the use of MRI for implant assessment.[13,14]
CBCT and multidetector CT
It allows the surgeon to have an accurate information of implant site, in edentulous patient or when multiple implants are considered thus aiding in diagnosis and provides the dentist with controlled surgical plan, is used when conventional radiograph fails to provide the needed information.[18] Assessment can
be done in all three planes of space without image distortion, superimposition of structures, and diff erential magnifi cation of the image based on geometry, also accurate location of anatomic landmarks as well as the height, width, angulation, and quality of alveolar bone for implant site. Also for case selection and a postsurgical evaluation to assess implant’s position in the alveolus.
Limitations
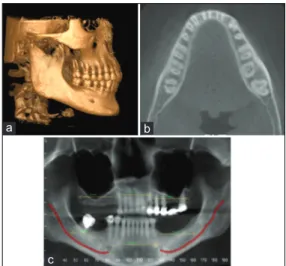
Increased susceptibility to movement artifacts and metallic restoration may lead to streak artefact, in CBCT no standard grayscale system present, so universality is questionable [Figure 6a-c and Table 3].[15-19]
Complications
Failure of the implant to osseointegrate with adjacent bone is the most common mishap leading to implant mobility, post-operative infection (perimplantitis) [Figure 7a-c].
Conclusion
Dental implantology is a rapidly expanding area of dentistry. The imaging modalities range from 2D projections to complex 3D imaging. The 2D modalities are readily available, cost eff ective with least radiation exposure, but have limitations of magnifi cations and superimpositions and so clinician will not be able to develop a 3D perspective of patient’s anatomy with a single image. However, in complex cases, more extensive and advanced radiographic evaluation is needed.[10] Hence,
cross-sectional imaging is increasingly considered essential for optimal implant placement, important roles in pre- and post-operative evaluation of the implant patient especially in complex reconstructions and multiple implants.[11,12]
Figure 5: Interactive computed image on the computer screen
Figure 7: (a) Saucerization, (b) perifi xtural bone loss, (c) implant fracture
c
b a
Figure 6: Cone-beam computed tomography, sagittal view (a), mandibular arch (b), inferior alveolar canal on cross-sectional image (c)
c
References
1. Bagchi P, Joshi N. Role of radiographic evaluation in treatment planning for dental implants: A review. J Dent Allied Sci 2012;1:21-5.
2. Tyndall DA, Brooks SL. Selection criteria for dental implant site imaging:A position paper of the American Academy of Oral and Maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:630-7.
3. Frederiksen NL. Diagnostic imaging in dental implantology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;80:540-54.
4. Bornstein MM, Scarfe WC, Vaughn VM, Jacobs R. Cone beam computed tomography in implant dentistry: A systematic review focusing on guidelines, indications, and radiation dose risks. Int J Oral Maxillofac Implants 2014;29 Suppl:55-77. 5. Patel S, Kumar NA. Implant radiology. J Indian Dent Assoc
2009;3:2.
6. Lingeshwar D, Dhanasekar B, Aparna IN. Diagnostic imaging in implant dentistry. Int J Oral Implantol Clin Res 2010;1:147-53. 7. Jayadevappa BS, Kodhandarama GS, Santosh SV, Rashid WT.
Imaging of dental implants. J Oral Health Res 2010;1:2. 8. Siu AS, Chu FC, Li TK, Chow TW, Deng FL. Imaging modalities
for preoperative assessment in dental implant therapy: An overview. Hong Kong Dent J 2010;7:23-30.
9. Kalra D, Jain G, Deoghare A, Lambade P. Role of imaging in dental implants. J Indian Acad Oral Med Radiol 2010;22:34-8. 10. DelBalso AM, Greiner FG, Licata M. Role of diagnostic imaging
in evaluation of the dental implant patient. Radiographics 1994;14:699-719.
11. Mupparapu M, Singer SR. Implant imaging for the dentist. J Can Dent Assoc 2004;70:32.
12. Manisundar N, Saravanakumar B, Hemalatha VT, Manigandan T, Amudhan A. Implant imaging - A literature review. Biosci Biotechnol Res Asia 2014;11:179-87.
13. Almog DM, Romano PR. CT-based dental imaging for implant planning and surgical guidance. N Y State Dent J 2007;73:51-3. 14. Gahleitner A, Watzek G, Imhof H. Dental CT: imaging
technique, anatomy, and pathologic conditions of the jaws. Eur Radiol 2003;13:366-76.
15. Scarfe WC, Farman AG, Sukovic P. Clinical applications of cone-beam computed tomography in dental practice. J Can Dent Assoc 2006;72:75-80.
16. Tyndall DA, Rathore S. Cone-beam CT diagnostic applications: caries, periodontal bone assessment, and endodontic applications. Dent Clin North Am 2008;52:825-41, vii.
17. Kumar V, Satheesh K. Applications of cone beam computed tomography (CBCT) in implant treatment planning. JSM Dent 2013;1:1008.
18. De Vos W, Casselman J, Swennen GR. Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: a systematic review of the literature. Int J Oral Maxillofac Surg 2009;38:609-25.
19. Alamri HM, Sadrameli M, Alshalhoob MA, Sadrameli M, Alshehri MA. Applications of CBCT in dental practice: A review of the literature. Gen Dent 2012;60:390-400.
Table 3: Dose comparisons of dental imaging modalities
Technique Single periapical fi lm Full mouth radiographic survey Panoramic CT maxilla CT mandible MRI CBCT
Eff ective dose (μsv) 10 150 26 104 761 0 20-70