R E S E A R C H B R I E F
Fracture resistance of endodontically treated premolars
with optimum and overprepared post spaces
Khalid M. Abdelaziz1, Cinderella K. Keshk2, Omar S. Al-Mashhour3, Mohamed A. Alhudairy3, Mohamed S. Asiri3, Abdulla
M. Alshehri3, Mohamed I. Elshinawy1,4
1Department of Restorative Dental Sciences, King Khalid University, College of Dentistry, Abha, Saudi Arabia, 2BDS Program,Faculty of Dentistry, Al-Ahram
Canadian University, 6th October City, Giza, Egypt, 3Intern, College of Dentistry, King Khalid University, Abha, Saudi Arabia, 4Department of Endodontics, Faculty
of Dentistry, Tanta University, Tanta, Egypt
Abstract
Background: Premolars are usually loss their integrity and strength following endodontic treatment. This situation necessitates the use of post-core-crown system at the time of tooth restorations; however, the criteria of post space preparation may affect the retention of the utilized posts and the resistance of the restored teeth to fracture.
Aim: This study aims to evaluate the effect of post space preparation criteria on the fracture resistance of endodontically treated premolars. Materials and Methods: A total of 40 extracted single-rooted premolars were subjected to endodontic treatment after cutting their crowns 2 mm above the cervical line. Root canals in Group 1 (n = 20) were optimally prepared to receive #2 fiber post (Relyx fiber post), while those in Group 2 (n = 20) were overprepared using #3 drill to receive the same size of posts. All posts were fixed into their respective spaces using self-adhesive resin cement (RelyX Unicem) before building resin composite cores up. Additional 20 premolars with no endodontic treatment served as control. All teeth were then prepared to receive standardized zirconia-based crowns. The fracture resistance of teeth in each group was evaluated on a universal testing machine before and after store aging and thermocycling. Both ANOVA and Tukey’s comparisons at α = 0.05 were used to statistically analyze the results. Results: All endodontically treated teeth fractured at lower stress values than non-treated teeth (P < 0.05). Teeth with over prepared post spaces fractured at lower stress values than those with optimally prepared post spaces (P = 0.0001382 and 0.000138). Non-aged teeth in all groups showed more resistance to fracture than aged ones (P = 0.0001382, 0.0001386, and 0.0001424). Signs of catastrophic tooth fracture were seen in most of the tested specimens. Conclusion:
Although all restoration options provide premolars resistant to fracture under regular masticatory values, their resistance is decreased by aging. Over preparation of post spaces results in lower resistance of the restored teeth to fracture on loading. Clinical Significance: Because endodontically treated teeth, even those restored with post-core-crown systems, usually show a reduction in their fracture resistance by age, dentists should utilize the most conservative techniques while restoring these kinds of teeth.
Keywords: Fiber post, fracture resistance, post space, premolars, self-adhesive cement, zirconia crowns
Correspondence
Dr. Khalid M Abdelaziz, Department of Restorative Dental Sciences, College of Dentistry, King Khalid University, PO Box 3263, Abha 61471, Saudi Arabia.
Tel.: +966172418044/+966530870912. Fax: +966172418066.
E-mail: [email protected]
Received: 12 January 2018 Accepted: 17 April 2018
Doi: 10.15713/ins.ijcdmr.126
How to cite the article:
Khalid M. Abdelaziz, Cinderella K. Keshk, Omar S. Al-Mashhour, Mohamed A. Alhudairy, Mohamed S. Asiri, Abdulla M. Alshehri, Mohamed I. Elshinawy, “Fracture resistance of endodontically treated premolars with optimum and overprepared post spaces,” Int J Contemp Dent Med Rev, vol. 2018, Article ID: 010418, 2018. doi: 10.15713/ins.ijcdmr.126
Introduction
Restoration of endodontically treated teeth with post-core system is usually recommended when the remaining coronal tooth structure cannot retain and support the overlaying crown restorations.[1-4] Fiber-reinforced composite (FRC) posts have
been introduced as an alternative to both cast and ceramic
posts.[5] Currently, this kind of posts is widely used in restoring
the endodontically treated teeth due to its mechanical behavior that helps the restored teeth to survive under chewing loads.
[2,6,7] Although FRC posts are esthetically acceptable and easily
bonded to the tooth structure,[5] the loss of post and crown
fracture usually have to be extracted, root fracture is considered to be the most serious cause of failure.[8-11]
The use of adhesive cementation would also improve the post retention and root fracture resistance in spite of the expected interference of the endodontic procedure and materials with the adhesion of resin-based cements.[12-14] On the other hand, the
self-etching and self-adhesive resin cements have recently been introduced aiming to simplify the cementation procedure and to save both dentist and patient’s time.[15,16] One study did confirm
better retention of fiber posts luted with thicker films of resin-based cements into overprepared dowel spaces.[17] Many others
have also extensively examined the retention of endodontic posts in different clinically simulated situations and few more studied the fracture resistance of endodontically treated teeth. However, none did assess the influence of post space preparation criteria on the fracture resistance of the restored teeth.[18-20]
Based on the aforementioned literature, the current study aimed to assess the influence of optimally and overprepared post spaces (over-PPS) on fracture resistance of teeth restored with a post-core-crown system. The null hypotheses, therefore, suggested no adverse effect of over-PPS or simulated aging on the fracture resistance of teeth restored with post-core-crown system.
Materials and Methods
Crowns of 40 extracted single-rooted premolars were cut off 2 mm above the cervical line. All teeth were prepared to receive regular endodontic treatment. Following the protocol shown in Table 1, root canals were prepared in two groups (n = 20 each). Teeth in Group 1 (G1) were first prepared to the optimum diameter using #2 size-matching drill (RelyX Fiber Post, 3M ESPE, St. Paul, MN), washed using normal saline and then dried using paper points, while those in Group 2 (G2) were overprepared using #3 drill, 1.9 mm in diameter, before their washing and drying.
The self-adhesive resin cement (RelyX Unicem Aplicap, 3M ESPE, St. Paul, MN) was used to lute the selected posts into the prepared dowel spaces. Cement capsules were first activated for 2 s and mechanically mixed in Silamat S6 amalgamator (Ivoclar
Vivadent, Schaan, Liechtenstein) for 15 s. By the help of the special applicator, the mixed cement was directly injected through capsule nozzle into the prepared dowel spaces and against the bodies of the selected posts. All posts were inserted to the full depth of their respective spaces using hand pressure and gentle agitation to spill the excess cement out. The excess cement was flushed to the top of the coronal tooth structure using microbrushes. Following the setting of cement material, the lengths of the exposed posts were cut off to be 4 mm long above the flat coronal tooth structure. Resin composite cores (Filtek Supreme XT, 3M ESPE, St. Paul, MN); 6 mm high,were then built up in three increments; each was light cured (Elipar S10 light curing device, 3M ESPE, Seefeld, Germany) for 20 s, against the remaining tooth structure and to totally envelop the exposed posts’ length.
Another 20 premolars with no endodontic treatment served as control (Cont). All teeth were then prepared (1.2 mm axial reduction with shoulder FL, 6° axial taper, 7 mm occlusogingival height) to receive standardized CAD-CAM fabricated zirconia-based crowns. The prepared teeth were optically scanned using Ceramill Map400 (Amann Girrbach, Koblach, Austria), the standardized crowns were designed with Ceramill Mind software and the crowns were then milled on Ceramill Motion2 (Amann Girrbach, Koblach, Austria) out of zirconia-based ceramic blocks (ZR) (Ceramill Zi, Amann Girrbach, Koblach, Austria).
The fitting surfaces of the fabricated crowns were bombarded with a mixture of 50 and 110 µm alumina (Al2O3) particles
for 10 s using a pressure of 250 KPa before their cementation onto their respected teeth using the same self-adhesive resin cement. 10 teeth out of each group were then subjected to aging circumstances (1 m storage in water and 3500 cycles of thermocycling at 5–55°C with 1 min dwell time)before coating their roots with a single layer of low viscosity rubber impression material (Imprint II, 3M ESPE, St. Paul, MN) in resemblance to the natural periodontal ligament.[21] The coated roots were
then embedded into acrylic blocks to help the conduction of the fracture resistance test. The buccal cusps of all restored teeth were obliquely stressed (at 45° inclination) to fracture by the aid of a round end rod on a universal testing machine (Instron, Model 3300, Instron Corp, Grove City, PA) running at a crosshead speed of 0.05 mm/min[21] [Figure 1]. The maximum
Table 1: Levels of the study
Groups (n=20 each) Subgroups (n=10 each)
G1 #2 fiber posts (1.6 mm) luted with optimum cement thickness into
Opt‑PPS (1.6 mm) Composite core build‑up
Restored with zirconia‑based crowns
SG1: Non‑aged
SG2: Aged (1‑month storage in water and thermocycling)
G2 #2 fiber posts (1.6 mm) luted with thicker cement thickness into
over‑PPS (1.9 mm) Composite core build‑up
Restored with zirconia‑based crowns
SG1: Non‑aged
SG2: Aged (1‑month storage in water and thermocycling)
Control Natural teeth with no endodontic treatment
Restored with zirconia‑based crowns SG1: Non‑aged SG2: Aged (1‑month storage in water and
thermocycling)
load at failure were recorded for each specimen and the collected data were statistically analyzed using both ANOVA and Tukey’s comparisons at a = 0.05 to determine the significance of the differences detected between subgroups. The fracture pattern of each specimen was also assessed to find out the specific areas of weakness (crown, core, post, or the root).
Results
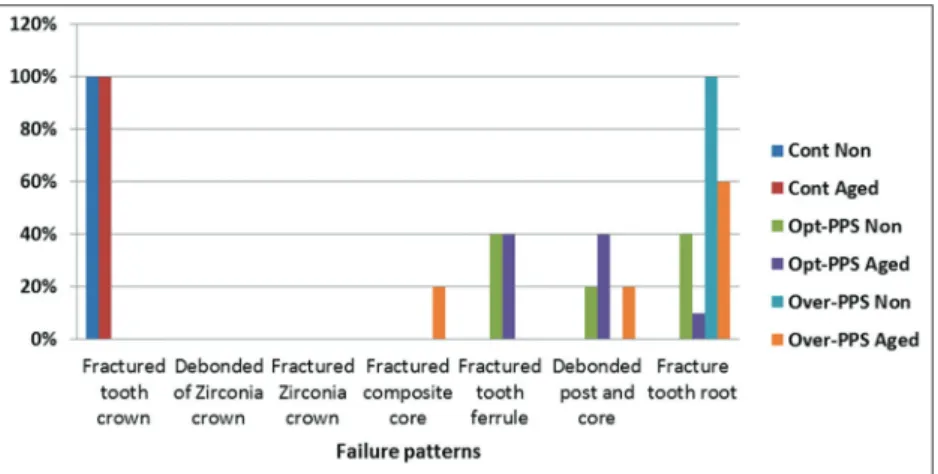
The mean values ±standard deviation of the fracture loads (N) in all subgroups were listed in Table 2. Statistical analysis of the collected data indicated some difference between the tested subgroups (ANOVA, P < 3.415E-37). All endodontically treated teeth in G1 and G2 were less resistant to fracture than non-treated teeth (control) (Tukey’s, P < 0.05). Teeth with over-PPS in G2 fractured at lower force values than those with optimally prepared post spaces (Opt-PPS) in G1 (Tukey’s, P = 0.0001382 and 0.000138 for SG1and SG2, respectively). Non-aged teeth (SG1) in all groups showed more resistance to fracture than aged ones (SG2) (Tukey’s, P = 0.0001382, 0.0001386, and 0.0001424 for Cont., G1, and G2, respectively). All fractures of the control specimens (Cont.) were noticed in tooth crowns. Most of the teeth with over-PPS (G2) showed fractures in their roots; while those with opt-PPS (G1) showed a varied distribution of different failure patterns [Figures 2 and 3].
Discussion
The restoration of endodontically treated teeth is always a point of concern in daily dental practice. The current advances in both endodontics and restorative dentistry aid in preserving many teeth those formally considered for extraction. However, the loss of tooth structure and altered physical characteristics following endodontic therapy necessitates a form of restorative treatment that for sure would affect the clinical longevity of the treated teeth.[22] The use of endodontic posts is currently a routine
procedure in restoring massively destructed teeth to help provide the constructed cores with the necessary retention and resistance to displacement.[23] These functions are best achieved using the
FRC posts due to their superior mechanical properties. Although the failure of this restorative approach is usually considered when either tooth root fracture or post dislodgement is encountered,[24]
adhesive luting of the endodontic posts revealed improved retention and accordingly minimal incidence of debonding. [25-27] However, the effect of over-PPS and the mandatory use of
thicker films of resin-based cement to lute the utilized FRC posts on the survival of the restored endodontically treated teeth, to the best of our knowledge, has not been extensively evaluated. Therefore, this in vitro study had the concern to assess such influence in the presence of oblique displacing loads. Although the null hypothesis denied the effect of both over-PPS and simulated aging on the fracture resistance values of restored premolars, the recorded results [Tables 2 and 3] necessitated the rejection of that null hypothesis.
The results revealed lower resistance to fracture of the endodontically treated teeth in comparison to non-treated ones with tooth body fracture being the dominant sign of failure. This finding could be supported by one study that revealed significant weakness in the endodontically treated teeth in comparison to vital teeth. The noticed weakness was partly related to the compromised structural integrity that greatly influence the ability of the treated teeth to survive under functional and impact stresses.[28] In spite of the recorded
lower resistance to fracture came in agreement with previous findings, these records were found to be greater than the known values of normal chewing loads (68.65–147.1 N) and could, accordingly, satisfy the clinical requirements.[29,30] This
finding could, on the one hand, be explained by the influence of adhesive protocols applied in this study to lute FRC posts into their respective post spaces and supported, on the other hand, by a finite element analysis that proved the role of bonded posts in reducing stresses inside tooth roots.[31] Other studies also
confirmed the strengthening effect of the adhesively luted posts that would help the survival of endodontically treated teeth on mastication.[27,32]
Results of the current study also revealed adverse effects of both over-PPS and simulated aging on the fracture resistance of the restored teeth. Some researchers ranked the luting cement to be the weakest link in the tooth/post/core complex. Therefore, the thicker films of cement needed to lute FRC Figure 1: Testing the fracture resistance of restored teeth
Figure 2: Failures in test specimens: (a) horizontal Fracture in tooth root, (b) Horizontal fracture of tooth crown, and (c) Fracture in the composite core
posts into the overprepared spaces may aid in compromising the long-term prognosis of the restored teeth.[33-38] This
postulation, in some way, could support the results of the current study that indicated lower fracture resistance of specimens with over-PPS. Other studies referred similar findings to the altered stress distribution in the presence of endodontic posts.[39-41] When these stresses reach a critical
value, a slowly growing crack may cause a successive adhesive failure at post-cement-root dentin interface. After loss of post adhesion, the post is more or less mobile within the root and is consequently allowed to act like a wedge transferring the stresses to root canal walls and increasing the possibility of root fracture specially in case of either thinner canal walls or thicker resin cement.[39,40,42] Moreover, the accidentally trapped
voids that result from improper placement of composite resin around the coronal portion of the FRC posts could weaken the bond between the post and the core and this can jeopardize the fracture resistance of the restored teeth.[43,44]
At the same time, failures of the tested specimens were mostly reported at the cervical area of the restored teeth [Figures 2 and 3]. The fractographic analysis of teeth restored with posts and cores proved that fractures usually start at the inner region adjacent to root canals and continue toward the outer surface of the tooth.[45] However, the known match
between the elastic modulus of FRC posts and dentin can offer more homogenous distribution of stresses at post-dentin interface. This information could, accordingly, explain why all favorable fractures were limited to the cervical portion of the root including the core-dentin interface since the
stresses were concentrated in the cervical area and the outer root surface.[45,46] Previous investigators also proved that the
incidence of intraoral adhesive failures normally increased in response to cyclic loading and other environmental factors such as temperature, pH changes, and microorganisms.[47]
Their notice surely supports the findings of the current study that indicated adverse effect of aging on the fracture resistance values of the tested specimens. The limited number of specimens and the difficulty related to reproducing the complexity of functional loads in the oral environment may be considered among the shortcomings of the present study. Therefore, further studies including finite element analysis and long-term cyclic loading are recommended to complement the findings of the present study.
Conclusion
All the recruited restorative options can provide premolars resistant to fracture on mastication; this feature is deteriorated on aging. Over-PPS and utilizing thicker films of cement to lute FRC posts adversely affect the resistance of the restored premolars to fracture. Therefore, preservation of tooth tissue during both endodontic and restorative procedure is recommended to improve their ability to survive on function.
References
1. Mitsui FH, Marchi GM, Pimenta LA, Ferraresi PM. In vitro
study of fracture resistance of bovine roots using different intraradicular post systems. Quintessence Int 2004;35:612‑6. 2. Christensen GJ. Post concepts are changing. J Am Dent Assoc
2004;135:1308‑10.
3. Christensen GJ. Posts and cores: State of the art. J Am Dent Assoc 1998;129:96‑7.
4. Federick DR. An application of the dowel and composite resin core technique. J Prosthet Dent 1974;32:420‑5.
5. Qualtrough AJ, Mannocci F. Tooth‑colored post systems: A review. Oper Dent 2003;28:86‑91.
Figure 3: Incidences of failure patterns (%) in different subgroups
Table 2: Mean fracture loads (N) in different subgroups
Subgroups Groups
Control (Cont) Opt‑PPS (G1) Over‑PPS (G2)
Non‑aged (SG1) 410.54±14.03a 299.61±22.34b 208.84±13.83c
Aged (SG2) 321.45±10.04d 253.23±18.85e 166.42±17.08f
6. De Santis R, Prisco D, Apicella A, Ambrosio L, Rengo S, Nicolais L. Carbon fiber post adhesion to resin luting cement in the restoration of endodontically treated teeth. J Mater Sci Mater Med 2000;11:201‑6.
7. Duret B, Duret F, Reynaud M. Long‑life physical property preservation and postendodontic rehabilitation with the composipost. Compend Contin Educ Dent Suppl 1996;20:50‑6. 8. Bolhuis P, De Gee A, Feilzer A. Influence of fatigue loading
on four post‑and‑core systems in maxillary premolars. Quintessence Int 2004;35:657‑67.
9. Stockton LW, Williams PT. Retention and shear bond strength of two post systems. Oper Dent 1999;24:210‑6.
10. King PA, Setchell DJ, Rees JS. Clinical evaluation of a carbon fibre reinforced carbon endodontic post. J Oral Rehabil 2003;30:785‑9.
11. Al‑harbi F, Nathanson D. In vitro assessment of retention of four
esthetic dowels to resin core foundation and teeth. J Prosthet Dent 2003;90:547‑55.
12. Balbosh A, Ludwig K, Kern M. Comparison of titanium dowel retention using four different luting agents. J Prosthet Dent 2005;94:227‑33.
13. Gerth HU, Dammaschke T, Züchner H, Schäfer E. Chemical analysis and bonding reaction of RelyX unicem and bifix composites‑a comparative study. Dent Mater 2006;22:934‑41. 14. Zicari F, Couthino E, De Munck J, Poitevin A, Scotti R, Naert I,
et al. Bonding effectiveness and sealing ability of fiber‑post bonding. Dent Mater 2008;24:967‑77.
15. Wang VJ, Chen YM, Yip KH, Smales RJ, Meng QF, Chen L. Effect of two fiber post types and two luting cement systems on regional post retention using the push‑out test. Dent Mater 2008;24:372‑7.
16. Cantoro A, Goracci C, Vichi A, Mazzoni A, Fadda GM, Ferrari M. Retentive strength and sealing ability of new self‑adhesive resin cements in fiber post luting. Dent Mater 2011;27:e197‑204. 17. Othman HI, Elshinawy MI, Abdelaziz KM. Retention of
fiber post to optimally and over prepared dowel spaces. J Adv Prosthodont 2013;5:16‑20.
18. Boone KJ, Murchison DF, Schindler WG, Walker WA 3rd. Post
retention: The effect of sequence of post‑space preparation, cementation time, and different sealers. J Endod 2001;27:768‑71. 19. McMichen FR, Pearson G, Rahbaran S, Gulabivala K.
A comparative study of selected physical properties of five root‑ canal sealers. Int Endod J 2003;36:629‑35.
20. Al‑Omiri MK, Rayyan MR, Abu‑Hammad O. Stress analysis of endodontically treated teeth restored with post‑retained crowns: A finite element analysis study. J Am Dent Assoc 2011;142:289‑300. 21. Abdelaziz KM, Keshk CK, Alshadidi A, Mafraq S, Murchison DF. Fracture resistance of ceramic crowns supported with indirect chair‑side composite cores. J Int Soc Prev Community Dent 2018;8:34‑40.
22. Kumar L, Pal B, Pujari P. An assessment of fracture resistance of three composite resin core build‑up materials on three prefabricated non‑metallic posts, cemented in endodontically
treated teeth: An in vitro study. Peer J 2015;3:e795.
23. Erdemir A, Ari H, Güngüneş H, Belli S. Effect of medications for root canal treatment on bonding to root canal dentin. J Endod 2004;30:113‑6.
24. Bergman B, Lundquist P, Sjögren U, Sundquist G. Restorative and endodontic results after treatment with cast posts and cores. J Prosthet Dent 1989;61:10‑5.
25. Standlee JP, Caputo AA. Endodontic dowel retention with resinous cements. J Prosthet Dent 1992;68:9137.
26. Varela SG, Rabade LB, Lombardero PR, Sixto JM, Bahillo JD,
Park SA. In vitro study of endodontic post cementation protocols
that use resin cements. J Prosthet Dent 2003;89:146‑53. 27. Nissan J, Dmitry Y, Assif D. The use of reinforced composite
resin cement as compensation for reduced post length. J Prosthet Dent 2001;86:304‑8.
28. Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J Endodont 1992;18:332‑5.
29. Tortopidis D, Lyons MF, Baxendale RH, Gilmour WH. The variability of bite force measurement between sessions, different positions within dental arch. J Oral Rehabil 1998;25:681‑6. 30. Ferrari M, Vicchi A, Mannocci F, Mason PN. Retrospective study of
the clinical performance of fiber posts. Am J Dent 2000;13:9B‑13. 31. Asmussen E, Peutzfeldt A, Sahafi A. Finite element analysis
of stresses in endodontically treated, dowel‑restored teeth. J Prosthet Dent 2005;94:321‑9.
32. Mendoza DB, Eakle WS, Kahl EA, Ho R. Root reinforcement with a resinbonded preformed post. J Prosthet Dent 1997;78:10‑4. 33. Teixeira CS, Silva‑Sousa YT, Sousa‑Neto MD. Bond strength
of fiber posts to weakened roots after resin restoration with different light‑curing times. J Endod 2009;35:1034‑9.
34. Zogheib LV, Pereira JR, do Valle AL, de Oliveira JA, Pegoraro LF. Fracture resistance of weakened roots restored with composite resin and glass fiber post. Braz Dent J 2008;19:329‑33.
35. Marchi GM, Mitsui FH, Cavalcanti AN. Effect of remaining dentine structure and thermal‑mechanical aging on the fracture resistance of bovine roots with different post and core systems. Int Endod J 2008;41:969‑76.
36. Teixeira C, Felippe MC, Silva‑Sousa YT, de Sousa‑Neto MD. Interfacial evaluation of experimentally weakened roots restored with adhesive materials and fibre posts: An SEM analysis. J Dent 2008;36:672‑82.
37. Moosavi H, Maleknejad F, Kimyai S. Fracture resistance of endodontically‑treated teeth restored using three root reinforcement methods. J Contemp Dent Pract 2008;9:30‑7. 38. Bonfante G, Kaizer OB, Pegoraro LF, do Valle AL. Fracture
strength of teeth with flared root canals restored with glass fibre posts. Int Dent J 2007;57:153‑60.
39. Coelho CS, Biffi JC, Silva GR, Abrahão A, Campos RE, Soares CJ. Finite element analysis of weakened roots restored with composite resin and posts. Dent Mater J 2009;28:671‑8. 40. Santos AF, Meira JB, Tanaka CB, Xavier TA, Ballester RY,
Lima RG, et al. Can fiber posts increase root stresses and reduce
fracture? J Dent Res 2010;89:587‑91.
41. Soares CJ, Castro CG, Filho PC, Soares PV, Magalhaes D, Martins LR. Two‑dimensional FEA of dowels of different compositions and external surface configurations. J Prosthodont 2009;18:36‑42. 42. Silva GR, Santos‑Filho PC, Simamoto PC Jr., Martins LR,
Mota AS, Soares CJ. Effect of post type and restorative techniques on the strain and fracture resistance of flared incisor roots. Braz Dent J 2011;22:230‑7.
43. Dilmener FT, Sipani C, Dalkiz M. Resistance of three new esthetic post and core systems to compressive loading. J Prosth Dent 2006;95:130‑6.
2011;19:28‑33.
45. Kishen A, Kumar GV, Chen NN. Stress‑strain response in human dentine: Rethinking fracture predilection in post‑core restored teeth. Dent Traumatol 2004;20:90‑100.
46. Pegoretti A, Fambri L, Zappini G, Bianchetti M. Finite element
analysis of a glass fiber reinforced composite endodontic post. Biomaterials 2002;23:2667‑82.
47. Huysmans MC, Peters MC, Van der Varst PG, Plasschaert AJ. Failure behaviour of fatigue‑tested post and cores. Int Endod J 1993;26:294‑300.