Randomized, Controlled Trial of Slow Versus Rapid Feeding Volume
Advancement in Preterm Infants
Judith Caple, RNC, MSN, NNP; Debra Armentrout, RNC, MSN, NNP; Valerie Huseby, RNC, MSN, NNP; Brenda Halbardier, RNC, MSN, NNP; Jose Garcia, MD; John W. Sparks, MD; and Fernando R. Moya, MD
ABSTRACT. Objectives. To determine whether
in-fants who are fed initially and advanced at 30 mL/kg per day (intervention) take fewer days to get to full feedings than those who are fed initially and advanced at 20 mL/kg per day (control), without increasing their inci-dence of feeding complications and necrotizing entero-colitis (NEC). We also examined whether these infants regain birth weight earlier, have fewer days of intrave-nous fluids, and a have shorter hospital stay.
Methods. A randomized, controlled, single-center trial was conducted in a Neonatal Intensive Care Unit of a community-based county hospital in Houston, Texas. Infants between 1000 and 2000 g at birth, gestational age
<35 weeks, and weight appropriate for gestational age
were allocated randomly to feedings of expressed human milk or Enfamil formula starting and advanced at either 30 mL/kg per day or 20 mL/kg per day. Infants remained in the study until discharge or development of stage
>IIA NEC.
Results. A total of 155 infants were enrolled: 72 in-fants in the intervention group and 83 in the control group. Infants in the intervention group achieved full-volume feedings sooner (7 vs 10 days, median), regained birth weight faster (11 vs 13 days, median), and had fewer days of intravenous fluids (6 vs 8 days, median). Three infants in the intervention group and 2 control infants developed NEC for an overall incidence of 3.2% (relative risk: 1.73; 95% confidence interval: 0.30 –10.06).
Conclusion. Among infants between 1000 and 2000 g at birth, starting and advancing feedings at 30 mL/kg per day seems to be a safe practice and results in fewer days to reach full-volume feedings than using 20 mL/kg per day. This intervention also leads to faster weight gain and fewer days of intravenous fluids.Pediatrics2004;114: 1597–1600; enteral feedings, newborn, necrotizing entero-colitis.
ABBREVIATIONS. NEC, necrotizing enterocolitis; EHM, ex-pressed human milk; NPO, nothing by mouth.
O
ptimal enteral feeding methods in preterm infants have not been well defined.1 Contro-versy exists regarding when feedings should be started, whether minimal enteral feedings shouldbe used routinely in small preterm infants, and how fast to advance enteral feedings.2–5 Preterm infants can exhibit delayed gastric emptying and often have feeding residuals, although what constitutes a clini-cally significant gastric residual remains unclear.6 However, recent evidence suggests that very low birth weight infants who develop necrotizing entero-colitis (NEC) have more gastric residuals than those who do not.7On the basis of these and other factors, enteral feedings are frequently advanced slowly in these neonates. This practice may compromise the precarious nutritional status of some of these infants and prolong the use of intravenous fluids.
Increments of enteral feeding of 10 to 20 mL/kg per day have been reported as safe in a prospective study,4 but several retrospective studies have sug-gested that advancing feedings rapidly is associated with an increased risk for NEC.8,9In 1 of these stud-ies, feeding increments were as high as 40 to 50 mL/kg per day.8Conversely, a relatively more rapid advancement of enteral feedings in preterm infants may improve their growth and nutritional status, decrease the need for and hazards of intravenous infusion solutions, and potentially shorten the length of hospitalization. Rayyis et al5 reported no differ-ence in the inciddiffer-ence of feeding intolerance or NEC in infants who received 35-mL versus 15-mL feeding advancements. Intermediate rates of advancement have not been studied. Therefore, we examined whether infants who were fed initially and advanced at 30 mL/kg per day take fewer days to get to full feedings than those who were fed initially and ad-vanced at 20 mL/kg per day, without increases in their incidence of feeding complications and NEC. Also, we studied whether infants who were fed the higher volume regain birth weight earlier, have fewer days of intravenous fluids, and have a shorter hospital stay than those who were advanced at the slower rate.
METHODS
All eligible infants were cared for in either the level 2 or 3 neonatal intensive care unit of a large community-based county hospital in Houston, Texas, during 1994 –1995. Entry criteria in-cluded birth weight of 1000 to 2000 g, gestational age of 35 weeks or less determined by the modified Ballard examination,10and
weight and length appropriate for gestational age. We chose not to include infants who weighed⬍1000 g because their feedings are often started many days after birth as a result of their degree of sickness; feedings are frequently stopped for various reasons; and given our low number of admissions of infants⬍1000 g, it would not have been feasible to study enough infants in such a group in
From the Department of Pediatrics, University of Texas–Houston Medical School, Houston, Texas.
Accepted for publication Jun 17, 2004. doi:10.1542/peds.2004-1232
Reprint requests to (J.C.) Department of Pediatrics, University of Texas– Houston Medical School, 6431 Fannin St, MSB 3.218, Houston, TX 77030. E-mail: [email protected]
a single-center trial. Exclusion criteria were the presence of major congenital anomalies or congenital abnormalities of the gastroin-testinal tract, antenatal exposure to controlled substances, and extramural birth. Informed parental consent was obtained before enrollment. Infants were continued in the study until discharged from the hospital or the development of stage IIA or greater NEC using Bell’s staging criteria.11Infants were allocated into the
in-tervention and control groups by blinded, random-draw, numer-ical assignment. People who were not involved in the study drew the numbers from an envelope that was kept in a locked drawer. Infants were assigned to both groups on the date of enrollment into the study. Before the initiation of feedings, attending physi-cians and caregivers were unaware of group assignment.
The attending physicians determined the timing of the initia-tion of feedings and of the infants’ discharge to home. When an infant had a venous or arterial umbilical catheter, feedings were begun 24 hours after its removal. Infants who were given indo-methacin for closure of a patent ductus arteriosus were not fed while receiving the drug and for 24 hours after the last dose was given. Waiting 24 hours after indomethacin therapy and removal of umbilical lines was considered standard of care at our facility during that period.
Expressed human milk (EHM) or standard formula of 20 kcal/30 mL (Enfamil; Mead-Johnson Nutritionals, Evansville, IN) was used for initiating feedings on the basis of recommendations of the formula company at the time.12In the intervention group,
feedings were initiated with 30 mL/kg per day of either Enfamil 20 cal/oz formula or EHM and advanced by 30 mL/kg per day until 150 mL/kg per day was reached. Feedings in the control group were initiated with 20 mL/kg per day of either Enfamil 20 cal/oz formula or EHM and advanced by 20 mL/kg per day until 140 mL/kg per day was reached. The last day of advancement in the control group was 10 mL/kg per day for a total of 150 mL/kg per day. All feedings were given as a bolus. Infants received intravenous fluids for the usual clinical indications until the en-teral intake was 120 mL/kg per day. After a volume of 150 mL/kg per day was reached, both groups were switched to 24 cal/oz Enfamil premature formula or EHM fortified with Human Milk Fortifier, 4 packages per 100 mL of EHM to make 24 cal/oz (Mead Johnson Nutritionals). Infants were returned to 20 cal/oz Enfamil or nonfortified human milk when they weighed⬃1800 to 1900 g. They were discharged from the hospital when they weighed ⬃2000 g and were medically stable.
The following conditions, defined a priori, were cause for dis-continuation of feedings: residual gastric contents of more than one third of the volume of the previous feeding, vomiting ⬎3 times in a 24-hour period not associated with eructation, bile-stained vomitus or residuals, distended abdomen, guaiac-positive stools not associated with a rectal fissure or trauma, or abnormal findings on abdominal radiographs. Pediatric radiologists without knowledge of group assignment interpreted all abdominal radio-graphs.
Infants who were ordered to have nothing by mouth (NPO) for ⬍24 hours had feedings resumed at the volume that they were receiving before they were order to receive NPO and were subse-quently advanced according to initial group assignment. Infants who were ordered to receive NPO for⬎24 hours had feedings resumed at their initial feeding volume (20 or 30 mL/kg per day) and then were advanced at those same volumes.
The primary outcome measure was days to get to full feedings. Sample size calculations were done using an␣⫽.05 and⫽.8, medium effect size, 2-sided hypothesis. Using these criteria, the minimum sample size needed to evaluate the effect of feeding advancement volume was 64 per group.13Recruitment was
con-tinued to include⬃25% more infants in both groups to allow for attrition as a result of removal from the protocol by the parents or attendings, transfer to another institution, and lack of compliance. Secondary outcomes were days to regain birth weight, days of intravenous fluids, length of hospital stay, and the incidence of feeding complications and NEC. Analysis of the data was done using Minitab version 12 and Epistat 5.3. Thettest was used to compare continuous variables with a normal distribution, whereas the Mann-Whitney test was used to analyze continuous variables that were not normally distributed. Categorical variables were compared using Fisher exact test.
RESULTS
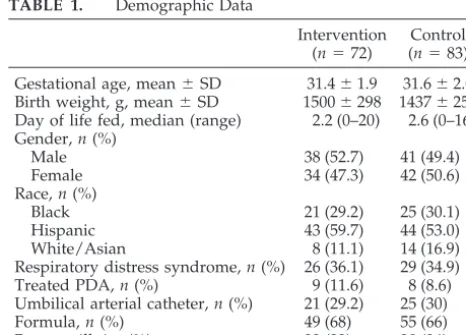
A total of 160 preterm infants were initially en-rolled, but 5 infants were withdrawn from the study. Two infants were found to meet exclusion criteria after enrollment; 1 had fetal alcohol syndrome and the second an in utero intestinal perforation and peritoneal calcifications diagnosed by radiograph. One infant who weighed 1920 g and was assigned to the lower feeding volume was withdrawn from the study by the attending after only a few feeds. An-other infant who was born to a human immunode-ficiency virus–positive mother was advanced at 50 mL/kg per day and developed NEC on day 12. The remaining 155 infants were analyzed on an intention-to-treat basis. Their characteristics are shown in Ta-ble 1. The groups were comparaTa-ble for gestational age, birth weight, and day of life when feedings were begun. Both groups had a preponderance of His-panic infants. There were similar numbers of boys and girls and of infants who were fed EHM (partial or full volume) in both groups. None of the other demographic variables was significantly different.
Infants who were fed and advanced at 30 mL/kg per day achieved full-volume feedings of 150 mL/kg per day and 120 kcal/kg per day before the control group (Table 2). The time to regain birth weight and to reach a weight of 2000 g was significantly shorter in the intervention group. Also, infants in the inter-vention group had significantly fewer days of intra-venous fluids. The median length of stay in the in-tervention group was 5 days shorter than the control group, but this difference only approached statistical significance (P ⫽.15).
Three of the 72 infants in the intervention group and 2 of the 83 infants in the control group devel-oped NEC, for an overall incidence of 3.2% (relative risk for NEC: 1.73; 95% confidence interval: 0.30 – 10.06;P ⫽ .66). The gestational age of the 3 infants who developed NEC in the intervention group was between 30 and 33 weeks, and the age of onset of NEC was between 5 and 8 days after birth. Two of them were receiving feedings of EHM before receiv-ing a diagnosis of NEC. Both control infants who developed NEC were of 29 weeks’ gestation, and
TABLE 1. Demographic Data
Intervention (n⫽72)
Control (n⫽83)
Gestational age, mean⫾SD 31.4⫾1.9 31.6⫾2.0 Birth weight, g, mean⫾SD 1500⫾298 1437⫾257 Day of life fed, median (range) 2.2 (0–20) 2.6 (0–16) Gender,n(%)
Male 38 (52.7) 41 (49.4)
Female 34 (47.3) 42 (50.6)
Race,n(%)
Black 21 (29.2) 25 (30.1)
Hispanic 43 (59.7) 44 (53.0) White/Asian 8 (11.1) 14 (16.9) Respiratory distress syndrome,n(%) 26 (36.1) 29 (34.9) Treated PDA,n(%) 9 (11.6) 8 (8.6) Umbilical arterial catheter,n(%) 21 (29.2) 25 (30) Formula,n(%) 49 (68) 55 (66) Breast milk,*n(%) 23 (32) 28 (34) PDA indicates patent ductus arteriosus.
* Partial or full volume.
NEC was diagnosed at 11 and 41 days after birth, after several days of full feedings with formula. At our institution, the incidence of NEC in preterm in-fants who weighed between 1000 and 2000 g and were not enrolled in the study during the same pe-riod was 4.1%.
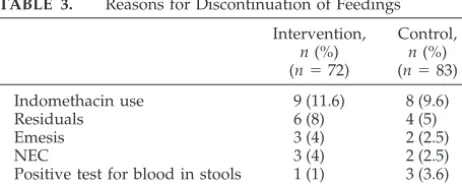
The reasons for discontinuation of feedings during the study are shown in Table 3. Indomethacin use was the most common cause for stopping feeds. Other complications were less frequent, and no dif-ferences between groups were detected.
DISCUSSION
Defining the best method for feeding preterm in-fants remains a challenging goal. These inin-fants often have feeding difficulties primarily because of imma-turity of their gastrointestinal system.1,3,6,14 It has been well established that inadequate provision of adequate nutrition in very low birth weight neonates often leads to suboptimal growth at discharge.15 De-spite the importance of this subject, many of the published studies regarding feeding practices have been based on retrospective data or have had a small sample size.2,4,8,9,16,17Several studies have indicated that early enteral feeding may stimulate the prema-ture intestinal tract and improve feeding tolerance, but systematic reviews examining the use of minimal enteral feedings or comparing early versus delayed initiation of progressive enteral feedings have been inconclusive.3,16–19One of the major concerns related to feeding premature infants is the occurrence of NEC. Although prematurity per se is the primary risk factor for NEC, a relationship of the rate of advancement of enteral feeding with NEC has been suggested, but causality has not been proved.4,8,9,20
In our study, the second largest controlled trial of feeding advancement in preterm infants, we showed that advancing feedings at a rate of 30 mL/kg per day is as safe as advancing at the rate of 20 mL/kg per day. Infants in the intervention group reached
full volume of feedings (150 mL/kg per day) and regained birth weight before control infants. In ad-dition, the low incidence of NEC in our study was comparable in both groups. Data from our study, that of the small trial of Book et al4and the largest trial to date reported by Rayyis et al, which included 185 infants,5were included in a systematic review by Kennedy et al.21These authors concluded that more rapid rates of advancing feeding volume result in a reduction in days to attain full enteral feedings and to regain birth weight but expressed concern about adopting this practice widely given the limited infor-mation regarding safety, particularly with regard to NEC. A recent study by Berserth et al20that included infants ⬍32 weeks’ gestation, compared feeding 20 mL/kg per day for 10 days and then advancing the feeding volume, to starting at 20 mL/kg per day and advancing daily by 20 mL/kg per day until a volume of 150 mL/kg per day was attained. The trial was stopped prematurely because the data safety com-mittee found an increased risk of NEC in infants who were advanced daily (10%) compared with those who had a period of minimal enteral feedings (1.4%). However, the mean gestational age and birth weight of infants in this trial was much less than in our study. Moreover, these authors reported that the in-cidence of proven NEC in their neonatal intensive care unit was 12%, which is higher than reports from other centers, including this report.20,22
The reasons for stopping feedings were uncom-mon in both groups from our study, as has been reported by others.6,7,20We chose to give all feedings as a bolus, which has also been shown to lead to full feedings earlier than administering them continu-ously using infusion pumps.23,24 We showed that infants who were advanced more rapidly had signif-icantly fewer days of intravenous fluids and went home ⬃5 days before the control infants. Although our study was not powered to determine significant differences in length of stay, both of these findings suggest that overall costs of neonatal care may be reduced by advancing feedings more rapidly in in-fants between 1000 and 2000 g.
Finding the best method to feed premature infants while minimizing complications is of utmost impor-tance. Most of the studies to date that have ad-dressed this critical aspect of neonatal care have taken place at a single institution. Thus, many ques-tions remain unanswered. Only a large, multicenter, prospective trial with a large enough sample size would be able to test adequately better ways of op-TABLE 2. Main Outcomes of the Study
Intervention, median (range)
(n⫽72)
Control, median (range)
(n⫽83)
PValue 95% CI for Difference in Medians Day of age
Full volume reached 7 (5–48) 10 (8–27) ⬍.01 ⫺3.00 to⫺2.00 Full calories reached 8 (5–52) 11 (9–31) ⬍.01 ⫺3.00 to⫺2.00 Birth weight regained 11 (3–26) 13 (5–34) ⬍.01 ⫺3.00 to⫺1.00 Weighed 2000 g 24 (11–63) 29 (13–75) .04 ⫺8.00 to 0.00 Length of stay, d 26 (11–111) 31 (12–190) .15 ⫺8.00 to 1.00 Days of intravenous fluids 6 (4–69) 8 (6–58) ⬍.01 ⫺3.00 to⫺2.00 CI indicates confidence interval.
TABLE 3. Reasons for Discontinuation of Feedings Intervention,
n(%) (n⫽72)
Control,
n(%) (n⫽83)
Indomethacin use 9 (11.6) 8 (9.6)
Residuals 6 (8) 4 (5)
Emesis 3 (4) 2 (2.5)
NEC 3 (4) 2 (2.5)
timizing enteral nutrition without increasing mor-bidity like NEC.
REFERENCES
1. Fletcher AB. Nutrition. In: Avery GB, ed.Neonatology. 4th ed. Philadel-phia, PA: JB. Lippincott; 1994:330 –356
2. LaGamma, EF, Ostertag, SG, Birenbaum H. Failure of delayed oral feedings to prevent necrotizing enterocolitis.Am J Dis Child.1985;139: 385–389
3. Berseth CL, Nordyke C. Enteral nutrients promote postnatal maturation of intestinal motor activity in preterm infants.Am J Physiol.1993;264: G1046 –G1051
4. Book LS, Herbst JJ, Jung AL. Comparison of fast and slow feeding rate schedules to the development of necrotizing enterocolitis.J Pediatr.
1976;89:463– 466
5. Rayyis S, Ambalavanan N, Wright L, Carlo WA. Randomized trial of “slow” versus “fast” feed advancements on the incidence of necrotizing enterocolitis in very low birth weight infants.J Pediatr.1999;134:293–297 6. Mihatsch WA, von Schoenaich P, Fahnenstich H, et al. The significance of gastric residuals in the early enteral feeding advancement of ex-tremely low birth weight infants.Pediatrics.2002;109:457– 459 7. Cobb BA, Carlo WA, Ambalavanan N. Gastric residuals and their
relationship to necrotizing enterocolitis in very low birth weight infants.
Pediatrics.2004;113:50 –53
8. Anderson DM, Kliegman RM. The relationship of neonatal alimentation practices to the occurrence of endemic necrotizing enterocolitis.Am J Perinatol.1991;8:62– 67
9. McKeown RE, Marsh TD, Amarnath U, et al. Role of delayed feeding and of feeding increments in necrotizing enterocolitis.J Pediatr.1992; 121:764 –770
10. Ballard JL, Khoury JC, Wedig K, Wang L, Eilers-Wlasman BL, Lipp R. New Ballard Score, expanded to include extremely premature infants.
J Pediatr.1991;119:417– 423
11. Bell MJ, Ternberg JL, Feigin RD, et al. Neonatal necrotizing enterocolitis, therapeutic decisions based upon clinical staging.Ann Surg.1978;187: 1–7
12. Mead Johnson Nutritionals Pediatric Products Handbook. Evansville, IN: Mead Johnson Nutritionals; 1993:16 –17
13. Lipsey MW. Design, sample size and alpha. In: Statistical Power for Experimental Research in Design Sensitivity. Newbury Park, CA, Sage Publications; 1990:122–146
14. Berseth CL. Gastrointestinal motility in the neonate. Clin Perinatol.
1996;23:179 –190
15. Ehrenkranz RA. Growth outcomes of very low-birth weight infants in the newborn intensive care unit.Clin Perinatol.2000;27:325–345 16. Stagle TA, Gross SJ. Effect of early low-volume enteral substrate on
subsequent feeding tolerance in very low birth weight infants.J Pediatr.
1988;113:526 –531
17. Berseth CL. Effect of early feeding on maturation of the preterm infant’s small intestine.J Pediatr.1992;120:947–953
18. Tyson JE, Kennedy KA. Minimal enteral nutrition for promoting feed-ing tolerance and preventfeed-ing morbidity in parenterally fed infants.
Cochrane Database Syst Rev.2000;(2):CD000504
19. Kennedy KA, Tyson JE, Chamnanvanikij S. Early versus delayed initi-ation of progressive enteral feedings for parenterally fed low birth weight or preterm infants. Cochrane Database Syst Rev. 2000;(2): CD001970
20. Berseth CL, Bisquera JA, Paje VU. Prolonging small feeding volumes early in life decreases the incidence of necrotizing enterocolitis in very low birth weight infants.Pediatrics.2003;111:529 –534
21. Kennedy KA, Tyson JE, Chamnanvanikij S. Rapid versus slow rate of advancement of feedings for promoting growth and preventing necro-tizing enterocolitis in parenterally fed low-birth-weight infants. Co-chrane Database Syst Rev.2000;(2):CD001241
22. Lemons JA, Bauer CR, Oh W, et al. Very-low-birth-weight outcomes of the NICHD Neonatal Research Network, January 1995 through Decem-ber 1996.Pediatrics.2001;107(1). Available at: www.pediatrics.org/cgi/ content/full/107/1/e1
23. Schanler RJ, Shulman RJ, Lau C, Smith EO, Heitkemper MM. Feeding strategies for premature infants: randomized trial of gastrointestinal priming and tube-feeding method.Pediatrics.1999;103:434 – 439 24. Dollberg S, Kuint J, Mazkereth R, Mimouni FB. Feeding tolerance in
preterm infants: randomized trial of bolus and continuous feeding.J Am Coll Nutr.2000;19:797– 800
BACK-ALLEY HIP REPLACEMENTS
“Voters yearning for the federal government to start rationing American health care might want to take note of a study just released by our neighbors up north. The Vancouver-based Fraser Institute yesterday published its 14th annual report on hospital waiting times in Canada. . . . Under Canada’s government-run health care monopoly, Fraser reports that the average wait for hospital treatment is 17.9 weeks. That’s the average over 12 specialties and 10 provinces. To take just 1 example, the projected wait for hip-replacement surgery in British Columbia is 52 weeks. . . . The waiting times have fueled Canada’s growing gray market in health care. Patients seeking to avoid the pain or inconvenience of long waits increasingly seek treatment in private clinics. . . . The government itself uses private clinics for Royal Canadian Mounted Police, provincial workman’s compensation cases and prison inmates. Thus the Canadian joke about the prisoner who asks his cellmate, ‘What are you in for?’ Answer: ‘Hip replacement.’ . . . What the Fraser survey demonstrates is that Canada’s universal health care system has created shortages that leave sick Canadians wanting. There are many things to admire about Canada, but medical care is not 1 of them.”
Wall Street Journal. October 20, 2004
Noted by JFL, MD
DOI: 10.1542/peds.2004-1232
2004;114;1597
Pediatrics
John W. Sparks and Fernando R. Moya
Judith Caple, Debra Armentrout, Valerie Huseby, Brenda Halbardier, Jose Garcia,
Advancement in Preterm Infants
Randomized, Controlled Trial of Slow Versus Rapid Feeding Volume
Services
Updated Information &
http://pediatrics.aappublications.org/content/114/6/1597
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/114/6/1597#BIBL
This article cites 20 articles, 4 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/nutrition_sub Nutrition
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2004-1232
2004;114;1597
Pediatrics
John W. Sparks and Fernando R. Moya
Judith Caple, Debra Armentrout, Valerie Huseby, Brenda Halbardier, Jose Garcia,
Advancement in Preterm Infants
Randomized, Controlled Trial of Slow Versus Rapid Feeding Volume
http://pediatrics.aappublications.org/content/114/6/1597
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2004 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 29, 2020 www.aappublications.org/news