4. Jaffe DM, Tanz RR, Davis AT, Henretig F, Fleisher G. Antibiotic admin-istration to treat possible occult bacteremia in febrile children.N Engl J Med.1987;317:1175–1180
5. Rothrock SG, Harper MB, Green SM, et al. Do oral antibiotics prevent meningitis and serious bacterial infections in children withStreptococcus pneumoniae occult bacteremia? A meta-analysis. Pediatrics. 1997;99: 438 – 444
6. Baraff LJ, Oslund S, Prather M. Effect of antibiotic therapy and etiologic microorganism on the risk of bacterial meningitis in children with occult bacteremia.Pediatrics.1993;92:140 –143
7. Harper MB, Bachur R, Fleisher GR. Effect of antibiotic therapy on the outcome of outpatients with unsuspected bacteremia.Pediatr Infect Dis J.1995;14:760 –767
Back to Sleep: Good Advice for Parents but Not
for Hospitals?
To the Editor.—
We read with interest the article by Hein and Pettit1reporting that some newborn nursery nurses in Iowa were advocating the side versus supine sleeping position. The authors expressed con-cern that mothers who observe this position being used in the hospital are more likely to place their infants on their sides at home. They also criticized the American Academy of Pediatrics (AAP) and the “Back to Sleep” (BTS) campaign by referencing a 1996 AAP statement and BTS brochure that listed side positioning as an “alternative” to back sleeping. Unfortunately, the criticism reflects the unavoidable lag time for manuscripts to be published. Since its organization in 1991, the AAP Task Force on Infant Sleep Position and SIDS has been very careful to avoid making recommendations that were not based on peer-reviewed data. Before 1996, the data regarding SIDS risk showed only a minimal advantage of supine positioning over side positioning for sleep. In one study comparing supine to side positioning, the 95% confi-dence limits of the odds ratios ranged from 1.15 to 6.78. Other studies showed no advantage. Side sleeping, however, was con-sistently shown to be safer than prone. Therefore, the Task Force recommended at that time that side was a “reasonable alternative” to fully supine. Since then, additional studies have been published that show more convincingly an advantage of supine over side positioning. Still, side positioning confers a substantially lower risk when compared with the prone position.
With these new data, the latest Task Force recommendations3 (published 1 month before the date that Hein and Pettit submitted their article but not referenced in their article) and the latest BTS brochure have removed the “reasonable alternative” statement and the picture demonstrating side positioning. Both documents do mention that side is safer than prone, because this is what the evidence has shown. But “Back is Best” is the primary message. It is of interest that annual survey data2have shown that public
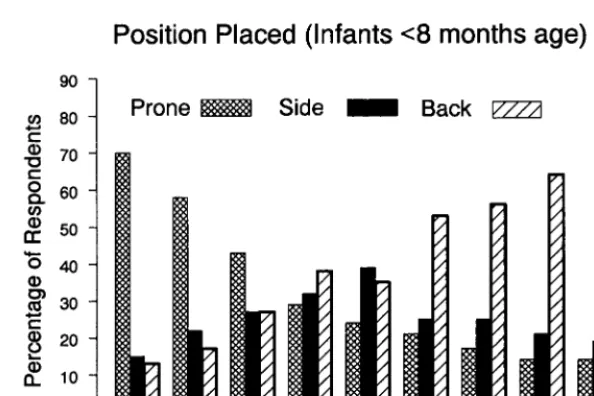
behavior has followed the data and the recommendations quite closely (Fig 1). Following the 1992 recommendation to simply “avoid prone,” there has been a steady decrease in prone posi-tioning, coincident with decreasing rates of SIDS. After the data supporting “back is best” were published, prone has continued to decrease and side has also progressively declined. We encourage clinicians to read the latest recommendations2and to distribute the most recent brochure. Copies of the public brochure may be obtained by calling 1-800-505-CRIB or by printing them from the Internet site: http://www.nichd.nih.gov/sids/sids.htm.
AAP Task Force on Infant Sleep Position and SIDS
John Kattwinkel, MD, Chairperson John G. Brooks, MD
Maurice E. Keenan, MD Michael Malloy, MD
Consultant
Marian Willinger, PhD
REFERENCES
1. Hein HA, Pettit SF. Back to sleep: good advice for parents but not for hospitals?Pediatrics.2001;107:537–539
2. Annual survey data provided by National Institute of Child Health and Human Development, Bethesda, MD
3. Kattwinkel J, Brooks J, Keenan ME, Malloy M, Willinger M, Scheers NJ. Changing concepts of sudden infant death syndrome: implications for the sleeping environment and sleep position.Pediatrics.2000;105: 650 – 656
Circumcisions: Again
To the Editor.—
The flurry of recent articles and commentaries addressing po-tential medical benefits of circumcision1– 4provide much food for thought. I agree with the Academy’s Task Force on Circumcision5 that the benefits of circumcision are not sufficient to recommend it routinely, that parents should be given accurate and unbiased information, and that procedural analgesia should be provided. It is unfortunate that the coverage in the lay press suggested that the AAP had changed its position to one opposing circumcision. A better headline would have read “AAP Task Force notes benefits, risks of circumcision; urges anesthesia.”
Nonetheless, I agree with Schoen, Wiswell, and Moses4that the language used by the Task Force is partly responsible for this misunderstanding. The Task Force statement says: “Existing sci-entific evidence demonstrates potential medical benefits; however,
Fig 1. Positions in which infants were placed for sleep.
these data are not sufficient to recommend routine neonatal cir-cumcision. In circumstances in which there are potential benefits and risks yet the procedure is not essential to the child’s current well-being, parents should determine what is in the best interests of the child.”
Although it is true that the benefits are “potential” in that most uncircumcised males will not develop conditions circumcision would have prevented, this is not the reason not to recommend it. We routinely recommend immunizations, car seat use, and safer sex, even though their benefits and risks are “potential” in the same way as those of circumcision and they also are “not essential to the child’s current well-being.”
The key difference between circumcision and preventive inter-ventions that the AAP does recommend is neither the quality of the evidence nor the absolute magnitude of the benefits; it is the nature of the intervention. Circumcision involves surgery to re-move a natural part of the boy’s body and alter its appearance forever. It is a procedure with considerable nonmedical signifi-cance in many cultures. Thus, although there are definite medical benefits that seem to outweigh the medical risks, I think it is appropriate for the AAP to refrain from routinely recommending it, because it is not solely a medical decision.
This being said, it is important not to exaggerate the known benefit of preventing urinary tract infections (UTIs). The degree to which urinary tract infections in infancy lead to hypertension and end-stage renal disease (ESRD) in adulthood is not known, but is almost certainly less than suggested by combining the results of the long-term studies cited by Wiswell.1Using those figures, if 2.2% of uncircumcised boys got UTIs and 44% of them developed renal scarring and 10% of those with scarring developed ESRD over the next 30 years, the 30-year risk of ESRD from infancy would be about 2.2%⫻44%⫻10%, or about 1 in 1000. In fact, according to the US Renal Data Service, ESRD in children younger than 20 years old has an annual incidence of only about 13 million per year, of which only about 2.7% is attributed to chronic pyelo-nephritis or reflux nephropathy.6Over the next 25 years the an-nual incidence rises to 109 million per year, but the proportion attributed to chronic pyelonephritis or reflux nephropathy de-clines to 0.7%. Even if all the cases in males were attributable to UTIs in those who were uncircumcised, the 45-year risk would still be an order or magnitude lower than would be projected from the numbers cited by Wiswell.
Thomas B. Newman, MD, MPH Department of Epidemiology
University of California, San Francisco San Francisco, CA 94143
REFERENCES
1. Wiswell TE. The prepuce, urinary tract infections, and the conse-quences.Pediatrics.2000;105:860 – 862
2. Schoen EJ, Colby CJ, Ray GT. Newborn circumcision decreases inci-dence and costs of urinary tract infections during the first year of life. Pediatrics.2000;105:789 –793
3. American Academy of Pediatrics, Task Force on Circumcision. Circum-cision debate.Pediatrics.2000;105:641– 642
4. Schoen EJ, Wiswell TE, Moses S. New policy on circumcision-cause for concern.Pediatrics.2000;105:620 – 623
5. American Academy of Pediatrics, Task Force on Circumcision. Circum-cision policy statement.Pediatrics.1999;103:686 – 693
6. US Renal Data Service.Annual Data Report. 1999, Chapter 2: Incidence and Prevalence of ESRD. Available at: http://www.usrds.org/chapters/ ch02.pdf
To the Editor.—
The 1999 Circumcision Policy Statement by the Task Force on Circumcision of the American Academy of Pediatrics does not recommend routine neonatal circumcision. Notwithstanding, the need for routine neonatal circumcision continues as a controver-sial topic in the American pediatric literature. We read with inter-est the study by Schoen et al1and the commentary by Wiswell2on circumcision; both authors are long-time proponents of routine neonatal circumcision and have contributed much to this debate. Wiswell continues to discuss the risk of end-stage renal disease (ESRD) as a justification for routine neonatal circumcision.2 Cur-rent research does not support this position.3–7
Sreenarasimhaiah and Hellerstein3 reported on 102 patients with ESRD assessed in Kansas City, Missouri, between 1986 and 1995. Urinary tract infection (UTI) was considered an important contributing factor(our italics) in only 1 patient!3
Wennerstro¨m et al4from Goteborg, Sweden, a center that has provided decades of excellent research on UTI, recently reported a long-term prospective follow-up on 1221 children (232 boys) with a first recognized symptomatic UTI during the years 1970 and 1979. Circumcision is not common in Sweden. Only 21 boys were found to have scarring and, of these, 18 (86%) were consid-ered to have primary or congenital scarring, rather than acquired resulting from UTI. The authors note that “chronic renal failure caused by pyelonephritic renal scarring in Swedish children has decreased during the last few decades. In fact, in a population of 8.5 million, no child has been registered in this category during the last decade.”4Based on Swedish epidemiologic data, we estimate that⬎500 000 circumcisions are necessary to prevent end-stage renal failure in one boy.5–7
We suggest it is time to put the specter of ESRD as a conse-quence of failure to circumcise into the history books as an anach-ronism previously fed on well-intentioned speculation but less enlightened data.
Wm. Lane M. Robson, MD, FRCP(C), FAAP, FRCP (Glasgow)
Pediatric Nephrology The Children’s Hospital Greenville Hospital System Greenville, SC 29605-4490
Robert S. Van Howe, MD Department of Pediatrics
Marshfield Clinic—Lakeland Center Minocqua, WI
REFERENCES
1. Schoen EJ, Colby CJ, Ray GT. Newborn circumcision decreases inci-dence and costs of urinary tract infections during the first year of life. Pediatrics.2000;105:789 –793
2. Wiswell TE. The prepuce, urinary tract infections, and the conse-quences.Pediatrics.2000;105:860 – 862
3. Sreenarasimhaiah S, Hellerstein S. Urinary tract infections per se do not cause end-stage kidney disease.Pediatr Nephrol.1998;12:210 –213 4. Wennerstro¨m M, Hansson S, Jodal U, Stokland E. Primary and acquired
renal scarring in boys and girls with urinary tract infection.J Pediatr. 2000;136:30 –34
5. Esbjo¨rner E, Aronson S, Berg U, Jodal U, Linne T. Children with chronic renal failure in Sweden 1978 –1985.Pediatr Nephrol.1990;4:249 –252 6. Esbjo¨rner E, Berg U, Hansson S. Epidemiology of chronic renal failure
in children: a report from Sweden, 1986 –1994.Pediatr Nephrol.1997;11: 438 – 442
7. Helin I, Winberg J. Chronic renal failure in Swedish children. Acta Paediatr (Scand).1980;69:607– 611
To the Editor.—
I was intrigued by the article in the April 2000 issue ofPediatrics entitled “Circumcision and Urinary Tract Infections During the First Year of Life” and its accompanying editorial. I have another study in which you may be interested entitled “Do Moustaches Cause Staphylococcal Pharyngitis: (Implications for UTIs and Cir-cumcision).
Abstract. 1000 teenage males with fever had throat cultures performed; 500 had moustaches and 500 did not. Culture tech-nique included swabbing the throat, first running the swab through the moustache (if present).
Results.Statistically significant differences in staphylococcal re-covery rates were seen in those with moustaches, with a 20-fold increase in culture-positive “pharyngitis” seen in those with moustaches.
Conclusion.Moustaches cause a drain on our medical expenses, causing unnecessary episodes of fever and potentially more seri-ous sequelae.
This farce is simply to illustrate the point that the presence of the foreskin can make statistical analysis of culture results
diffi-LETTERS TO THE EDITOR 523
at Viet Nam:AAP Sponsored on August 30, 2020 www.aappublications.org/news
cult, if these cultures are derived using a technique potentially contaminated by the very foreskin implicated in the conclusions. I believe that good evidence exists to support the claim that the foreskin allows bacterial adherence, and so the concentration of bacteria locally will be higher in the region compared with a circumcised individual. Going through this region to obtain cul-tures used to make a diagnosis of urinary tract infection (UTI) is an obvious complicating factor in any study looking at potential infectious consequences of the presence of the foreskin.
I would be very interested indeed in reviewing a study of UTI and circumcision in which all of the culture data are collected via suprapubic aspiration, and in which the presence of inflammatory changes in the urinalysis (white cells, protein) are used in con-junction with culture results to define a UTI. I have not been able to find a large study that satisfies these criteria. Realistically, to state that the foreskin harbors more bacteria than a circumcised penis, and then to go through the region for culture collection, is asking for technical difficulties in data interpretation.
Mark F. Mangano, MD Radnor, PA 19087
In Reply.—
Dr Newman addresses the problematic semantics of the 1999 AAP Circumcision Task Force Statement. If similar wording were applied to routine health care (“not essential to a child’s current well being”), virtually all preventive medicine strategies would be eliminated (immunizations, etc). Although there are ample data detailing the short-term consequences (bacteremia, renal scarring, etc) of urinary tract infection (UTI), long-term data concerning the subsequent development of hypertension and end-stage renal dis-ease (ESRD) are scant. Published information varies considerably. Unfortunately, there are no large, comprehensive, prospectively accumulated databases that denote the incidence of ESRD after UTI. Although Newman quotes only 2.7% of ESRD in children to be attributable to the adverse effects of such infections, others suggest that as much as 22% to 43% of ESRD may be attributable to pyelonephritis.1–3 Similarly, although Newman states that among adults aged 20 to 45 years with ESRD the proportion attributed to childhood infection is only 0.7%, others put the number as high as 13% to 21%.1,4
Dr Mangano intimates that all studies assessing UTI in uncir-cumcised males have erroneously demonstrated infections when there were none present. He speculates that urine culture speci-mens obtained via bladder catheterization are contaminated by uropathogenic organisms. His speculation is erroneous. The latter method of urine collection is reliable in both circumcised and uncircumcised boys. Isolation of multiple organisms, as well as colony counts ⬍10 000 to 50 000 colony-forming units/mL, are typical manifestations of contaminated urine cultures. These were not the findings in the 15 studies I referenced in my commentary. I remind Dr Mangano that when one obtains urine via bladder catheterization in uncircumcised boys, it is not obtained “through” the prepuce. Rather, the distal glans and urethral me-atus are initially gently exposed and aseptically cleaned.5A sterile catheter is then directly inserted into the urethral meatus, with care taken not to touch surrounding tissue. Apparently, Dr Man-gano is unfamiliar with the largest investigation to date in which suprapubic bladder aspiration was the preferred method of urine collection.6In that study, of 468 uncircumcised boys with UTIs, 92% of the urine culture specimens were obtained by suprapubic aspiration. Additionally, as most pediatricians recognize, urinal-ysis findings are notoriously unreliable in helping to substantiate UTIs in infants. The “50-50 rule” is a well-known mnemonic in this regard: 50% of young children with UTIs do not have increased numbers of white blood cells in their urine, while 50% of those with elevated white blood cell levels in their urine do not have UTIs.
Robson and Van Howe assert that ESRD is an exceedingly rare consequence of UTI that pediatricians should ignore. Unfortu-nately, they choose to reference only a few selected publications concerning childhood chronic renal failure (CRF), while they ig-nore the substantial literature attributing adult CRF to childhood UTI. Interestingly, in the very references they do provide, Sreenarasimhaiah and Hellerstein7 note that the severe conse-quences of UTI (hypertension and ESRD) are late events that often
manifest 20 years or more after the initial UTI. Helin and Winberg8 similarly acknowledge the role of childhood UTI as the precursor of hypertension and CRF in adults. Additionally, Wennerstro¨m and colleagues9 comment that in most parts of the world, the detection rate of UTI in small children is low (ie, few such infec-tions are diagnosed and treated), while the long-term conse-quences of these infections are considerable. In the recent publi-cation of Craig and colleagues,10 their review of the world literature suggests that pyelonephritis is the second leading cause of ESRD in childhood, with approximately 20% to 25% of ESRD cases being attributable to infection.
Esbjo¨rner et al11describe the remarkable differences in ESRD attibutable to pyelonephritis in Sweden compared with that of multiple other countries. The International Reflux Study in Chil-dren in the 1980s revealed that 3 times as many boys with CRF attributed to UTI were enrolled from Europe compared with the United States (J. Duckett, personal communication). I know of no reason for this difference other than the higher circumcision rates in the United States and the 10- to 20-fold decreased risk for UTI among these boys. The major prerequisites for renal scarring are infection and inflammation, not reflux. Wennerstro¨m et al’s data9 are from individuals with UTIs that occurred more than 20 years ago, long before the widespread use of nuclear scanning to eval-uate such children. The latter techniques are several times more likely to reveal renal scarring than were the intravenous pyelog-raphy studies described by these authors. Thus, Robson and Van Howe mislead the readers by using the Wennerstro¨m data to infer that most renal scarring in males is congenital in nature. Further-more, they misrepresent my commentary, stating that it is a con-tinuation of efforts using the risk of ESRD to justify routine neo-natal circumcision. I have never suggested ESRD should be the basis for routine neonatal circumcision. I have only discussed it as one of many potential sequelae of childhood UTI.
The developing kidney of early childhood is much more likely to be injured as a consequence of UTI compared with later in life. The current published data12assessing the incidence of long-term consequences of childhood UTIs are worrisome, noting relatively high rates of altered renal function, hypertension, and ESRD. What is clearly needed are large prospective trials in which co-horts of children with UTIs are followed well into adulthood to assess for sequelae of such infections.
Thomas E. Wiswell, MD Department of Pediatrics SUNY Stony Brook
Stony Brook, NY 11794-8111
REFERENCES
1. Chantler C. Kidney diseases in children. In: Schrier RW, Gottschalk CW, eds. Diseases of the Kidney. 5th ed. Boston, MA: Little, Brown and Company; 1993:2394 –2403
2. Batisky D. Pediatric urinary tract infections.Pediatr Ann.1996;25:266, 269 –272, 274, 276
3. Altemeier WA. A backward look at urinary tract infections.Pediatr Ann. 1996;25:255–256, 268, 280
4. Shaw KN, Gorelick MH. Urinary tract infection in the pediatric patient. Pediatr Clin North Am.1999;46:1111–1124
5. Sanchez JL, Walsh RF. Procedures in the evaluation of the febrile pediatric patient.Pediatr Ann.1996;25:686 – 692
6. Wiswell TE, Roscelli JD. Corroborative evidence for the decreased in-cidence of urinary tract infections in circumcised male infants. Pediat-rics.1986;78:96 –99
7. Sreenarasimhaiah S, Hellerstein S. Urinary tract infections per se do not cause end-stage kidney disease.Pediatr Nephrol.1998;12:210 –213 8. Helin I, Winberg J. Chronic renal failure in Swedish children. Acta
Paediatr Scand.1980;69:607– 611
9. Wennerstro¨m M, Hansson S, Jodal U, Stokiland E. Primary and ac-quired renal scarring in boys and girls with urinary tract infection. J Pediatr.2000;136:30 –34
10. Craig JC, Irwig LM, Knight JF, Roy LP. Does treatment of vesicoureteric reflux in childhood prevent end-stage renal disease attributable to reflux nephropathy?Pediatrics.2000;105:1236 –1241
11. Esbjo¨rner E, Aronson S, Berg U, Jodal U, Linne T. Children with chronic renal failure in Sweden, 1978 –1985.Pediatr Nephrol.1990;4:249 –252 12. Wiswell TE. The prepuce, urinary tract infections, and the
conse-quences.Pediatrics.2000;105:860 – 862
2001;108;522
Pediatrics
Thomas B. Newman
Circumcisions: Again
Services
Updated Information &
http://pediatrics.aappublications.org/content/108/2/522.2
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/108/2/522.2#BIBL
This article cites 21 articles, 10 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
at Viet Nam:AAP Sponsored on August 30, 2020 www.aappublications.org/news
2001;108;522
Pediatrics
Thomas B. Newman
Circumcisions: Again
http://pediatrics.aappublications.org/content/108/2/522.2
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2001
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 30, 2020 www.aappublications.org/news