PEDIATRICS (ISSN 0031 4005). Copyright © 1990 by the American Academy of Pediatrics.
By 1915 the concept of caloric feeding had be-come almost universal in America but there were
still dissenters who believed that infants did not
thrive as well on pasteurized milk as they did on raw milk. The early meetings of the American Pediatric Society contained many reports about the pros and cons of raw as opposed to pasteurized milk; some believed that infants fed raw milk had far less chance of developing scurvy than those fed pasteurized milk.6
During the first two decades of this century there appeared a number of “new milks” for infant feed-ing. Among these were buttermilk, protein milk (Eiweissmilch), butter-flour mixture, and soybean and acidified milks. Each of these had their advo-cates but all were superseded by the evaporated milk formula, described by Marriott and Schoenthal7 in 1929. During the period from 1930 to 1960 evaporated milk became the most widely accepted and versatile milk for infant formulas. By
1960 it was estimated that 80% of bottle-fed infants in the United States were fed evaporated milk or some prepared milk feeding marketed in evaporated form.
The mid-1970s saw a decrease in the number of infants fed evaporated milk formulas, from approx-imately 45% in 1958 to less than 5% by 1978, and a concomitant increase in those receiving prepared milk formulas (humanized milk), rising from ap-proximately 28% in 1958 to more than 85% by 1980. Most of these prepared products are pur-chased in the form ofconcentrated liquid (133 kcal/ 100 mL) formulas.8
Although the long and difficult road to develop
scientifically balanced milk formulas has made the mechanics of infant feeding so simplified, neverthe-less certain problems still remain that occasionally challenge the physician in the feeding of infants. For this reason, the American Academy of Pediat-rics and several other professional medical groups have issued statements against infant formula ad-vertisements on television, in magazines, and in mailed coupon offers.’ The infant’s health care should not be guided by the television set but by the health care professional.
REFERENCES
THOMAS E. CONE, JR, MD
Department of Medicine The Children’s Hospital Boston, Massachusetts
1. Feeding your baby: a word to the TV-wise. Parents Curr. 1990;4:1
2. Cone TE Jr. History of American Pediatrics. Boston, MA: Little-Brown; 1979:112-114, 138-139
3. Meigs AV. Milk Analysis and Infant Feeding. Philadelphia, PA: Blakiston; 1885
4. Rotch TM. An historical sketch of the development of percentage feeding. NY Med J. 1907;85:532-546
5. Rubner M, Heubner 0. Die Nat#{252}rliche Ernahrung eines S#{228}uglings.J Biol. 1898;36:1-18
6. Faber HK, McIntosh R. History of the American Pediatric Society. New York, NY: McGraw-Hill; 1966:94
7. Marriott WM, Schoenthal L. An experimental study of the use of unsweetened evaporated milk for the preparation of infant feeding formulas. Arch Pediatr. 1929;46:135-140 8. Cone TE Jr. 200 Years of Feeding Infants in America.
Columbus, OH: Ross Laboratories; 1976:87-89
Measles
One More
Time
Although measles vaccine has been licensed for more than a quarter of a century, we have failed to eradicate the disease. It appeared as though we might be approaching this goal in 1983 when only
1497 cases were reported. In 1989, however, we had
approximately 17 000 cases. Prior to this there were a series of “miniepidemics” in 1971, 1976, and 1986, occurring at increasing intervals each with fewer cases than the previous one (Fig 1).’ The epidemic of 1989 was a clear departure from this pattern. One of the responses was to recommend a routine two-dose schedule of measles vaccine.
It is important to evaluate what happened in 1989 to understand why the epidemic occurred if
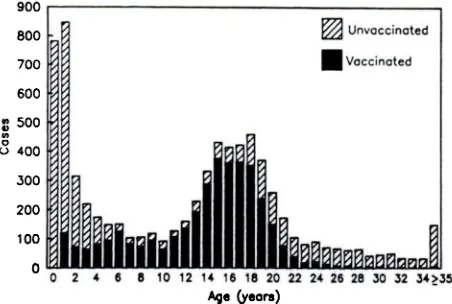
we are to prevent such outbreaks in the future. There appeared to be two groups that were most affected: preschoolers who were largely unimmun-ized and those 15 to 19 years of age, most of whom were immunized (Fig 2).2 In 1989, the younger group had a higher attack rate and suffered greater morbidity, 69% of the deaths vs none. Cases in the older group, however, were very disruptive of school routines. The two-dose strategy addresses the latter group.
As in the past,’ the focality of the 1989 epidemic was notable. Twenty-three states accounted for 96% of the cases with California, Texas, Ohio, and
Illinois alone accounting for about two thirds.
Dur-ing the first half of 1989, 31.9% of the cases
1.000
900
. 800
.- 700
v, 600
500
p400
300
0.
200
100
§15
080 82 4 86 88
YEM
I
-1 I
II I I I Fl ii
I
Fig I. Reported measles cases-United States, 1950-1989 (provisional data).’
Unvoccinoted
U
VaccinatedL
LL
2 4 6 8 10 12 1, 15
Age (years)
Fig 2. Age distribution of measles patients, by vaccine status-United States, based on first 26 weeks of 1989 (provisional data).
In 1989 there were approximately four to six
times the number of cases of measles in Mexico as
in 1988. Some of the hardest hit Mexican states were on the US border. Tamaulipas had both a
larger number of cases and a high attack rate. It
shares a busy border crossing with Cammeron and
Hidalgo Counties in Texas. Theirs were among the
highest measles rates in the state. It is probably no
coincidence that during the first half of 1989, 60%
of US cases were reported from Texas and Califor-nia.2 In 1988, a Hispanic preschooler was 12.6 times
as likely to get measles as a non-Hispanic white
and 3.6 times as a Black child of the same age in
Los Angeles.3 In 1989, 44% of cases in Houston and
59% of measles patients in Los Angeles were
His-panic children.
The cases among school attendees are disturbing because there are now laws requiring immunization as a condition for attendance in all states. Despite this, 27% of the school children who contracted
measles during 1989 were unimmunized.2 States
vary in the stringency of their enforcement and their immunization requirements. Idaho, for in-stance, required proof only for entry to
kindergar-ten through fifth grade. What is more unsettling is
the finding that outbreaks have occurred in schools
with 98% or more of the enrollees with records of
immunization.4’5 Although, the recommendations
of the Immunization Practices Committee state “A
parental history of vaccination, by itself, is not
considered adequate documentation. A physician
should not provide an immunization record for a
patient unless s/he has administered the vaccine or
has seen a record that documents vaccination,”6
some documentation may be faulty. Of concern,
however, is that there may have been loss of
vac-cine-induced immunity or failure to immunize suc-cessfully. A second dose of vaccine would be ex-pected to reduce the number of the unprotected for whatever reason.
Although the incidence of measles does not
in-crease sharply in school-aged children until 15 years
of age (Fig 2),2 ie, those immunized prior to 1975,
one recommendation is to reimmunize as early as
school entry. The logistical advantage of this
rec-ommendation, particularly in the public sector, is
obvious. On the other hand, it will not immediately
have a direct impact on the cases occurring in the
15- to 19-year-old group. In addition, there are
several lines of evidence to suggest that the risk of
measles in those immunized in the seventies may be far greater than those immunized more recently.
Thus, the advantage of reimmunizing 5-year-old
children might be considerably less than giving
measles vaccine to those immunized in the
seven-ties. Indeed, serologic studies5’7 of children who
were vaccinated in the eighties suggest a success
rate of close to 99%. Our laboratory, using the same
serology (5), found that 95% of those immunized earlier were seropositive. In addition, the risk of measles in school outbreaks was found to be greater in those immunized prior to 1977 or 1979 than later.8 Finally, the incidence of measles and the number of cases in vaccine recipients was lower in
There have been several alternative explanations of why measles risk increases in older school chil-dren. There is greater mobility in middle and high schools and opportunity for exposure as compared with lower grades where children are more likely to remain in one room. Social events outside school are more frequent. Some children have been said to attend these while ill so as not to miss them.9 One of the most disconcerting possibilities is that
vac-cine-induced immunity has waned. According to
one study,’#{176}5% of children who seroconverted later contracted measles. Confirmation of this observa-tion is vital. Evidence that the risk of measles increases as the interval since immunization in-creases is equivocal.’
The cost of a two-dose program started at school
entry to prevent cases 10 years hence would be
considerable. Given the periodicity of measles out-breaks, it is preferable to estimate cost for a decade of prevented cases rather than for one “bad year.” A two-dose strategy would prevent cases in school children, not in preschoolers. If one had put a two-dose schedule in place in 1980 and the second dose produced no failures, approximately 20 000 to 25 000 cases that occurred during the eighties in school-aged children would have been prevented. If 3.5 million children were reimmunized annually with measles-mumps-rubella vaccine purchased by Centers for Disease Control at the current price of about $16 per dose, approximately one-half billion dollars would have been spent for vaccine alone. The bonus would be prevention of some cases of rubella and mumps. On the other hand, costs other than vaccine, eg, administration of vaccine, are not included. Finally, the Centers for Disease Control price is much lower than that of the private sector which would presumably perform about half of the reimmunizations.
One of the reasons for a two-dose schedule is the cost of outbreak control in schools and the disrup-tive effect of these outbreaks. It is certain that the frustration experienced in outbreak control also is a contributing factor. Hundreds of thousands of dollars are expended in efforts that often have less than a dramatic impact on terminating these out-breaks.9 It is clear that the number of large
out-breaks are few but account for a substantial
pro-portion of the total number of cases.2” Most af-fected schools have had attack rates of 1% to
3#{149}5%#{149}4.5.912 In at least one community in which no
organized effort was made to reimmunize, the at-tack rates in the three affected schools were 0.5%, 1.8%, and 3#{149}4%#{149}5It appears that less than a “total
response” to each introduction of measles into a
school might be appropriate.
In some states, multiple school outbreaks have been observed.1’ What is sorely needed are criteria
to predict which introductions are likely to be small and self-limited and which are likely to lead to continued spread. Unfortunately, efforts to identify criteria for an appropriate response have been un-successful.” Thus, the type of response required for each introduction cannot be predicted. Ideally, one would prefer to identify these responses prior to the introduction of measles into the community. In any case, a two-dose schedule with the second dose given at school entry would not impact on the cost of control of school outbreaks for about a decade if the current pattern prevails (Fig 2), ie, that the highest attack rate in schools is in the 15-to 19-year-old group. The cost of control of out-breaks during the next decade would be added to the cost of a second dose of measles vaccine.
A strategy of immunizing 12-year-old children would have a more immediate impact on the 15- to
19-year-old group, the group with the highest mci-dence of measles except for the preschool children.2 The implementation of a reimmunization program, particularly in the public sector, would be very difficult and expensive. The threat of excluding from school those who did not comply, as is used at school entry, might well accelerate the rate of drop-outs in inner city schools.
Although only 9% of cases in 1989 occurred in institutes of higher learning, disruption of normal activities created a great deal of notoriety, particu-larly when cancellation of sporting events has been involved. In 1983 the American College Health Association adopted a Preadmission Immunization Policy recommending immunization against mea-sles and rubella.’2 Continuing outbreaks in insti-tutions of higher learning attest to the lack of implementation of this policy. Some states have passed laws requiring evidence ofprotection against measles as a condition of attendance at these insti-tutions.
Although outbreaks in educational institutions
have rarely involved more than 1% to 3.5% of students, they have been more disruptive and at-tracted greater notoriety that cases among pre-schoolers. Cases in the latter have been at least as numerous and produced more morbidity.” The
provision data for 1989 indicate that 69% of the
deaths occurred in preschools and 29% occurred in infants less than 1 year of age.
against measles.” Although we focus on a two-dose strategy to address perhaps 1% to as many as 5% of unprotected students in educational institutions, there exists a much larger unprotected preschool group. The latter presents two problems: those who
are too young to immunize and those who should
have received measles vaccine and did not.
There is an obvious advantage to earlier
immu-nization, viz, that younger children are protected
against disease. There also is a less obvious one,
and that is that older children may be less likely to be brought back for immunization. Children in a prepaid health program were 10% more likely to be
immunized against measles by 2 years of age if they
were scheduled for immunization at 12 rather than
15 months of age. By comparison, no difference was
found in a public health clinic. Of the latter,
how-ever, 85% to 90% were described as “regular attend-ees.” Among those identified as “irregular
attend-ees,” only 20% of those scheduled for 15 months
and 30% scheduled for 12 months were immunized
by 2 years ofage.’3 The study does not include those “irregular attendees” who may have dropped out
prior to 12 months of age. It is likely that if
im-munization against measles could be accomplished at 6 months of age, a larger proportion of preschool
children would receive vaccine. Results of the
eval-uation of the Edmonston-Zagreb strain of measles vaccine in Mexico first appeared in 1984. These revealed that 6-month-old infants could be
success-fully immunized.’4 Initial studies in the United
States are about to begin. If the effectiveness is
confirmed, this vaccine would protect younger chil-dren and immunize against measles at an age when babies probably are more likely to return for mea-sles vaccine. The availability of such a vaccine in Mexico, moreover, could decrease the importation of both measles patients and susceptible children.
For the present, we still need to achieve a better immunization rate in preschool children. Every en-counter in a health care facility must be considered an opportunity to immunize all family members against measles. The practice of reappointing these
persons to immunization clinics should no longer
be acceptable. The provision of vaccine by govern-mental agencies to local jurisdictions should be made contingent on eliminating barriers to immu-nization of hard-to-reach groups. Innovative meth-ods of getting children immunized must be encour-aged and rewarded.
There appear to be two major targets of preven-tion-preschool cases and school-based cases. A two-dose schedule might address the latter. It would not have impact on the more difficult problem of
measles in preschoolers. The low immunization
rates in inner cities where epidemics have afflicted this group” probably reflect the fact that during
interepidemic periods immunization has a rela-tively low priority. Motivation to sustain immuni-zation during these periods must be increased. It is much easier to immunize during an epidemic than when there has been no measles in the community for several years. If we are unable to sustain high levels of immunization during interepidemic pe-nods, the pattern of measles outbreaks predicted previously,’5 ie, smaller outbreaks at increasing in-tervals (Fig 1), will have interposed large outbreaks as we are now experiencing. The unprotected young in the inner cities are like a tinderbox waiting to be ignited by sparks over which we have little control at the current time.
A two-dose strategy, if the failure rate in measles vaccine at the present time is only 1%, could elim-mate approximately 35 000 susceptible persons, ie, potential measles patients, each year. It is clear, however, that there are finite resources available and these should be used in a manner that is likely to most effectively reduce the risk of measles. Col-lege outbreaks get the most attention. School out-breaks cause disruption of routines and parental
loss of wages. Preschool outbreaks cause the
great-est number of deaths and complications.
ACKNOWLEDGMENTS
PHILIP
A.
BRUNELL, MDPediatric Infectious Diseases Ahmanson Pediatric Center Cedars-Sinai Medical Center Los Angeles, CA
I thank Drs W. Orenstein, N. Saldana, R. Feigen, L. Dales, and S. Waterman, and E. F. Mihalek and W. J. Hodgson for generously providing data that was included in this commentary.
REFERENCES
1. Orenstein WA, Markowitz LE, Hersh BS, Preblud SR, Hinman AR. The elusiveness of measles elimination: ten years and still counting. In: Centers for Disease ControL Proceedings ofthe 23rd National Immunization Conference. 1989;67-73
2. Measles-United States, First 26 Weeks, 1989. MMWR.
1989;38:863-872
3. Measles-Los Angeles County, California, 1988. MMWR.
1989;38:49-57
4. Nkowane BM, Bert SW, Orenstein WA, Baltier M. Measles outbreak in a vaccinated school population: Epidemiology, chains of transmission and the role of vaccine failures. Am
J Pub Health. 1987;77:434-438
5. Gustavson TL, Brunell PA, Lievens AW, et al. Measles outbreak in a “fully immunized” secondary school popula-tion. N Engl J Med. 1987;316:771-774
6. Vaccine Usage: MMWR measles prevention: Recommen-dations ofthe Immunization Practices Committee. MMWR.
1989;38:6-11
PEDIATRICS (ISSN 0031 4005). Copyright © 1990 by the American Academy of Pediatrics.
Am J Epidemiol. 1989;129:173-182
8. Measles-United States, 1988. MMWR. 1989;38:35 9. Davis RM, Whitman ED, Orenstein, WA, et al. A persistent
outbreak of measles despite appropriate prevention and control measures. Am J EpidemioL 1987;126:438-449
10. Mathias RG, Meekison WG, Arcand TA, Schechter MT. The role of secondary vaccine failures in measles outbreaks. Am J Pub Health. 1989;74:475-478
11. Markowitz LE, Preblud SR, Orenstein WA, et al. Patterns of transmission in measles outbreaks in the United States,
1985-1986. New EngI J Med. 1989;320:75-81
12. Measles on College Campuses-United States, 1985.
MMWR. 1989;34:445-449
13. Sherrod JL, Kane R, Cherry JD, Fricker J, Maples K. Effect of timing of measles vaccination on compliance with im-munizations during the second year of life. J Pediatr. 1983;102:186-190
14. Sabin AB, Arechiga AF, DeCastro JF, et a!. Successful immunization of infants with and without maternal anti-body by aerosolized measles vaccine, II. Vaccine compari-sons and evidence for multiple antibody response. JAMA.
1983;251:2363-2371
15. Brunell PA. Measles vaccine-one or two doses? Pediatrics. 1988;81:722-724
Osteoporosis:
A “New
Morbidity”
for Dieting
Female
Adolescents?
Almost half of the adult skeletal mass is laid down during the adolescent years. The concept of
the “bone bank” reminds us that “deposits” of
calcium are normally made to the skeleton until
about 35 years of age in females. Subsequently, there are continuous “withdrawals” ofbone mineral and loss of skeletal mass, eventually resulting in osteopenia (significantly reduced bone mass) and
osteoporosis (osteopenia associated with
atrau-matic fractures) in more than 20 million
postmen-opausal women, at an annual cost of $7 to 10 billion
in the United States.’
Because there is no cure, prevention of the most common and conspicuous physical finding of adult osteoporosis, the so-called “dowager’s hump” (marked thoracic kyphosis due to vertebral compression fractures), as well as the more serious complications, such as hip fractures, must focus on optimizing the peak bone mass and maintaining the
skeletal mass. In adults, a mere 10% decrease in
bone mineral density (BMD) is associated with a two- to threefold increase in fracture risk. The report by Bachrach and colleagues2 underscores the need for clinicians to consider osteopenia and os-teoporosis as potentially significant problems not only for the elderly, but also for young females with anorexia nervosa, in particular, and those with de-creased weight for height, in general.
Reports of BMD and pathological fractures to date have focused primarily on women with long-standing anorexia nervosa. Earlier studies also used techniques, such as metacarpal cortical thickness measurements3’4 or single-photon absorptiometry,5 that are not applicable to vertebral or femoral bone. Small sample size6 and lack of appropriate control data7 limit the clinical interpretation of recent
in-vestigations of BMD in adolescents with anorexia nervosa. Thus, this study reporting vertebral and whole body bone mineral density more than 2 SD less than values for age-match controls in 12 of 18 female adolescents with anorexia nervosa (half of whom were diagnosed less than a year earlier) is an important, although worrisome, addition to the lit-erature.
The risk factors for osteopenia in anorexia ner-vosa are well known and are related to a negative net balance between bone resorption and forma-tion. Factors related to increased bone loss through resorption include hypoestrogenemia (amenorrhea) and glucocorticoid excess (chronic stress). De-creased bone formation also occurs with glucocor-ticoid excess and with inadequate calcium and pro-tein intake.
The effect of exercise on BMD in anorexia ner-vosa remains controversial. Weight-bearing activity has been reported as being protective against5 as well as unrelated to2’6 bone loss; a recent report
suggests that moderate exercise is beneficial, but
strenuous exercise is detrimental to BMD.7 This
nonlinear effect may explain the finding by
Bach-rach and colleagues of “severe osteopenia in several patients who engaged in regular vigorous exercise.” Unfortunately, there is no reliable means of ac-tually measuring the amount of weight-bearing ac-tivity through time, so that patients have been placed in one of two or three hierarchical levels of exercise. Ideally, the type, frequency, duration, and intensity of activity all need to be considered, and the combined effect could be transformed into a unit of measurement that allows for comparison among patients and studies.
Calcium intake in anorexia nervosa is generally low, but it has not been found to be related to BMD in this or other studies of anorexia nervosa. What
is important in this regard is actual calcium (and