Maciej Dzierżanowski
1, A, C, D, F, Marcin Dzierżanowski
1, B, C, Katarzyna Wrzecion
1, A–C,
Witold Słomko
1, B, C, Agnieszka Radzimińska
2, B, C, Urszula Kaźmierczak
2, B, C,
Katarzyna Strojek
2, B, C, Grzegorz Srokowski
2, B, C, Walery Żukow
3, E, FDiscopathy of the Lumbar-Sacral Segment
and Its Influence on Sexual Dysfunction
Dyskopatia kręgosłupa w odcinku lędźwiowo-krzyżowym
a zaburzenia funkcji seksualnych
1 Department and Institute of Manual Therapy, Nicolaus Copernicus University
Collegium Medicum, Toruń/Bydgoszcz, Poland
2 Department and Institute of Kinesiotherapy and Therapeutic Massage, Nicolaus Copernicus University
Collegium Medicum, Toruń/Bydgoszcz, Poland
3 Department of Health and Tourism, University of Economy, Bydgoszcz, Poland
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Background. Intervertebral disc disease is a widespread medical and social problem. Degeneration of interverte-bral discs can lead to disc disease, commonly known as discopathy. One of the consequences of discopathy is pres-sure on the spinal cord or nerve roots that supply the genitals and sexual centers located in the core. In addition, the accompanying pain and limitation of mobility can lead to the occurrence of sexual dysfunction.
Objectives. The goal of the study was to ascertain the influence of discopathy in the lumbosacral (L-S) segment on the occurrence of sexual dysfunction.
Material and Methods. The study involved 50 hospitalized patients with discopathy in the L-S segment were asked to complete a specially prepared questionnaire (11 questions). The goal of the survey was to compare the patients’ satisfaction with their sex life before and after the disease. The questions were constructed in a way that excluded other indicators that could affect their sexual activity, i.e.: bad moods, bad family relations, or a lack of sexual activ-ity due to age or the lack of a partner.
Results. Discopathy in the lumbar-sacral segment has an influence on sexual activity. A decrease in the assessment of satisfaction with one’s sex life can be observed among patients with discopathy.
Conclusions. The pain and neurological symptoms associated with intervertebral disc disease reduce the patients’ satisfaction with their sex lives. Patients in the group surveyed noted a change in sexual performance, often resulting in passivity, discouragement, weakness or a complete lack of interest in sex. The disorders also affect the emotional state. The patients also noted a significant decrease in physical activity (Adv Clin Exp Med 2013, 22, 1, 93–100).
Key words: discopathy, lumbar-sacral segment, sexual dysfunction.
Streszczenie
Wprowadzenie. Choroba krążka międzykręgowego jest powszechnym problemem społecznym. Gdy krążek między-kręgowy ulegnie zwyrodnieniu, prowadzi to do powstawania choroby dyskowej, powszechnie nazywanej dyskopatią. Konsekwencją dyskopatii w odcinku lędźwiowo-krzyżowym może być ucisk na rdzeń kręgowy lub korzenie nerwowe zaopatrujące narządy płciowe i ośrodki seksualne umiejscowione w rdzeniu. Dodatkowo towarzyszące dolegliwości bólowe oraz ograniczenie sprawności ruchowej mogą prowadzić do wystąpienia zaburzeń funkcji seksualnych.
Cel pracy. W przeprowadzonych badaniach starano się dowieść wpływu dyskopatii w odcinku L-S na występowa-nie zaburzeń funkcji seksualnych.
Materiał i metody. Zbadano 50 pacjentów ze stwierdzoną dyskopatią L-S skierowanych na leczenie ambulatoryjne lub szpitalne. Do badań wykorzystano własną ankietę składającą się z 11 pytań. Badania miały na celu
porówna-Adv Clin Exp Med 2013, 22, 1, 93–100 ISSN 1899–5276
ORIGINAL PAPERS
Nowadays back pain has become one of the so-called lifestyle diseases, affecting 50–80% of the population [1]. One of the most recognizable caus-es of back pain is discopathy. This disease entails gradual pathological changes in intervertebral disc elements, such as annulus fibrosus damage and nucleus pulposus transfer, finally leading to disc hernia [2–4]. It results in pressure on the spinal cord structures. Intervertebral disc damage most frequently occurs in the lumbosacral (L-S) seg-ment, as the lower parts of the spine are subjected to bigger overloading forces. Characteristic symp-toms of L-S segment discopathy include: pain radi-ating to the buttocks, the back surface of the thigh and side surface of the shin; sense disorders, such as paresthesia, burning, tightening in a lower limb; perineum anesthesia; urination and defecation dis-orders; sexual function disorders, such as erection, ejaculation and orgasm disorders [2, 4–6].
Frequent complications of discopathy include neurological disorders, severe pain and limitations to physical activity, which may often lead to lower-ing the person’s quality of life or result in apathy or depression [7, 8].
All these factors may influence not only the person’s social life but also his or her sex life and relations with a partner.
Sexual disorders may appear in patients suf-fering from injuries and diseases of the peripheral nerves, starting from the neurone and finishing at the receptor. Sexual dysfunctions in motor nerve diseases or injuries are rather rare. They may entail difficulty moving during the sexual act, forcing the subject into passivity [9].
More serious discomforts appear when sen-sory nerves are injured. These injuries generate unpleasant feelings from nerveless skin or mucous membranes, or even pain that makes sexual
in-tercourse impossible. A lack of stimulus from the nerveless skin of the penis or vagina negatively in-fluences the chain of sexual reactions. The most serious disorders involve injuries to the autonomic sympathetic and parasympathetic nerves, which frequently completely hinder the sex act [5, 6, 10]. Diseases of the nervous system are often the cause of sexual disorders. Problems with sexual functions in patients who are neurologically ill, particularly in patients with spinal cord and pe-ripheral motor neurone injuries, include: erectile disorder; ejaculation disorder; orgasm disorder; movement disorder; weakening or lack of sexual excitability [11–13].
Despite the common simultaneous occurrence of intervertebral disc diseases and sexual disorders, the phenomenon has not been widely discussed in Polish literature. It may be that the problem of sexual disorders is not perceived as an important aspect of human existence that warrants inclusion in the general course of treatment. The basic aim of the survey is to show if L-S segment discopathy has any influence on the occurrence of sexual dis-orders.
Material and Methods
The study was conducted in a group of patients with diagnosed lumbar- or sacral-segment discopa-thy. The patients were being treated at the Reh-Med Rheumatology and Rehabilitation Clinic in Bydgo-szcz, Poland, and at the A. Korczak Lower Silesian Rehabilitation Center in Kamienna Góra, Poland.
The examined group consisted of 50 patients, including 25 women and 25 men, aged between 20 and 69 years. The study was conducted during the period from January to June 2011.
nie stanu zadowolenia z życia seksualnego z czasu przed wystąpieniem choroby oraz w czasie jej trwania, a także wykluczenie innych czynników mogących mieć wpływ na pogorszenie życia intymnego, tj. zły stan emocjonalny, złe relacje z rodziną lub całkowity brak życia seksualnego z powodu np. wieku czy braku partnera.
Wyniki. Dyskopatia na poziomie L-S kręgosłupa wpływa na występowanie zaburzeń seksualnych. Można zauważyć spadek oceny satysfakcji z życia seksualnego sprzed choroby ze średniej wartości 4,5 pkt. do średniej wartości 3 pkt. Objawy bólowe oraz neurologiczne towarzyszące chorobie krążka międzykręgowego zmniejszają stopień satysfakcji z życia seksualnego pacjentów w grupie mężczyzn 92%, a w grupie 68% zauważyło zmianę w sprawności seksualnej, najczęściej wywołując bierność, zniechęcenie, osłabienie lub całkowity brak zainteresowania seksem. Zaburzenia wpływają również na stan emocjonalny, u 29 (58%) respondentów zmienił się, w tym kobiety wykazywały większą skłonność do zmiany nastroju. Znaczny wpływ ujawnia się również w aktywności fizycznej, gdzie 80% kobiet i 78% mężczyzn zauważyło jej ograniczenie.
Wnioski. Na podstawie analizy wyników badań ankietowych stwierdzono, że dyskopatia w odcinku lędźwiowo-krzyżowym wywiera wpływ na życie seksualne pacjentów. U chorych z rozpoznaną dyskopatią L-S stopień satys-fakcji z życia seksualnego w czasie choroby zmniejsza się, powodując negatywny wpływ na życie seksualne pacjen-tów. Dolegliwości wywołane dyskopatią w odcinku L-S kręgosłupa najczęściej powodują bierność, zniechęcenie lub wycofanie się z życia intymnego. Choroba dyskowa wpływa negatywnie na jakość życia pacjentów. Zmniejsza ich aktywność życiową, aktywność fizyczną oraz wpływa na stan emocjonalny pacjentów, powodując głównie rozdraż-nienie i smutek (Adv Clin Exp Med 2013, 22, 1, 93–100).
Survey Tools
A questionnaire served as the survey tool. It was created on the basis of the Satisfaction With Life Scale (SWLS) and modified according to the needs of the survey. The questionnaire form consisted of two parts, one general and one more detailed. The general part concerned informa-tion about the patient’s age, sex, marital status and length of marriage, education, profession and place of residence.
The detailed part required the patient to choose the number reflecting their state on a scale from 1 to 6, where 1 meant “low” and 6 – “high”. The patients were also asked to describe themselves in terms of physical, intellectual, emotional, sexual and social attributes. The form included questions about their: satisfaction with their sex life; social relations; family relations, mostly with the spouse.
The questions inquired about periods both be-fore and during the occurrence of the symptoms of the disease. Some of the questions examined the patient’s social and family relations and aimed at the exclusion of other aspects influencing sexual disorders.
The results of the questionnaire were record-ed on a special Microsoft Excel spreadsheet. The statistical analysis was prepared with the use of Statistica 9.0 PL software. Astatistical conclusion validation method was used for the verification of the hypothesis. It was based on the chi-square tests (c2) and the Wilcoxon test, and p = 0.05 was
as-sumed as the level of statistical relevance.
Results
The examined group consisted of 25 women (50%) and 25 men (50%). The biggest group of patients were those in the age range from 40 to 49 years (52%).
The analysis of questionnaire results shows that: 34% of the respondents completed higher ed-ucation, 46% – secondary and 20% primary; 82% of respondents live in cities: 28% in big cities, 34%
in medium-sized cities and 20% in small cities; 18% of respondents live in the country; 70% of patients are married, 22% are single, 6% are divorced, one person lives with a long-term partner (2%).
The analysis of the questionnaire results shows that the most popular professions performed by the respondents were: medical professions (ten patients); pensioners (nine patients); salespeople/ dealers (six patients); office workers (six patients); industry workers (five patients).
The respondents generally assessed their social position as good (giving an average rating of 4.38 out of a possible 6); their status in the family on an average level of 4.26; and they assessed their posi-tion at work at an average level of 4.16. The analy-sis of the questionnaire shows that women assess their status in the family higher than the men.
The analysis of the results showed that married people assess emotional support from their family, relations with their partners and other family mem-bers as good. No significant differences were noticed between the points of view of men and women.
Only four people (two women and two men) assessed emotional support from their family as bad (1 or 2 points on the scale of 6), and two peo-ple (one woman and one man) saw their relations with their partners as unsatisfactory. However, these data do not influence the relevance of the study’s investigation of the impact of disc disease on the subjects’ sex lives.
The statistical analysis showed a significant difference in the patients’ assessment of their sat-isfaction with their sex lives in the periods before the illness and during it.
The decrease in the patients’ assessment of their satisfaction with their sex lives is apparent in the average value of 4.5 point before the illness and the average value of 3 points during the illness. Table 1. The age structure of the examined group
Tabela 1. Struktura wieku badanej grupys
Age – years
(Wiek – lata) Number of patients (Liczba pacjentów) %
20–29 6 12
30–39 14 28
40–49 26 52
50–69 4 8
Table 2. Assessment of social position
Tabela 2. Ocena pozycji społecznej Type of social
role (Rodzaj roli społecznej)
Generally – aver-age value (Ogółem – wartość średnia)
Men – average value (Mężczyźni – wartość średnia)
Women – aver-age value (Kobiety – wartość średnia) In the family
(Rodzina) 4.26 4.08 4.42
At work (Praca zawodowa)
4.16 4.08 4.23
Among friends
Comparing the group of men and women we can notice that men assess their sexual satisfaction during their illness on a much lower level than the women. Women on the average rate their satisfac-tion as a 5 before their illness and 4 during their illness, which means that their sex lives are still on a satisfactory level. On the other hand, men on the average rate their satisfaction as a 5 before their illness and 2 during their illness, which means that their sex lives become unsatisfactory because of the illness.
Table 3. Assessment of family relations
Tabela 3. Ocena relacji w rodzinie
Emotional support from their family (Wsparcie emocjonalne ze strony rodziny)
Relations with spouse (Relacje ze współ- małżonkiem)
Relations with other members of the family
(Relacje z innymi członkami rodziny) All
(Ogółem) 4.051 4.308 4.051
Women
(Kobiety) 4.055 4.399 4.071
Men
(Mężczyźni) 4.047 4.238 4.00
Table 4. Wilcoxon signed-rank test: Assessment of satisfaction with sex lives before and during the illness
Tabela 4. Test Wilcoxona: ocena satysfakcji z życia seksualnego przed i podczas choroby Two variables
(2 zmienne) Z P
Before and during
(Przed i podczas) 5.041 < 0001
Table 5. Satisfaction with sex lives
Tabela 5. Zadowolenie z życia seksualnego
All – average value
(Ogółem – wartość średnia) Women – average value (Kobiety – wartość średnia) Men – average value (Mężczyźni – wartość średnia) Before the illness
(Przed chorobą) 4.5 5 4
During the illness
(Podczas choroby) 3 4 2
Table 6. Mann-Whitney U test on sex life satisfaction
Tabela 6. Test U Manna-Whitneya – zadowolenie z życia seksualnego
Variable
(Zmienna) Z P
Before
(Przed) 0.902 0.3040
During
(Podczas) 4.307 0.000007
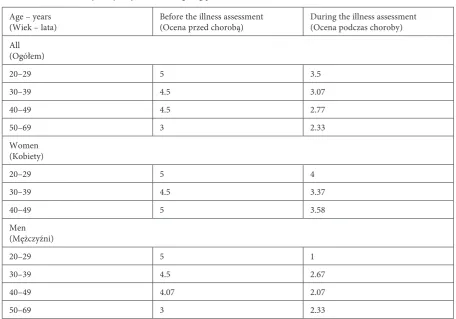
A reduction in sex life satisfaction was observed in each age group. The most noticeable decrease was noted in the group of men aged between 40 and 49 years. The average assessment in this group changed from a satisfactory level of 4.5 points to an unsatisfactory level of 2.77. The women aged 40 to 49 also reported a significant drop in satisfac-tion with their sex lives.
The men in every age group reported a similar difference in their levels of sexual satisfaction be-fore and during their illness: a reduction of 2 points on the scale. However, male sexual satisfaction be-fore illness decreased with age.
The quantitative analysis of the results showed that most respondents assessed their sex lives as satisfying before their illness and as unsatisfying during their illness. This tendency was the same for men and women.
The difference between the genders appears in the quantitative analysis of the results. Only two men stat-ed that their sex lives did not change during the course of disc disease. Twelve men assessed their sexual abili-ties as worse or restricted, and eleven men assumed a passive role or refrained from engaging in sex.
In the group of women, eight patients did not note any change in their sex lives; eight stated that they were less active, five were passive and reluc-tant and four lost interest in sex.
Over half of the examined patients (56%) noted that disc disease had a negative influence on their physical activity. In the course of the disease the respondents felt less active, restricted and in pain.
The analysis of the patients’ assessment of their emotional state before and during their ill-ness shows that 21 respondents (42%) did not no-tice any change and 29 (58%) did note a change in their emotional state. Women reported more no-ticeable changes in their mood. The most frequent changes noted by the respondents were sorrow, anger, irritation, dissatisfaction and gloom.
Discussion
An analysis of the available medical docu-mentation and the results of the survey presented above show that intervertebral disc disease af-Table 7. Self-assessment of satisfaction with sex life compared by gender and age
Tabela 7. Samoocena satysfakcji z życia seksualnego wg płci i wieku
Age – years
(Wiek – lata) Before the illness assessment (Ocena przed chorobą) During the illness assessment (Ocena podczas choroby) All
(Ogółem)
20–29 5 3.5
30–39 4.5 3.07
40–49 4.5 2.77
50–69 3 2.33
Women (Kobiety)
20–29 5 4
30–39 4.5 3.37
40–49 5 3.58
Men (Mężczyźni)
20–29 5 1
30–39 4.5 2.67
40–49 4.07 2.07
50–69 3 2.33
Table 8. Patients’ assessments of their state of health
Tabela 8. Ocena pacjenta ich stanu zdrowia
Healthy
(Zdrowi) % Ill (Chorzy) %
All
(Ogółem) 51.62 48.78
Women
(Kobiety) 59.2 41.2
Men
(Mężczyźni) 44.04 56.36
Table 9. Comparison of two dependent variables for the examined group: Wilcoxon’s test (Patients’ assessments of their state of health)
Tabela 9. Porównanie dwóch zmiennych zależnych w gru-pie badanej: test Wilcoxona (ocena pacjentów ich stanu zdrowia)
Two variables
(2 zmienne) Z p
Before and during
Table 10. Men’s assessment of their sexual activity
Tabela 10. Samoocena aktywności seksualnej mężczyzn
Answer
(Odpowiedź) Number of men
(Liczba)
Percentage of men (Odsetek) % I haven’t noticed any changes
(Nie zauważyłem żadnych zmian)
2 8
I feel restricted
(Czuję się ograniczony) 7 28
I assess my abilities as weak (Oceniam swoje
umiejętności jako słabe)
5 20
I’m passive, not interested, in pain, scared
(Jestem pasywny, nie intere- suję się tym, czuję ból, strach)
11 44
Table 11. Women’s assessment of their sexual activity
Tabela 11. Samoocena aktywności seksualnej kobiet
Answer
(Odpowiedź) Number of women
(Liczba)
Percentage of women (Odsetek) % I haven’t noticed any
changes
(Nie zauważyłam żadnych zmian)
8 32%
I’m less active
(Jestem mniej aktywna) 8 32%
I’m passive, reluctant
(Jestem bierna, niechętna) 5 20%
I’m not interested in sex (Nie jestem zaintereso-wana seksem)
4 16%
Table 12. Patients’ assessment of their physical activity before and during illness
Tabela 12. Ocena pacjentów aktywności fizycznej przed i podczas choroby
Answer
(Odpowiedź) Number of responders
(Liczba badanych)
Percentage of respon-dents (Odsetek) % Women
(Kobiety) no change (brak zmian) I’m less fit/active (jestem mniej aktywna) I feel restricted/in pain (ból mnie ogranicza) I feel lazy/tired (czuję się leniwa/ zmęczona)
5
10
5
5
20
40
20
20
Men (Męźczyźni) no change (brak zmian) I feel weaker (czuję się słabszy) I feel passive/restricted/ in pain
(czuję, że jestem bierny/ból mnie ogranicza)
6
7
12
24
28
48
fects large numbers of patients whose age level is steadily dropping. On the basis of the analysis of the group examined, it can be stated that 40% of the respondents are in the age range from 20 to 39 years, and that 52% are aged between 40 and 49 years, which conforms with reports in the litera-ture that the patients suffering from discopathy is lowering and that the problem is spreading in the form of a so-called lifestyle disease.
Spine diseases are problematic, as they influ-ence many aspects of the patient’s life. Disorders accompanying L-S segment discopathy may lead to activity impairment, worsening the patient’s qual-ity of life [1, 7, 14]. Chronic pain makes everyday activities difficult. It is not easy to dress, to wash and to fulfill physiological needs [4, 5, 8, 15]. Since disc disease results in limited capacity or total
inca-pacity for work, it is becoming a serious economic problem [16].
According to an earlier survey conducted by Pytel and Wrzosek, 55% of the patients suffering from L-S segment discopathy describe the pain ac-companying going upstairs and bending as unbear-able. Pain, discomfort and neurological disorders may last up to 11 months. Such a long period of discomfort, the nature and the degree of pain dur-ing the performance of everyday activities, means that these patients’ quality of life is worsened and that they are forced into passivity in many aspects of life [4].
In the survey presented above, only 52% of the respondents described their state as healthy. In an earlier survey by Jabłońska et al., all the re-spondents noted the impact of the disease on their quality of life, and approximately 87% of them de-scribed the impact as significant [17].
One of the most important factors reducing the quality of life is the presence of pain. This fac-tor is described as significant by 96.6% of the re-spondents interviewed by the authors mentioned above [4, 17].
most frequent symptoms of depression are sleep-ing disorders, eatsleep-ing disorders, low self-esteem, low libido, irritability, a lower need for socializing, low physical and professional activity [7]. All of these factors influence the quality of life and sex life considered as a part of patient’s quality of life.
A survey conducted by Lew-Starowicz between 2002 and 2005 among sexually active Poles showed that when assessing their sex lives the respondents take the following aspects into account: emotions (such as love, friendship, fondness) toward the partner (91%), their partner’s faithfulness (82%) and their own state of health (77%). The survey showed that sex is an important aspect of life and that sexual disorders have a negative influence on the respondents’ quality of life [11–13].
Diseases of the nervous system are a frequent source of sexual disorders, but such disorders are rarely the only symptom of the disease. In neurol-ogy, therefore, this type of disorder is rarely taken into consideration, and may even be ignored dur-ing examinations. The available Polish literature on sexual disorders is rather poor and the problem Table 13. Patients’ assessment of their emotional state
Tabela 13. Ocena pacjentów ich stanu emocjonalnego
Answer
(Odpowiedź) Number of responders
(Liczba badanych)
Percentage of respon-dents (Odsetek) % Women
(Kobiety) no change (brak zmian) I’m impatient (jestem niecierpliwa) I feel dissatisfied, nervous, angry, uptight (czuję niezadowolona, nerwowa, zła, spięta) I’m sad, gloomy, worried
(jestem smutna, ponu- ra, zmartwiona) Ii’m apathetic, with- drawn
(jestem apatyczna, wycofana)
9
3
7
7
4
36
12
28
28
16
Men (Mężczyźni) no change (brak zmian) I’m nervous (jestem nerwowy) I feel frustrated (czuję frustrację) I feel calmer
(czuję się spokojniejszy) 12
6
3
4
48
24
12
16
is not widely given attention in medical practice [5, 6].
Diseases of the central nervous system may be accompanied by all types of sexual disorders, includ-ing both organic and functional disorders. They may be divided into three groups: 1) disorders that make sexual intercourse difficult or impossible (erectile disorders, ejaculation disorders, orgasm disorders and movement disorders); 2) sexual excitability disorders (increase, decrease or lack of excitability, sexual deviations); 3) paroxysmal sex sensations.
The first group of disorders affects patients with spinal cord injuries and peripheral motor neuron injuries. These disorders may affect people suffering from discopathy. The second group of disorders are usually consequences of injuries or diseases of the upper segments of nervous system, particularly the limbic system and cortex. The third group consists of disorders associated with differ-ent types of epilepsy and are often connected with injuries to the parietal and temporal lobes. The last group refers to extensive changes in diseases of the brain, pituitary gland or hypothalamus [5, 11, 12].
The most frequent disorders caused by L-S seg-ment discopathy are erection disorders in men and orgasm disorders in women. These disorders were taken into consideration while comparing the re-sults of the current survey with those from the available medical literature.
Impotence can coexist with almost all diseases in men of all age groups. Patients with injured spi-nal cords or with other L-S segment diseases usu-ally suffer from erection disorders. Earlier surveys showed that:
– a good state of health has a positive impact on sexual ability;
– chronic diseases correlate with impotence; – penile vascular reactivity depends on the proper reaction of the erection center in the spinal cord located in L-S segment, the activity of nerve routes (e.g. the pudendal nerve, the autonomic nervous system) and the efficiency of the pelvis;
– neurological disorders are recognized as the most frequent causes of impotence, affecting approximately 18.1% of patients, whereas disor-ders of a psychogenic nature affect approximately 10.4% [10, 11].
The survey described in this study showed that 94% of the male respondents noticed decreased sexual activity or refrained from sexual activity. In addition, 56.36% of the male respondents assessed their state of health as unwell. The analysis of the survey results led to the conclusion that discopathy impairs sexual activity, which confirms the results of earlier surveys.
positively influenced by: a satisfying relationship, an optimal period of foreplay and intercourse, a higher level of education, activity and erotic imagination, self-acceptance and the acceptance of one’s own social role [10, 12].
The analysis of the survey presented in the current paper showed that the female respon-dents’ level of satisfaction with their sexual lives decreased from an average value of 5 prior to the onset of disc disease to 4 during the course of the illness. The change is aggravated by a passive at-titude, a feeling of discouragement and feelings of frustration, anger, sorrow and depression.
The available literature on intervertebral disc diseases confirms the scale and common occur-rence of a correlation between L-S segment dis-copathy and sex-life disorders. The authors con-cluded that the analysis of the conducted survey showed that L-S segment discopathy influences the patients’ sex lives to a large degree. The answers to the questionnaire indicate that patients diagnosed with L-S segment discopathy notice a reduction in their level of sexual satisfaction and negative effects on their sex lives. Discomfort in the L-S segment caused by discopathy frequently results in feelings of passiveness and discouragement, or withdrawal from sexual activity.
References
Dzierżanowski M, Słomko W, Pawlak J, Tyborki M, Pastor A:
[1] Skuteczność mikroendoskopowej dyscektomii oraz rehabilitacji pooperacyjnej w leczeniu dyskopatii lędźwiowej. In: Selected problems of the foundations of rehabilitation, physiotherapy, locomotor activity of people with disabilities, ballroom dance. Wybrane zagadnie-nia z podstaw rehabilitacji, fizjoterapii, aktywności ruchowej osób niepełnosprawnych, tańca towarzyskiego. Ed. Kwasnik Z et al. RSW, Radom 2009, 27–55.
Dziak A:
[2] Bóle i dysfunkcje kręgosłupa. PZWL, Kraków 2007.
Stodolny J:
[3] Choroba przeciążeniowa kręgosłupa. ZLNatura, Warszawa 2008.
Pytel A, Wrzosek Z:
[4] Główne czynniki ryzyka dyskopatii lędźwiowo-krzyżowej kręgosłupa. Kwart Ortop 2009, 75 (3), 331–338.
Sawka M:
[5] Neurogenne zaburzenia erekcji pochodzenia rdzeniowego. Seksuol Pol 2004, 2 (1), 19–23.
Sawka M:
[6] Neurogenne przyczyny zaburzeń erekcji. Seksuol Pol 2004, 2(1), 13–17.
Radziszewski K:
[7] Analiza objawów depresyjnych u pacjentów z dyskopatią lędźwiową leczonych zachowawczo bądź operacyjnie. Post Psychiatr Neurol 2006, 15(2), 77–81.
Radziszewski K:
[8] Analiza porównawcza stanu neurologicznego chorych na dyskopatię kręgosłupa lędźwiowego leczonych zachowawczo lub operacyjnie. Pol Merk Lek 2007, XXII 129, 186–191.
Tederko P, Radomski D:
[9] Zdrowie seksualne osób po urazie kręgosłupa powikłanym zaburzeniami neurologicz-nymi. Seksuol Pol 2009, 7(2), 65–71.
Lew-Starowicz Z:
[10] Leczenie czynnościowych zaburzeń seksualnych. PZWL, Warszawa 1999.
Lew-Starowicz Z:
[11] Diagnostyka różnicowa zaburzeń erekcji. Seksuol Pol 2005, 3(2), 60–63.
Lew-Starowicz Z:
[12] Leczenie zaburzeń seksualnych. PZWL, Warszawa 1997.
Lew-Starowicz Z:
[13] Seksualność a jakość życia człowieka. Przegl Seksuol 2006, 5, 21–26.
Radziszewski K:
[14] Analiza sprawności ruchowej pacjentów leczonych z powodu dyskopatii kręgosłupa lędźwiowe-go. Valetudinaria – Post Med Klin Wojsk 2008, (13)1, 13–18.
Hoffman J, Dejewska I:
[15] Wpływ rehabilitacji na wyniki leczenia operacyjnego dyskopatii odcinka lędźwiowo-krzy-żowego. Kwart Ortop 2009, 2, 159–161.
Pawlak J, Dzierżanowski M, Słomko W, Tyborki M, Pastor A:
[16] Ocena efektywności zastosowania masażu leczni-czego w procesie rehabilitacji pacjentów z dysfunkcjami odcinka L-S kręgosłupa. In: Selected problems of the foun-dations of rehabilitation, physiotherapy, locomotor activity of people with disabilities, ballroom dance. Wybrane zagadnienia z podstaw rehabilitacji, fizjoterapii, aktywności ruchowej osób niepełnosprawnych, tańca towarzyskie-go. Ed. Kwasnik Z et al. RSW, Radom 2009, 20–27.
Jabłońska R, Beuth W, Ślusarz R, Saracen A:
[17] Factors which determine the efficiency of patients who underwent surgical treatment of disc disease. Ed. Kotwica Z, Saracen A, Neurosurgery – new trends in therapy, nursing and rehabilitation. Medicam, Gryfice 2009, 49–56.
Address for correspondence:
Walery Żukow
Department of Health and Tourism University of Economy in Bydgoszcz Garbary 2
85-229 Bydgoszcz Poland
E-mail: [email protected]
Conflict of interest: None declared