Katarzyna Neubauer
1, Robert Dudkowiak
2, Leszek Paradowski
1Left-Sided Diverticulosis of the Large Bowel
as the Second Most Common Abnormality
in Colonoscopy – Review of 425 Cases of Colonic
Diverticulosis
Lewostronna uchyłkowatość jelita grubego jako druga co do częstości
nieprawidłowość w kolonoskopii – przegląd 425 przypadków
uchyłkowatości jelita grubego
1 Department of Gastroenterology and Hepatology, Wroclaw Medical University, Poland
2 Division of Dietetics, Department of Gastroenterology and Hepatology, Wroclaw Medical University, Poland
Abstract
Background. Colonic diverticulosis is characterized by different prevalence rate in different world regions and an increase in morbidity rates corresponding to the change of lifestyle due to the civilization development.
Objectives. This study was aimed to evaluate frequency of diverticulosis in colonoscopic examinations. Additionally, age and gender of patients, location of diverticula, presence of complications of diverticulosis and accompanying diseases were evaluated.
Material and Methods. The authors analyzed 3011 colonoscopic reports of patients hospitalized in Department of Gastroenterology and Hepatology, Wroclaw Medical University. Study group encompasses 1776 women at the age of 17–98 (mean age 54.4) and 1235 men at the age of 18–100 (mean age 52.5).
Results. Diverticula were found in 425 (14.11%) patients. The most common abnormality were polyps present in 434 of patients. The most frequent location of diverticulosis was sigmoid and descending colon. Disease spreads in continuous way. Patients with diverticulosis were older than patients without diverticulosis. There was no signifi-cant difference between mean age and location of diverticula (right-sided versus left-sided; p = 0.328). Frequency of diverticulosis did not differ between men and women. The only one complication detected in colonoscopy was SCAD (segmental colitis associated with diverticulosis). Among accompanying conditions polyps were the most frequent and present in 96 (22.58%) patients with diverticulosis.
Conclusions. Diverticulosis is the second most common abnormality of the large intestine in colonoscopy. Diverticula occur the most frequently in sigmoid and descending colon and spread in continuous way. Men and women are affected with the same frequency and prevalence increases with age. The most common accompanying condition are polyps (Adv Clin Exp Med 2010, 19, 4, 513–518).
Key words: large bowel diverticulosis, colonic polyps.
Streszczenie
Wprowadzenie. Uchyłkowatość jelita grubego charakteryzuje zmienna częstość występowania w różnych regio-nach świata i wzrost wskaźników zachorowalności równoległy do towarzyszących rozwojowi cywilizacji zmian stylu życia.
Cel. Ocena częstości występowania uchyłkowatości w badaniach kolonoskopowych. Dodatkowo określano wiek, płeć pacjentów, umiejscowienie uchyłków, obecność powikłań uchyłkowatości i chorób towarzyszących.
Materiał i metody. Badanie polegało na analizie 3011 kolonoskopii przeprowadzonych u pacjentów hospitalizowa-nych w Klinice Gastroenterologii i Hepatologii Akademii Medycznej we Wrocławiu. W grupie badanej było 1776 kobiet w wieku 17–98 lat (średni wiek 54,4) oraz 1235 mężczyzn w wieku od 18–100 lat (średni wiek 52,5).
Wyniki. Uchyłki stwierdzono u 425 (14,11%) pacjentów. Najczęstszą nieprawidłowością jelita grubego były polipy, stwierdzone u 434 pacjentów. Uchyłki były najczęściej umiejscowione w esicy i zstępnicy. Choroba szerzyła się w spo-sób ciągły. Pacjenci z uchyłkowatością byli starsi od pacjentów bez uchyłkowatości. Nie wykazano istotnej
statystycz-Adv Clin Exp Med 2010, 19, 4, 513–518 ISSN 1230-025X
ORIGINAL PAPERS
Diverticula of the large intestine are acquired protrusions of mucosa and submucosa through the wall of the colon. Etiopathogenesis of colonic diverticulosis is not fully elucidated and appears to be complex. Dietary fiber deficiency is the most often suggested to be a key factor in diverticula de-velopment [1]. This opinion is supported by the findings from epidemiological studies conducted in different world regions and in different time. From one hand, colonic diverticulosis belongs to the western civilization diseases with the highest prevalence rate in Europe and the United States, where diet is typically poor in fiber [2]. It is com-mon condition in Europe and it may be specu-lated that the incidence rate will increase in the future [3]. Similar observations were additionally made in other regions of the world [4]. From the other hand, increasing prevalence rate of colonic diverticulosis in last years was demonstrated in countries adopting western life style, where until now diverticulosis was rather rare. Some animal studies also confirmed, that fibre is a main player in disease pathogenesis [5].
Most of the patients with colonic diverticu-losis does not experience any symptoms. Rela-tion between diverticulosis and symptoms is often made, however it is difficult to prove. Symptoms prescribed to the diverticulosis may be also related to functional disorders of the large bowel since the presence of anatomic abnormalities does not eliminate the diagnosis of functional disorder [6]. Diverticulosis was found in 7.7% of patients with non-constipated irritable bowel syndrome [7]. However, the presence of diverticula is always re-lated with the risk of serious complications. The most common complication is diverticulitis, which often requires admission to the hospital or even surgical interventions. Other complications in-volve diverticular bleeding and segmental colitis associated with diverticulosis (SCAD) [8, 9].
As diverticulosis often remains asymptomatic, data regarding the incidence and location of diver-ticula come mostly from autopsy, endoscopic or radiological studies. Contemporary, diverticulosis is diagnosed mainly with colonoscopy, however it may be also demonstrated in barium enema, CT colonoscopy or even ultrasound examination [10].
Results of those studies demonstrated that there is a geographic variation not only between diverticulosios frequency but also its location. It is well documented that diverticulosis in Asian coun-tries appears predominantly in the right colon and in other world regions in the left colon [11, 12].
As Poland belongs to the countries, where life style has changed during last decades it is interest-ing to know the frequency of diverticulosis. In the future such data may also serve for comparative reasons.
This study was aimed to assess frequency and location of diverticulosis and accompanying ab-normalities of the large bowel in colonoscopies of patients hospitalized in Department of Gastro-enterology and Hepatology in years 2004–2005, Wroclaw Medical University.
Material and Methods
Study group consisted of the patients hospi-talized in Department of Gastroenterology and Hepatology, Wroclaw Medical University, which had colonoscopy. 3011 colonoscopic reports were evaluated. Indications for colonoscopy were: gas-trointestinal symptoms (abdominal pain, consti-pation, diarrhea), obscure anemia, symptoms and signs of colonic bleeding, alarm symptoms (weight loss, etc.), inflammatory bowel disease suspicion and monitoring. The patients` age was between 17–100 years (52.5; SD ± 16.36). Study group en-compasses 1776 women at the age of 17–98 (54.4) and 1235 men at the age of 18–100 (52.5).
Large intestine was divided into two parts: right-side (proximal do the splenic flexure) and left-side (distal to splenic flexure). Statistical analy-sis was performed using Student’s t-test and chi-square test. Results were considered statistically significant with p < 0.05.
Results
Diverticulosis was diagnosed in 425 (14.11%) patients (268 men, 157 women). Mean age of pa-tients with diverticulosis was 65.96 years (25–94
nie różnicy między średnim wiekiem pacjentów a umiejscowieniem uchyłków (prawostronne versus lewostronne; p = 0,328). Częstość występowania uchyłkowatości była taka sama u mężczyzn i kobiet. Jedynym powikłaniem stwier-dzanym w kolonoskopii było SCAD (segmental colitis associated with diverticulosis). Spośród towarzyszących uchył-kom nieprawidłowości jelita grubego najczęściej stwierdzano polipy, które były obecne u 96 (22,58%) pacjentów.
Wnioski. Uchyłkowatość jelita grubego jest drugą co do częstości występowania nieprawidłowością jelita grube-go stwierdzaną w kolonoskopii. Uchyłki występują najczęściej w esicy i zstępnicy i szerzą się w sposób ciągły. Uchyłkowatość dotyczy równie często kobiet i mężczyzn, a ich częstość występowania rośnie z wiekiem. Najczęstszą chorobą jelita grubego współistniejącą z uchyłkowatością są polipy (Adv Clin Exp Med 2010, 19, 4, 513–518).
years, SD ± 10.72). Patients with diverticulosis were significantly older than patients without di-verticulosis (mean age 51 years; SD 16.02, p < 0.01). There was no difference regarding frequency of di-verticulosis between men and women (p = 0.065) (Table 1). Prevalence of diverticulosis, depending on age range and sex is shown in Figure 1.
The most common affected segments of the large intestine were sigmoid colon (n = 397; 93.41%) and descending colon (n = 158; 37.17%). No patients had diverticula in caecum. There were two cases of diverticula in rectum. A de-tailed distribution of diverticula according to sex considering their number and location in seg-ments of the large intestine is shown in Table 2. In 10 patients (4 men, 6 women, mean age 65.78 years; SD ± 9.73) diverticulosis was limited to the transverse and ascending colon. There was no significant difference between mean age and location of diverticula (right-sided versus left-sided; p = 0.328) (Fig. 2). Diverticula of sigmoid colon coexisted with diverticula of: descending colon (n = 145); transverse colon (n = 48); as-cending colon (n = 41).
Distribution of diverticulosis within the large bowel is demonstrated in Table 3.
There was no patients with diverticulitis and diverticular bleeding. 20 (4.7%) patients had seg-mental colitis associated with diverticulosis.
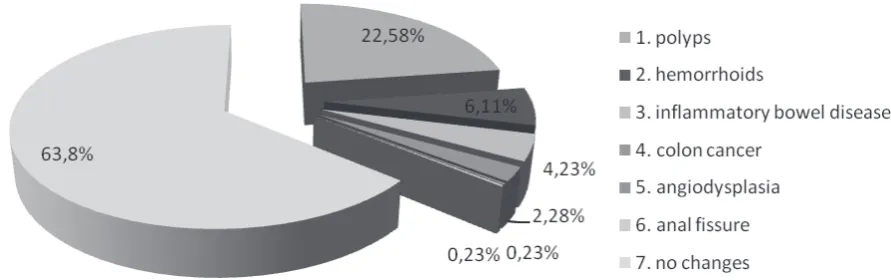
Accompanying diseases of the large bowel, the most common colonic abnormality in patients with diverticulosis were polyps (Fig. 3.). Colonic polyps were detected in 96 (22.58%) patients with diverticulosis.
Malignant changes were observed in 12 (2.82%) cases and the distribution of colorectal cancer (CRC) was as follows: 5 rectum, 4 sigmoid colon,
Table 1. Prevalence of diverticulosis regarding gender
Tabela 1. Występowanie uchyłkowatości w zależności od płci
Sex
(Płeć) With diverticula n (%)(Z uchyłkami n (%)) Without diverticula n (%)(Bez uchyłków n (%)) Women
(Kobiety) 268 (8.9) 1508 (50.08) Men
(Mężczyźni) 157 (5.2) 1078 (35.8)
1 2 13
55
69
100
18
2
0 3 7
39 49 41
13 0 0
20 40 60 80 100 120
20–29 30–39 40–49 50–59 60–69 70–79 80–89 90–99
women (kobiety)
men (mężczyźni)
Fig. 1. Prevalence of diverticulosis for age according to sex
Ryc. 1. Występowanie uchyłkowatości w zależności od wieku z uwzględnieniem płci
Median (mediana) 25%–75% Min.–Max
1 0
Location (lokalizacja)
20 30 40 50 60 70 80 90 100
Age (wiek
)
Fig. 2. Location of diverticula and age: 1 – right side of colon,
0 – left side of colon
Ryc. 2. Umiejscowienie uchyłków a wiek pacjentów: 1 – prawa strona jelita grubego,
Table 2. Diverticula distribution according to sex considering their number and exact, segmental location in the large intestine
Tabela 2. Rozmieszczenie uchyłków w zależności od płci i wieku, uwzględniając ich liczbę i umiejscowienie w poszczegól-nych segmentach jelita grubego
Sex
(Płeć) Age categories(Przedział wiekowy)
No of patients (Liczba pacjentów)
Location (Rozmieszczenie)
R SC DC TC AC C
W 20–29 1 1 0 0 0 0 0
M 0 0 0 0 0 0 0
W 30–39 2 0 2 1 0 0 0
M 3 0 2 2 0 0 0
W 40–49 13 0 13 6 1 0 0
M 7 0 6 5 2 2 0
W 50–59 55 0 50 14 5 4 0
M 39 0 35 13 7 3 0
W 60–69 69 0 64 28 12 8 0
M 49 0 47 22 7 4 0
W 70–79 100 1 98 34 11 10 0
M 41 0 37 14 9 5 0
W 80–89 18 0 16 8 3 1 0
M 13 0 13 7 4 4 0
W 90–99 2 0 2 0 0 0 0
M 0 0 0 0 0 0 0
W xx 8 0 6 1 1 0 0
M 5 0 5 3 0 0 0
Table 3. Distribution of diverticula within the bowel
Tabela 3. Rozmieszczenie uchyłków w jelicie grubym
Location (Umiejscowienie) n (%) Rectum (Odbytnica) 2 (0.47) Sigmoid colon (Esica) 397 (93.41) Descending colon (Zstępnica) 158 (37.17) Transverse colon (Poprzecznica) 62 (14.58) Ascending colon (Wstępnica) 43 (10.11) Caecum (Kątnica) 0 (0)
Fig. 3. Coexistence of diverticulum and polyp
Ryc. 3. Współistnienie uchyłka jelita grubego i polipa
R – rectum. R – odbytnica. SC – sigmoid colon. SC – esica.
DC – descending colon. DC – zstępnica.
TC – transverse colon. TC – poprzecznica AC – ascending colon. AC – wstępnica. C – caecum. C – kątnica.
1 descending colon, 0 transverse colon, 1 ascend-ing colon and 1 caecum.
Other findings included: inflammatory bowel disease (n = 18); hemorrhoids (n = 26); angiodys-plasia (n = 1); anal fissure (n = 1) (Fig. 4).
Discussion
This study has demonstrated that diverticulo-sis is the second most frequent finding in colonos-copy in patients hospitalized in gastroenterol-ogy department in Lower-Silesia, Poland. Patients with diverticulosis are older than patients without diverticulosis, what reflects the increase of diver-ticulosis prevalence with age [13].
Similarly to the epidemiological data from western countries, the most common location of diverticulosis in own group was left side of the bowel. Sigmoid colon was affected in almost 95% of patients. There were two patients in own study group with the diverticula located in rectum. This finding can be considered as a case report, as nu-merous sources emphasized that diverticula do not occur in this part of the large bowel due to its anatomical structure. Involvement of the right colon (15% transverse colon, 10% descending co-lon) was rarer than involvement of the left bowel. There were no patients with diverticula in caecum. Right colon diverticulosis is typical for Asian pop-ulations. Phenomenon of the geographic variation in diverticula location within the large bowel is not fully elucidated. It seems that additionally right co-lon diverticulosis differs from left coco-lon diverticu-losis with age of patients and spectrum of clinical manifestations. Knowledge about anatomic pat-tern of diverticulosis is important because of its influence on clinical manifestation. Asian patients with diverticulitis may present with the
symp-toms of acute appendicitis. Additionally, they are younger than patients with left-sided diverticulitis [14]. In Poland patients with diverticulitis mani-fested the most often pain in the left abdominal quadrant. Summarizing, the most common loca-tion of the diverticulosis in Lower-Silesian popu-lation of patients is sigmoid colon. Additionally, the authors observed that diverticulosis within the large intestine spreads in continuous way. All of sigmoid diverticula coexist with diverticula of de-scending colon and most of them also with the di-verticula of upper parts of the large bowel. Also six of thirteen descending diverticula (not connected with sigmoid diverticula) were associated with di-verticula of transverse colon.
The only one complication of diverticulosis found in own group was SCAD. There were no patients with diverticulits, what is explained by the fact that diverticulitis is contraindication for colonoscopy. However, the diagnosis of divertic-ulosis always carries the risk of diverticulitis and there are studies showing increase in hospitaliza-tion rate related to diverticular disease [15]. Other study in Poland demonstrated that significant part of patients with diverticulosis is overweight or obese [16]. As obesity is a risk factor of diverticuli-tis it may be speculated that this complication will also occur in own study group [17]. There were also no patients with diverticular bleeding, what probably result from the fact that patients with acute lower gastrointestinal bleeding are typically hospitalized in surgical departments. SCAD is the rarest complication of diverticulosis and may be a diagnostic challenge as endoscopic picture may resemble inflammatory bowel disease [18].
The most common accompanying findings in patients with diverticulosis were polyps. The problem if diverticula are a risk factor for polyps is still not clear and the results of studies
regard-Fig. 4. Changes accompanying the large intestine diverticulosis
Ryc. 4. Zmiany towarzyszące uchyłkowatości jelita grubego
ing it are controversial [19, 20]. The coexistence of both conditions may be partly explained by similar risk factors, mostly age. It needs to be highlighted that colonic polyps are precancer conditions of the large bowel. In the structure of incidence of malig-nancies colorectal cancer has a second place among males and females in Poland [21]. Further studies are needed to clarify the exact relation between diverticulosis and polyps, what can influence e.g. colorectal cancer screening programs.
References
[1] Stolmann N, Raskin JB: Diverticular disease of the colon. Lancet 2004, 363, 631–639.
[2] Painter NS, Burkitt DP: Diverticular disease of the colon: a deficiency disease of Western civilization. Br Med J 1971, 5759, 450–454.
[3] Delvaux M: Diverticular disease of the colon in Europe: epidemiology, impact on citizen health and prevention. Aliment Pharmacol Ther 2003, 18 (Suppl. 3), 71–74.
[4] Warner E, Crighton EJ, Moineddin R, Mamdani M, Upshur R: Fourteen-year study of hospital admissions for diverticular disease in Ontario. Can J Gastroenterol 2007, 21.
[5] Wess L, Eastwood M, Busuttil A, Edwards C, Miller A: An association between maternal diet and colonic diver-ticulosis in an animal model. Gut 1996, 423–427.
[6] Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC: Functional Bowel Disorders. Gastroenterology 2006, 130, 1480–1491.
[7] Chey WD, Nojkov B, Rubenstein JH, Dobhan RR, Greenson JK, Cash BD: The Yield of Colonoscopy in Patients With Non-Constipated Irritable Bowel Syndrome: Results From a Prospective, Controlled US Trial. Am J Gastroenterol 2010, 105, 842–847.
[8] Parra-Blanco A: Colonic Diverticular Disease: Pathophysiology and Clinical Picture. Digestion 2006, Suppl. 1, 73, 47–57.
[9] Freeman HJ: Segmental colitis associated with diverticulosis syndrome. World J Gastroenterol 2008, 14, 6442–6443.
[10] Hale WB: Colonoscopy in the diagnosis and management of diverticular disease. J Clin Gastroenterol 2008, 42, 1142–1148.
[11] Lee YS: Diverticular disease of the large bowel in Singapore. An autopsy survey. Dis Colon Rectum 1986, 29, 330–335.
[12] Miura S, Kodaira S, Shatari T, Nishioka M, Hosoda Y, Hisa TK: Recent trends in diverticulosis of the right colon in Japan: retrospective study in a regional hospital. Dis Colon Rectum 2000, 43, 1383–1389.
[13] Comparato G, Pilotto A, Franze A, Franceschi M, Di Mario F: Diverticular disease in elderly. Dig Dis 2007, 25, 151–159.
[14] Matshushima K: Management of right-sided diverticulitis: a retrospective review from hospital in Japan. Surg Today 2010, 40, 321–325.
[15] Jeyarajah S, Faiz O, Bottle A, Aylin P, Bjarnason I, Tekkis PP, Papagrigoriadis S: Diverticular disease hospital admissions are increasing, with poor outcomes in the elderly and emergency admissions. Aliment Pharmacol Ther. 2009, 30, 1171–1182.
[16] Neubauer K: Obesity and overweight in patients with colonic diverticulosis. Gastroenterol Pol 2010, 17, 74–76.
[17] Strate LL, Liu YL, Aldoori WH, Syngal S, Giovannucci EL: Obesity increases the risks of diverticulitis and diver-ticular bleeding. Gastroenterology 2009, 136, 115–122.
[18] Sheth AA, Longo W, Floch MH: Diverticular disease diverticulitis. Am J Gastroenterol 2008, 103, 1550–1556.
[19] Hirata T, Kawakami Y, Kinjo N, Arakaki S, Arakaki T, Hokama A, Kinjo F, Fujita A: Association between colonic polyps and diverticular disease. World J Gastroenterol 2008, 14, 2411–2413.
[20] Meurs-Szojda MM, Terhaar JS, Kuik DJ, Mulder CJJ, Felt-Bersma RJF: Diverticulosis and diverticulitis form no risk for polyps and colorectal neoplasia in 4,241 colonoscopies. Int J Colorectal Dis 2008, 23, 979–984.
[21] Wojciechowska U, Didkowska J, Zatoński W: Nowotwory złośliwe w Polsce w 2006 roku, Warszawa 2008.
Address for correspondence:
Katarzyna Neubauer
Department of Gastroenterology and Hepatology Wroclaw Medical University
ul. Borowska 213 50-556 Wrocław Poland
Tel.: +48 71 733 21 20
E-mail: [email protected] Conflict of Interest: None declared
Received: 27.07.2010 Revised: 27.07.2010 Accepted: 27.07.2010