Aleksandra Harat
1, A–D, F, Paweł Sokal
2, B–D, F, Piotr Zieliński
2, C–F,
Marek Harat
2, A–D, F, Teresa Rusicka
3, A, B, D, F, Leszek Herbowski
4, C, D, FAssessment of Economic Effectiveness in Treatment
of Neuropathic Pain and Refractory Angina Pectoris
Using Spinal Cord Stimulation*
Ocena efektywności ekonomicznej leczenia bólu neuropatycznego
i lekoopornej dusznicy bolesnej za pomocą neurostymulatora rdzenia
kręgowego
1 Department of Preventive Medicine and Environmental Health, Nicolaus Copernicus University Collegium Medicum in Bydgoszcz, Poland
2 Clinic of Neurosurgery, Military Hospital no. 10 in Bydgoszcz, Poland
3 Hemodynamics Laboratory, Cardiac Rehabilitation Hospital, Kowanówko, Poland
4 Ward of Neurosurgery and Neurotraumatology, Marie Curie-Skłodowska Independent Public Provincial Hospital, Szczecin, Poland
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation; D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Background. The implementation of new diagnostic and therapeutic technologies is related to expanding financial
needs. The escalation of expenses for health protection and simultaneous economic problems has resulted in an interest in the subject of economic assessment. Decision makers in the health sector should have reasonable tools that will allow them to make complex evaluations of the economic suitability of health technologies. Economic analysis should also prove that launching new procedures can save money. Numerous studies indicate that chronic pain and psycho-sociological variables lead to a worse quality of life. Chronic pain issues are a major public health problem, by virtue of the difficulties in efficient therapy and the social costs reflected in incapability of work and disability. Spinal cord stimulation is the most efficacious procedure in the treatment of chronic pain.
Objectives. The aim of the study was to estimate the costs of treatment of 37 patients suffering from refractory
angina pectoris and neuropathic pain who underwent SCS surgery between 2002 and 2008 in the Neurosurgery Clinic of the 10th Military Hospital in Bydgoszcz in the period of two years before and two years after spinal cord stimulation. The authors also assessed quality of life, using the SF 36 questionnaire, and degree of pain using VAS.
Material and Methods. The issue was examined with a cost-benefit analysis. Cost was understood as the expenses
made two years before and two years after the SCS procedure. The benefits were health care expenses saved by implementation of the SCS procedure. All the costs included in both alternative treatment techniques in a period of 5 years underwent a discounting procedure. The authors also included the price of the neurostimulator under a sensitivity analysis. To assess the quality of life before and after the SCS procedure, a SF 36 questionnaire was used, and to assess the level of pain before and after the SCS procedure, the VAS scale.
Results. The costs of treatment of refractory angina pectoris and neuropathic pain are lower when using spinal cord
stimulation. In the case of refractory angina pectoris, savings reached 46% whereas in the case of neuropathic pain, 13.2%. The costs of the purchase of the device returned in three years for angina pectoris and seven years for neuro-pathic pain. SCS in both cases brought a reduction of the level of pain and an improvement to quality of life.
Adv Clin Exp Med 2012, 21, 5, 653–663 ISSN 1899–5276
oRIgINAL PAPERS
© Copyright by Wroclaw Medical University
Pain is an unpleasant sensory and emotional experience associated with actual or potential age of tissue or described in terms of such dam-age [1]. Chronic pain is increasingly prevalent in societies of the twenty-first century. A number of factors cause chronic pain but the result is always the same: an individual cannot fully function.
Neuropathic Pain
Neuropathic pain is defined as pain caused or initiated by primary changes or disturbances in the nervous system [1]. It can take many forms, such as diabetic polyneuropathy (DPN), postherpetic neuralgia (PHN), trigeminal neuralgia, complex re-gional pain syndrome (CRPS), phantom pain and failed-back surgery syndrome (FBSS) – pain after unsuccessful neurosurgical intervention [2, 3].
Experimental studies point out three compo-nents in the etiology of neuropathic pain: chang-es in electrical excitability of the damaged axon membrane and the first afferent neuron of the spi-nal ganglion, changes in the processing of received signals in the posterior horn of the spinal cord and
disintegration of pre-programmed response in high-levels of CNS to situations affecting the in-tegrity of the body. Presently, ongoing studies are examining the mechanism of activation of microg-lia cells as an additional factor that may participate in the increase of neuropathic pain [2, 3].
Treatment of neuropathic pain is more diffi-cult than the treatment of nociceptive pain, mainly due to the fixed nature of central and peripheral sensitization [4].
The first step in the treatment of this type of pain is pharmacotherapy. The first used are non-steroidal anti-inflammatory drugs. The next step is to add weak opiates and/or supportive medication. In cases of further persistence of pain, the patient is advised to use a stronger opiate and adjunctive drug in order to improve the control of pain (anti-depressants, anticonvulsants, baclofen, stimulants, corticosteroids, anesthetics, and capsaicin applied topically) [4, 5].
Despite the enormous progress in pharmacolo-gy in therapy against neuropathic pain, there is still a significant number of patients treated pharmaco-logically who do not feel sufficient relief. given the assumption that effective treatment of pain is that
Conclusions. SCS in both neuropathic pain and refractory angina pectoris is a procedure that brings benefits in the
form of savings. After using SCS in both cases, the quality of life improved and the level of pain was reduced (Adv
Clin Exp Med 2012, 21, 5, 653–663).
Key words: economic analysis, cost-benefit analysis, neuropathic pain, refractory angina pectoris, spinal cord
stim-ulation.
Streszczenie
Wprowadzenie. Wdrażanie do diagnozowania i leczenia zdobyczy nowych technologii wiąże się z rosnącymi
potrzebami finansowymi. Analizy ekonomiczne mogą dostarczyć dowodów na to, że wprowadzenie określonego standardu terapeutycznego przyniesie oszczędności finansowe w przyszłości. Zespoły bólu przewlekłego stają się coraz istotniejszym problemem zdrowia publicznego z uwagi na trudności w skutecznym leczeniu oraz koszty społeczne odzwierciedlone w niezdolnosci do pracy i inwalidztwie. Stymulacja rdzenia kręgowego (SCS) jest dziś jednym z najskuteczniejszych zabiegów terapeutycznych.
Cel pracy. ocena kosztów leczenia 37 pacjentów z bólem neuropatycznym i lekooporną dusznicą bolesną
opero-wanych z powodu dolegliwości bólowych od 2002 do 2008 roku w Klinice Neurochirurgii 10. Wojskowego Szpitala Klinicznego w Bydgoszczy, a także ocena jakości życia według formularza SF-36 oraz odczuwania bólu według skali VAS.
Materiał i metody. Do badania użyto analizy koszt–korzyść. Koszty poddano operacji dyskontowania. Podjęto też
analizę wrażliwości ceny stymulatora. Do oceny skali bólu użyto skali VAS przed i po zabiegu, a jakość życia oce-niono za pomocą kwestionariusza SF-36.
Wyniki. Przeprowadzona analiza wykazała, że leczenie lekoopornej dusznicy bolesnej za pomocą SCS jest
tań-sze o 46% w stosunku do leczenia bez implantu, a koszt implantu zwraca się średnio w ciągu trzech lat. Leczenie bólu neuropatycznego z użyciem SCS jest tańsze o 13,2%, a koszty implantu zwracają się średnio po 7 latach. Wszczepienie stymulatora zarówno w przypadku lekoopornej dusznicy bolesnej, jak i bólu neuropatycznego spo-wodowało istotne zmniejszenie odczuwanego przez pacjentów bólu, mierzonego w skali VAS. Jakość życia badana za pomocą kwestionariusza SF-36 zarówno u pacjentów z lekooporną dusznicą bolesną, jak i u pacjentów z bólem neuropatycznym poprawiła się istotnie.
Wnioski. SCS jest zabiegiem przynoszącym korzyści w postaci oszczędności zarówno w przypadku leczenia bólu
neuropatycznego, jak i lekoopornej dusznicy bolesnej. Po zastosowaniu SCS pacjenci odczuwają istotne zmniejsze-nie dolegliwości bólowych oraz ich jakość życia poprawia się (Adv Clin Exp Med 2012, 21, 5, 653–663).
Słowa kluczowe: analizy ekonomiczne, koszt–korzyść, ból neuropatyczny, lekooporna dusznica bolesna,
which reduces pain by at least 50%, only 30–40% of patients are treated successfully [4].
In non-pharmacological treatment, transcutane-ous electrical nerve stimulation blocks, or such inva-sive techniques as thermolesions are applied [4].
Spinal cord stimulation (SCS) is one of the most common surgical techniques undertaken in the treatment of neuropathic pain. The mechanism of action is based on the theory of gate control by Melzack and Wall, suggesting that stimulation of large diameter afferent nerve fibers inhibits con-duction of pain stimuli to the brain [6].
Conducted pain signals in the spinal cord are blocked by an electric stimulus. orthodromic transmission of impulses causes paresthesia. Stim-ulation of a-beta fibers of large diameter in dor-sal columns stimulates the activation mechanism of the gate, which inhibits transmission of pain in the fibers of small diameter in dorsal horns [7, 8]. Another mechanism explaining the effect of SCS is a segmental block of neuronal transmission of pain stimuli, which is caused by local changes in the spinal cord and the neurons responsible for leading pain [7, 8].
The indication for SCS is neuropathic pain re-sulting from an injury of the nervous system and ischemic pain in peripheral artery diseases and angina pectoris. The most frequent indication is FBSS: pain in the dorsal region associated with ad-hesive postinflammatory arachnoiditis, lower back pain or pain in the extremities caused by root or nerve injury resistant to conservative treatment and neurosurgical interventions in degenerative disc disease, CPRPS type I as causalgia, and type II, postherpetic neuralgia and phantom pain [7, 9].
A very important issue is the proper selection of patients. The criteria for inclusion into the SCS intervention provided by oakley are the following: duration of pain – 6 months, pain radiating below the knee root of greater pain intensity than the dorsal region, the lack of pain above dermatome TH10, at least one surgical intervention in anam-nesis, the patient’s consent, the results of a psycho-logical exam indicating the patient has strong mo-tivation to return to professional life [7, 10].
The effectiveness of SCS in neuropathic pain is high. Long-term studies estimate that in a well-se-lected group of patients, achieved pain reduction is about 50% with approximately 60–70% improve-ment of quality of life and reduction of intake of analgesics [9, 11].
Many studies have shown that neuropathic pain is not only a factor in lowering of the qual-ity of life related to health, but it also burdens the health care system and social security, generating costs in these sectors [12, 13]. The main costs are caused by direct medical care, loss of working
ca-pacity (affecting up to 43% of patients) [13] or re-duced productivity, as well as home care costs.
Refractory Angina Pectoris
Angina pectoris is a form of ischemic heart disease. Most damage is caused by atherosclerotic plaque, platelet activation and thrombus forma-tion. There are also other possible pathophysio-logical mechanisms such as coronary artery spasm, rapid progression of stenosis within the plaque, the primary thrombus, pulmonary artery or extracor-dial mechanisms [14]. It is manifested by frequent retrosternal severe pain, which can also occur at rest – without relation to exercise or stress [14–16]. Management is based on lifestyle modification, pharmacotherapy and the use of revascularization techniques such as implantation of coronary artery bypass graft (CABg) or coronaroplasty (PCI) us-ing balloon angioplasty, or stents and atherectomy [14–16].
8–10% of cases of unstable angina are refrac-tory to pharmacological treatments aimed at im-proving blood supply to the heart. SCS inhibits conduction of the electrical stimulation of pain stimuli and gives a chance for improvement for these patients [15]. SCS is eligible to patients with refractory angina who meet the following criteria:
– “Advanced changes in the coronary arteries confirmed by coronary angiography, which are not eligible for PCI or CABg;
– pain associated with coronary heart failure in NYHA III or IV grade;
– positive exercise test showing reversible ischemia;
– the optimal pharmacological treatment used at least a month before, involving at least two coro-nary drugs (beta-blockers, long acting nitrates, cal-cium channel blockers and angiotensin converting enzyme) in maximum doses” [17].
Factors excluding patients from SCS are also: an inability to complete the exercise test, myocardial infarction or unstable angina CCS class IV during the last three months, abnormalities in the spine, se-vere valvular defect, and age over 76 years [17].
SCS in refractory angina is based on the theory of gate control by Melzack and Wall and involves modulation of pain impulses flowing to the dorsal horn of the spinal cord. Consequently, following the increased release of gABA and increased se-cretion of endorphins, the effect is to reduce pain, reduce sympathetic activity, reduced myocardial demand for oxygen and development of myocar-dial microcirculation [15].
oxygen to the heart muscle, which resulted in pro-longation of exercise duration, improved heart rate and blood pressure, increased pain threshold and decreased duration of pain [18]. This procedure also resulted in improvement in the functioning of patients – who returned to active social life (pre-viously abandoned because of frustration and fre-quent hospitalizations) [18, 19].
Since the use of SCS does not completely abol-ish the sensation of pain – only changes its intensity and character – there is no possibility of a so-called “silent heart attack”. There are also no reports of the occurrence of any disturbances in patients who have both a pacemaker and neurostimulator (how-ever, patients should have only properly configured bipolar pacemakers implanted) [17, 18, 20].
Economic Analysis
in Healthcare
In highly developed societies economic condi-tions are the domain of all fields, including modern medicine. Expansion of new diagnostic and thera-peutic technologies brings growing financial needs. This fact, and the scarcity of financial resources, is a major challenge for health systems around the world, which must provide optimal community health care. This goal can only be achieved by ra-tionalizing expenditures, using medical knowledge that is economically supported [15, 21].
Access to medical care largely depends on the socio-economic development of a country, as well as on assumptions of health and social policy – which are linked to the macroeconomic factors of the functioning of the health care system. Bar-riers in access to medical care – giving rise to an increase in unfulfilled health needs – are the result of an irrational allocation of resources [21, 23].
Economic analyses facing the reality of cuts in funding for health care are intended to rationalize choices concerning the allocation of resources in health care. Carrying out analyses can also prove that the introduction of a specific diagnostic or therapeutic procedure will save money in the fu-ture and also give evidence of its clinical efficacy [21, 23].
Cost-benefit analysis (CBA) is considered to be a full-fledged economic evaluation. Analysis re-sults reveal whether the costs that the procedure absorbs are no greater than the benefits that can be achieved. It compares both the costs and ef-fects (benefits) of programs, which are expressed in monetary units. The direct benefits include the expenses that are avoided by implementing the program. The sphere of the patient’s productivity, expressed for example in the growth of earnings
or ability to work, are considered indirect benefits. Improving health and reducing pain and suffering are intangible benefits [21, 23, 24].
The result of a CBA may be the index value of cost-benefit ratio (costs / benefits ratio C / B) or net benefits (net benefit) – the difference between benefit and cost. When choosing from among ana-lyzed procedures we choose the one that has great-est net benefit or lowgreat-est C / B [15, 21, 23, 24].
Indirect costs are considered in two ways: within the health sector are the costs incurred in the years of life that are gained by the introduction of patient care; outside the health care sector are the costs related to the loss of the ability to take up paid work or decreased productivity resulting from the absence of the patient in the workplace [15, 21, 23, 26].
Recipients for whom economic tools are relevant are very numerous. Among them are both paying for medical services and patients – for both groups effi-cient and cost-effective treatment is important [21]. The aim of this study was to assess the costs of treat-ing patients with neuropathic pain and ischemic pain during the two years prior to SCS and to com-pare them with a two-year postoperative period.
The breakdown of costs in the period before and after surgery had to demonstrate:
– to what extent the cost of treatment will re-duce after implantation of a neurostimulator in the estimated five-year period?
– in what period after SCS its costs will offset reductions in treatment costs?
– which treatment method has the advantage, taking into account one-way sensitivity analysis of implant prices?
– if the use of SCS affects the quality of life of patients and the intensity of pain?
Material and Methods
The material for the study were the costs of treatment of patients with neuropathic pain and refractory angina pectoris in the two years prior to SCS and two-year postoperative period; SF-36 quality of life of patients forms, before and after SCS, and pain intensity measurements on the VAS scale before and after surgery.
The groups surveyed included 37 patients operated on due to pain in the period from 2002 to 2008 in the Department of Neurosurgery, 10th
Military Hospital in Bydgoszcz. The group of pa-tients with neuropathic pain included 25 papa-tients, while the group of patients with angina pectoris numbered 12.
years before and two years after SCS. The basis for calculating the costs for patients with neuropathic pain consisted of the following information: costs of medications (the amount of reimbursement paid by the payer – NHF), hospitalization costs – asso-ciated with treatment of pain, costs of outpatient specialist treatment, cost of rehabilitation, costs of the neurostimulator and its implantation.
The basis for calculating the costs for patients with ischemic pain in refractory angina pectoris consisted of the information concerning: costs of medications (the amount of reimbursement paid by the payer – NHF), costs of departure of medi-cal rescue teams, costs of treatment in hospital emergency departments, costs of hospitalization for cardiac branches, cost of outpatient specialist treatment, cost of the neurostimulator and its im-plantation.
The study used a cost–benefit analysis. Costs were understood as inputs consumed two years be-fore and two years after surgery of the spinal cord stimulator implanted in areas of cost assigned to each of the pain syndromes. Benefits were under-stood as the expenditures avoided through the in-troduction of SCS. The value of the costs and ben-efits was presented in monetary units [21, 23, 27]. Costs were estimated in the following five years (period due to the assumed average time of neurostimulator battery life [24]), there was a need for discounting operations (taking into account the calculation of time, which causes the value of goods in the possession of which we are today, tomorrow will be lower) [21, 22, 27]. one of the main assumptions of discounting is the declining value of money over time.
In order to carry out discounting operations it was necessary to take into account the discount rate, the number of years in which expenditure will be incurred and its future value [21, 27]. Then, a discounting factor (DF) for each year was calcu-lated according to the standard formula:
DF = 1 / (1 + r) ⁿ
Where “r” means the discount rate of 5% [22], and “n” – the year in which costs are incurred. Discounting rates for the next five years (included in Table 1), calculated on the basis of the pattern, were referenced to the annual costs and thus the obtained results showed the real value of incurred expenses in the future [21, 24, 27].
In the next stage of the calculation, a sensitiv-ity analysis was carried out. As a sensitive param-eter in the study, the authors selected the price of the neurostimulator. The scope of its volatility was defined as 30% and results were calculated assum-ing a sensitive parameter variability and stability of other parameters [21, 23, 24].
The study also involved pain intensity mea-sured in VAS. It is a 10-grade scale. Value 0 is at-tributed to lack of pain, while 10 – the strongest pain which the patient can imagine. Patients as-sessed pain before and after surgery SCS [28, 29].
The study also assessed the quality of life of pa-tients before and after SCS, using the SF-36 form (Qualimetric Incorporated No. 007635 QM). The questionnaire consists of 36 questions, divided in-to sub-scales examining eight areas: physical func-tioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional and mental health. The results were calculated accord-ing to the instructions and presented on a scale of 0 to 100, with a score of 100 meaning the best per-formance in a given field, and 0 very serious health condition due to pain or disability [30].
Statistical Analysis
For all calculations, the following statistical methods of data analysis were used. Descriptive statistics involved Shapiro-Wilk Test – to verify the normal distribution, Student’s T test for dependent samples, Wilcoxon’s Test of sequence of pairs. The level of significance was p < 0.05. The statistical analysis package was made with “Statistica”.
Results
Treatment of Neuropathic Pain
Table 2 shows the cost of treatment of 25 pa-tients with neuropathic pain two years before and two years after SCS surgery. SCS has no alterna-tive, all the patients before surgery receive the best treatment. In the case of lack of its effectiveness, patients are qualified for the SCS.
on average, a year of treatment for patients with neuropathic pain without the use of SCS is earmarked at 6312 PLN.
The cost of treatment in the next 5 years, adjusted for annual average increase in prices of
Table 1. Discounting factors [22]
Tabela 1. Współczynniki dyskontowania [22]
Years
(Lata) Discounting factors (Współczynniki dyskontowania)
1 0.952
2 0.907
3 0.864
4 0.823
drugs, totaled 32,464 PLN [21, 24]. After the dis-counting operations (based on disdis-counting factors from Table 1), the amount spent on the treatment of patients with neuropathic pain without SCS in the next 5 years amounted to 28,322 PLN.
In the structure of the cost of treatment of patients with neuropathic pain without the use of SCS, the majority involved the costs of medica-tions – 63%, then out-patient care 17%, and 10% for rehabilitation and hospitalization (Fig. 1).
The average annual cost of treating patients with neuropathic pain using SCS amounted to 5453 PLN (Table 2). The five-year cost, after taking into account increase in the prices of medications, amounted to 28,172 PLN, and after discounting this sum, amounts to 24,359 PLN [15, 21, 22, 24].
In the cost structure, after the application of SCS, a prominent place is occupied by medications 55%, successively hospitalization 26%, out-patient care 12% and rehabilitation 7% (Fig. 2).
Fig. 3 summarizes the structures of the cost of treatment of neuropathic pain in both methods. In all areas – with the exception of hospitalization – savings were observed (the largest on medications and outpatient specialist care).
The results were analyzed statistically (using the Shapiro-Wilk normality test and Wilcoxon’s sequence of pairs test), which showed there was a statistically significant difference between the expenditure on medications and outpatient spe-cialist care before and after SCS implantation. No significant changes were shown in the cost of
hospitalization and rehabilitation before and af-ter SCS.
The introduction of SCS as an alternative method of treatment of neuropathic pain resulted in savings of 13.2%.
The neurostimulator and its implantation car-ries a cost of 33,377 PLN. The price of the implant underwent sensitivity analysis [21, 22]. The results of the sensitivity analysis showed that the cost of the implant and the implant surgery will be reim-bursed: in the case of a constant price of the neu-roimplant – over 7 years; in the case of an increase in the price of the neuroimplant – within 9 years; in the case of a decrease in the price of the neu-roimplant – within 5.5 years.
To assess the quality of life, a SF-36 question-naire was used. For statistical purposes, the authors used the Shapiro-Wilk test of normal distribution and Wilcoxon’s test of sequence of pairs.
Statistical analysis showed that there is a sta-tistically significant difference between the qual-ity of life in the parameters: physical functioning, role physical, role emotional, bodily pain, general health, vitality and social functioning and mental health as measured before surgery, and the same parameters measured using the SF-36 after the op-eration.
In the area of physical functioning prior to surgery, patients rated the quality of life at 13.8, while after the treatment the point value increased to 29 (p < 0.000402).
Role physical was evaluated before surgery to
Table 2. Median cost of treatment of neuropathic pain with and without SCS
Tabela 2. Średni koszt leczenia bólu neuropatycznego bez i z zastosowaniem neuroimplantu
Costs during the two years prior to surgery – PLN
(Koszty w ciągu 2 lat przed operacją)
Implantation of the neurostimulator (Wszczepienie neuro-stymulatora)
Costs within two years after surgery – PLN
(Koszty w ciągu 2 lat po operacji)
Drug costs (Koszt leków) 7815 – 5863
Hospitalization costs
(Koszt hospitalizacji) 1284 – 2904
Cost of outpatient specialist treatment (Koszt specjalistycznego leczenia ambulato-ryjnego)
2167 – 1339
Cost of rehabilitation
(Koszt rehabilitacji) 1357 – 799
Costs of implantation of the
neurostimula-tor (Koszt wszczepienia neurostymulaneurostimula-tora) – 6436 –
Neurostimulator costs
(Koszt neurostymulatora) – 26941 –
22.25. After surgery, statistically significant im-provement was noted: 37.5 (p < 0.006706). In as-sessing the mental state, the point value of 27 be-fore surgery significantly increased to 45.44 (p < 0.000056).
Quality of life determined by pain experienced was assessed before treatment at 8.5. After sur-gery this parameter was estimated to be 30.6 (p < 0.000099).
Further parameters:
– general health: 23.5 initially, after surgery increased to 31.66 (p < 0.000182);
– vitality: before surgery, evaluated at 19.25, after surgery the patient’s functioning in this area improved to a point value of 33.4 (p < 0.000247);
– social functioning: in this area before sur-gery, patients functioned at a level of 12 points, and after the procedure this value increased sig-nificantly to 33.9 (p < 0.000301);
– role emotional: initially estimated at 22, after surgery increased significantly to 53.66 (p < 0.000060).
In summary, the introduction of SCS improved functioning in all areas covered in the SF-36 ques-tionnaire and it was a statistically significant im-provement.
Patients suffering from neuropathic pain eval-uated pain intensity using the VAS before and after surgery. For the statistical analysis, the
Shapiro-63% 10%
17%
10%
medicaons leki
hospitalizaon hospitalizacja
out-paent care ambulatoryjna opieka specjalistyczna
rehabilitaon rehabilitacja
55% 26%
12%
7%
medicaons leki
hospitalizaon hospitalizacja
out-paent care ambulatoryjna opieka specjalistyczna
rehabilitaon rehabilitacja
0 5000 10000 15000 20000 25000
medicaons leki
hospit alizaon hospit
alizacja
out-paent car e
opie
ka ambulatoryjna rehabilit
aon
rehabilit acja
costs without the use of SCS kwota leczenia bez zastosowania neuroimplantu
costs with the use of SCS kwota leczenia z zastosowaniem neuroimplantu
Fig. 1. The structure of costs of treatment of
neuro-pathic pain without spinal cord stimulation in a 5 year period
Ryc. 1. Struktura kosztów leczenia bólu
neuropatycz-nego bez zastosowania neuroimplantu w perspektywie 5 lat
Fig. 2. The structure of costs of treatment of
neuro-pathic pain using spinal cord stimulation in a 5 year period
Ryc. 2. Struktura kosztów leczenia bólu
neuropatycz-nego z zastosowaniem neuroimplantu w perspektywie 5 lat
Fig. 3. The comparison of cost structures of alternative
methods of treatment of neuropathic pain in a 5 year period
Rys. 3. Porównanie struktury kosztów alternatywnych
Wilk normality test and the Wilcoxon’s sequence of pairs test were used.
on average, the intensity of pain before sur-gery was assessed at 7.84. The level of pain de-creased significantly after the introduction of this alternative method of treatment and amounted to 4.12. It was a statistically significant change (p < 0.000027).
Treatment of Refractory
Angina Pectoris
Table 3 includes the averaged cost of treatment of 12 patients with refractory angina pectoris in-curred two years before and two years after SCS. Average annual spending on treatment of patients with refractory angina pectoris, treated without spinal cord stimulation is 5,075 PLN.
The study shows expenditures in the five-year period, hence an annual drug price increase of 3% was included [15, 21, 22, 24], which gave the to-tal amount of 25,745 PLN. The costs of treatment in the five years, after taking into account the de-creasing value of money over time, amounted to 22,036 PLN [21, 22, 27].
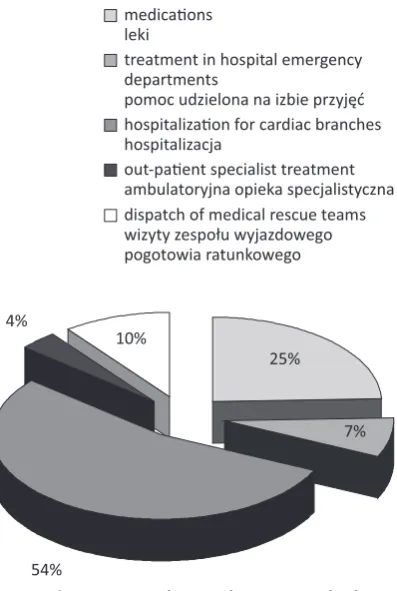
By analyzing the structure of expenditures on the treatment of patients with refractory angina without SCS, the most cost-intensive one is
hospi-talization – 54% of total expenditure, followed suc-cessively by medications – 25%, cost of dispatch of medical rescue teams –10%, cost of treatment in hospital emergency departments – 7% and out-patient care – 4% (Fig. 4).
The average annual cost of treatment of refrac-tory angina pectoris using SCS was 2,698 PLN. Af-ter including a 3% increase in the price of medica-tions, this resulted in 13,816 PLN [15, 21, 22, 24], and after discounting, 11,950 PLN.
In the cost structure, as for the period before the SCS operation, the largest costs are consumed by hospitalization – 48% of total expenditure. Sec-ond place was taken by medications – 40% and successive costs were dispatch of medical rescue teams – 6%, out-patient care – 4% and aid granted to the emergency room – 2% (Fig. 5).
Fig. 6 submits a statement of expenditures for both methods of treatment. The greatest differences were observed in the cost of treatment in hospital emergency departments, dispatches of emergency medical teams and in hospitalization, for treatment of patients with refractory angina with SCS.
An inventory of the cost of treating patients with refractory angina pectoris by the two alterna-tive methods have shown that SCS therapy is more favorable from an economic standpoint, and the percentage difference in spending on treatment of patients after implantation is 46%.
Table 3. Median cost of treatment of refractory angina pectoris with and without SCS
Tabela 3. Średni koszt leczenia lekoopornej dusznicy bolesnej bez i z zastosowaniem SCS Costs during the
two years prior to surgery – PLN (Koszty w ciągu 2 lat przed operacją)
Implantation of the neurostimula-tor (Wszczepienie neurostymulatora)
Costs within two years after surgery – PLN
(Koszty w ciągu 2 lat po operacji)
Cost of medications
(Koszt leków) 2376 – 2086
Cost of treatment in hospital emergency departments
(Koszt leczenia na oddziale intensywnej terapii) 767 – 90
Costs of hospitalization for cardiac branches
(Koszt hospitalizacji na oddziałach kardiologicznych) 5580 – 2634
Cost of out-patient treatment
(Koszt leczenia ambulatoryjnego) 375 – 227
Cost of dispatch of medical rescue teams
(Koszt wysłania zespołu ratownictwa medycznego) 1051 – 359
Cost of implantation of the neurostimulator
(Koszt wszczepienia neurostymulatora) – 5013 –
Neurostimulator costs
(Koszt neurostymulatora) – 31378 –
Sum
The results were subjected to statistical analy-sis, which showed a statistically significant dif-ference between the cost of treatment in hospital emergency departments, the cost of dispatches of emergency medical teams and spending on medi-cations before and after SCS.
There were no statistically significant changes in the cost of hospitalization before and after SCS. There were also no statistically significant changes in the cost of outpatient specialist care before and after surgery, but there is a statistical tendency for their reduction.
The implant and the implant surgery is at a cost of 36,391 PLN [21]. Results of a sensitiv-ity analysis [21] showed that the cost of the im-plant and the surgery will be offset: in the case of a constant price of the neuroimplant – over 3 years; in the case of an increase in the price of the neuroimplant – within 4 years; in the case
Fig. 4. The structure of costs of treatment of refractory
angina pectoris without using spinal cord stimulation in a 5 year period
Ryc. 4. Struktura kosztów leczenia lekoopornej
dusznicy bolesnej bez zastosowania neuroimplantu w perspektywie 5 lat
Fig. 5. The structure of costs of treatment of refractory
angina pectoris using spinal cord stimulation in a 5 year period
Ryc. 5. Struktura kosztów leczenia lekoopornej
dusznicy bolesnej z zastosowaniem neuroimplantu w perspektywie 5 lat
25%
7%
54% 4%
10%
medicaons leki
treatment in hospital emergency departments
pomoc udzielona na izbie przyjęć hospitalizaon for cardiac branches hospitalizacja
out-paent specialist treatment ambulatoryjna opieka specjalistyczna dispatch of medical rescue teams wizyty zespołu wyjazdowego pogotowia ratunkowego
40%
2% 47%
4%
7% medicaons leki
treatment in hospital emergency departments
pomoc udzielona na izbie przyjęć hospitalizaon for cardiac branches hospitalizacja
out-paent specialist treatment ambulatoryjna opieka specjalistyczna dispatch of medical rescue teams wizyty zespołu wyjazdowego pogotowia ratunkowego
0 2000 4000 6000 8000 10000 12000 14000
medicaons leki
treatment in hospi tal
emer
gency departments
pomoc udzielona na izbie przyję ć
hospit alizaon f
or car diac b
ranches hospit
alizacja
out-paent specialis t treatment
ambulatoryjna opiek a specjalis
tyczna
dispat ch of medical
rescue t eams
wizyty z espołu wyjaz
dowego
pogotowia ratunk
oweg o costs without the use of SCS kwota leczenia bez zastosowania neuroimplantu
costs with the use of SCS kwota leczenia z zastosowaniem neuroimplantu
Fig. 6. The comparison of cost structures of alternative
methods of treatment of refractory angina pectoris in a 5 year period
Ryc. 6. Porównanie struktury kosztów alternatywnych
of a decrease in the price of the neuroimplant – within 2.5 years.
To evaluate the quality of life of patients with angina pectoris, a SF-36 form was used. Statisti-cal analysis was performed using the Shapiro-Wilk normality of distribution test, the Student’s t test and the Wilcoxon’s test.
There is a statistically significant difference be-tween the quality of life in the parameters: physical functioning, mental health, bodily pain, general health, vitality and social functioning, measured before surgery and these parameters measured af-ter the operation. There were no statistically signif-icant changes in the parameters role physical and role emotional, measured before surgery and the same parameters measured after the operation.
Assessment of physical functioning prior to surgery was 42 and was significantly lower com-pared to after SCS – 57.08 (p < 0.030330).
In the area of operation associated with the role physical, the result before treatment was 27.08 and after surgery rose slightly to 29.16. It was not a statistically significant change (p < 0.600180).
In assessing mental health, the point value of 38 before surgery significantly increased to 53.66 (p < 0.007649).
The area of bodily pain before surgery was rated at 9.58, and its value increased significantly after surgery to 60.83 (p < 0.002218).
general health before surgery was rated on the average of 16.66, and after surgery was on the or-der of 32.63. It was a statistically significant change (p < 0.003346).
In the area of vitality, before treatment the val-ue was 21.66. After the treatment it had increased significantly to 47.50 (p < 0.000004).
Quality of life expressed in functioning associ-ated with role emotional, before the treatment was assessed at 50 and after surgery at 77.77 (this was not statistically significant) (p < 0.090970).
In summary, the introduction of alternative treatment – which is SCS – for refractory angina pectoris has brought improvement in functioning in all areas, but in the areas associated with role physical and role emotional were not statistically significant.
Patients with refractory angina pectoris inde-pendently assessed pain intensity with VAS. For the statistical analysis, the Shapiro-Wilk normal-ity of distribution test and Wilcoxon’s sequence of pairs test were used.
on average, the intensity of pain before sur-gery was assessed at 6.91. The level of pain de-creased significantly after the introduction of SCS and amounted to 2.33. It was a statistically signifi-cant change (p < 0.002218).
Discussion
SCS in Poland is still a rare procedure, carried out in only a few centers. There is no national pub-lication covering the analysis of treatment costs of a larger group of patients suffering from chronic pain syndromes than the group covered by the re-search in this study. In many centers abroad, where the importance of economic analysis in the health sector is recognized, studies conducted indicate that SCS is a cost-effective method and improves the quality of life of patients [8, 10–12, 18, 19].
Cost analysis was presented from the perspec-tive of the payer, based on data available from the Headquarters of NHF.
The need to undertake this type of research, among others, was emphasized by the 7th Congress
of the Polish Society of the Study of Pain, held in September 2010 in gdansk. Research on cost-ef-fectiveness in various countries is a very important contribution to the medical care sector. Various health insurance schemes, as well as different ways of financing SCS, require research into cost effec-tiveness at the national level, with the increasing popularity of this method in a growing number of patients undergoing this procedure.
In assessments of modern medical technol-ogy, all its aspects should be taken into account. Cost analysis is a fundamental step that should be taken when selecting therapy. Selection of an appropriate methodology, passage of time in pro-spective studies and examination of the behavior of sensitive parameters is essential in a proper economic analysis. However, a holistic approach to a patient’s health forbids the limitation only to its physicality. The spheres of mental and social functioning complete the picture of the usefulness of therapy. It should therefore complement the analysis of tools for testing the quality of life and pain perception. Thus, the analysis gives the full data that planners and decision makers at various levels of the organization and implementation of health care should take into account when allocat-ing resources [15, 21, 23–25, 27].
References
[1] Merskey H, Bogduk N: Classification of Chronic Pain, 2nd ed. Seattle, WA 1994, IASP Press.
[2] Dobrogowski J, Kocot-Kępska L: Różne zespoły bólu neuropatycznego występujące u jednego pacjenta – opisy
[3] Wordliczek J, Dobrogowski J: Mechanizmy powstawania bólu. In: Leczenie bólu. Wydawnictwo Lekarskie PZWL 2007, Warszawa.
[4] Suchorzewski M, Wujtewicz M: opioidy w leczeniu bólu neuropatycznego. Med Paliatywna Prakt 2007, 1,
49–53.
[5] Bradley WG, Daroff RB, Fenickel G.M, Jarnovic J: Neurologia w praktyce klinicznej. Tom 1, Czelej, Lublin
2007.
[6] Melzack R, Wall PD: Pain mechanisms: a new theory. Science 1965, 150, 971–979.
[7] Harat M (red.): Neurochirurgia czynnościowa. Bydgoszcz 2007.
[8] Linderoth B, Meyerson BA: Spinal cord stimulation: mechanism of action. In: Surgical management of pain. Eds.:
Burchiel KJ. Thieme, New York 2002, 505–526.
[9] Ząbek M, Sławek J, Harat M, Koszewski W, Opala G, Friedman A: Stymulacja mózgu i rdzenia kręgowego
w leczeniu zaburzeń ruchowych oraz zespołów bólowych – podstawy teoretyczne i zalecenia praktyczne. Neurol Neurochir Pol 2006, 40, 1–9.
[10] Oakley JC: Spinal cord stimulation for the treatment of chronic pain. In: Neurosurgical pain management. Ed.:
Follet KA. Elsevier 2004, 131–143.
[11] Van Buyten JP, Van Zundert J, Vueghs P (ed.): Efficacy of spinal cord stimulation: 10 years of experience in
a pain centre in Belgium. Eur J Pain 2001, 5, 299–307.
[12] O’Connor AB: Neuropathic pain: a review of the quality of life impact, costs and cost-effectiveness of therapy.
Pharmacoeconomics 2009, 27, 95–112.
[13] McCarberg BH, Billington R: Consequences of neuropathic pain: quality of life issues and associated costs. Am
J Managed Care 2006, 12, 263–268.
[14] Januszewicz W, Kokot F: Interna. PZWL, Warszawa 2004.
[15] Cuprych A: ocena ekonomiczna efektywności leczenia stymulatorem rdzenia lekoopornej dusznicy bolesnej. Toruń 2006.
[16] Wysocki H: Zaawansowana choroba niedokrwienna serca – niekonwencjonalne metody leczenia. Przew Lek 2003,
6, 5.
[17] Rusicka-Piekarz T, Topoliński B, Harat M: Elektrostymulacja rdzenia kręgowego jako alternatywna metoda
leczenia dolegliwości bólowych w dusznicy bolesnej. Folia Cardiol 2004, 11, 327–335.
[18] Borjesson M, Andrell M, Lundberg D, Manheimer C: Spinal cord stimulation in severe angina pectoris – A
sys-tematic review based on the Swedish Council on Technology assessment in health care report on long-standing pain. Pain 2008, 140, 501–508.
[19] Hautvast RWM, Blanksma PK, de Jongste MJL (ed.): Effect of spinal cord stimulation on myocardial blood
flow assessed by positron emission tomography in patient with refractory angina pectoris. Am J Cardiol 1996, 77, 462–467.
[20] Sokal P, Harat M, Rusicka-Piekarz T: Stymulacja rdzenia kręgowego w krańcowej dusznicy bolesnej. Neurol
Neurochir Pol 2005, 39, 417–419.
[21] Orlewska E: Wytyczne Polskiego Towarzystwa Farmakoekonomicznego przeprowadzania oceny ekonomicznej
technologii medycznych. Warszawa 2009. www.farmakoekonomika.pl.
[22] Davies D: Sztuka zarządzania finansami. PWN, Warszawa 1993, s. 174.
[23] Drummond MF (ed.): Metody badań ekonomicznych programów ochrony zdrowia. Via Media, gdańsk 2003.
[24] Klewenhagen A: ocena ekonomiczna efektywności leczenia współczesnymi neuroimplantami wybranych chorób
ośrodkowego układu nerwowego. gdańsk 2005.
[25] Krajewski K, Wójtowicz M (ed.): Zarządzanie finansami placówek medycznych, Instytut Przedsiębiorczości
i Samorządności, Warszawa 2001.
[26] Jaeschke R, Guyatt G, Cook D: Analiza ekonomiczna – ocena i zastosowanie wyników. Med Prakt 1999, 4, 155–
162.
[27] Getzen T: Ekonomika Zdrowia, Wydawnictwo Naukowe PWN, Warszawa 2000.
[28] Cepuch G, Wordliczek J, Golec A: Wybrane skale do badania natężenia bólu u młodzieży – ocena ich
przydatno-ści. Pol Med Paliatywna 2006, 5, 108–113.
[29] Strong J, Sturgess J, Unruh AM, Vicenzino B: Kliniczna ocena i pomiar bólu. In: Ból podręcznik dla terapeutów.
Ed.: Strong J. Elsevier 2007, Churchill Livingstone, 127–154.
[30] Ware EJ, Kosinski M, Bjorner JB, Turner-Bowker DM, Gandek B, Maruish MB: SF 36 v 2 Health Survey:
Administration guide for clinical trial investigators. RI: QualityMetric Incorporated 2008 Lincoln.
Address for correspondence:
Aleksandra Harat Sandomierska 16 85-830 Bydgoszcz Poland
Tel.: +48 52 585 54 08
E-mail: [email protected], [email protected]
Conflict of interest: None declared