Cite this article : Cekmez F, Erdinc HK, Arcagok BC, et al. Evaluation the effectiveness of Multiplex PCR system(Septitest) for the rapid detection of blood pathogens in late onset sepsis of Extremely Low Birth Preterms. J J Med Diagnosis and Image. 2019; 5(1):023.
Original Article
Evaluation the effectiveness of Multiplex PCR system(Septitest) for the rapid detec
-tion of blood pathogens in late onset sepsis of Extremely Low Birth Preterms
Cekmez F1*, Erdinc HK2, Arcagok BC2, Ozdek S2
1Department of Neonatology, Acibadem Mehmet Ali Aydınlar University School of Medicine, Istanbul, Turkey.
2Department of Neonatology, Acibadem Altunizade Hospital, Istanbul, Turkey
*Corresponding author: Cekmez F, Department of Neonatology, Acibadem Mehmet Ali Aydınlar University School of Medi-cine, Istanbul, Turkey, Email: [email protected]
Received Date: 03-28-2019 Accepted Date: 04-12-2019 Published Date: 04-18-2019 Copyright: © 2019 Cekmez F
Introduction:
Sepsis is a clinical syndrome, caused by many
physio-logic changes of systemic inflammation, which are due to
the proven or suspected infection [1]. Sepsis is still a ma-jor cause of morbidity and mortality in the neonatal period, particularly in preterm infants. Early signs and symptoms of infection are generally occult and can easily be
over-looked. However, although the onset of the disease is often unspecific, the clinical course may be fulminant, leading to
septic shock, disseminated intravascular coagulation, and
death within hours of initial clinical symptoms [2]. Because of difficulties in determining the infections, many biomark
-ers are being searched for early diagnosis, but none of them
could have reached enough achievement up to now. Thus, much efforts have been focused to find effective and sensi -tive markers for sepsis [3].
Although many new markers were found and used to de -termine the infections, blood culture remains the`gold-stan-dard`for the diagnosis of bloodstream infection, but, results
of blood culture may take up to 48–72 hours until positive results can be reported [4, 5]. Because this reason, begin -ning of proper treatment may be delayed. Researchings are focused on speeding up the determination process.
Advances in molecular microbiology have provided
cul-Jacobs Journal of Medical Diagnosis and Medical Imaging
Abstract:
Sepsis is still a major cause of morbi=dity and mortality in the neonatal period, particularly in preterm infants.
Because of difficulties in determining the infections, many biomarkers are being searched for early diagnosis. We evaluated the clinical value of a multiplex-real-time-PCR assay in episodes of suspected late-onset sepsis in ELBW preterms. A total of 30 ELBW preterm with high probable sepsis were included in the study. The qPCR in this study showed 46% positivity in patients but in positivity in blood culture is %35. The concordance of positive blood cultures to detect the bacteria in the same multiplex qPCR in patients with study group was 76%.
Our studies showed that multiplex PCR tests can be a potentially useful tool in preterm sepsis.
Jacobs Publishers
ture-independent molecular assays for rapid diagnosis of the causative agent of infection. PCR-assays developed for
specific detection of pathogens in the blood were described as early as 1993 [6,7]. Studies demonstrated that PCR can give results from micro volume samples as small as100μl [8] and this is very important advantage in ELBW preterm besides rapid result. We evaluated the clinical value of a
multiplex-real-time-PCR assay in episodes of suspected
late-onset sepsis in ELBW preterms.
Material and Methods: Study population
The present study enrolled ELBW preterm babies with late onset sepsis (6 days |<), admitted to nicu, in Tekden Hos
-pital and Acıbadem Altunizade Hos-pital between 2016 and 2018. Preterms with congenital anomalies or maternal chronical disorders were excluded. According to [9] the ba
-bies were classified into four groups as group 1 [high prob
-able sepsis], group 2 (prob-able sepsis), group 3 (possible sepsis) and group 4 (no sepsis) (Table 1) [10]. A total of 30 ELBW preterm with high probable sepsis were includ -ed in the study. Ethical approval has been receiv-ed from Acibadem University.
Blood samples
Blood was collected from preterm babies the first day of sepsis (pre-treatment). . After clotting, the serum was sep
-arated and immediately explored for analyses. Whole blood cell count (WBC) was performed using an automatic count
-er, Cell Dyn 3,700. Aseptic non-touch venepuncture was per
-formed by trained clinical study staff: 0.5 ml blood (EDTA microfuge tube) for quantitative PCR (all infants), 0.5–1.0 ml whole blood inoculated into a single pediatric blood culture (BC) bottle (BACTEC Peds Plus, Becton Dickinson, Sparks MD; all cases and control infants clinically unwell on assessment), and 0.5 ml (serum microfuge tube) for C-reac
-tive protein (CRP) (all infants, COBAS, Roche Diagnostics).
Multiplex-PCR
Samples were studied in Gelişim Laboratory by using Sep
-sitest. SepsiTest is a CE-marked PCR test for detecting bac
-terial and fungal DNA in 1ml of K-EDTA- (potassium-EDTA) or citrate-treated whole blood. The test is able to identify
species from more than 200 genera of bacteria and 65 gen
-era of fungi. SepsiTest involves three distinct processes:
extracting and purifying microbial DNA using
centrifuga-tion, universal PCR and Sanger sequencing. The PCR result
is available after 4 hours in optimal conditions, although it
could take longer depending on laboratory workflow, and indicates whether bacteria or fungi are present in the sam
-ple. Amplicons from positive samples are then sequenced to confirm the PCR result and to determine which bacterial or
fungal species are present.
Statistical analysis
Descriptive data were expressed as mean ± standard devia
-tion. Chi-square or Fisher’s Exact test was used to compare categorical variables, and the Wilcoxon Rank Sum test was used to compare continuous variables. The correlations among numerical data were analysed by the Pearson cor
-relation coefficient (r). A p value < 0.05 was considered sta
-tistically significant. Statistical analysis was performed with SPSS 12.0 software (IBM, Chicago, IL, USA).
Results:
A total of 30 ELBW preterm with high probable sep
-sis were included in the study. Two of them who met the exclusion criteria (1 who had congenital heart disease and 1 who had intestinal malformation) were excluded. Clin
-ical demographics and laboratory findings are gestational weeks (28.7 ± 2 w), gestational weights (870 ± 60 g), white blood cell count /mm3 ( 11,720 ± 3,230), CRP (mg/dl) (16.7 ± 4.8), I/T ratio (0.04 ± 0.015). The qPCR in this study showed 46 % positivity in patients (when using universal primer) but in positivity in blood culture is %35. The con -cordance of positive blood cultures to detect the bacteria in
the same multiplex qPCR in patients with study group was 76%.
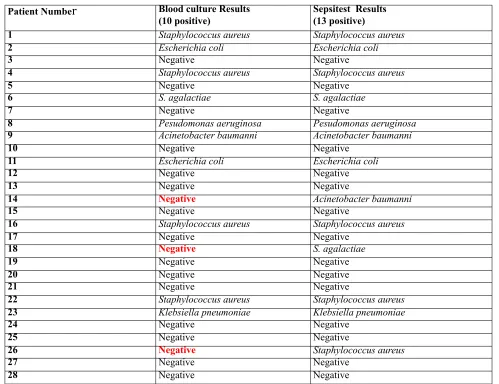
After the analysis of blood culture, there were 2 samples were positive for E. Coli (%7.1), 4 samples were positive for S. Aureus (%14.2), 1 samples were positive for for S. Agalactiae(%3.5), 1 sample were positive for P. Aeru
samples were positive for S. Aureus (% 17.8), 2 samples were positive for S. Agalactiae(%7.1), 1 sample were pos-itive for P. Aeruginosa (%3.5), 1 sample were pospos-itive for K. Pneumoniae (%3.5), 2 sample were positive for
A.bau-manni (%7.1). Table 2 shows the final results of the blood culture and multiplex qPCR in the selected population. Discussion:
Neonatal mortality, due to the infections, persists as a major problem at global public health [11]. The diag
-nosis of infectious as a co-morbidity in the sick newborn through clinical signs or conventional laboratory and cul
-ture techniques are very difficult [12]. Thus, new diagnostic techniques, especially the molecular methods supply to de
-termine more faster, more specific and more sensitive than blood culture in the diagnosis of neonatal sepsis [13,14]. It
seems to have the potential to replace the current
microbi-ological methods.
Microbiological blood culture is still considered the gold standard in the diagnosis of neonatal sepsis, but its sensi
-tivity is usually low in newborns, regardless of its delay of 48–72 hours in showing positive results [13].
In this study, the blood culture positivity rate was 35%, it seems high than literature because we selected only patients with laboratory positive findings but described higher rates of positivity in their blood cultures, such as the 23.59% found by Patel et al. [15 ] and 42% observed by Hussein and Khaled [16]. In some studies, positivity of blood culture rate in neoatal sepsis is aproximately %4-5 [17]. The low positivity rate can be influenced by several factors, such as the technique used in the analysis of cul
-tures in each service, the existing limitation on the blood volume obtained for culture due to weight and clinical con
-dition of the patient (which was most often premature), and the observed high rate of use of antenatal antibiotics [16]. Current studies showed that mutiplex pcr devices have higher and fast spesifity and sensitivity comparing to blood cultures [13]. The qPCR in this study showed 46 % positiv -ity in patients (when using universal primer) but in
posi-tivity in blood culture is %35. The concordance of positive blood cultures to detect the bacteria in the same multiplex qPCR in patients with study group was 76%, a result similar to that found by Bloos et al.[18].
Although the Sepsitest PCR system includes fungal pathogens frequently encountered in neonatal intensive
care units, the potential advantage of PCR based diagnostics could not be evaluated since no episodes of fungal sepsis occurred in our study. The main reason of this conclusion was caused by the practice of fluconazole prophylaxis in all preterm infants below 28 weeks of gestational age at our
neonatal intensive care unit, which represent the group
with the highest risk for fungal sepsis among neonatal units
[19].
Current studies showed that multiplex PCR tests
can be a potentially useful tool in clinical emergencies in
comparison with microbiological culture-based methods,
with the objective of facilitating progression to
antimicro-bial therapy that is specific, which is especially relevant in newborns, as empirical treatment is often abused in neona -tal intensive care units. A further limitation is the fact that
multiplex PCR tests still remain a cost- and staff- intense procedure, as PCR costs are 5-times higher compared to conventional blood cultures costs, and staff needs special cost- and time-intense training. Because of this reason, it
seems that there is necessity to solve the cost-effectivity problem to use this tool in our clinical practise.
Table 1:
Groups Criteria
Group 1 (high probable sepsis) At least 3
sepsis-relat-ed clinical signs,a CRP > 1 mg per 100 ml At least 2 other altered serum parameters in addition to CRPand Blood cul -ture; negative or positive
Group 2 (probable sepsis) Less than sepsis-related clini
-cal signsa CRP > 1 mg per 100 ml At least 2 other altered se
-rum parameters in addition to CRP Blood culture; negative Group 3 (possible sepsis) Less than sepsis-related clin
-ical signs CRP < 1 mg per 100 ml Less than other altered serum parameters Blood culture; negative
Group 4 (no sepsis) No sepsis related clinical signsa CRP < 1 mg per 100 ml No altered serum parameters
CRP, C-reactive protein.
a Sepsis-related clinical signs: temperature instability, need for supplemented oxygen, need for ventilation, tachycardia/ bradicardia, hypotension, feeding intolerance, abdominal distention. bSerum parameters other than CRP: white blood cell count, absolute neutrophil count, platelet count
Jacobs Publishers
References:
1. Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and or
-gan dysfunction in pediatrics. Pediatr Crit Care Med 2005; 6(1): 2-8.
2. Ceccon MEJR. New Perspectives in Neonatal Sepsis. Pedi
-atria 2008; 30: 198-202.
3. Ng PC. Diagnostic markers of infection in neonates. Arch
Dis Child Fetal Neonatal Ed 2004; 89(3): 229-235.
4. Peters RP, van Agtmael MA, DannerSA, et al. New devel -opments in the diagnosis of bloodstream infections. Lancet
Infect Dis 2004; 4(12): 751–760.
5. Mussap M, Molinari MP, Senno E, et al. New diagnostic
tools for neonatal sepsis: the role of a real-time polymerase
chain reaction for the early detection and identification of
bacterial and fungal species in blood samples. J Chemother 2007; 2: 31–34.
6. Song JH, Cho H, Park MY, et al. Detection of Salmonella typhi in the blood of patients with typhoid fever by poly
-merase chain reaction. J Clin Microbiol 1993; 31(6):1439–
1443.
7. Klaschik S, Lehmann LE, Raadts A, et al. Detection and differentiation of in vitro-spiked bacteria by real-time PCR
and melting-curve analysis. J Clin Microbiol 2004; 42(2): 512–517.
8. Kasper DC, Altiok I, Mechtler TP, et al. Molecular Detection of Late-Onset Neonatal Sepsis in Premature Infants Using Small Blood Volumes: Neonatology 2013; 103(4): 268–273.
9. Gitto E, Karbownik M, Reiter RJ, et al. Effects of melatonin treatment in septic newborns. Pediatr Res 2001; 50(6): 756-760.
Table 2:
Patient Numbe
Shows the final results of the blood culture and multiplex qPCR in the selected population.
r
Blood culture Results(10 positive) Sepsitest Results(13 positive)
1 Staphylococcus aureus Staphylococcus aureus
2 Escherichia coli Escherichia coli
3 Negative Negative
4 Staphylococcus aureus Staphylococcus aureus
5 Negative Negative
6 S. agalactiae S. agalactiae
7 Negative Negative
8 Pesudomonas aeruginosa Pesudomonas aeruginosa
9 Acinetobacter baumanni Acinetobacter baumanni
10 Negative Negative
11 Escherichia coli Escherichia coli
12 Negative Negative
13 Negative Negative
14 Negative Acinetobacter baumanni
15 Negative Negative
16 Staphylococcus aureus Staphylococcus aureus
17 Negative Negative
18 Negative S. agalactiae
19 Negative Negative
20 Negative Negative
21 Negative Negative
22 Staphylococcus aureus Staphylococcus aureus
23 Klebsiella pneumoniae Klebsiella pneumoniae
24 Negative Negative
25 Negative Negative
26 Negative Staphylococcus aureus
27 Negative Negative
10. PCR İLE İLGİLİ
11. Thaver D, Zaidi AKM. Burden of Neonatal Infections in Developing Countries: A Review of Evidence From Commu
-nity-Based Studies. Pediatr Infect Dis J 2009; 28(1): 3-9. 12. Edmond K, Zaidi A. New approaches to preventing, diag
-nosing, and treating neonatal sepsis. PLoS Med 2010; 7(3): e1000213.
13. Pammi M, Flores A, Leeflang M, et al. Molecular Assays in the Diagnosis of Neonatal Sepsis: A Systematic Review and Meta-analysis. Pediatrics 2011; 128(4): 973-985.
14. Al-Zahrani AK, Ghonaim MM, Hussein YM, et al. Evalu -ation of recent methods versus conventional methods for
diagnosis of early-onset neonatal sepsis. J Infect Dev Ctries 2015; 9(4): 388-393.
15. Patel D, Nimbalkar A, Sethi A, et al. Blood Culture Iso
-lates in Neonatal Sepsis and their Sensitivity in Anand
Dis-trict of India. Indian J Pediatr 2014; 81(8): 785- 790. 16. Hussein AB, Khaled MA. C-reactive protein in Neonates With Suspected Septicemia. RMJ 2007; 32: 24-27.
17. Al-Taiar A, Hammoud MS, Thalib L, et al. Pattern and eti
-ology of culture-proven early-onset neonatal sepsis: a five-year prospective study. Int J Infect Dis 2011; 15(9): 631-634
18. Bloos F, Hinder F, Becker K, et al. A multicenter trial to compare blood culture with polymerase chain reaction in severe human sepsis. Intensive Care Med 2010; 36(2): 241-247.
19. Lee J, Kim HS, Shin SH, et al. Efficacy and safety of fluco