KNOWLEDGE AND COMPETENCY OF MIDWIVES IN IMPLEMENTATION OF ACTIVE MANAGEMENT OF THIRD STAGE OF LABOUR IN MERU
COUNTY, KENYA
BENSON KIOGORA MUGAMBI (BSC.NURSING) Q139/CE/20845/2012
A THESIS SUBMITTED IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF MASTER OF
PUBLIC HEALTH (REPRODUCTIVE HEALTH) IN THE SCHOOL OF PUBLIC HEALTH OF KENYATTA UNIVERSITY.
DECLARATION
This thesis is my original work and has never been presented to any other institution of Higher Learning for an academic Award.
Signature ……….………... Date………...
Benson K. Mugambi -Q139/CE/20845/2012 Department of Population and Reproductive Health
SUPERVISORS
We confirm the work reported in this thesis was carried out by candidate under our supervision as the University Supervisor.
Signature ……….………... Date………...
Dr. Daniel Muia, PhD Department of Sociology
Signature ……….………... Date………...
DEDICATION
AKNOWLEDGEMENTS
I wish to acknowledge my thesis mentors and supervisor Dr Daniel Muia and Dr Onditi Kodhiambo of Kenyatta University for their support and guidance through my thesis writing. Both availed themselves when there was need and helped me in fine tuning my work and more so, creating their time for one on one discussions.
Am also grateful to the entire staff of Meru teaching and referral hospital (MTRH), Kanyakine level four hospital, Gatimbi health centre and Nkubu mission hospital particularly to the midwives who expressed much interest in my study and voluntarily gave their consent. Special thanks also goes to Kenya medical training college of Meru for their input and encouragement as colleagues, and more so for granting me permission during data collection period
I greatly acknowledge the work done by my thesis assistants during the period of data collection and their effort in ensuring the activity was complete as per the stipulated time.
My special gratitude also goes to all the respondents who agreed to participate in the study. To my classmates and Kenyatta university library staff thanks for all the support provided.
TABLE OF CONTENTS
DECLARATION ... ii
DEDICATION ... iii
AKNOWLEDGEMENTS ... iv
LIST OF TABLE ... ix
LIST OF FIGURE ... xi
ABBREVIATION AND ACRONYMS ... xii
ABSTRACT ... xv
CHAPTER ONE ... 1
INTRODUCTION ... 1
1.1 Background information ... 1
1.2 Statement of Research Problem ... 3
1.4 Research Questions ... 5
1.5 Hypothesis ... 5
1.6Broad Objective ... 6
1.6.1 Specific Objectives ... 6
1.7 Significance of the Study ... 6
1.8 CONCEPTUAL FRAME WORK ... 7
CHAPTER TWO ... 10
2.1 Introduction ... 10
2.1.0. Scientific evidence supporting active management of third stage of labor (AMTSL) ... 10
2.1.1 Practice ... 13
2.3 Challenges affecting midwives competency in implementation of AMTSL ... 17
2.3.0 Knowledge as a factor in AMTSL ... 19
2.3.1 Training of Staff in regard to care delivery. ... 19
2.3.2 Competency and work experience ... 20
CHAPTER THREE ... 21
RESEARCH METHODOLOGY ... 21
3.1 Study Design ... 21
3.2 Variables ... 21
3.2.1 Independent variables ... 21
3.2.2 Dependent variable ... 22
3.2.3 Study Area ... 22
3.3.0 Inclusion criteria ... 23
3.3.1Exclusion criteria ... 23
3.4 Sampling Technique ... 23
3.5 Sample Size and Determination ... 24
3.6 Validity and Reliability of Research ... 26
3.7 Data Collection Technique ... 26
3.8 Primary Data ... 27
3.9 Data Collection Instruments ... 27
3.10 Data Cleaning and Storage ... 27
CHAPTER FOUR ... 29
4.1 Introduction ... 29
4.3 Demographic Information ... 30
4.4 Knowledge of respodents………..38
4.4.1 Training information on AMTSL………..39
4.6 knowledge on AMSTL by Midwives in Active Management of Third Stage of Labor ... 44
4.7 Association between recommended route for uterotonicd drug and the most recommended dose………..46
4.7 Guidelines, Motivations and Views behind AMSTL Implementation ... 53
CHAPTER FIVE: DISCUSSION, SUMMARY, CONCLUSION ANDRECOMMENDATION………...63
5.0 Introduction ... 63
5.10 Discussion………...63
5.2 summary………....67
5.3 conclusion……….69
5.4 recommendation………...70
5.5 Recommendation for further studies………70
REFERENCE/CITATION ... 71
CONSENT FORM FOR THE RESPODENTS ... 76
APPENDIX II ... 77
QUESTIONARE TO THE MIDWIVES, MERU COUNTY HEALTH FACILITIES ... 77
Observation checklist Client (mother) consent form ... 82
APPENDIX V :MAP (LOCATION AND DIRECTION TO MERU COUNTY) ... 84
APPENDIX VI: RESEARCH CLEARANCE (NACOSTI)………85
LIST OF TABLES
TABLE 1.0: RESPONDENTS’ AGE ... 30
TABLE 2: HIGHEST EDUCATION LEVEL ... 32
TABLE 3;HIGHEST MIDWIFERY EDUCATION ... 32
TABLE 4: CROSS TABULATION BETWEEN HIGHEST EDUCATION LEVEL & RECOMMENDED DOSE FOR SELECTED DRUG ... 34
TABLE 5: JOB PROFILE ... 35
TABLE 7: YEAR OF AMTSL EXPERIENCE & RECOMMENDED DOSE FOR SELECTED DRUG ... 36
TABLE 8: CROSS TABULATION RESULTS BETWEEN HIGHEST EDUCATION LEVEL & DURATION OF MIDWIFERY PRACTICE ... 37
TABLE 9: CORRELATIONS BETWEEN DEMOGRAPHIC CHARACTERISTICS OF THE RESPONDENTS ... 38
TABLE 10: KNOWLEDGE OF AMTSL ... 39
TABLE 11: CROSS TABULATION BETWEEN RESPONDENTS WHO KNOW AMTSL & PLACES OF TRAINING ON AMTSL ... 41
TABLE 12: YEAR OF AMTSL EXPERTISE ... 42
TABLE 15: CROSS TABULATION RESULTS BETWEEN USAGE OF AMTSL &HIGHEST EDUCATION LEVEL ... 43
TABLE 16: USAGE OF AMTSL ... 44
TABLE 19: ONE-SAMPLE TEST ... 47
TABLE 20: THREE MAIN SEQUENTIAL COMPONENTS OF AMTSL ... 48
TABLE 23: FACTOR ANALYSIS: ROTATED COMPONENT MATRIXA ... 52
TABLE 24 : TOTAL VARIANCE EXPLAINED ... 53
TABLE 25: REFERENCES ON GUIDES ON AMTSL PERFORMANCE ... 54
TABLE 26: BARRIERS FACED IN CORRECT AMTSL ADMINISTRATION... 55
TABLE 27: SUGGESTION ON AMTSL REINFORCEMENT ... 56
TABLE 28: AMTSL COMPONENTS ... 58
TABLE 29: RESIDUAL STATISTICS: REGRESSION ANALYSIS OF GUIDELINES, MOTIVATIONS AND VIEWS BEHIND AMSTL IMPLEMENTATION ... 59
TABLE 30: COEFFICIENTSA ... 60
TABLE 31: MODEL SUMMARY ... 61
LIST OF FIGURE
FIGURE 1: CONCEPTUAL FRAMEWORK ... 9
FIGURE 1: RESPONDENTS’ GENDER ... 31
FIGURE 2: PLACE OF TRAINING ON AMSTL ... 39
FIGURE 3: RECOMMENDED DOSE FOR SELECTED DRUG ... 45
FIGURE 5: FACTORS THAT PROMOTE AMTSL ADMINISTRATION ... 55
ABBREVIATION AND ACRONYMS AM TSL Active Management of Third Stage of Labor BEOC Basic Essential Obstetric Care
CCT Controlled Cord Traction
DIC Disseminated Intravascular Coagulation
FIGO International Federation of Gynecology and Obstetrics ICM International Confederation of Midwives
I.M Intramuscular
I.V Intravenous
KDHS Kenya Demographic Health Survey
KUERC Kenyatta University Ethical Review Committee KSPA Kenya Survey for Population Audit
MTRH Meru Teaching and Referral Hospital. MOH Ministry Of Health
MMR Maternal Mortality Rate
MDG Millennium Development Goals
MSPAS Ministry of Public Health and Social work
NCAPD National Coordinating Agency for Population and Development NACOSTI National Commission for Science and Technology Institute
PPH Postpartum Hemorrhage.
POPPHI Prevention of Postpartum Hemorrhage Initiative SPSS Statistical Package for Social Sciences
UNFPA United Nations Population Fund
UN United Nations
OPERATIONAL DEFINITIONS OF SIGNIFICANT TERMS
Practices: The way midwives working in selected health facilities of Meru County give care of third stage of labor as stipulated in the National obstetric guideline; specifically advising mothers on safe motherhood.
Knowledge: Midwives intellectual perception on third stage management of labor following delivery of a baby and the key components involved in management that is Uterotonic administration, controlled cord traction and uterine massage.
Active Management of the Third Stage of Labor (AMTSL): an evidence-based, low-cost intervention used to prevent postpartum hemorrhage that can help to prevent Primary PPH.
Postpartum hemorrhage: It is defined as excessive bleeding from the birth canal after the birth of the baby up to 6 weeks postpartum, amounting to 500ml or more or any amount that causes deterioration of the maternal condition.
Uterotonic drugs: are substances that stimulate uterine contractions or increase uterine tone.
Third stage of labor: this is a stage which commences with the completed delivery of the fetus and ends with the completed delivery of the placenta and its attached membranes.
Controlled cord traction: this involves traction on the cord, during a contraction, combined with counter-traction upward on the uterine body by a hand placed immediately above the symphysis pubis.
Uterine massage: an action used after the delivery of the placenta in which one hand is placed on top of the uterus to rub or knead the uterus until its firm.
ABSTRACT
CHAPTER ONE
INTRODUCTION
1.1 Background information
The number of women dying from causes related to pregnancy and childbirth globally is approximately 216/100000 live births which is a significant decline from 1990 though far below the target set by the united nations as part of its millennium development goals which aimed to see a drop of 75% by 2015 (WHO, 2015).
development and pursuing global partnerships. Postpartum hemorrhage (PPH) is one of the world's leading causes of maternal mortality (UN, 2010). It occurs in over 10% of all births and is associated with case fatality rate of 1%. PPH is generally defined as blood loss greater than or equal to 500 ml within 24 hours after birth, while severe condition is blood loss greater than or equal to 1000 ml within 24 hours. Most cases of morbidity and mortality due to PPH occur in the first 24 hours following delivery and these are regarded as primary whereas any abnormal or excessive bleeding from the birth canal occurring between 24 hours and 6 weeks postnatal is regarded as secondary PPH. It may result from failure of the uterus to contract adequately (atony), genital tract trauma (i.e. vaginal or cervical lacerations), uterine rupture, retained placental tissue, or maternal bleeding disorders. Uterine atony is the most common cause and consequently the leading cause of maternal mortality worldwide (ICM, 2003). Twenty five percent of all maternal deaths are caused by severe hemorrhage (WHO, 2005). According to Kenya demographic health survey (2009) report indicate that maternal mortality remains high in Kenya and the target was to reduce it to 147/100,000 live births by the year 2015. According to Health information system data, PPH accounts for about 33.9% of maternal deaths in Africa, Kenya being one of them.
pubis. CCT facilitates expulsion of the placenta once it has been separated from the uterine wall. The third component is the massage of the uterus after delivery of the placenta, which is an action used after the delivery of the placenta in which the provider or the woman places one hand on the fundus of the uterus through the woman's abdomen to rub or knead the uterus until it is firm (ICM/FIGO, 2003). This ICM/FIGO definition is also supported by the World Health Organization (WHO, 2006). The FIGO/ICM Joint Statement and the WHO report on the Managing Complications in Pregnancy and Childbirth do not include immediate cord clumping (WHO, 2000). Studies show that there is considerable evidence that early cord clamping does not benefit mothers or babies and may even be harmful (Niermeyer, et al., 2006).The Current policy environment in Kenya is very supportive of AMTSL implementation and the use of uterotonics in AMSTL to prevent PPH is highly advocated (MOH, 2008). Therefore the main purpose of this study was to assess the current level of knowledge and competency of midwives in preventing primary PPH through AMTSL in selected health facilities of Meru County.
1.2 Statement of Research Problem
Data obtained from delivery register of Meru teaching and referral hospital (2014), showed that some women suffer from complications related to child birth and most frequently during third stage of labor. From the data obtained in six months i.e. June to December 2014, it reviewed that cases of postpartum hemorrhage are still a threat in safe mother hood practices. Out of an average of 420 mothers delivered each month through spontaneous vaginal delivery, an average of fourteen cases of PPH are reported. In reference to retrospective data, some months recorded as many as 13 cases of PPH for example in the month of June. An average of 5 maternal deaths is reported per month, of which most are secondary to postpartum hemorrhage.
Little is known on the current situation in the implementation of all the components of AMTSL in Kenya which leaves a critical gap in the continuum of care needed for safe motherhood and the achievement of MDGs 5 which was a target by 2015. This was evidenced by the number of deaths reported in one selected health facility of Meru County despite continuous education to both in-service and pre-service midwives during their training.
1.3 Justification of the Study
due to PPH were 488/100000 live births contrary to WHO recommendation on safe motherhood initiative.
Despite progressive training of midwives on active management of third stage of labor, there is limited study evaluation that has been done in Meru County to determine its effectiveness. The researcher will therefore be interested in determining midwives knowledge and competency in implementation of active management of third stage of labor. The World Health Organization (WHO) recommends that in making pregnancy safer, technical updates on prevention of PPH by AMTSL should be practiced by all skilled attendants at every birth to prevent postpartum hemorrhage and to achieve MDG 5 which targeted reducing of maternal death by 147/100000 live births.
1.4 Research Questions
i. What is the influence of midwife demographic characteristics in the outcome of active management of third stage of labor in selected health facilities of Meru County?
ii. What is the level of knowledge of midwives on active management of third stage of labor in selected health facilities of Meru County?
iii. What is the competency of midwives in active management of third stage of labor in selected health facilities of Meru County?
1.5 Hypothesis
1.6Broad Objective
To assess the current level of knowledge and competency of midwives in implementation of active management of third stage of labor in selected health facilities of Meru County.
1.6.1 Specific Objectives
To establish the influence of midwife demographic characteristics in the outcomes of active management of third stage of labor in selected health facilities of Meru County.
To determine the level of knowledge of midwives on active management of third stage of labor in selected health facilities of Meru County.
To assess the competency of midwives in active management of third stage of labor in selected health facilities of Meru county
1.7 Significance of the Study
focusing on similar area of study as well as creation of awareness to the midwives. This study aimed at providing the midwives working within the Meru County and beyond with the descriptive information necessary to assess AMTSL practices and to identify major gaps to its use in order to reduce obstetric emergencies due to PPH which is the main cause of maternal death and also help to achieve MDG 5 which was a target by 2015.
1.8 Delimitation
This study was restricted to Meru County and the data was generated from maternity labor ward specifically from trained and skilled birth attendants. The study also
involved only mothers with spontaneous virginal delivery and not those done caesarian section
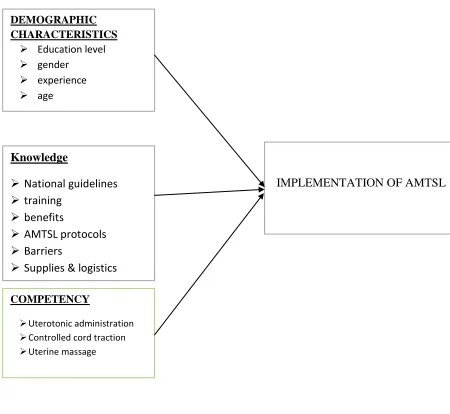
1.8 CONCEPTUAL FRAME WORK Demographic characteristics
The knowledge and skills required to perform AMTSL are essential for routine use of the practice in the health set up by the midwives. Provider education, age, experience, and gender are also important aspects to effective management of third stage of labor.
Knowledge
knowledge and practices on storage of uterotonic drugs through refresher courses. Adding column to labor and delivery log books in monitoring the use of active management of third stage of labor and implementing clinical audits is considered a major factor in focused management of third stage of labor.
AMTSL components
INDEPENDENT VARIABLES DEPENDENT VARIABLES
Figure 1: Conceptual Framework
IMPLEMENTATION OF AMTSL DEMOGRAPHIC
CHARACTERISTICS Education level gender
experience
age
Knowledge
National guidelines
training
benefits
AMTSL protocols
Barriers
Supplies & logistics
COMPETENCY
Uterotonic administration
Controlled cord traction
CHAPTER TWO
LITERATURE REVIEW
2.1 Introduction
According to the World Health Organization (WHO Recommendations for the Prevention of Postpartum Hemorrhage: WHO Document Production Services, Geneva (2007), postpartum hemorrhage is considered to be the cause of a quarter of maternal morbidity and mortality rates worldwide. In an attempt to reduce the risk of hemorrhage, a group of interventions have been introduced into clinical practice that constitute active management conducted during the third stage of labor and are recommended by the international organizations (Haris T, 2012). Hemorrhage is the main cause of maternal death in a number of countries. It has been estimated that at least 25% of these deaths are due to hemorrhage - the majority due to postpartum hemorrhage (WHO 2014).
2.1.0. Scientific evidence supporting active management of third stage of
labor (AMTSL)
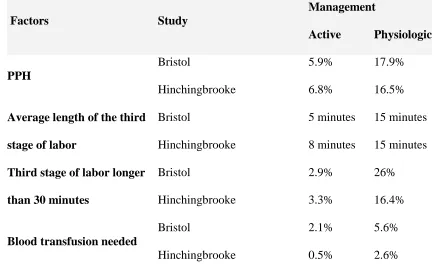
Table 1a: Bristol, (2002) and Hinchingbrooke, (1998) Study results comparing active and physiologic management of the third stage of labor
Factors Study
Management
Active Physiologic
PPH
Bristol 5.9% 17.9%
Hinchingbrooke 6.8% 16.5%
Average length of the third stage of labor
Bristol 5 minutes 15 minutes
Hinchingbrooke 8 minutes 15 minutes Third stage of labor longer
than 30 minutes
Bristol 2.9% 26%
Hinchingbrooke 3.3% 16.4%
Blood transfusion needed
Bristol 2.1% 5.6%
Hinchingbrooke 0.5% 2.6%
Active management of the third stage of labor (AMTSL) is an evidence-based, low-cost intervention used in prevention of postpartum hemorrhage (PPH). Bristol et al, (2002) and Hinchinbrook et al., (1998) randomized control trials provide conclusive evidence that active management of the third stage of labor (AMTSL) significantly reduces postpartum hemorrhage, decreases blood loss and decreases the need for blood transfusions (Cotter et al, 2001).
its use. In this study focus, the data will be drawn from specific and elaborate sample population and more so, from the midwives working in labor ward in order to gather firsthand account on active management of third stage of labor (AMSTL).
2.1.1 Practice
The third stage of labor is defined as the period between delivery of the infant and delivery of the placenta. The major complication associated with this stage is postpartum hemorrhage, defined as vaginal bleeding of more than 500 ml in the first 24 hours after delivery (Prendivilleet al 2012). The most common cause of immediate severe postpartum hemorrhage is uterine atony. Retained placenta, vaginal or cervical lacerations, and uterine rupture or inversion can also contribute to the complications (J Midwifery Women’s Health, 2010). Postpartum hemorrhage remains the most common cause of maternal mortality worldwide, accounting for one-fourth of the maternal deaths (WHO, 2006).
insufficient evidence for drawing conclusions about the effectiveness of this practice in its altered states. These results do suggest, however, that the use of active management of third stage of labor (AMTSL) is quite low and, where it is practiced, the definition varies within and between countries with most of developing countries practicing expectant management (Sleep J, 2013). Kenya being a developing country, a similar case scenario can be drawn from the above in those cases of widely spread use of expectant management.
clamping the cord (performed in 93% of cases), and the least common was delayed cord clamping of two minutes or more (performed in 51% of cases). Most women (76%) received assistance with initiating breastfeeding within the first hour after delivery. Overall, 65% of women received the five elements of immediate newborn care: delayed cord clamping, placing the newborn skin-to skin with the mother, drying and wrapping the baby, cutting and tying the cord, and helping the mother initiate breastfeeding. During an active third stage of labor, the midwife needs to continually observe the woman, monitoring her blood loss visually and how she feels and behaves (assessing for signs and/or symptoms of excessive blood loss), to ensure that the wellbeing of the woman and her baby is not compromised. The midwife also needs to ensure that the woman has an empty bladder since full bladder can prevent the uterus from contracting effectively (WHO, 2012)
The time the placenta is birthed should be documented by the midwife in the woman’s labor notes. NICE (2007) recommends that the placenta should be birthed within 30 minutes in active management of the third stage of labor.
2.2.1.0 Provider- related factors to quality obstetric care.
A study conducted in Tanzania by Nyamtema et al (2008) to assess staffing needs for quality perinatal care revealed that, the most reported incentives included paying overtime, timely promotion, salary Increments, in-service training, seminars, workshop and provision of mid-morning tea for staff.
2.2.1.1 Supplies and logistics
The sufficient availability of high- quality uterotonic drugs, needles, and syringes at national and local levels is essential for routine use of active management of third stage of labor (AMTSL). Effective use of active management of third stage of labor (AMTSL) also implies appropriate conditions during transport and storage to ensure the use of chemically-active drugs and safe, sterile needle and syringes (Dupont C, et al 2014).
According to a research conducted in Guatemala, various challenges and practices were highlighted, the study documented practices during the third and fourth stages of labor in a representative sample of public health facilities from six of the eight regions of Guatemala. The seven percent of the observed deliveries complied with the strict definition, and 12 percent complied with the more relaxed definition of active management of third stage of labor (AMTSL) use. This means that between 88 and 93 percent of the women delivering vaginally in national public health network facilities did not receive adequate prevention of postpartum hemorrhage.
2.3 Challenges affecting midwives competency in implementation of AMTSL
the third stage of labor, a uterotonic drug (oxytocin or misoprostol) should be offered by a health worker trained in its use for prevention of PPH (WHO, 2006).
Evidence regarding adoption of this practice, however, is limited. Evaluations of donor funded projects incorporating AMTSL tend to be limited to reporting on the numbers of providers trained and the percent achieving competence following training. Apart from a 2003 article by the Global Network for Perinatal and Reproductive Health which offers limited information into the adoption of this practice (WHO, 2005). Their results targeted on an evaluation of the15 university-based referral obstetric centers in low and high income countries. The results however showed substantial variation between and within hospitals. The proportions of the service providers using AMTSL being quite low and, where it is practiced, the definition varies within and between countries.
A cross sectional survey done by (Festin et al 2003) to investigate the variation on use of AMTSL detected a significant intra county and inter county variation on active management of third stage of labor and confirmed a big gap between knowledge and practice and recommended evidence based clinical management defined by FIGO/ICM joint statement. Due to lack of consistency and conflicting ideas on active management of third stage of labor practice, a survey carried in low income countries found Egyptian teaching and referral hospitals with only 15% of observed deliveries conducted using correct practice (cherine et al, 2004). Among these low income countries, except Indonesia which did not have conflicting policies (Stanton et al, 2009)
contraceptives, shortage of personnel and lack of key equipment which are necessary in care of patients particularly those with unsafe induced abortion and although one of the priorities of the Kenyan National Reproductive Health Strategy is to extend the coverage of post abortion care, so far such services remain scarce (NCAPD and ORC Macro, 2010).
2.3.0 Knowledge as a factor in AMTSL
Khan et al (2006) in their study recommended that training of midwives on the update of standard treatment guidelines was key in complying with ICM/FIGO recommendation practices on storage of uterotonic drugs through refresher courses, adding column to labor and delivery log books to monitor the use of active management of third stage of labor and implementing clinical audits focused on AMTSL. Knowledge on AMTSL is a main component in complying with guidelines during service delivery. Regrettably, researches conducted on knowledge of mid-wives on AMTSL indicate that majority have limited knowledge. In a survey conducted by NCAPD et al., (2010), on Kenya Service provision, knowledge of mid-wives in prevention of post partum was inadequate. The survey reported that the proportions of delivery care providers who correctly mentioned the items for monitoring of labor and delivery was 3% .Only 7% correctly mentioned items to assess in a woman who presents with bleeding after delivery.
2.3.1Training of Staff in regard to care delivery.
mistreatment of women in public health facilities in Kenya is reportedly rife (NCAPD, et al., 2010) and majority of health care workers prefer short cuts which also impose negatively to those under training. Unfortunately very important information to include counseling and other ANC profile consultations are left unattended leading to un preferred outcomes during third stage of labor. Many if not most service providers, also lack more advanced skill, for example recognizing and treating life threatening complications. Efstathiou (2011) articulated training as a major component in realization of improved standards towards effective management of third stage of labor. Studies show that lack of knowledge is a contributing factor to low utilization of standard documents. The integration of curriculum during midwifery training plays a vital role in understanding the standard document and its implementation (Nyakanda 2012).
2.3.2 Competency and work experience
CHAPTER THREE RESEARCH METHODOLOGY 3.1 Study Design
The study adopted a descriptive cross-sectional study design. A cross-sectional survey is the research design that collects information from a sample that has been drawn from a predetermined population (Fraenkel and Wallen, 2000). It was a descriptive survey as the researcher intended to collect the data and describe it in relation to the midwives knowledge and competency on active management of third stage of labor within Meru County. The research design bore both qualitative and quantitative design because in qualitative the researcher was able to establish the cause and effects of postpartum hemorrhage in management of third stage of labor. Qualitatively the researcher was able to seek description and analysis of the practice and the demographic characteristic of midwives towards work. Quantitatively the researcher was able to verify the data established qualitatively by proving, confirming and substantiating the components in active management of third stage of labor. It was also important in statistical work when quantifying the target group awareness on the area of study.
3.2 Variables
3.2.1 Independent variables
The last component was competency based on uterotonic administration, controlled cord traction and uterine massage.
3.2.2 Dependent variable
Implementation of active management of third stage of labor (AMTSL) was the dependent variable and this was determined using the standard guidelines of the three principles which include timely oxytocin administration, controlled cord traction and proper uterine massage.
3.2.3 Study Area
3.3 Study Population
Frankel and Wallen (2000) describe a population as the group of interest to the researcher. It is the group of whom the researcher liked to generalize the results of the study. The target population of this study included 375 nurse midwives working in maternity department in various units to include labor ward, post natal ward, neonatal ward and antenatal ward in selected health facilities. Among the selected maternity facilities, a sample population of 125 midwives participated in the study as they were directly offering AMTSL services.
3.3.0 Inclusion criteria
Midwives working at the labor ward in the selected health facilities who were directly involved in conducting of the deliveries
3.3.1 Exclusion criteria
Midwives not working at the labor ward in the selected health facilities and are not involved in conducting of the deliveries.
3.4 Sampling Technique
Name of the hospital Population 30% of target population Sample Size
1.Meru level five hospital 150 50
2.Kanyakine level 4 hospital 75 25
3.Gatimbi sub county hospital 60 20
4.Nkubu mission hospital 90 30
TOTAL 375 125
3.5 Sample Size and Determination
Sample size was determined using the formula as designed by fisher et al (1998)
𝑛 = 𝑍2𝑃(1 − 𝑃)
𝑑2
n- Desired sample size
Z- Is the corresponding confidence level (i.e. 1.96 for 95% confidence interval?)
d- Is the margin of error (i.e. 0.05 = ± 5% )
p-is the estimated value for the proportion of a sample that has the condition of interest.
𝑛 = 1. 962(0.43)𝑥(0.57)
0.052
𝑛 = 188
Finite population correction for population less than 10,000.
Since the sample population was 375 midwives working in selected health facilities of Meru County, the researcher used Yamane formula (1967 to calculate the sample size.
𝑛𝑓 = 𝑛
1 + 𝑛/𝑁
Where
nf=desired sample size
n= calculated sample size
N=estimate of population in study area
𝑛𝑓 = 188
1 + 188/375
nf=125
Thus a sample of 125 respondents was required.
3.5.1 Pre testing
The tools for pre testing were designed well to ensure validity and reliability during the exercise and adjusted accordingly.
3.6 Validity and Reliability of Research
Validity is the ability of the tool to measure what is supposed to be measured while reliability is internal consistency or dependability with which an instrument measures the attribute or variable to establish if participants in the study are able to understand the instructions and respond correctly. It assesses the results of a certain measure, whether it yields the same result in other circumstances or whether other observers (Saunders et al, 2007) achieve similar results.
A pilot study was conducted to determine sample power without varying research instruments to ensure validity (Osborn et al, 2009).A test retest was done to the same respondents using same questionnaires and checklist and adjusted accordingly. Research assistants were qualified midwives trained on AMTSL. The assistants were trained on how to use the questionnaires and observational checklist to ensure consistency.
3.7 Data Collection Technique
3.8 Primary Data
The researcher used questionnaire which had various parts (demographic characteristics, AMTSL knowledge, and competencies) containing both open (unstructured) and closed ended (structured) questions to interview the research participants. This method of obtaining data was the most appropriate to the researcher since all midwives could read and comprehend.
3.9 Data Collection Instruments
Data was collected by use of self-administered questionnaire and observation checklist as the main tool for data collection. The questionnaires were administered to the respondents and all clarification done in areas of concern on the questions. The tool was structured alongside the three main objectives of the study and had four parts. Part one focused on the demographic data of the respondents, part two on midwives characteristics, three on knowledge and four on midwives competency. Research assistants were trained prior to the exercise on how to administer the questionnaires to the respondents. The researcher supervised the assistants and cross checked the exercise regularly to ascertain competence and commitment to obtaining unbiased data.
3.10 Data Cleaning and Storage
Both descriptive and inferential statistics were used to analyze the data in this study. Both measures of central tendency (means and median) and measures of dispersion (variances, percentiles, range) were utilized in the analysis based on the nature of data collected. Chi-square test was used to test association of different variables.
3.11 Ethical Considerations
CHAPTER FOUR: RESULTS 4.1 Introduction
This chapter presents the results on the findings of data collected following analysis and interpretation of the raw data. The findings are presented according to the objective of the study and the questionnaire. The data presented covered the influence of midwife demographic characteristics in the outcomes of active management of third stage of labor, the level of knowledge of midwives on active management of third stage of labor and the competency of midwives in active management of third stage of labor.
The chapter also presents analysis and findings of the study as set out in the research methodology. The study findings presented showed the current level of knowledge and competency of midwives in implementation of active management of third stage of labor in selected health facilities of Meru County. The data was gathered exclusively from the semi-structured questionnaires, interview schedules and observation checklists as the research instruments. These instruments were designed in line with the objectives of the study. The results here were presented in data tables, figures and discussions.
4.2. Response Rate
4.3 Demographic Information
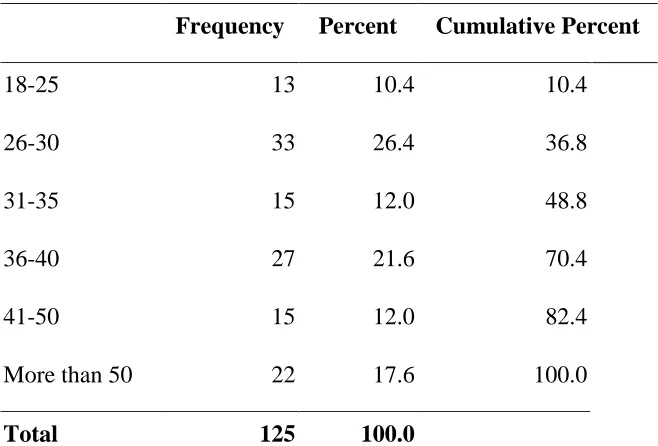
The researcher wanted to find out the demographic information of the respondents. The demographic information included the respondents’ ages, gender, highest education levels, highest midwifery education and their job profiles. As presented in the table 1 below, majority 33(26.4%) of the respondents fell into the ages of 26-30 years. In addition 27(21.6%) of the respondents fell into the age bracket of 36-40 years, 22(17.6%) of the respondents were more than 50 years. The same proportion 15(12.0%) of the respondents fell in the ages of 31-35 years and 41-50 years. The minority 13(10.4%) of the respondents were between 18-25 years old. The results show that the respondents are in their youth stage. According to government of Kenya on definition of the term youth; it refers to a person who is between 18 years to 45 years (Government of Kenya, 2014).
Table 1.0 Respondents’ Age
Frequency Percent Cumulative Percent
18-25 13 10.4 10.4
26-30 33 26.4 36.8
31-35 15 12.0 48.8
36-40 27 21.6 70.4
41-50 15 12.0 82.4
More than 50 22 17.6 100.0
Total 125 100.0
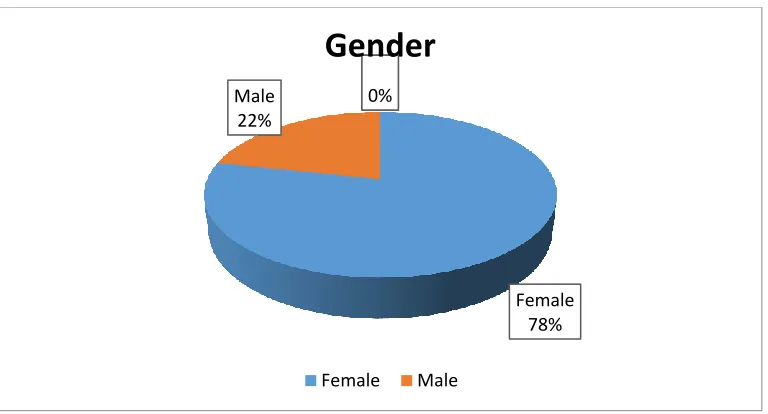
while the minority 27(21.6%) of the respondents were male. The findings indicated that most of the respondents involved in the study were females compared to males.
Figure 1: Respondents’ gender
In the table 2 below, the researcher wanted to find out the highest level of education of the respondents. Majority 72(57.6%) of the respondents had college as their highest level of education while 19(15.2%) of the respondents had university as their highest level of education. Moreover, 19(15.2%) of the respondents had certificate level while 15(12%) had advanced diplomas their highest education level. These findings showed that diploma was the highest level of education attained by the respondents compared to other levels.
Female 78% Male
22%
0% 0%
Gender
Table 2. Highest Education Level
Frequency Percent Cumulative Percent
Certificate 19 15.2 15.2
Diploma 72 57.6 72.8
Advanced diploma 15 12 84.8
University 19 15.2 100.0
Total 125 100.0
The level of knowledge of the midwives on active management of the third stage of labor is important in reducing cases of postpartum bleeding. As a result therefore, the researcher wanted to find out the highest midwifery education the respondents had. As presented in table 3 below, majority 72(57.6%) of the respondents had diploma, 19(15.2%) had a degree, 19(15.2%) of the respondents were certificate holders while the minority 15(12.0%) had advanced diplomas as their highest midwifery qualification. The findings show that the respondents are learned and they have gone to school. Table 3.Highest Midwifery Education
Frequency Percent Cumulative %
Certificate 19 15.2 15.2
Diploma 72 57.6 72.8
Advanced Diploma 15 12.0 84.8
Table 4. Cross tabulation between Highest Education Level & Recommended dose for selected Drug
Count
Recommended dose for selected Drug
Total
5 IU 10 IU 2.5 IU
Highest Education Level:
Certificate
11 8 0 19
Advanced diploma
3 12 0 15
diploma 15 55 2 72
University 1 18 0 19
Total 30 93 2 125
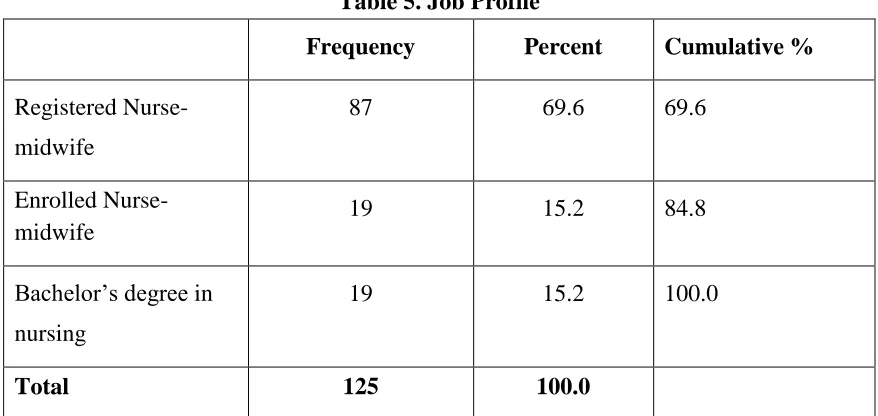
Table 5. Job Profile
Frequency Percent Cumulative % Registered
Nurse-midwife
87 69.6 69.6
Enrolled Nurse-midwife
19 15.2 84.8
Bachelor’s degree in nursing
19 15.2 100.0
Total 125 100.0
The study aimed at finding out the duration of practice of the respondents. As tabulated in the table 6 below, majority 39(31.2%) of the respondents had practiced for between 7-10 years, 30(24.0%) of the respondents had practiced for 3-6 years, 29(23.2%) of the respondents had practiced for more than 15 years, 15(12.0%) of the respondents had practiced for 11-15 years while the minority 12(9.6%) had practiced for up to two years. Table 6. Duration of Midwifery Practice
Frequency Percent Cumulative Percent
0-2 12 9.6 9.6
3-6 30 24.0 33.6
7-10 39 31.2 64.8
11-15 15 12.0 76.8
More than 15 29 23.2 100.0
Total 125 100.0
In review of the age experience, some midwives (37) gave under dose of 5I.U and the minority (4) said 2.5 I.U as the right dosage. In reference to experience, the study found out that the number of years served did not ultimately reflect the competency level of the respondents since errors in dosages were captured in all age experience specifications.
Table 7. Year of AMTSL experience &recommended dose for selected Drug
Count
Recommended dose for selected Drug
Total 5 IU 10 IU 2.5 IU
Year of AMTSL experience 10yrs& above 2 3 0 5
9yrs 0 4 4 8
8yrs 5 21 0 26
7yrs 6 15 0 21
6yrs 16 19 0 35
1-5yrs yr 8 22 0 30
Total 37 84 4 125
that the minority number of midwives (16) had less experience of between 0-2 years while 12 midwives had 15 and above years of experience in all categories.
Table 8 Cross tabulation results between Highest Education Level & Duration of Midwifery Practice
Count
Duration of Midwifery Practice
Total No of years served by
the respondents: 0-2 3-6 7-10 11-15
More than 15 Highest Education
Level
certificate 0 2 12 5 0 19
Advanced
diploma 0 7 4 4 0 15
Diploma 14 13 16 17 12 72
University 2 5 8 4 0 19
Total 16 27 40 30 12 125
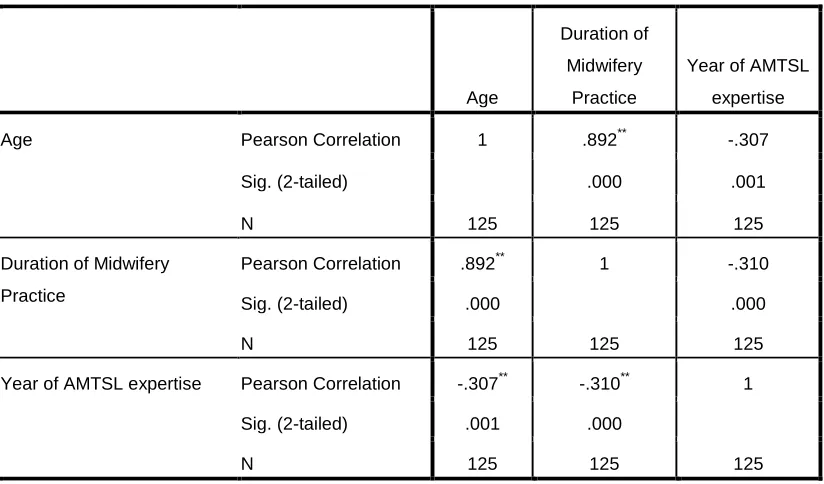
Table 9 Correlations between Demographic Characteristics of the Respondents
Age
Duration of
Midwifery
Practice
Year of AMTSL
expertise
Age Pearson Correlation 1 .892** -.307
Sig. (2-tailed) .000 .001
N 125 125 125
Duration of Midwifery
Practice
Pearson Correlation .892** 1 -.310
Sig. (2-tailed) .000 .000
N 125 125 125
Year of AMTSL expertise Pearson Correlation -.307** -.310** 1
Sig. (2-tailed) .001 .000
N 125 125 125
**. Correlation is significant at the 0.01 level (2-tailed).
4.4 knowledge of the Respondents
The researcher wanted to know the level of knowledge and competency of midwives in implementation of active management of third stage of labor. An item was included in the questionnaire and it was measured by indicators such as Knowledge of AMTSL, place of training on AMTSL, year of experience and the usage of AMTSL.
Table 10. Knowledge of AMTSL
Frequency Percent Cumulative %
Yes 125 100.0 100.0
4.4.1 Training Information on AMTSL
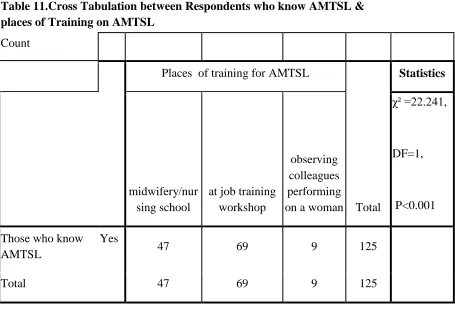
In the figure 2 below, the researcher wanted to find out the place of training on AMTSL standards. Majority 69(55.2%) of the respondents stated that they received training at job training workshop. 47(37.6%) of the respondents had received their training at the midwifery/nursing school. The minority 9(7.2%) of the respondents received their training by observing when being performed. The findings demonstrated therefore that majority had received training at job training workshop as compared to nursing school and work environment.
Figure 2: place of training on AMSTL
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00%
At midwifery/nursing
school
At job training workshop
Observing when performed
Table 11.Cross Tabulation between Respondents who know AMTSL & places of Training on AMTSL
Count
Places of training for AMTSL
Total
Statistics
midwifery/nur sing school
at job training workshop
observing colleagues performing on a woman
χ² =22.241,
DF=1,
P<0.001 Those who know
AMTSL
Yes
47 69 9 125
Total 47 69 9 125
Table 12. Year of AMTSL Expertise
Frequency Percent Cumulative Percent
2007 5 4.0 4.0
2008 8 6.4 10.4
2009 26 20.8 31.2
2010 21 16.8 48.0
2011 35 28.0 76.0
other years 30 24.0 100.0
Total 125 100.0
Table 13.The Association between Knowledge and Utilization of AMTSL
Frequency Percent Valid Percent Statistics
Yes 122 97.6 97.6
No 3 2.4 2.4
χ² =113.29, DF=1, P<0.001
Total 125 100.0 100.0
Table 14 shows association between usage of AMSTL and level of education. Majority 122 (97.6%) of the respondents from all levels of education said they use AMSTL while a small section of the respondents 3(2.4%) did not use the procedure.
Table 15 Cross tabulation results between Usage of AMTSL &Highest Education Level
Count
Highest Education Level
Total certificate
Advanced
diploma diploma University Usage of
AMTSL
Yes
19 15 69 19 122(97.6
%)
No 0 0 3 0 3(2.4%)
Total
4.6 knowledge on AMSTL by Midwives in Active Management of Third Stage of Labor
The researcher wanted to find out the competence in terms of knowledge of the midwives regarding the AMTSL standards and their utilization in practice. As tabulated in table 16 below, majority 122(97.6%) of the respondents use the AMTS specifications while the minority 3(2.4%) of the respondents did not use them.
Table 16 Usage of AMTSL
Frequency Percent Cumulative Percent
Yes 122 97.6 97.6
No 3 2.4 100.0
Total 125 100.0
Table 17.First line of Uterotonic Drug Recommended in AMTSL
Frequency Percent
IV Ergometrine (0.5 mg) 4 3.2
IM Oxytocin (10 IU) 121 96.8
Total 125 100.0
The study also intended to find out the recommended dose of the Uterotonic drug that the respondents administered during management of third stage of labor. As tabulated in figure 3 below, majority 84(67.2%) of the respondents administered 10 IU, 37(29.6%) of the respondents administered 5 IU while the minority 4(3.2%) administered 2.5 IU.
Moreover, the researcher wanted to find out the route through which the uterotonic drugs were administered. As tabulated in the table 18 below, majority 121(96.8%) of the respondents administered through intramuscular (IM) injection while a very small proportion of the respondents administered through the intravenous (IV) and oral administration. The study established that intramuscular (IM) injection was best preferred compared to intravenous (IV) and oral administration.
Table 18. Recommended Route for Uterotonic Drug
Frequency Percent Cumulative Percent
Oral 2 1.6 1.6
Intramuscular (IM) 121 96.8 98.4
Intravenous (IV) 2 1.6 100.0
Total 125 100.0
4.7 Association between Recommended Route for Uterotonic Drug and the most recommended dose
Table 19. One-Sample Test
Test Value = 0
T Df
Sig. (2-tailed) Mean Difference 95% Confidence Interval of the Difference Lower Upper Recommended
dose for selected
Drug 38.036 124 .000 1.736 1.65 1.83
χ²:77.58, df; 2, sig. 0.001 Recommended Route for Uterotonic Drug
124.499 124 .000 2.000 1.97 2.03
χ²:226.57, df; 2, sig. 0.001
Table 20. Three main Sequential Components of AMTSL
Frequency Percent Cumulative % Oxytocin administration, immediate uterine
massage after delivery of placenta and CCT 31 24.8 24.8
Immediate uterine massage after delivery of
placenta, CCT and Oxytocin Administration 7 5.6 30.4
Oxytocin Administration, CCT and
immediate uterine massage after delivery of placenta
87 69.6 100.0
Total 125 100.0
Table 21. Harmful Practices during AMTSL Performance
Frequency Percent
Cumulative Percent Massaging Uterus before Delivery of the
Placentas 25 20.0 20.0
Applying Controlled Cord Traction
(CCT) without Fundal Support 44 35.2 55.2
Both 56 44.8 100.0
Total 125 100.0
According to the data presented in the table 22 below, majority 67(53.6%) of the respondents gave the duration of AMTSL completion as between 5-10 minutes, 34(27.2%) of the respondents gave almost 5 minutes, 23(18.4%) gave duration as almost 3 minutes while the minority 1(0.8%) of the respondents (others) were not sure. Table 22. Duration of AMTSL Completion
Frequency Percent Cumulative Percent
almost 3 minutes 23 18.4 18.4
almost 5 minutes 34 27.2 45.6
between 5-10 minutes 67 53.6 99.2
Others 1 .8 100.0
In the data presented in figure 4 below, the researcher wanted to find out from the respondents the interval of uterine massage within the first 2 hours post-delivery. Majority 89(71.2%) of the respondents gave 15 minutes as time interval, 34(27.2%) of the respondents gave 30 minutes while the minority 2(1.6%) gave 45 minutes as time interval. These results showed that a significant number (28.8%) of the respondents didn’t have the knowledge about the uterine massage interval.
Table 23 Factor Analysis: Rotated Component Matrixa
Component
1 2 3
First line of Uterotonic Drug Recommended
for AMTSL .632 .075 -.197
Recommended dose for selected Drug .683 .093 -.125 Recommended Route for Uterotonic Drug -.048 .092 .898 Three main Sequential Components of
AMTSL .629 .538 .160
Harmful Practices During AMTSL
Performance .718 .153 .421
Duration of AMTSL Completion .027 .941 .049
Interval of Uterine Massage First 2 Hours
Post Delivery -.723 .174 -.388
Extraction Method: Principal Component Analysis.
Rotation Method: Varimax with Kaiser Normalization.
Table 24 . Total Variance Explained
Compone nt
Initial Eigen values Rotation Sums of Squared Loadings
Total
% of Variance
Cumulative
% Total
% of Variance
Cumulative %
1 2.627 37.532 37.532 2.302 32.886 32.886
2 1.095 15.649 53.181 1.251 17.879 50.765
3 1.048 14.964 68.145 1.217 17.380 68.145
4 .756 10.804 78.949
5 .679 9.696 88.645
6 .470 6.708 95.353
7 .325 4.647 100.000
Extraction Method: Principal Component Analysis.
The factor analysis shows that the first three components are the important (2.627, 1.095 and 1.048) compared to 4, 5, 6 and 7. Extraction Method used is Principal Component Analysis.
4.70 Guidelines, Motivations and Views behind AMSTL Implementation
Midwifery text book by Margaret Mayors while 6(4.8%) of the respondents used WHO guidelines. Moreover, 20(16.0%) of the respondents had no reference to use.
Table 25. References on Guides on AMTSL Performance
Frequency Percent Cumulative %
AMTSL Wall Charts 58 46.4 46.4
Ministry of Health Guide Book 11 8.8 55.2
Midwifery Text Books by Margaret
Mayor 7 5.6 60.8
WHO Guidelines 6 4.8 65.6
Procedure Manual 23 18.4 84.0
None 20 16.0 100.0
Total 125 100.0
Figure 5. Factors that Promote AMTSL Administration
The researcher wanted to find out barriers faced by the respondents on following the AMTSL standards. As tabulated in the table 26 below, majority 51(40.8%) of the respondents stated that understaffing was a problem, 27(21.6%) stated that there was no sufficient training, 26(20.8%) of the respondents said that shortage of drugs was a barrier while the minority 21(16.8%) of the respondents faced no barrier.
Table 26. Barriers Faced in Correct AMTSL Administration
Frequency Percent Cumulative %
Understaffing 51 40.8 40.8
No Sufficient Training 27 21.6 62.4
Shortage of Drugs 26 20.8 83.2
No barrier 21 16.8 100.0
Total 125 100.0
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00% 90.00% 100.00%
To avoid PPH No Idea
The data presented in the table 27 below showed that the majority 76(60.8%) of the respondents suggested that more training was required so as to reinforce the use of AMTSL standards. In addition, 46(36.8%) of the respondents suggested enough staffing while the minority 3(2.4%) of the respondents had no suggestions on the ways of reinforcing the use of AMTSL standards.
Table 27. Suggestion on AMTSL Reinforcement
Frequency Percent Cumulative %
Enough Staffing 46 36.8 36.8
More Training 76 60.8 97.6
No Suggestion 3 2.4 100.0
Total 125 100.0
Figure 6. Effects of Gender on AMTSL Implementation
In the table 28 below, the principal investigator wanted to find out whether the various components of the AMTSL standards were being done during their practice. Majority 63(50.4%) of the respondents agreed that correct oxytocin administration within one minute post-delivery was done while the minority 62(49.6%) of the respondents accepted that correct oxytocin administration within one minute post-delivery was not done. Moreover, majority 102(81.6%) of the respondents agreed that delivery of placenta by CCT method was done while the minority 23(18.4%) of the respondents said that delivery of placenta by CCT method was not done.
In addition, the researcher wanted to find out whether immediate massage of the uterus was done by the attendants. Majority 79(63.2%) of the respondents agreed that immediate massage of the uterus was done by the attendants while the minority 46(36.8%) of the respondents stated that immediate massage of the uterus was not done
No 94% Yes
6%
Effects of Gender on AMTSL Implementation
by the attendants. Furthermore, the researcher wanted to find out if quarter hourly massage of the uterus within 2 hours was done. Majority 76(60.8%) of the respondents agreed that quarter hourly massage of the uterus within 2 hours was not done while the minority 49(39.2%) of the respondents agreed that quarter hourly massage of the uterus within 2 hours was done.
Table 28. AMTSL Components
Frequency Percent
Cumulative Percent
Correct Oxytocin Administration Within One minute Post delivery
Done 63 50.4 50.4
Not Done
62 49.6 100.0
Midwives Delivery of Placenta by CCT Method
Done 102 81.6 81.6
Not Done
23 18.4 100.0
Immediate Massage of the Uterus by birth Attendant
Done 79 63.2 63.2
Not Done
46 36.8 100.0
Quarter Hourly Massage of the Uterus within First 2 hours
Done 49 39.2 63.2
Not Done
76 60.8 100.0
Table 29. Residuals Statistics: Regression analysis of Guidelines, Motivations and Views behind AMSTL Implementation
Minimum Maximum Mean
Std.
Deviation N
Predicted Value .91 7.19 2.88 1.288 125
Residual -2.277 3.533 .000 1.590 125
Std. Predicted
Value -1.532 3.344 .000 1.000 125
Std. Residual -1.385 2.149 .000 .967 125
Table 30. Coefficientsa Model Unstandardized Coefficients Standardized Coefficients
t Sig.
95% Confidence Interval
for B
B Std. Error Beta
Lower
Bound Upper Bound
1 (Constant) 2.816 1.260 2.235 .027 .321 5.312
Factors that Promote
AMTSL Administration 1.864 .536 .314 3.481 .001 .804 2.925
Barriers Faced in Correct
AMTSL Administration -.305 .186 -.169 -1.638 .104 -.674 .064
Suggestion on AMTSL
Reinforcement 1.428 .383 .421 3.732 .000 .670 2.185
Effects of Gender on
AMTSL Implementation -1.605 .703 -.181 -2.282 .024 -2.999 -.212
Correct Oxytocin
Administration Within
One minute Post delivery
-.472 .350 -.116 -1.346 .181 -1.166 .222
Midwives Delivery of
Placenta by CCT Method -.150 .422 -.029 -.356 .723 -.987 .686
Immediate Massage of
the Uterus by birth
Attendant
-.340 .365 -.080 -.932 .353 -1.062 .382
Quarter Hourly Massage
of the Uterus within First
2 hours
-.470 .368 -.113 -1.280 .203 -1.199 .258
Table31. From regression analysis, Standardized Coefficients values shows that Factors that Promote AMTSL Administration (Standardized beta = 314 t=3.481 significance .001), Suggestion on AMTSL Reinforcement (Standardized beta =.421, t=3.732 and sig .000) and Effects of Gender on AMTSL Implementation (Standardized beta -.181 t= -2.282 and sig .024) are the only indicators showing strong association and showing some significance.
Table 31. Model Summary
Mod
el R
R Square Adjusted R Square Std. Error of the Estimate Change Statistics Durbin-Watson R Square Change F
Change df1 df2
Sig. F Change
1 .629a .396 .354 1.644 .396 9.505 8 116 .000 1.769
a. Predictors: (Constant), Quarter Hourly Massage of the Uterus within First 2 hours, Barriers Faced in Correct AMTSL
Administration, Immediate Massage of the Uterus by birth Attendant, Effects of Gender on AMTSL Implementation, Midwives
Delivery of Placenta by CCT Method, Factors that Promote AMTSL Administration, Correct Oxytocin Administration Within One
minute Post delivery, Suggestion on AMTSL Reinforcement
b. Dependent Variable: References on guides on AMTSL performance.
Table 32. ANOVAb
Model
Sum of
Squares Df Mean Square F Sig.
1 Regression 205.576 8 25.697 9.505 .000a
Residual 313.624 116 2.704
Total 519.200 124
a. Predictors: (Constant), Quarter Hourly Massage of the Uterus within First 2 hours, Barriers Faced in
Correct AMTSL Administration, Immediate Massage of the Uterus by birth Attendant, Effects of Gender
on AMTSL Implementation, Midwives Delivery of Placenta by CCT Method, Factors that Promote
AMTSL Administration, Correct Oxytocin Administration Within One minute Post delivery, Suggestion
on AMTSL Reinforcement.
b. Dependent Variable: References on guides on AMTSL performance
CHAPTER FIVE
SUMMARY OF FINDINGS, DISCUSSIONS, CONCLUSIONS AND
RECOMMENDATIONS
5.0 Introduction
This chapter covers the summary of the study, the conclusion and the recommendations on the current level of knowledge and competency of midwives in implementation of active management of third stage of labor in selected health facilities of Meru County.
5.10 Discussions
Active management of third stage of labor is an important strategy in reducing post partum hemorrhage which leads to maternal morbidity and mortality. The WHO in conjunction with ICM/FIGO introduced it in order to reduce maternal deaths related to PPH. Primary data was collected using questionnaires, interview guide and observational checklistand the data analyzed using SPSS VERSION 20.0. The mean age of midwives was 36-40 years and majorities were females (78%) compared to males (22%). From the study, 125 respondents filled-in and returned the questionnaires making a response rate of 100%. According to Mugenda and Mugenda (1999) a response rate of 50% is adequate for analysis and reporting; therefore, the response rate obtained in this study was excellent for analysis and reporting.
60.8% of the respondents did not carry quarter hourly massage of the uterus within the first 2 hours as stipulated in the guidelines. A comparative study done in the seven countries i.e. Benin, El Salvador, Ethiopia, Honduras, Indonesia, Nicaragua and the United Republic of Tanzania by WHO, (2009) was in agreement as it indicated that the general use of oxytocin, during the third or fourth stage of labor is nearly universal but the practice of fundal massage immediately after delivery of the placenta and follow-up palpation is low in most countries, suggesting insufficient surveillance of women during the hours when most maternal deaths occur worldwide. Knowledge of AMSTL was low among the birth attendants in Meru county as (55.2%) of the midwives could not mention the three sequential components of AMSTL correctly. In a study carried out in Tanzania only 9% of birth attendants could correctly mention the three components of AMSTL (Godfrey, et al 2009). The study was therefore important in assessing the effort made by Kenyan government in ensuring compliance to the international standards set out by WHO in collaboration with ICM/FIGO and in this regard, it’s clear a significant milestone has been achieved though not fully.
The findings of this study revealed that majority of the midwives were aware of AMTSL as an obstetric intervention in the prevention of PPH and that it is made up of three (3) components and this was in agreement with previous studies (Vivio et al., 2010; Afshari et al., 2012; Harvey et al, 2007) which reported that more than half of the respondents were aware of AMTSL.
On utilization of AMSTL the findings revealed that though midwives indicated high practice (97.6%), on observation only correct delivery of the placenta by CCT had the highest score (81.6%) as per the standard guidelines. This shown a wide gap that existed between the current evidence based standard and current levels of provider competence a similar observation noted in Nicaragua by Harvey et al., (2007). Immediate massage of the uterus (63.2%) and controlled cord traction (81.6%) were done by most midwives but few massaged the uterus quarter hourly within the first two hours. The findings were contradicted by a study carried out by Rizvi, et al., (2004) which reported 100% adherence on successful reduction of massive PPH by use of standard guidelines by the midwives.
Most of the midwives performed clerical duties citing understaffing (40.8%) thus reducing the time for provision of intra partum and post partum care and this significantly contributed to the poor maternal outcome. This was in agreement by Ashcroft et al., (2003) who suggested that absolute staffing level was crucial for
The study also established that majority (78%) of the midwives were females. This implies that gender variation is a common factor observed by other studies and these findings concurred with previous reports (Piper, 2010; Dean, 2011) about the origin of midwifery practice by women inside the order of Catholic Church in the late middle ages.
WHO,(2014) recommended that maternity care providers should receive fresher training or updates in midwifery every 3-5 years in order to improve on the skill. On contrally the study carried in Meru County21.6% reported no refresher training done and therefore a need to observe such guidelines for better outcome. The availability of WHO reference materials in selected health facilities of Meru county was low (18.4%) contrary to Guatemala with (66.75%) of these documents. The association between availability of standard document and utilization of AMSTL is statistically significant. Majority 122(97.6) of midwives in Meru county use AMSTL as the standard guideline and this study was in agreement with a report by POPPH (2006b) at cereboni which (81.3%) use AMSTL.
5.1.1Studylimitations
The study was limited to midwives in selected health facilities of Meru County excluding other midwives who could have challenges in their area of AMSTL practice and this can affect results due to generalization. Another limitation was use of observational check list method that can affect the validity and reliability of study outcome especially when the respondents are aware of being observed as they perform AMTSL and change the behavior under the study. Stratification of the health facilities was also a major challenge since the county had upgraded some facilities within the period of data collection and in essence some facilities could not meet the standard classification for that tier during that period.
5.2 Summary
The findings revealed that majority (78%) of the midwives were female and aged between 26 and 30 years. In addition most (81.6%) of the midwives had college as their highest education level and (69.6%) had diploma in midwifery. The registered nurse midwives who were the majority had an experience of between 7 to 10 years of experience in their profession.