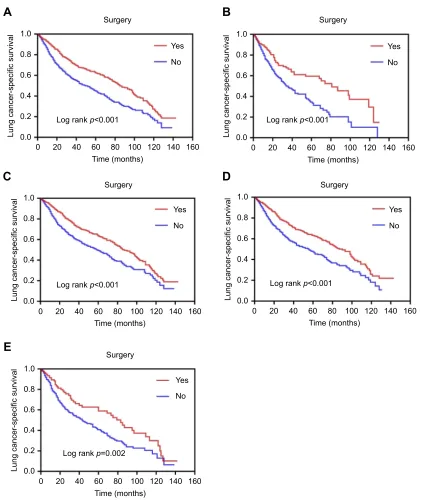
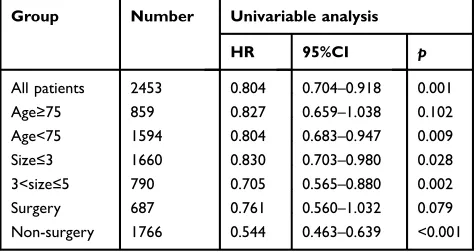
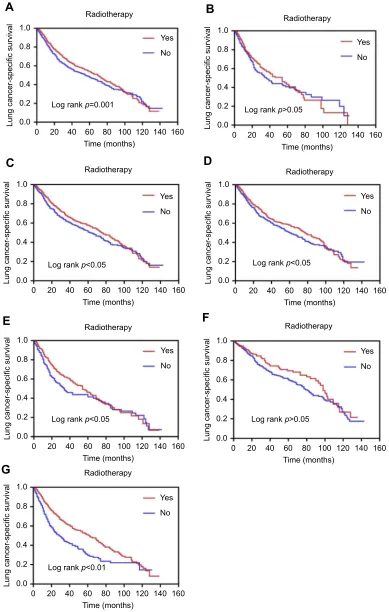
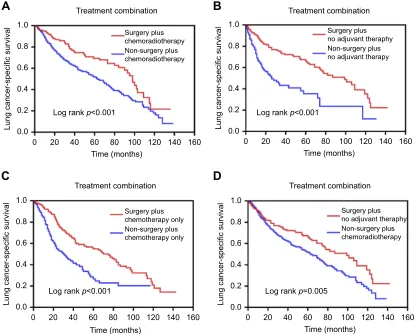
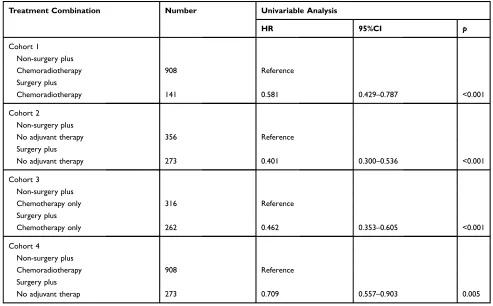
<p>Role of surgery in patients with early stage small-cell lung cancer</p>
Full text
Figure
Related documents
The results confirm gender gaps related to farm performance, networking, diversification strategies and access to rural policies, by enlightening diverse paths of development in
These include: entry into commercial banking, ownership of bank restrictions, capital standards, allowable activities for banks, external auditing requirements,
Motivated by the above consideration, this study uses the non-parametric cointegration test recently proposed by Bierens (1997) to re-examine the issue of stock markets
In this paper, I provide evidence on the development of gross and net asset posi- tions for a group of 23 developed countries over the period 1960-2008. The data show that both
The project aims to capture that process water in a storage reservoir and pump it back into the building’s industrial line (effectively recycling the water).. (2) Please
The Bank increased the monetary policy restriction when the economy experienced adverse cost-push shocks in 1998 and 2002-2003 that not only affected inflation, but also
The second most important incentive for the Serbian dairy producers to implement HACCP was the quality increase of their products (Table 4) which could be unexpected
To determine whether amlodipine can alter the inflammatory responses, we investigated its effects on gingival fibroblast cell culture, analyzing the gene expression profile
