Building platform for implementation of GPP in the
Republic of Macedonia
A Report of the Project 2012
Authors
Professor Lidija Petrushevska-Tozi, PhD
Faculty of Pharmacy, University Ss Cyril and Methodius, Skopje, Macedonia
Pharmaceutical Chamber of Macedonia
Professor Kristina Mladenovska, PhD
Faculty of Pharmacy, University Ss Cyril and Methodius, Skopje, Macedonia
Pharmaceutical Chamber of Macedonia
Contributors
Jasminka Patceva, pharm.spec
Pharmaceutical Chamber of Macedonia
Dr Dick Thromb,
EuroPharm Forum, President
Kirsten Holme,
Professional secretary EuroPharm Forum ,
Project manager at Pharmakon WHO Collaborative Centar
Nina Sautenkova,
WHO Europe, programme manager at World Health Organization
Acknowledgements
The authors and PCoM gratefully acknowledge the EuroPharm Forum and WHO Europe for
financial and expert support for the project. We are particularly thankful to Kirsten Holme, Dick
Tromb and Nina Sautenkova for their commitment to help pharmacists in Macedonia to
implement GPP. We would like to thank the pharmacists in Macedonia (community and
hospital) for participating in this study by answering and commenting the questionnaires. All
outstanding errors are our own.
Suggested citation: Petrushevska-Tozi L, Mladenovska K.
Building platform for implementation
of GPP in Macedonia. A Report from the project 2012,
Pharmaceutical Chamber of Macedonia,
2012
Content
Introduction
5
Methodology
18
Results
23
I Community pharmacy practice and services
23
I.1. Demographic characteristics and management of community pharmacies
23
I.2. Indicators and components included in the PP and PSs assessment
tool and scores from the community pharmacies in the RoM
30
II Hospital pharmacy practice and services
38
I.1. Demographic characteristics and management of hospital pharmacies
38
I.2. Indicators and components included in the PP and PSs assessment
tool and scores from the hospital pharmacies in the RoM
44
Discussion and recommendation for improvement of PP and services
54
Legal framework
54
Economic framework
60
Workforce framework
62
Standards for good pharmacy practice
67
Conclusion
78
References
88
Annex 1
93
Glossary
RoM Republic of Macedonia MoH Ministry of Health HIF Health Insurance Fund
HPL Health Protection Law (Law on Health Protection)
DB Drug Bureau
PCoM Pharmaceutical Chamber of Macedonia MCoM Medical Chamber of Macedonia
MAP Macedonian Association of Pharmacists
FF-UKIM Faculty of Pharmacy at the University “Ss Cyril and Methodius” Skopje HIL Health Insurance Law (Law on Health Insurance)
LMMD Law on Medicines and Medical Devices NDIC National Drug Information Centre NCP National Centre for Pharmacovigilance GPP Good Pharmacy Practice
DRG Diagnoses Related Groups HEI High Educational Institutions FIP Federation International Pharmacy
PSs Pharmacy Services
PP Pharmacy Practice
PC Pharmaceutical Care
CPD Continuing Professional Development
CE Continuous Education
CCE Center for Continuous Education PoM Prescription only medicines NPoM Non prescription only medicines
DPFM-UGD Department of Pharmacy at the Faculty of Medicine, University “Goce Delcev” Stip DPUT Department of Pharmacy at the University Tetovo
PK Pharmaco Kinetics
PD Pharmaco Dinamics
TDM Therapeutic Drug Monitoring MTM Medication therapy management ADR Adverse drug reaction
CPOE Computer prescribing order entry system
Introduction
The Republic of Macedonia (RoM) is a landlocked country in the heart of the Balkan Peninsula (Fig. 1), in Southeastern Europe, with about 2 100 000 inhabitants and 25.713 km2. In autumn 1991, after 45 years union with five other republics in the Socialist Federal Republic of Yugoslavia, the country gained independence in a peaceful secession and established political system as a parliamentary democracy. As foreign policy priorities, peaceful and stable relations with the all neighboring countries and accession to the European Union and the collective security system of the North Atlantic Treaty Organization are considered. Economic reforms have focused on fully establishing market economy structures, including deregulation and introduction of the necessary privatization trends in the public sector, liberalization of international trade, etc. Alongside facing a number of unforeseen obstacles owing to regional instability, reform implementation has been faced with frequent political changes. Since independence, the RoM has seen six prime ministers and 11 different compositions of government. During the same period, 14 ministers of health have been appointed, which indicates the stewardship challenges for continuous and consistent health policy1,2,3.
Fig. 1. Map of the Republic of Macedonia(Source: United Nations Cartographic Section).
The population density is 79.00 inhabitants/km2, 60 % live in urban areas. The population growth rate is 0.257% (2010 est.). Life expectancy at birth for both sexes has increased slightly from 72.12 years in 1991 to 74.92 years in 2010. However, this figure is still much lower than in Western Europe and was five years below the EU average of 78.49 years in 2004. Median age is 35.4 yrs (2010) with 11.6% of population over 65 years. In the period 1999-2009, the percent of population up to 14 years decreased from 22.8 to 17.1%, while for population older than 65 years, it increased from 22.8 to 11.6%. Thus, the RoM shows a tendency towards an ageing population with similar problems of health care and social care system as elsewhere in EU. Neonatal mortality rate, under 5 mortality rate, maternal mortality ratio and adolescent fertility rate are lower than average in the region. Immunization coverage is high. Cardiovascular diseases (57.9%) and malignancies (19.4%) are the main causes of mortality, followed by
With a gross national income per capita of around $4120 in 2008, the RoM is a lower middle-income country. GDP per capita (PPP) is $10,500 (2011 est.) Official unemployment is high, 29.1%. Macroeconomic stability is maintained and GDP growth is modest, but positive. According to WHO estimates, total health expenditure as a percentage of GDP in the RoM amounted from 6.8% in 2002 to 6.9% in 2009. This represents a significantly lower figure than that of the most of the other ex-Yugoslav countries and the EU. In the same year, the health care expenditure in US$ (with purchasing power parity) per capita amounted to US$ 341, with 84.7% of health expenditure coming from public sources. Expenditure for investment in the health sector (0.7%) continued to be insufficient5.
Following independence, the RoM inherited the health care model from the former Yugoslavia. In line with the highly decentralized health system structures that had been in place in the Socialist Federal Republic of Macedonia, the beginning of the 1990s saw a health system that was organized in stand-alone, self-managing communities, with only the projects requiring large-scale capital investments being centrally coordinated6. The decentralized system led to fragmentation of service delivery and significant oversupply and duplication of both facilities and services. Moreover, a series of different units were established that frequently contained elements of primary, secondary and tertiary care. From that period until recently, the country has moved from highly decentralized to more centralize structures, while at present, the political aim is to move back to a decentralized system. The RoM set up an insurance-based health system with the Government and the Ministry of Health (MoH) providing the legal framework for operation and stewardship and the Health Insurance Fund (HIF) being responsible for the collection of contributions, allocation of funds and supervision and contracting of providers. Today HIF is an independent institution monitored by the MoH, with a central office in Skopje and branch offices at local level.
Numbers of other reform initiatives in the field of health care were undertaken with an aim of sustaining access for the whole population to a comprehensive health system as well as to improve the quality of health services and enhance financial sustainability. But still the system was facing a number of challenges. The Ministry of Health’s core functions were focused on health policy formulation and implementation, priority-settings and monitoring of the health system’s performance. The need for the MoH to develop a stronger role in policy development, implementation, monitoring and analysis and to establish its role as a leader of strategic development in the health sector, including human resources policy, has long been recognized but has proven difficult to address7. Against this background, the development of a new law was initiated. The Health Protection Law (HPL)8 of August 1991 laid the groundwork for the current health system and has served as the framework for health policy ever since. Based on the HCL, Drug Bureau (DB) was established as a unit of the MoH to take care of pharmaceuticals, registration and licensing procedures for medicines, remedial medicines and medical devices and to participate in the preparation of the essential and positive drug lists. Also, based on the HCL and later by means of a separate Health Insurance Law (HIL)9, the system of compulsory health insurance was established. Equity, solidarity and reciprocity as well as provision of universal coverage for the population have been defined as its core values. However, the established structures have been characterized by large-scale inefficiencies in performance, the absence of uniform performance standards, inequalities in health care delivery and insufficient financial support from the central budget for the health care system. In 1992, “medical”, “dentists” and “pharmacists” chambers were established, being responsible for licensing/relicensing of health professionals and their continuous professional development; and the responsibility for continuous education was given to the medical, dentists and pharmacists associations.
The Pharmaceutical Chamber of Macedonia (PCoM) was established as a professional association of all registered pharmacists of Macedonia. It is responsible for protection and promotion of the pharmacists’ competences and strengthening the role of the pharmacists in all aspects of the heath care system10. PCoM regulates the ethical aspects of the pharmacy profession, but also protects its interests and/or the interests of the pharmacists. As a professional organization, it assures the continuing education and licensing and re-licensing processes in the manner of professional development. For all the activities, good relations and cooperation with the governmental bodies (e.g. MoH, HIF, DB, Accreditation Agency), non-governmental associations (Medical Chamber of Macedonia (MCoM), Macedonian Association of Pharmacists (MAP), etc.) and academia (Faculties/Departments of Pharmacy) have been established, which can be confirmed by the involvement of the PCoM in all key projects and legislation procedures related to the pharmacy practice and education of pharmacists. PCoM has been involved in drafting Law on medicines and medical devices, Law on health care, Law on recognition of professional qualifications, Health strategy 2020, Contracts between the community pharmacies and HIF and related rulebooks. Considering the education of pharmacists, the PCoM collaborated with the Faculty of Pharmacy at the University “Ss Cyril and Methodius” (FF-UKIM) in Skopje in the project titled “Restructuring of Pharmacy Education in the Republic of Macedonia”, financed by TEMPUS program (as a joint project of the Faculties of Pharmacy in Skopje, Copenhagen and Stockholm and the PCoM). The project activities resulted in a modern graduate study program for obtaining title Master in pharmacy organized as a 1stand 2ndintegrated cycle according to Bologna. Also, partnership with the MCoM was established regarding continuous education and professional development i.e. re-licensing of pharmacists.
Besides reform achievements in pharmaceutical sector related to the strengthening of the capacities (e.g. establishing of MoH, HIF, DB, PCoM), the establishment of a National Drug Information Centre (NDIC) in 1998 as an institution responsible for collection, processing and dissemination of information and data concerning drug control, registration and rational prescribing was one of the major achievements. A National Centre for Pharmacovigilance (NCP) was also established in 1991. In 1997, it was networked with the WHO Center for Drug Adverse Effects as accompany member, while full membership was obtained in 2000. The main task of this Center is to collect data on adverse drug reactions and give recommendations regarding any withdrawal of a drug from the market that may ultimately be necessary11.
Today, health care in the RoM is delivered through a system of health care institutions covering the country’s territory relatively evenly. The health facilities range from health care stations and centers at primary health care level and specialty-consultative and inpatient departments at secondary level to university clinics and institutes at tertiary level, with the latter also carrying out research and educational activities. Recent years have seen substantial growth of the private sector, especially in the field of primary health care. The private practice is regulated by the Law on health care of 1991 with amendments in 2004 and 2005. In 2005, the private sector employed roughly one third of all physicians working in primary care, the privatization of dentists’ offices at primary care level has been completed and the process of privatizing publicly-owned pharmacies by sale or leasing has been initiated in 2005 and completed in 2007.8 With the privatization process, pharmacists and pharmacy managers (not obligatory having pharmaceutical education) became owners of the space and equipment only, with the same level and scope of services (i.e. procurement, storage and dispensing of medicines) and lot of professional problems typical for the countries in transition. The privatization system intended to spread liberalization, however, led pharmacy to be increasingly seen as a part of the commercial sector rather than a part of the professional system within health care.
In order the process of privatization to be supported, the World Bank provided assistance through several projects such as the project for “Quality Improvement of Health Services and Licensing” by which the model for continuing education and licensing was established based on a modern best practice processes for the health professionals (including pharmacists). In addition, under the “Health sector management project”12, also financed by the World Bank, the MoH of the RoM (Project Coordination Unit) and the PCoM prepared and realized training seminars for "Developing pharmacy practice" for community pharmacists conducted by the experts from the university and practice (2007/08). The main goal of the training seminars was to improve the quality of pharmaceutical services in community pharmacies and to increase patient satisfaction by establishing a basis of a modern best practice process and Good Pharmacy Practice (GPP) for the pharmacy professionals in the reformed health care system in Macedonia. The key objectives were focused on preparing appropriate training material on pharmaceutical care and GPP, including pharmacovigilance. Fourteen workshops for about 500 participants from all around the country were carried out. The key outcome included recognition of the new roles, skills and attitudes beyond the scope of the traditional pharmacy practice and within the GPP, which pharmacists need to master in order to become members of multi-disciplinary health care teams as well as added values which they can provide through their professional input and expansion of existing roles. The enthusiasm among the community pharmacists for adopting new roles and responsibilities was evident although aware that the implementation of GPP in community pharmacies was a major problem due to the overall economic development and lot of problems that had to be solved within the overall health system, among which the following with the highest priority: legislation not supporting the best pharmacy practice and pharmaceutical care concept; low level of community pharmacy practice and services; lack of knowledge sufficient for introducing and implementation of pharmaceutical care services in community pharmacies; low level of cooperation (partnership) between the health care providers (e.g. prescriptionists and pharmacists); lack of inter-professional training programs, etc13.
In 2009, FIP Foundation for education and research under FIP approved the PCoM application for the project titled ”Implementation of GPP in Macedonia” under the call for projects Future Implementation Plan for Good Pharmacy Practice (GPP)14. Implementation of pharmaceutical care services in community pharmacies, improving quality of the pharmacy practice and pharmaceutical care in community pharmacy settings through implementation of GPP standards established on a basis of a modern best practice process were the main objectives of the project. The following aims were also included in the project proposal: (i) review on the current status of Macedonian community pharmacy in both practice and research; (ii) identification of the perceived barriers to implementing best pharmacy practice and pharmaceutical care in the community pharmacy settings; (iii) definition of the main priorities for intervention to improve the quality of the pharmacy practice and pharmaceutical care services in line with the National Drug Policy and WHO/FIP Guidelines on GPP; (iv) setting up a plan of action for stepwise approach and managing pharmacy practice and pharmaceutical care changes; (v) providing assistance in developing mechanisms and tools for monitoring of the implementation process and dissemination of the results. Unfortunately, although approved, this project was never financed by FIP. Today, there are 740 private-owned community pharmacies all around the state with unbalanced distribution in some geographic regions (Table 1) and 44 hospital pharmacies located in general and clinical hospitals in secondary and tertiary care with in-patients beds (Table 2). Five private hospitals/hospital pharmacies have been established since 2005 covering the following specialties:
Table 1. Network of community pharmacies per regions/cities Region/Location of community pharmacy Actual number* Maximum number** Citizens (total) Pelagonija 107 77 234.137 Bitola 56 31 93.585 Mogila 0 2 6.542 Novaci 0 1 3.386 Demir Hisar 3 3 8.826 Krusevo 2 3 9.569 Prilep 34 25 76.389 Dolneni 0 5 13.743 Krivogastani 3 2 5.862 Resen 9 5 16.215 Vardar 54 43 133.106 Veles 27 18 55.064 Gradsko 0 1 3.632 Caska 1 3 7.690 Kavadarci 23 13 39.011 Rosoman 2 1 4.140 Negotino 1 6 19.417 Demir Kapija 0 1 4.152 North-East 57 58 175.045 Kratovo 3 3 9.848 Kriva Palanka 5 7 20.431 Rankovce 0 1 3.873 Kumanovo 49 36 107.365 Lipkovo 0 10 29.156 Staro Nagoricane 0 1 4.372 South-West 70 74 221.855 Debar 5 7 20.217 Kicevo 17 10 30.226 Drugovo 0 1 1.273 Zajas 1 4 11.853 Oslomej 1 4 10.590 Makedonski Brod 1 2 6.609 Plasnica 1 2 4.762 Ohrid 25 18 54.759 Debarca 0 2 4.730 Struga 17 21 64.453 Vevcani 1 1 2.499 Skopje 233 207 619.718 South-East 76 59 172.858 Valandovo 4 4 11.936 Gevgelija 14 8 22.951 Bogdanci 3 3 8.499 Dojran 1 1 3.338 Radovis 11 10 28.695 Konce 0 1 3.565
Bosilovo 2 5 14.129 Vasilevo 3 4 12.572 Novo Selo 5 4 11.070 Polog 76 106 314.804 Gostivar 22 28 82.554 Vrapciste 2 9 26.798 Mariovo, Rostusa 1 3 8.843 Tetovo 40 30 89.730 Brvenica 1 5 16.432 Bogovinje 1 10 30.154 Zelino 1 9 26.697 Jegunovce 0 4 10.866 Tearce 5 8 22.730 East 67 67 200.522 Berovo 3 4 13.404 Pehcevo 1 2 5.188 Vinica 1 7 19.533 Delcevo 6 6 16.964 M. Kamenica 5 3 7.863 Kocani 22 13 38.187 Zrnovci 0 1 3.146 Cesinovo,Oblesevo 0 2 7.226 Probistip 6 5 15.665 Sv. Nikole 2 6 18.114 Lozovo 0 1 2.638 Stip 21 16 48.517 Karbinci 0 1 4.077
*actual number-the number of existing pharmacies
**maximum number-the number of maximum needed pharmacies
Source: Regulation for Network of Health Institutions (Official Gazette of RoM, No. 81/12)
general medicine, gynecology/obstetrics, (cardio)surgery and ophthalmology. A new Rulebook for establishing pharmacies is expected to be issued by the end of the year. The MoH has drawn up a “medical map” (carte sanitaire 2008) to provide regulatory basis for further expansion of the private sector i.e. in future, licenses for opening private clinics or hospitals or community pharmacy will be issued according to the need. In July 2012, the MoH has drafted a network of health institutions, incl. network of community pharmacies, to ensure proper coverage with health institutions all over the country15. Health institutions included in the network have signed contracts with the HIF. Contracts with the HIF can be signed only after obtaining license for work issued by the MoH. All state/private health facilities are allowed to apply for contracts with the HIF. HIF, however, have the right to contract selectively, according to the criteria set out in the Rulebook16. The contracts with the HIF are modified every year in order to best regulate the mutual relationships17,18. As there is only one HIF in the RoM, the provisions in the contracts are mostly in favor of the HIF.
Table 2. Network of general and clinical hospitals (with central and satellite pharmacies) in secondary and tertiary health care level with in-patients beds
Name / location of the hospital (hospital pharmacy) Ownership/Level of care Clinical Hospital, Bitola Public / Secondary
General Hospital, Gostivar Public / Secondary General Hospital, Gevgelija Public / Secondary
General Hospital, Veles Public / Secondary
General Hospital, Kavadarci Public / Secondary General Hospital, Kicevo Public / Secondary General Hospital, Kocani Public / Secondary City General Hospital 8thSeptember, Skopje Public / Secondary University Clinic of Surgical Diseases Sveti Naum Ohridski, Skopje Public / Tertiary Psychiatric Hospital, Skopje Public / Secondary University Pediatric Clinic, Skopje Public / Tertiary University Hospital Pharmacy, Skopje Public / Tertiary University Clinic of Hematology, Skopje Public / Tertiary University Clinic of Abdominal Surgery, Skopje Public / Tertiary University Clinic of Gynecology and Obstetrics, Skopje Public / Tertiary University Clinic of Radiotherapy and Oncology, Skopje Public / Tertiary University Clinics of Urgency, Traumatology, Orthopedic, Anesthesiology and
Reanimation, Skopje
Public / Tertiary Special Hospital for Gynecology and Obstetrics Cair, Skopje Public / Secondary General Hospital, Kumanovo Public / Secondary
General Hospital, Ohrid Public / Secondary
General Hospital, Prilep Public / Secondary Institute of Nephrology, Struga Public / Secondary General Hospital, Struga Public / Secondary General Hospital, Strumica Public / Secondary Clinical Hospital, Tetovo Public / Secondary
Clinical Hospital, Stip Public / Secondary
Psychiatric Hospital, Demir Hisar Public / Secondary Psychiatric Hospital, Negorci Public / Secondary Special Hospital for Pulmonary Diseases, Lesok Public / Secondary Institute for Prevention, Treatment and Rehabilitation of Chronic Respiratory,
Non-specific and Allergic Diseases, Otesevo, Resen
Public / Secondary Special Hospital for Pulmonary Diseases and Tuberculosis, Jasenovo, Caska Public / Secondary
General hospital, Debar Public / Secondary
Special Hospital for Orthopedic and Traumatology Sveti Erazmo, Ohrid Public / Secondary Re-Medika Hospital, General Hospital, Skopje Private / Secondary Special Hospital for Surgical Diseases Filip Vtori, Skopje Private / Secondary Acibadem Sistina Clinical Hospital, Skopje Private / Secondary Specialized Obstetric Gynecology Hospital Sveti Lazar, Skopje Private / Secondary Special Hospital for Ocular Diseases European Ophthalmology Hospital, Skopje Private / Secondary Health Institute, Kriva Palanka Public / Secondary Institute for Prevention, Treatment and Rehabilitation of Cardiovascular
Diseases, Ohrid
Public / Secondary Institute of Pediatric Pulmonary Diseases Kozle, Skopje Public / Secondary Institute of Pulmonary Diseases and Tuberculosis, Skopje Public / Secondary Institute of Physical Medicine and Rehabilitation, Skopje Public / Secondary Gerontology Institute 13 Noemvri, Skopje Public / Secondary
In the Strategic plan of the MoH for 2009-201119, more improvements in the health care system were planned according to the priorities of the Government. One of these priorities was drafting improved legislation. New Law of health protection was issued in March 201220. This Act clearly defines all pharmaceutical activities as
“part of the health care activities, including purchasing of medicines and medical devices, production of medicines, distribution and drug quality control, giving information on drugs to patients and other health care providers, counseling and education on rational and effective use of medicines and medical devices and therapeutic drug management”.
This definition gives real opportunity for the pharmacists to perform wide range of pharmaceutical activities and services. The reimbursement of the drugs is on the basis of referent prices21. At present, the HIF reimbursement practices for pharmaceuticals on the positive list of drugs take insufficient account of the pharmacists’ overhead costs22,23. For the community pharmacies, the HIF is paying for the medicaments plus fix margin according to the scale based on referent price of the medicine, lower fee for lower referent price, higher fee for higher referent price (lower is 0,2 euro, higher is 3,33 euro). For the hospital pharmacies, the expenses are calculated according to the DRG system. The reference pricing system was established for the drugs in the primary care. Data collection on drug expenditure in the country is difficult as drug consumption is not monitored closely. In 2007, Law on medicines and medical devices was issued11. The Law is generally harmonized with the EU legislation, following all the EU provisions concerning pharmaceuticals. Under this Law, the pricing of medicines is regulated, which is not in line with the EU legislation. There is a single act titled “Methodology for establishing medication prices”24, adopted by the Government in October, 2011, which strictly defines the establishment of drug prices, on the basis of comparative study conducted in 12 countries (in the region, EU, including Russia and Turkey).
The pharmaceutical sector currently operates on the basis of a positive list of drugs (by generic names) that defines which drugs are eligible for reimbursement by the compulsory health insurance. The sector is supervised by the DB. The DB (MoH) and the PCoM issued National Drug Formulary25 in 2006 The National Drug Registry26, first time issued in 2006, is updated every year.
In the RoM, unlike most of the EU27 and most world countries, there is no Pharmacy law as a single legislative act to regulate the pharmacy practice and scope of pharmaceutical activities and services. Instead, in the Law on medicines and medical devices from 200711 there are 2 articles that outline the activities related to the medicinal retailing within pharmacies. This Act considers pharmacies to be legal entities where purchasing, storage and dispensing of medicines are undertaken. It is very encouraging that this Law creates new opportunity for pharmacies by endorsing the need to introduce quality systems and to organize work process according to the principles of GPP28. This document is a very short one with only 4 articles, but it provides directions for the evolution of the pharmaceutical activities into the pharmaceutical care concept. The GPP guideline explicitly quotes the need for development of national GPP standards to guarantee professional roles of the pharmacists and to ensure essential conditions are in place for implementation of GPP. Unfortunately, to date neither national standards have been developed, nor the wider professional debate has been initiated by the DB (MoH) to promote the concept of pharmaceutical care on a national basis.
In 2007 the Government, MoH and the DB have also clearly recognized the need for improvement in the health policy, decision making process at all level of health protection and the quality and efficiency of
achieving the goals were set out in the “Health strategy of the Republic of Macedonia (2020) for safe, efficient and just health system”29. The main objective of the Strategy at the level of primary care is to ensure the population to have a better access to the family- and community-oriented health care services supported by a flexible and responsive health system. The pharmacy practice problems and priorities for improvement are described in a separate chapter (titled Pharmaceutical services) where the weaknesses in the pharmacy practice are identified, such as irrational prescribing of drugs, lack of drugs in the pharmacies, submission of claims for drug cost reimbursement in front of the HIF, lack of data for the overall drug consumption in the country, training of health professionals, etc. Also, it is recognized that a system of compulsory and accredited continuing education required for relicensing has not been established yet. The financing of continuing educational activities was and it is still a problem in a view of the low income of health care professionals, incl. pharmacists. As another major bottleneck, lack of access to internet sources of information was detected. The Strategy also recognizes the steps for improvement of the pharmacy practice and services, including
(i) revision of the national drug policy from 2001;
(ii) renewal of the positive list of essential drugs (based on clinical protocols and guidelines) that will be fully reimbursed by the HIF;
(iii) establishment of referent prices for drugs, with generic names;
(iv) strengthening and enlarging the functions of the DB with its transformation into an autonomous Drug Agency authorized to control all phases of drug registration, import and distribution of pharmaceuticals and implementation of GPP in pharmacies.
The Strategy also points that the concept of pharmaceutical care is not a dominant form of practice for most of the pharmacists in the RoM. The transformation from commodity-based mercantile operations into a clinical profession is evaluated as very slow. It is emphasized that encouragement and setting appropriate GPP guidelines containing national standards are needed, which would meet professional-determined needs for pharmaceutical care. The necessity of developing standards for the pharmacy services which ensure proper co-ordination and communication between the health- and pharmaceutical care providers and consumers is also emphasized. It is recommended the number of the pharmacists (especially in the hospitals) to be increased, partnership between physicians, nurses and pharmacists to be strengthen, the role of the pharmacists in reporting adverse effects to be increased, participation of the pharmacists in clinical studies and ethics committees to be recognized, the communication and co-ordination between the pharmacies and/or pharmacists in the hospitals and community pharmacists to be improved and employment of specialists in clinical pharmacy and pharmacoinformatics in the hospital pharmacies to become obligated.
Another similar document, “Green Book - Improvement of the Health System in RoM” was also issued in 2009/2010 by the Committee for improvement of the health system in the RoM30. The Committee was established by the MoH with an aim to help the Government to finish the reforms in the health system. Valuable recommendations were gathered by the health experts in five areas: (i) management of the health system; (ii) health care practice; (iii) financing; (iv) pharmacy; and (v) patients rights. PCoM (pharmacy experts) has actively participated in drafting the recommendations. Main recommendations were focused on the need of issuing Law on pharmacy practice as a single legislative act, defining the structure and role of the community/hospital pharmacies/pharmacists, defining the mechanisms for transfer of patients through the levels of health care, defining the roles of the pharmacists in prescribing, strengthening the communication between the health care providers (pharmacists and
pharmacists (depending on their professional needs), establishing standards for the pharmacy structure, developing programs for therapeutic management, stimulating use of clinical guidelines and specialized formularies, increasing the budget for medicines and medical devices, etc.
Considering education of pharmacists, accredited high educational institutions (HEIs) in the RoM are the FF-UKIM in Skopje, Department of Pharmacy at the Faculty of Medicine, University “Goce Delcev” in Stip and the Department of Pharmacy at the State University Tetovo in Tetovo. They are all public HEIs and accredited by the National Accreditation Committee, which is under jurisdiction of the Ministry of education and science of the RoM. Criteria for enrollment in the 1stand 2ndlevel integrated pharmacy study programs include 4-year secondary education (gymnasium or secondary medical school) and state exam, excluding entrance exam. At these HEIs, the students are enrolled as regular full-time students and their education is financed or co-financed by the State. The pharmacy study programs at all HEIs last 10 semesters (1stand 2ndcycle integrated, 300 ECTS-credits according to Bologna). In the last (10th) semester, professional practice is provided and after graduation, the students obtain a title Master in pharmacy. Professional practice is conducted in community and hospital pharmacy. In the practical teaching and training, professionals from the university clinical centers, and hospital, community and industrial pharmacists are included. In 2009/2010, the Faculty of Pharmacy at UKIM in Skopje in collaboration with the PCoM introduced new pharmacy study program according to Bologna, harmonized with the study programs of several Faculties of Pharmacy in Europe (see above) and with the Directive 2005/36 on recognition of professional qualifications. In the period 2010-2012, new study programs related to pharmacy practice at 2nd level were also introduced and the existing ones modernized, such as the academic specialist and master study programs in health management & pharmacoeconomy, phytotherapy. At the Departments of Pharmacy/ Faculties of Medicine in Stip and Tetovo, only study programs in pharmacy at 1stand 2ndintegrated level (300 ECTS-credits according to Bologna) are conducted.
After graduation and obtaining diploma Master in pharmacy, additional 6-month professional practice in community and hospital pharmacy and in national/regional drug information centers is required for the pharmacists to obtain license for independent work. The training program is in accordance with the rulebooks31-37 issued by the PCoM, which is in compliance with the LHP8. The internship period of 6 months embraces five pharmacy fields: (i) community pharmacy, (ii) hospital pharmacy, (iii) clinical pharmacy, (iv) pharmacoinformatics and (vi) pharmacy legislation. After 6-month training, the residents have to pass the state exam in order to become licensed pharmacists i.e. eligible for independent work, registered in the PCoM register. The training program is under supervision of certified mentors and conducted by trained and certified (by the MoH) educators. The training program, state exam and licensing are under jurisdiction of the PCoM and in accordance with the Law on health protection. The state exam is conducted in accordance with the “Rulebook on state exam for masters in pharmacy” and the Examination committee is consisted of accredited examiners. Under the same LHC, the PCoM is authorized for recognition of the training, state exam and license conducted/obtained abroad for domestic and foreign citizens. During the exam, knowledge and skills in the area of pharmacy practice in hospital and community pharmacy are assessed. Under the Health sector management project38, the examination process was positively evaluated by external evaluators39. The comments of the external evaluators were as follows: “The assessments are criterion-referenced and are very well designed, reliable and valid. There are mark sheets and supporting documents available for the examiners and the students well prepared. Criteria are clear. The combination of the three forms of assessment gives a good profile of the student’s readiness to practice safely and competently. Students receive feedback on their performance and thus the assessments are formative as well as summative.
would not reach this stage without their deficiencies being recognized and addressed by the faculty and the educators and mentors). The assessments, dealing with relatively small numbers, are very well run and organized and are a model of postgraduate assessment)”. In addition, it was emphasized that a
Fig. 2. Education and training of the pharmacists in the RoM Graduate degree course
Five years covering
- Basic biomedical sciences (incl. physiology, anatomy, biochemistry, microbiology, pathophysiology, pathology) - Pharmaceutical chemistry
- Pharmaceutical technology - Drug quality control
- Phytochemistry and phytotherapy - Food and nutritition
- Pharmacotherapy - Pharmacy practice Postgraduate pre-registration Six month-training - Pharmacy practice - Regulatory affairs Professional examination
- Licensing (entry into the professional register)
CE and CPD
- All registered pharmacists are subject to relicensing after 7 yrs
- Collect credits by attending various types of CPD activities
Post-graduate education and training
-Many pharmacists voluntarily pursue further post-graduate academic and health professional degrees in fields as clinical pharmacy, drug information, phytotherapy, clinical biochemistry, pharmacy practice, etc.
- Gain certificate as (health) specialists in specific fields
good system of communication is in place to identify struggling students and also to improve the assessment and overall learning process. The assessors were evaluated as very competent and well briefed, supportive and encouraging of the students whilst remaining rigorous in their expectations. Starting from 2006, 941 pharmacy residents have passed the internship program and 886 successfully passed the state exam.
The masters in pharmacy may/must renew their license after 7 years by fulfilling the following conditions: at least 60% of working time in the profession during this period and participation in continuing education courses and professional development programs. By the same LHP, the temporal and permanent confiscation of license is regulated. According to the “Rulebook for types of continuing education activities and professional development programs, criteria and credits allocation for continuing education and professional development”40, the Expert Committee at the PCoM approves accreditation of the educational activities upon submission of the application and allocates credits depending on the type of the continuing education activities and professional development program. For the past 6 years, 205 workshops, seminars, symposiums and other forms of continuous education have been accredited.
Continuing education and professional development as well as application of modern scientific and expert achievements in practice are the main objectives and tasks of the Macedonian a ssociation of pharmacists, which is actively involved in organizing educational and scientific events, conventions and congresses which are rated in the CME system. Other institutions are also involved in organizing various types of educational activities, such as the Center for continuing education (CCE) and the NDIC located at and under jurisdiction of the FF-UKIM in Skopje.
Pharmacists may also obtain health specialist title in adequate field of health practice according to the LHP8 and the Rulebook for health specialist and subspecialist studies of health practitioners41. The Faculty of Pharmacy at UKIM in Skopje is the only designated HEI for organizing health specialist studies for the pharmacists in the RoM. Health specialist study programs were recently (2011) modernized and there are training programs in clinical pharmacy, pharmacoinformatics, medical biochemistry, drug quality control and testing, pharmaceutical technology, sanitary chemistry, toxicological chemistry, herbal drugs (pharmacognosy), medicinal laboratory genetics and pharmacy practice. Health specialist studies are fully regulated by the Law on h ealth protection, by which a system of mentorship and educators was introduced and the responsibilities of the health institutions where training is conducted, in respect to quality, agreement protocols and planning are regulated.42 Adoption of standards for pharmacy services (PSs) in 1993 by the International Pharmaceutical Federation under the heading “Good pharmacy practice in community and hospital pharmacy settings” developed as a reference to be used by national pharmaceutical organizations, governments and international pharmaceutical organizations to set up nationally accepted standards of Good Pharmacy Practice (GPP), their subsequent adoption in a wide number of developing countries43,44and significant changes in practice, applied science and technology and pharmaceutical policy that have occurred worldwide in community and hospital settings45-49were the main provocation for the PCoM to propose the project titled “Building platform for implementation of GPP in the Republic of Macedonia” for financial and expert support by the EuroPharm and WHO.
The main goal of the project is to set up a platform for improving the quality of the PP and PSs in community/hospital pharmacy settings through implementation of the GPP standards established on
achieved, a survey for the standards of PP and for the quality of PSs in the RoM was conducted with the aims given below:
to define the standards for PP and quality of PSs in the community and hospital pharmacies in the RoM in respect to the standards set in the Joint FIP/WHO guideline on Good Pharmacy Practice (GPP): standards for quality of pharmacy services;
to define the regulatory system and political, legal and economic framework supporting the PP and services in the RoM;
to identify the gaps and perceived barriers to implementing the best PP and pharmaceutical care (PC) in the community and hospital pharmacy settings in the RoM;
to assess the level of education, knowledge and skills of both the community and hospital pharmacists and their attitude towards PP, PC and continuing professional development (CPD);
to identify the main priorities for intervention to improve the quality of the PP and PC in line with the National Drug Policy and WHO/FIP Guidelines on GPP based on consideration of the realities, policies, strategies and new roles;
to create a document with set of recommendations for improving the PP and set up a plan of action for stepwise approach and managing the PP and PC changes;
to provide assessment tool for quantification of PP status and quality of PSs that can facilitate comparison of results over time.
Methodology
For these aims to be achieved, a descriptive indicator study has been used. Structured and standardized questionnaires, separately for the community and hospital pharmacies were designed and as stakeholders, 740 in total (individual and chain-) community pharmacies and 44 (central and satellite) hospital pharmacies were adequately targeted. Simple random sample design was used for both, community and hospital pharmacists, so the questionnaires were delivered to all community and hospital pharmacies by e-mail or mail using data base (e-mail addresses) for the pharmacies of the PCoM. For completion of the questionnaire by the community pharmacists, instructions and explanations were given to the responsible pharmacists of the regional offices (8 regional offices). For completion of the questionnaire by the hospital pharmacists, a workshop was organized during which the questionnaire was discussed and explanations for the complex issues were given.
In addition, as stakeholders, the DB within the MoH of the RoM, HIF, PCoM and FF-UKIM were also considered in order to define the legal, economic and educational framework for the PP and PC in the RoM. The information from these stakeholders was collected by meetings and from available documentation and legislation.
The information from the questionnaire for the community pharmacies was collected partly by e-mail or mail (using the Dillman Method)50 and partly by face-to-face in the pharmacy where the respondent works. The time elapsed before receiving the completed questionnaires was not longer than 5 weeks (May-June, 2012). For the hospital pharmacies, having in regard the relatively low number of hospital pharmacies and participation of the hospital pharmacists at the workshop, the information was completely obtained by in-person. Of 740 total number of community pharmacies, 123 responses were obtained from the chain pharmacies and additional 122 responses from the individual pharmacies. Considering the hospital pharmacies, 31 responses out of 44 were obtained. It is worth to emphasize that in 17 out of these 44 general or clinical hospitals or institutes with in-patient beds, no pharmacists are employed and for the purchasing and dispensing of drugs and for the PC (if any) mostly medical technicians are engaged. Improving the standards of PP and quality of services and recognition of existing and adoption of new pharmacists’ roles was a motivation for the pharmacists to show enthusiasm and interest to participate in the survey.
Improving legislation and creating better climate for PP and PC services was the point of interest for the DA and MoH of the RoM, HIF and PCoM, while for the FF-UKIM, the interest was focused on creating new academic and/or specialist study programs and types of CPD activities (within the CCE established at the FF-UKIM) to increase pharmacists knowledge and skills for performing the best PP.
Populations of interest were all the pharmacists and pharmacy technicians employed at the community and hospital pharmacies on the territory of the RoM. According to the data from the Register of the PCoM, there are app. 1140 community pharmacists, 1225 pharmacy technicians (app. 74 working in the hospital pharmacies) and 56 hospital pharmacists. The number of community pharmacists varies significantly from year to year due to the great variations in the number of pharmacies (app. 30 community pharmacies are opened and 15 are closed per year). Most of the community pharmacists are female, 80%vs. 20% male pharmacists. Average number of pharmacist per community pharmacy is 1.4, while the average number of employees per pharmacy is 2.86. The average age is 30±5 yrs. For the hospital pharmacists, the proportion of female pharmacists is significantly higher, 95% vs. 5% male pharmacists, with an average age of 35±5 yrs. Average number of pharmacist per hospital pharmacy is
of employees per pharmacy is 3.79 (incl. cleaning personnel and administration). The number of prescriptions/per year for reimbursed medicines (by HIF) in 2010 was 15.228 (increasing app. 2000 per year), while average value per prescription is 1.9 euro.
The resources (financial and expert) for designing the questionnaires and conducting the survey were provided dominantly by the EuroPharm Forum, WHO and the PCoM. In creating questionnaires, conducting the survey/interviews and analysis of data collected, 2 professors with a background understanding of GPP from the FF-UKIM (members of the PCoM), Lidija Petrusevska Tozi (president of the PCoM for app. 10 yrs, professor at the FF-UKIM) and Kristina Mladenovska (specialist in clinical pharmacy, 10 yrs working experience in hospital pharmacy, professor at the FF-UKIM) and 1 administrative officer Jasminka Patceva (specialist in pharmaceutical regulatory affairs, 10 yrs working experience in community pharmacy, employed at the PCoM) were involved. The questionnaires were revised by Dr Dick Thromb, president of EuroPharm Forum, and Kirsten Holme, professional secretary EPF, Pharmakon-WHO Collaborative Centar, and Nina Sautenkova, NIS programme manager at World Health Organization, who also participated in creating the overall project proposal. The meetings were organized with the representatives from the stakeholders, the DB (MoH), HIF and FF-UKIM and the data were also collected by inspection in available documentation, laws and rulebooks. With the survey, the issues given below were explored.
For the community pharmacies (Annex 1), set of 155 structural process and outcome indicators were identified covering five essential components given below. The indicators describe the highest standards of PP and quality of PPs. Data for the demographic characteristics and management of the community pharmacies were also collected.
I Pharmacy structure and practices (60 indicators) - Pharmacy structure (premises, equipment, etc.)
-Supplying, storage and stock - Dispensing
- Access to drug information
II Patient – access to patient data, communication, counseling and education (25 indicators) III Manufacturing practice and drug quality control (13 indicators)
IV Staff – workflow, competency and professional development (25 indicators) - Workflow
- Competency, continuing education and professional development V Quality assurance, risk and data management (32 indicators)
For the hospital pharmacies (Annex 2), set of 191 structural process and outcome indicators were identified covering five essential components, given below. Data for the demographic characteristics and management of the community pharmacies were also collected.
I Patient safety (39 indicators) - Patient information
- Patient counseling and education II Drugs and medication devices (81 indicators)
- Drug & medication device information - Ordering communication
- Purchasing, storage, labeling, distribution and administration III Manufacturing practice (13 indicators)
- Production
- Drug quality control
IV Environment, workflow and staff availability and qualifications (30 indicators) - Environment and workflow
- Competency, continuing education and professional development V Quality assurance and risk management (28 indicators)
For the DB and MoH, the following issues were covered:
I Regulations/restrictions on location and number of pharmacies (geographic and demographic criteria) II Regulations/restrictions on ownership (limitation of ownership to pharmacists, limits to the ownership of multiple pharmacies i.e. pharmacy chains)
III Criteria for establishing pharmacy (room, equipment, staff) IV Distribution of pharmaceutical products outside a pharmacy V Opening hours
As source of information, the Law on health protection, Law on medicines and medical devices, rulebooks relevant for establishing pharmacies and performing pharmacy practice and Regulation for
For the HIF, the following issues were covered: I Pricing regulation
II Contracting
III Remunerations and incentives mechanisms
As source of information, the Law on health insurance, Law on medicines and medical devices, rulebooks relevant for contracting pharmacies and performing/reimbursement of pharmacy practice were considered.
For the PCoM, the following issues were covered: I Registration
II Licensing and relicensing III Accreditation of CPD activities
III Relations with governmental institutions, academia and professional associations
As source of information, the Law on health protection, Law on medicines and medical devices, rulebooks relevant for licensing/relicensing, accreditation of CE activities were considered.
For the FF-UKIM, the following issues were covered:
I Graduate study program in pharmacy, with particular emphasis on PP and PC (harmonization with Directive 2005/36/EC on the recognition of professional qualifications)
II Postgraduate professional (academic and specialist) study programs covering PP and PC (harmonization with Directive 2005/36/EC on the recognition of professional qualifications)
III Involvement of the NDIC at the FF-UKIM in PP of the community and hospital pharmacies
IV Involvement of the CCE at the FF-UKIM in continuing education and CPD of the community and hospital pharmacists
As source of information, the study programs accredited by the Ministry of education and science at the FF-UKIM, relevant rulebooks and the Statutes of the Faculty and University were considered51,52.
In writing the questionnaires, various publications of survey questions and guidelines and already established (published) indicators for assessing specific topics around PP were consulted53-64. The chosen PP indicators assess standard requirements for PP which are in line with the official licensing requirements in the RoM.
For the community and hospital pharmacists, cross-sectional descriptive surveys were conducted where combined pre-coded open ended and multiple choice closed questions were used with type of response format: A Activity fully applied; B Activity partially applied; C Activity not applied (applicable); D
-assessment tool for quantification of PP status and quality of PSs that can facilitate comparison of results over time within and between the community and hospital pharmacies. When calculating the GPP and PSs score, the maximum score of 100 (20 per section) and minimum zero for both community and hospital pharmacies were given for all the indicators (155 for community and 191 for hospital pharmacies, respectively) if all indicators were responded to A and D, respectively. The weight of each indicator in the section depended on the number of the indicators in the section and if all responded to A, it was calculated by dividing 20 with the number of indicators. For example, if the total sum of indicators per section I is 40 and each indicator responds to A, the weight of each indicator would be 0.500 (= 20/40). The weight of the indicators responded to C was calculated as a half of the weight of the indicator responded to A (in the given example, it would be 0,500/2 = 0.250), while the weight of each indicator responded to B was calculated by dividing the sum of the weights of the indicators responded to A and C by 2 (i.e. (0.500 + 0.250)/2 = 0.375). Thus, in the given example if all the indicators were responded to B, the total score would be 15 per section and 10 per section if the answers to all questions were C.
The questionnaires were previously tested by involving the target groups/stakeholders (actual respondents) in the design to evaluate the specific questions, format, questions sequences and instructions. During the pilot study, the measurability of the questions, interpretation of the questions by all respondents, whether close-ended questions have a response which applies to all respondents, clarity and understandability of the questions, length of the questions, time for completing and responses from the different response categories, etc., were evaluated. Considering that for almost all indicators a professional background was required to undertake the necessary assessment, both the surveyors and respondents were pharmacists.
The manual data collection sheet ensured independent data collection on site of all data required. The sheet contained data collection space for all indicators in the form of structured information. The data were saved by Excel software. Excel-based assessment tool depicts the findings in the form of a histogram and a spidograph of all components calculated for each pharmacy settings.
Results
I Community pharmacy practice and services
I.1. Demographic characteristics and management of community pharmacies
According to the data obtained with the survey, only 8.43% of the community pharmacists are state or local governance, while independent (owned by the pharmacist itself) and owned by two or more pharmacists (partnership of pharmacists) are 24.1% and 15.61%, respectively. Most of the respondents belong to corporate body owning more than 1 pharmacy (part of pharmacy chain), 53.3%. There is not a single community pharmacy with an international ownership or ownership of non-profit making institution (Fig. 3). 2,41 6,02 24,1 15,61 53,3 0 0 60 state governence local governence indipendant partnership coorporate body international ownership
Fig. 3. Ownership/institutions responsible for establishing community pharmacy
3,05 7,83 72,3 1,2 16,3 0 80 rural suburban city out of town health centre
Most of the pharmacies (72.3%) are located in the cities, especially in the centers of the cities. Only 7.83% of the community pharmacies are located in suburban areas, while very few (3.05%) are placed in rural areas. Within or near the health centers, there are 16.3% (Fig. 4) of community pharmacists, which indicates inadequate distribution of the community pharmacies for providing PSs for the patients. The categories that best describe the number of citizens currently served and the number of patients served by the community pharmacy is presented in Fig. 5.
3,01 6,63 12,7 10,8 31,3 27,1 24,7 16,3 14 21,7 13,3 17,5 0 35 up to 500 500-1000 1000-3000 3000-5000 5000-10 000 over 10 000 citizens served patients served
Fig. 5. The number of citizens and patients served in/by the community pharmacy
21,2 38,6 24,1 15,1 0 40 up to 2000 2000-3000 3000-5000 over 5000
Fig. 6. The number of prescriptions dispensed per month in the community pharmacy
Considering the category of patients currently served by the community pharmacies, 31.3% of them dispense medicines for 1000-3000 patients and 24.7% serve 3000-5000 patients. Approximately similar percentage (12.7%, 14.0% and 13.3%) of the pharmacies dispense medicines to 500 - 1000; 5000 - 10
month. Comparing the number of citizens and patients served in the community pharmacies, it is obvious that the number of citizens and number of patients go along for the pharmacies that have 1000-3000 citizens/patients. It is interested to note that the community pharmacies serving higher number of citizens, serve lower number of patients.
Considering the number of prescriptions dispensed by the community pharmacy per month (reimbursed or not by the HIF), most of the pharmacies (38.6) dispense up to 3000 prescriptions. Similar number of pharmacies dispenses medicines for up to 3000 or 5000 prescriptions (21.2% and 24.1%, respectively). Only 15.1% of the community pharmacies dispense over 5000 prescriptions and only 1.2% dispenses more than 6000 prescription (Fig. 6).
One of the parameters for evaluating the structure of the community pharmacy was the total size of the pharmacy floor. In only 3.01% of the community pharmacies, the total size of the floor is less than 25m2, while the community pharmacies with total floor size over 100m2 are 7.23%. Most of the community pharmacies (45.2%) are with floor size from 25-45m2and 26.5% have the size of 45-65m2(Fig. 7). Almost all of the community pharmacies (95.8%) are open 12 h/day, six days per week, and approximately 70% of the pharmacies are open for providing services on Sunday and holidays (67.5% and 76.5%, respectively). Only 10.8% of the community pharmacies provide on call services during the whole week. All the community pharmacies have installed a computer system. However, in 39.2% of them it is used as connection to other pharmacies (usually in chain pharmacies) and only 14.5% of the pharmacies use the computer system for gathering information from the NDIC.
3,01 45,2 26,5 17,5 7,23 0 10 20 30 40 50 up to 25m2 25-45m2 45-65m2 65-100m2 over 100m2
Fig. 7. Total size of the pharmacy floor
Considering the staff employed in the community pharmacies, the point of interest was the number of full-time or part-time employed with the degree graduated pharmacist or master in pharmacy, but also stuff with a health specialization (2nd cycle according to Bologna, see the Introduction). Almost all community pharmacies are equipped with 1-2 technicians and 1-2 pharmacists as full-time employed, with 1 responsible (licensed) pharmacist. There are no pharmacists with specialist competences such as competence in community pharmacy (due to lack of specialized education in this area), clinical pharmacy, pharmacoinformatics, regulatory affairs, nutrition, etc. Full-time employed cleaning personal is 0.38/pharmacy and administrative stuff 0.03/pharmacy (accounting personal). There are no part-time employed pharmacists, pharmacy technicians or administrative staff in the community pharmacies in
community pharmacies have specialists in certain field of medicine and pharmacy, mostly the specialists in pharmaceutical technology.
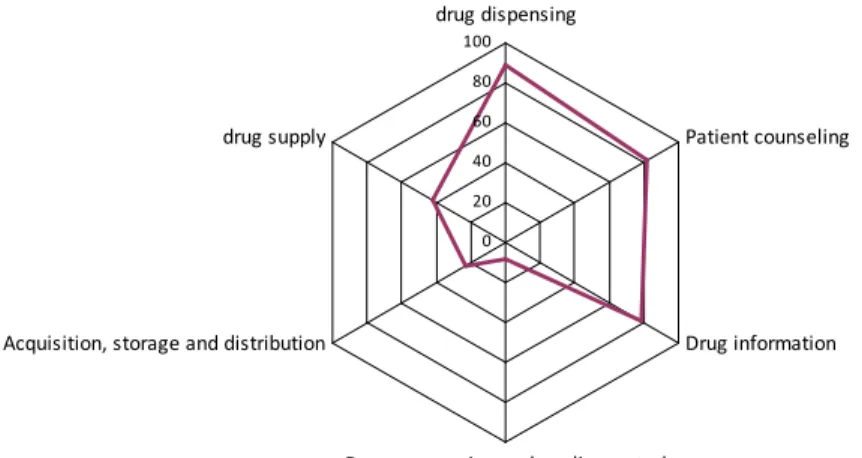
The pharmacists are involved in all activities in the community pharmacy, administrative and traditional activities (drug supply and dispensing) as well as activities related to pharmaceutical care services (patient counseling and education, giving information on medicines and medical devices, etc.) Considering the pharmacy technicians, they are mostly involved in drug dispensing (89.2%), patients counseling (81.9%) and giving drug information (78.9%). Around 42.2% of the employed pharmacy technicians are involved in drug supply and 23.5% are involved drug and medical devices acquisition, storage and distribution. Only 8.43% are engaged in drug preparation. These data are logical consequence of the actual situation regarding employment in the community pharmacies where usually 1 pharmacist and 1 pharmacy technician are employed (Fig. 8).
0 20 40 60 80 100 drug dispensing Patient counseling Drug information
Drug preparation and quality control Acquisition, storage and distribution
drug supply
Fig. 8. Tasks assigned to pharmacy technicians in the community pharmacy
Considering purchasing of medicines and medical devices, the survey showed that wholesalers are the main source for acquisition of drugs followed by industry (Fig. 9). Only 3.61% of the community pharmacies have their own production and only 4.22% purchase drugs from other community pharmacies. Most of the community pharmacies purchase medications daily (77.1%), 17.5% twice a week and only 1.2% purchase medications weekly. There is no community pharmacy that supplies medicines monthly.
6,02 98,2 3,61 4,22 3,01 0 100 industry wholesalers own production other pharmacies group purcharing
Fig. 9. Sources for purchasing of medicines and medical devices by the community pharmacy The types of pharmaceutical (care) services provided on an around-the-clock basis in the community pharmacies are presented in Table 3. In only half of the community pharmacies (53.61%), medicines use is reviewed. In addition, blood pressure is measured in 22.29% of the community pharmacies; hypertension is managed in 19.28%, while diabetes and asthma management is offered in 16.27% of the community pharmacies. Other services are offered in very low number of community pharmacies, there are pharmacies where no additional services other than (repeat) dispensing prescriptions are offered and some of them declared that the structure of the pharmacy does not provide minimum conditions for offering pharmaceutical care services.
Table 3. The pharmacy services provided in the community pharmacy The services provided in and by the community pharmacy %
Dispensing prescription 93.98
Repeat dispensing 88.55
Medicines use review 53.61
Disposal of medicines’ waste 40.36
Blood pressure measurement 22.29
Hypertension management 19.28 Glucose measurement 17.47 Diabetes management 16.27 Asthma management 16.27 Pregnancy test 11.45 Weight measurement 5.42 Smoking cessation 3.01 Cholesterol measurement 1.20
Home care services 1.20
Night services 1.20
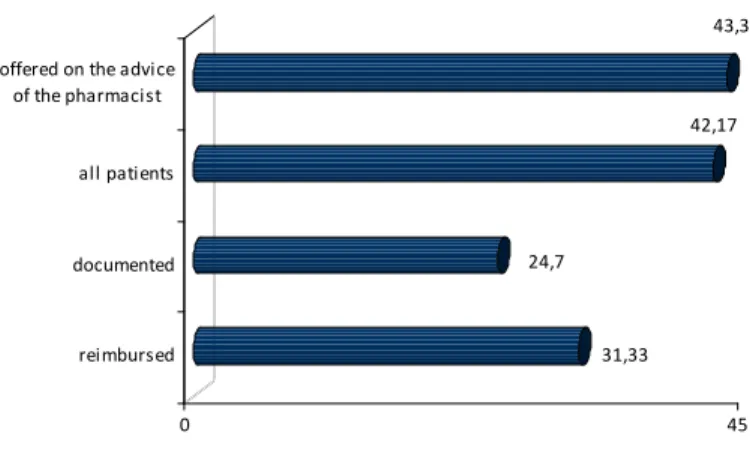
According to the data from the survey, the patients obtain information on the services provided in the pharmacy in 72.89% of the community pharmacies. These services are offered regularly in 63.86% of the pharmacies, for all patient groups in 42.17%, but in only 24.70% of the community pharmacies, the pharmacists document the pharmaceutical services they provide. In addition, only dispensing of prescription is reimbursed by the HIF, so 31.33% of the respondents claimed that services are reimbursed (Fig. 10). 31,33 24,7 42,17 43,37 0 45 reimbursed documented all patients offered on the advice of the pharmacist
Fig. 10. Information on the services provided in/by the community pharmacy
Considering the data obtained for the reimbursement of medicines, one can see that the most of the community pharmacies (95.18%) have a contract with the HIF and almost all of them (96.78%) have fulfilled all the provisions from the contracts with the HIF. The reimbursement is sufficient to satisfy the patient needs for medicines in only 63.05% of the community pharmacies, although the reimbursed medicines are available in the pharmacy each and every day in 83.73% of the community pharmacies. The evidence for reimbursed medicines is kept separately from the evidence for other medicinal products, readily available for inspection in almost all of the community pharmacies (93.98%). The received prescriptions are printed on paper in standardized form in 93.37% of the community pharmacies, in app. 1.21% they are e-prescriptions and in 5.42% they are handwritten in standardized form. The medicines without co-payment are first offered to the patients in 81.33% of the community pharmacies (Fig. 11)
The survey also gives data for the management characteristics of the community pharmacies in the RoM. The pharmacies are managed both (internally and externally) in 53.0% of the community pharmacies, but dominantly internally (in 43.4%), while the pharmacy managers respond to the pharmacy owners in app. 64.5% of the community pharmacies. In app. 92% of the community pharmacies, the pharmacy manager is qualified pharmacist. In 73% of the pharmacies, the responsible pharmacist is not the owner of the pharmacy and he/she responds to the pharmacy manager.
According to the information gathered during the survey, the pharmacists in the community pharmacies are in a phase of preparation of written SOPs. Up-to-date policies and SOPs established so far and the proportion of community pharmacies incorporating these standards are given below (Table 4).
7,23 93,98 81,33 83,73 62,05 0 100 e-prescription separate evidence medicines without co-payment availability sufficient budget
Fig. 11. Budgeting and reimbursement of medicines
Table 4. Up-to-date policies and SOPs established in the community pharmacies in the RoM
SOPs Community pharmacies (%)
Supplies, storage and delivery of products Product acquisition, storage and handling Fire safety
Management of disposal of expired stock Pest control Complain handling Cash management Hygiene procedures Medicines recall Documentation
Personnel education and training and competency evaluation Reporting adverse drug reactions
Key holding Personnel access Incident management
Use and maintenance of facilities and equipment Contingency in the event no pharmacy is present Monitoring environmental conditions
Products requiring specialized handling Labelling Movement of materials Compounding medicines Quality control Process validation 66.3 64.5 62.6 61.4 57.2 56.6 56.6 56.0 53.1 47.6 45.2 45.0 44.5 43.9 38.5 35.5 33.7 26.5 24.1 16.9 10.8 9.64 8.4 7.83