“survivor.” It will be difficult to rename all
inno-vations and established procedures for which the
question “does this work?” has not been answered,
“research projects.” However, the word “new”
should always be preceded by “experimental,”
be-cause “new” often implies “improved.” We need a
less negative word than “negative” to summarize
the findings of “negative” trials and a better way of
describing randomization than “random.”
We speak of “subjecting” interventions to a
ran-domized trial as if it were a cruel and unusual
punishment. It may be that for the trial
organiz-ens-no one ever made any friends by carrying out
a controlled trial-but for the innovation it should
be, and perhaps one day will be, the standard
pro-cedure. Identifying the stumbling blocks is another
step on that path.
REFERENCES
JUDITH LUMLEY, MA, MBBS, PHD Department of Paediatnics
Monash University
Queen Victoria Medical Centre
Melbourne
1. McKinlay JB: From ‘promising report’ to ‘standard proce-dure’: Seven stages in the career of a medical innovation.
Milbank Mem Fund Q 1981;59:374-411
2. Avery ME, Chernik V: On decision making surrounding
drug therapy: A continuing dilemma. N Engi J Med
1977;296:102-103
3. Sacks HS, Chalmers TC, Smith H: Sensitivity and specific-ity of clinical trials: Randomized v historical controls. Arch
Intern Med 1983;143:753-755
4. Wald NJ: Neural-tube defects and vitamins: The need for a randomized clinical trial. Br J Obstet Gynoecol 1984;91:516-523
5. Hobbins JC, Freeman R, Queenan JT: The fetal monitoring debate. Pediatrics 1979;63:942-951
6. Lumley J, Lester A, Renou P, et al: A failed RCT to determine the best method of delivery for very low birth weight infants. Controlled Clin Trials 1985;6:120-127
7. Anonymous: Consent: How informed. Lancet
1984;1:1445-1447
8. Hendricks, CH: The case for nonintervention in preterm labor, in Elder MG, Hendricks CH (ads): Preterm Labor.
London, Butterworths, 1981, pp 93-123
9. Renou P, Chang A, Anderson I, et al: Controlled trial of fetal intensive care. Am J Obstet Gynecol 1976;126:470-476 10. Lumley J, Lester A, Anderson I, et al: A randomized trial of
weekly antenatal cardiotocography in high-risk obstetric patients. Br J Obstet Gynaecol 1983;90:1018-1026
11. Detsky AS, Sackett DL: When was a clinical trial big enough? How many patients you needed depends on what you found. Arch Intern Med 1985;145:709-712
12. Rose M, Leibenluft RF: Antitrust implications of medical technology assessment. N Engi J Med 1986;314:1490-1493
13. Feinstein AR: The ‘chagrin factor’ and qualitative decision analysis. Arch Intern Med 1985;145:314-317
14. Hadders-Aigra H, Touwen B, Huisjes HJ: Follow-up of children exposed to ritodrine. Br J Obstet Gynaecol
1986;93:156-161
15. Lesko SM, Mitchell AA, Epstein MF, et al: Heparin use as a risk factor for intraventricular hemorrhage in low-birth-weight infants. N Engi J Med 1986;314:1156-1160
16. Astbury J, Yu V: Determinants ofstress for staff in neonatal intensive care units. Arch Dis Child 1982;57:108-111
Neonatal
Neurosonography
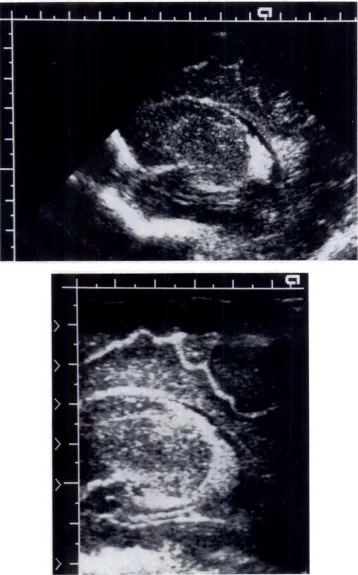
By this time, we should expect that the ultrasonic
diagnosis of peniventnicular hemorrhage should be
definitive with demonstration of an echodense
patch in an ependymal region that deforms the
adjacent ventricular contour in its early stages (Fig
1). The combined experience with transfontanel
viewing, which has spanned some four generations
of ultrasonic equipment, convincingly
demon-strates that the selection and operation of an
in-strument can have a profound effect on the
diag-nosis of acute neonatal intracranial pathology.
Visualizing intracranial hemorrhage is primarily a contrast or “gray scale” resolution task, not a
matter of spatial or detail resolution. That is, the
hemorrhage must stand out as different in some
way from the surrounding parenchyma. In the low
megahertz range, subependymal and panenchymal
hemorrhages are more reflective than “normal”
cor-tex or subcortical gray matter. That contrast
gra-dient is affected by biologic factors including the
size of the hemorrhage, local water content, and,
probably, tissue perfusion. Several instrument
fac-tons are equally important, principally the spectral
frequency composition and spatial configuration of
the pulse at its interaction depth. The final image
is a combination of interdependent tissue and
im-aging system variables. If the contrast gradient is
too low on “noise” too high, an area of hemorrhage
will be indistinguishable from the surrounding
tis-sue. Conversely, germinal matrix tissue is itself
echodense (Fig 2) and may be misinterpreted as
hemorrhage if the gradient is intensified by the gray
scale manipulation. Likewise, focal hemorrhages
are less often recognized by ultrasound in
cenebel-lum than their incidence’ because high background
reflectivity obscures detection. Organizational
changes within germinal matrix on other
hemon-nhage can be observed (Fig 3). Distinction of bloody
and clean CSF is another contrast-dependent task
(Fig 4).
Another concern are “side lobe” artifacts2 by
which a strong reflector in one part of the field is
Fig 1. Small hemorrhage occupying “thalamocaudate notch” in this parasagittal view. Note contrast or gray scale differences within image. This image was obtained with a large aperture, dynamically focused instrument operated at 5 MHz, 57-mm aperture, with 40 dB logarith-mic preprocessing and near linear gray scale assignment. Four or more image frames are integrated per view. Large scale divisions represent 10 mm.
Fig 2. Germinal matrix (arrows) is echodense. Cingu-late sulcus is shallow, barely visible. (Gestational age 24.7 weeks.)
also portrayed along an arc extending from its true
position. Side lobe levels are relatively high in many
of the mechanical sector-scanning units applied for
newborn cranial studies. Ghost images from chonoid
glomus side lobes are superimposed upon brain
Fig 3. Magnified coronal view. Discrete, 1-mm cysts herald resolution of subependymal hemorrhage. Cingu-late sulcus is at top of field and penetrates about 7#{189}mm on either side of interhemispheric fissure (30.4 weeks’ gestational age).
Fig 4. Coronal section of distended ventricles at level of foramena of Monro is photographically underexposed to accentuate reflectivity of blood. CSF is anechoic (echo free). Similar degree of reflectivity is found in endome-trioma, hematobilia, and hemorrhagic cysts elsewhere in
body at same examination frequency and transducer
ap-erture. There is organized clot along posterolateral wall of right lateral ventricle.
above a lateral ventricular margin, in a sagittal view, where they can be misinterpreted as an
Fig 5. Echodense patch appears opposite choroid glomus, apparently in supraventricular cortex in sector image (top). This “side lobe” artifact does not appear in higher resolution linear format view (bottom).
damage. This particular artifact is dependent upon
transducer design and operation; it is minimal for
dynamically focused phased linear array devices
(Fig 5).
Cortical reflectivity of the normal infant brain is
reasonably uniform (Fig 6). Asphyxial injury may
be recognized in an early stage of evolution as
Fig 6. Magnified view of parietal cortex. Sulci appear white. Parenchymal reflectivity is generally uniform.
Fig 7. Echodense patches at lateral margins of both lateral ventricles, left larger than right. Parenchymal reflectivity is also “coarse.” This asphyxial injury in-curred neuromotor sequelae.
gle-element transducer systems have an optimal
performance depth, limiting the general definition
of brain anatomy and pathology. As another
con-trast effect, hypoechoic rims develop around the
major sulci late in the third trimester (Fig 8) and
may represent myelination or a vascular gray-white
differentiation preceding myelination. There are
also changes in flow profiles in the anterior cerebral
artery circuit that accompany edema, induced by
asphyxia, that can be evaluated with simultaneous
pulsed Doppler sensing (Fig 9). In smaller infants,
the profiles are influenced by patent ductus and by
pulmonary hypertension. Recognition of these
ef-fects and duplex technology extend the pioneering
Fig 8. Hypoechoic rims surround sulci. This is a
devel-opmental milestone (also see Fig 1).
and, when more severe, as a nodular echodensity
(Fig 7). These patches are most often localized
within the motor strip, and their occurrence can be
correlated with outcome: unilateral, anterior foci
result in neurologic deficits limited to a hand on
arm, whereas bilateral, lower lesions are associated
with more typical, spastic diplegia. These are also
contrast gradient tasks that require high signal to
noise performance, and they are dependent upon
beam focal characteristics. Array systems can be
focused dynamically at several depths, whereas
approach of Bada and others3 using continuous wave Doppler devices.
Although it is correct to infer that most
echo-dense peniventrcular patches are hemorrhages, a
range of microscopic pathologic conditions
(includ-ing inflammation) will result in the same ultrasonic
appearance. We suggest that reporting be
descnip-tive, rather than interpretive, although some
at-tempt to assign a prognostic risk level is appropriate
for the clinical management process. We propose
also that pertinent instrument-operating features
should be explicit in scientific papers so that those
findings can be referred to individual practice
ap-plication (see Fig 1).
The ultrasonic image is a limited representation
of some features of tissue. Instrument factors
af-fecting image appearance can vary from institution
to institution depending jointly upon instrument
selection and use, and this will continue to
con-found comparative clinical investigation until the
method is itself better understood and operational
standardization is established in practice. Nonethe-less, there remains considerable scope for
technol-ogic advancement of ultrasound imaging for fetal
and neonatal neunosonography. The new
genera-tion of equipment4 and their successors should
per-mit a greater appreciation of dynamic anatomy of
the developing brain and help to structure
investi-gations of the pathophysiology, epidemiology, and
natural history of peniventnicular hemorrhage,
pa-renchymal edema, and other acquired peninatal and
neonatal insults.
ELAINE E. FARRELL, MD, FAAP
Evanston Hospital and
Northwestern University Medical School
Evanston, IL
JASON C. BIRNHOLZ, MD, FACR, FACOG
Rush-Presbyterian-St Luke’s Medical
Center and Rush Medical College
Chicago, IL
REFERENCES
1. Rorke LB: Pathology of Perinatal Brain Injury. New York, Raven Press, 1982, pp 37-44
2. Birnholz JC: Newborn cerebellar size. Pediatrics
1982;70:284-287
3. Bada HS, Haggar W, Chua C, et al: Noninvasive diagnosis of neonatal asphyxia and intraventricular hemorrhage by
Doppler ultrasound. J Pediatr 1979;95:775-779
4. Birnholz JC: Evolution ofthe ultrasonic examination. J GUn Ultrasound 1985;13:83-85
Screening
Infants
for
Neuroblastoma
in North
America
Since the first report of chemotherapy-induced
complete remission in childhood leukemia,’ medical
science has waged a global biologic wan against
cancer-a wan fought with nuclear energy, cellular toxins, and conventional arms such as surgery.
Many battles have been won, most notably in the
Children’s Crusade, but despite new attack weapons
developed by the strategists, the battle against the
arch enemy, disseminated neunoblastoma, has
con-tinued to yield a somber casualty list and few
sun-vivors among children olden than 12 months at
diagnosis. Despite the losses, we have leaned a lot
about the nature of this enemy. It is bizarre,
malig-nant, and so capricious that it may even retreat
without a fight, fall quickly under the sword, on resist for a time only to return in a sneak attack to kill its young victim.
In 1973, our allies in Kyoto, Japan,2’3 organized
a strategic defense plan aimed at the prevention of
this carnage of young children by catching the
enemy at its early preparations and foiling its plans
with but a minor skirmish-the “dove” approach to
the war on neuroblastoma. This strategy appeared
so successful that, in 1981, seven other centers
joined Sawada and his colleagues4 in Kyoto to
or-ganize the Mass Screening Study Group For
Neu-roblastoma under the aegis of the Japanese
govern-ment.
Woods and Tuchman5 have given us the
chal-lenge to join this strategic defense plan. They have
summarized the reports of the Japanese experience
with mass screening, pointing out the pitfalls of
using vanillylmandelic acid determination alone,
highlighting the cost effectiveness of preclinical
diagnosis, and speculating on the potential for a
bioscientific windfall as a bonus of the plan.
The Japanese have demonstrated that this
bio-logic strategic defense is effective. In their most
recent report,6 they have summarized the outcome
of the 25 cases detected through screening almost
half a million infants. Twenty-three ofthese infants
were disease free at a median follow-up of 39 months-a fantastic achievement!
Woods and Tuchman5 have given us all the
com-pelling reasons to embank on such a program in
North America. Who should we screen? If we