Refereed paper
Incidence of potential drug interactions in a
transplant centre setting and relevance of
electronic alerts for clinical practice support
Piera Polidori
Clinical Pharmacy Department, ISMETT, Palermo, Italy
Concetta Di Giorgio
School of Specialisation in Hospital Pharmacy, University of Palermo, Palermo, Italy
Alessio Provenzani
Clinical Pharmacy Department, ISMETT, Palermo, Italy
ABSTRACT
Background Adverse drug events may occur as a result of drug–drug interactions (DDIs). Infor-mation technology (IT) systems can be an import-ant decision-making tool for healthcare workers to identify DDIs.
Objective The aim of the study is to analyse drug prescriptions in our main hospital units, in order to measure the incidence and severity of potential DDIs. The utility of clinical decision-support sys-tems (CDSSs) and computerised physician order entry (CPOE) in term of alerts adherence was also assessed. DDIs were assessed using a Micromedex1
healthcare series database.
Methods The system, adopted by the hospital, generates alerts for prescriptions with negative interactions and thanks to an ’acknowledgement function’ it is possible to verify physician adherence to alerts. This function, although used previously, became mandatory from September 2010. Phys-ician adherence to alerts and mean monthly inci-dence of potential DDIs in analysed units, before and after the mandatory ‘acknowledgement func-tion’, were calculated.
Results The intensive care unit (ICU) registered the greatest incidence of potential DDIs (49.0%),
followed by the abdominal surgery unit and dialysis (43.4 and 42.0%, respectively). The cardiothoracic surgery unit (41.6%), step-down unit (38.3%) and post-anaesthesia care unit (30.0%) were compar-able. The operating theatre and endoscopy regis-tered the fewest potential DDIs (28.2 and 22.7%, respectively). Adherence to alerts after the ‘acknow-ledgement function’ increased by 25.0% in the ICU, 54.0% in the cardiothoracic surgery unit, 52.5% in the abdominal surgery unit, 58.0% in the step-down unit, 67.0% in dialysis, 51.0% in endoscopy and 48.0% in the post-anaesthesia care unit. In the operating theatre, adherence to alerts decreased from 34.0 to 30.0%. The incidence of potential DDIs after mandatory use of the ’acknowledgement function’ decreased slightly in endoscopy (–2.9%), the abdominal surgery unit (–2.7%), dialysis (–1.9%) and the step-down unit (–1.4%).
Conclusions Improving DDI alerts will improved patient safety by more appropriately alerting clin-icians.
Introduction
Drug–drug interactions (DDIs) are a complex clinical problem that should draw the attention of all health-care workers, especially physicians and pharmacists directly involved in choosing the right therapy for patients. Adverse drug events (ADEs) may occur as a result of potential DDIs (p-DDIs). Oftentimes they are predictable and preventable.1,2These adverse events result in increased rates of hospitalisation, increased lengths of stay, and contribute to patient morbidity and mortality.1,3,4Several factors can complicate the possibility of identifying and managing p-DDIs. For example, the use of polypharmacy, particularly com-mon acom-mong older adults, increases the risk of having adverse drug reactions and/or interactions.5A study of 4431 hospitalisations revealed an average of six drugs per patient.6Another study, on 907 patients, revealed an average of 9.6 drugs per patient.7The more associ-ations there are among different drugs, the greater the chance that their safety profiles will be lowered.8–10 Other factors, such as gender, age, genetics, comor-bidities, and state of health are also linked to the risk of DDIs.11,12
The most vulnerable patients are those with chronic diseases that require long-term multitherapy; patients with liver or kidney failure who are using drugs included in the group at risk of interaction, and geriatric and paediatric patients, whose metabolic activity is significantly related to age.13–19To ensure safe therapy for these patients, appropriate drug prescription is required. In the age of information technology (IT) systems, the use of electronic health records and computerised physician order entry (CPOE) can be an efficacy tool to promote patient safety.20–21Clinical decision-support systems (CDSSs) are an additional component of CPOE systems that can be utilised and have been defined as ‘computer software employing a knowledgebase designed for use by a clinician involved in patient care, as a direct aid to clinical decision making’.22CDSSs added to CPOE systems guide prescribers on appropriate dosing and alert them to duplicate therapies, drug allergies and DDIs.23So
patient safety, quality and efficiency of care can be improved.24
Although CDSSs provide several benefits, there are also limitations as a result of which p-DDI alerts receive no response from physicians.25–28 Unclear clinical significance, alert fatigue and database rating inconsistencies can, at times, lead to low p-DDI alert acceptance by prescribers.1
The goal of this study was to analyse drug prescrip-tions in our main hospital units, in order to measure the incidence and severity of p-DDIs. In addition, the utility of CDSS and CPOE in terms of alerts adherence was assessed.
Method
This retrospective observational study was carried out at ISMETT, a 90-bed transplant hospital in Palermo, Italy. All prescriptions in the intensive care unit (ICU), step-down unit (SDU), cardiothoracic surgery unit (CSU), abdominal surgery unit (ASU), dialysis, en-doscopy, operating theatre (OT) and post-anaesthesia care unit (PACU), from June 2010 to December 2010, were analysed for p-DDIs. All interactions were assessed using the Micromedex1Healthcare Series
database, and severity of p-DDI was analysed accord-ing to the decisional support system classification (Table 1) in the Sunrise1Eclipsys electronic medical record.
The mean incidence of p-DDIs for each unit was calculated. The value was obtained by dividing the mean number of p-DDIs for each unit by the mean number of drug prescriptions in that unit for each period of evaluation.
The program developed and adopted by our hos-pital allows physicians to obtain helpful information on drug prescriptions. It also generates alerts in case of active agents with negative interactions. It is possible to verify adherence to p-DDI alerts through the elec-tronic medical record. This verification was made
What is known
. Alerts can improve the quality and safety of physician prescriptions.
. The literature has reported that many alerts are frequently cancelled and ignored.
. Alerts can aid to prevent potential drug–drug interactions (p-DDIs) and possible related adverse reactions.
What this paper adds
. ‘Acknowledgement function’ mandatory use has demonstrated greater adherence to warning systems. . It is necessary to program software to reduce alert fatigue highlighting only severe alerts.
. In our setting, most p-DDIs are referred to few drugs and this knowledge facilitates their management in
possible thanks to an ‘acknowledgement function’, which carries the electronic signature of the physician (statement read yes/no) indicating his or her acknow-ledgement of the interactions. Statement read ‘yes’ means the physician displayed and read the alert and is aware that the combination drug choice is potentially harmful for the patient. This function, in the first period of study, was not required, so physicians could proceed with the prescription without responding to any alert. Beginning in September 2010, the ‘acknow-ledgement function’ became mandatory, prompting physicians to consider the alert. ‘Acknowledgement function’ can aid physicians to choose, when possible, a therapeutic alternative. For each unit, the adherence to alerts on the part of physicians and the incidence of p-DDIs, before and after introduction of the ‘acknow-ledgement function’, were compared to verify the function suitability as a strategy for improving quality of the process.
A pivot table was used as an analytical and reporting instrument in which the available data were processed by type of drug, unit and number of p-DDIs, and physician adherence to the alerts.
Results
The ICU registered a mean of 1053 p-DDIs for a mean of 2152 prescriptions per month (49.0%), followed by ASU and dialysis with an average of 604 and 15.6 p-DDIs, respectively, for a mean of 1390 and 37 pre-scriptions (43.4 and 42.0%, respectively). CSU regis-tered a mean of 520 p-DDIs for a mean of 1248 prescriptions monthly (41.6%), SDU registered a mean of 596 p-DDIs for a mean of 1555 prescriptions
monthly (38.3%) and PACU registered a mean of 99 p-DDIs for a mean of 332 prescriptions per month (30.0%).
OT and endoscopy, the smallest units, registered a mean of 166 p-DDIs for a mean of 588 prescriptions monthly (28.2%), and 8.8 p-DDIs for a mean of 39 prescriptions monthly (22.6%), respectively. Overall analysis of prescriptions identified the top five drugs responsible for p-DDIs in the main units in our hospital: furosemide (1768 p-DDIs), tacrolimus (1496 p-DDIs), omeprazole (801 p-DDIs), sodium-fructose-1.6-diphosphate (428 p-DDIs) and warfarin (395 p-DDIs). Although these interactions are known in the literature, the subject is so vast and growing both for mechanisms that determine p-DDIs and appearance on the market of new drugs, that remem-bering their importance is never enough.
In the first period of study (June 2010 to August 2010) adherence to alerts was 70.0% in the ICU, 41.0% in the CSU, 43.0% in the ASU, 36.0% in the SDU, 29.0% in dialysis, 10.0% in endoscopy and 42.0% in the PACU. From September 2010 to December 2010, after introduction of the mandatory reading of alerts for physicians, a marked improvement was found: 95.0% in the ICU, 95.0% in the CSU, 95.5% in the ASU, 94.0% in the SDU, 96.0% in dialysis, 61.0% in endoscopy and 90% in the PACU. In OT adherence to alerts decreased from 34.0 to 30.0%. A positive trend was observed (reduction of p-DDIs) in four units, which might be due to the greater adherence to warning systems. The better results were in endoscopy and ASU with a reduction of 2.9 and 2.7%, respectively, fol-lowed by dialysis and SDU with a reduction of 1.9 and 1.4%, respectively (Table 2).
Considering the total number of drug prescriptions (51 393) in the study period (seven months), the total number of p-DDIs was 21 447, or 41.7%.
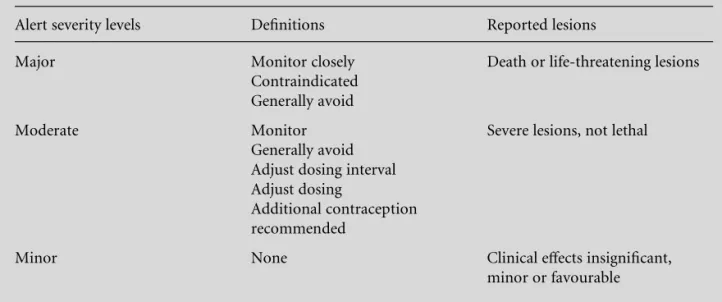
Table 1 Multum drug database of alert severity levels
Alert severity levels Definitions Reported lesions Major Monitor closely
Contraindicated Generally avoid
Death or life-threatening lesions
Moderate Monitor Generally avoid Adjust dosing interval Adjust dosing
Additional contraception recommended
Severe lesions, not lethal
Discussion
Principal findings
DDIs are a complex and controversial part of phar-macology. Our study showed that almost 42.0% of drugs prescribed in the analysed period and in the units reviewed interacted with other drugs prescribed for therapy. This may be because many of our patients are seriously ill and require multidrug therapies. Of the eight units evaluated, the ICU registered the greatest number of p-DDIs, followed by ASU and dialysis. CSU, SDU and PACU are comparable with the larger units in terms of number and type of interactions, whereas OT and endoscopy registered the fewest p-DDIs.
Another important result that emerged from the data was the increasing adherence on the part of physicians to the software alerts. More specifically, ASU, SDU and dialysis are among the units where there is more adherence. Effectively, in these units, there was a decrease, although low, in the incidence of p-DDIs from 42 to 39%. The exception was the OT in which adherence is very low. It was assumed that this may be due to unforeseen emergency situations that often occur. It is right, also, to remember that in the OT there is always an anaesthetist present to carefully monitor the patient. This study has identified the five drugs more involved in p-DDIs in our hospital, this could be a starting point for all healthcare workers responsible for medication safety.
It is hard to predict the clinical impact of p-DDIs. As a result, the rational and appropriate use of multi-drug therapies is a key factor of prevention. Often
p-DDIs cannot be avoided because of the need to use drugs in combination, especially when there are no therapeutic alternatives. This limitation is mitigated by constant patient monitoring of vital signs and drug blood levels. Despite a small reduction in p-DDIs, implementing computerised alerts can be an effective way of supporting clinical decision making, allowing clinicians to see all possible p-DDIs and evaluate their impact in terms of potential risks and benefits. Introducing alerts does not replace physician assess-ment: patients cannot be deprived of therapies based solely on the risk of interactions, but all alternatives must be taken into account. In conclusion, it is import-ant to make alerts as effective as possible. In this context new technologies can aid physicians and improve pre-scribing safety. However, there is yet the need to determine the most effective way to deliver alerts in order to eliminate possible unnecessary alerts.
Implications for practice
Although a slight decrease in the incidence of p-DDIs was observed, development of the ‘acknowledgement function’ has increased physician adherence to alerts. This is an important starting point for advanced forms of CDSSs that should support the physician in identifying important p-DDIs without generating clinically irrelevant alerts.
Comparisons with the literature
As widely addressed by Vaziriet al,29the prescribing alert systems used in primary care practice often have
Table 2 Incidence of potential DDIs before and after introducing the ‘acknowledgement function’
June/July/August interactions (%)
September/October/ November/December interactions (%)
~(%)
ICU 47.0 50.4 3.4
SDU 39.2 37.8 –1.4
CTU 41.0 42.4 1.4
ASU 45.0 42.3 –2.7
OT 27.2 28.7 1.5
PACU 27.1 31.9 4.8
low specificity and low utility. In fact, alerts are often ignored, or viewed uncritically by physicians, who rely on their experience, and on a careful monitoring of patients.30Healthcare IT leaders are working to resolve this important issue to everyone’s benefit, increasingly implementing systems that put out only effective alerts or apply alerting strategies.31
Limitations of the method
Alerts for interaction have a number of important limitations. Checking drug interactions can generate large numbers of clinically insignificant alerts (low severity) that clinicians might ignore. We experienced this at our hospital because too many p-DDIs of low priority were displayed, leading the user to reject the entire application. We urgently need better evidence on which p-DDIs are important. The strength of the alerts should be related to the severity and importance of the interactions, only in this way ‘alert fatigue’ may decrease.31
Calls for further research
CDSSs must support rather than impede, clinical work-flows through speedy, available and usable al-gorithms that provide parsimonious, clear, concise and actionable warnings and advice. A potential solution beyond using alerts in or not in this situation would be continuing to deliver decision support but, when alerting, ask clinicians explicitly whether the patient has an infection that requires treatment for which there is no other good option. Alerts should present the names of the interacting drugs, a brief description of the interaction, optional link to more detailed information and a menu for appropriate actions in response to the alert.
Conclusion
p-DDIs might cause an important amount of harm, which is largely preventable. The main goal for all healthcare workers is to participate in a system that ensures patient safety, and this should include evalu-ation of severe p-DDIs. There is a need for modifi-cation of DDI alerting systems to increase alert acceptance and maximise the benefits of this tech-nology. For this reason, the optimisation of resources by improving DDI alerts through careful and constant monitoring of therapies can ensure safer and more appropriate prescriptions.
ETHICAL APPROVAL
This study was approved by the Institutional Review Board and Ethic Committee of ISMETT.
CONFLICTS OF INTEREST
None.
REFERENCES
1 Smithburger PL, Buckley MS, Bejian S, Burenhei K and Kane-Gill SL. A critical evaluation of clinical decision support for the detection of drug–drug interactions.
Expert Opinion on Drug Safety2011;10:871–82. 2 Bertsche T, Pfaff J, Schiller Pet al.Prevention of adverse
drug reactions in intensive care patients by personal intervention based on an electronic clinical decision support system.Intensive Care Medicine2010;36:665– 72.
3 van Roon EN, Flikweert S, le Comte Met al.Clinical relevance of drug interactions: a structured assessment procedure.Drug Safety2005;28:1131–9.
4 Moura C, Prado N and Acurcio F. Potential drug–drug interactions associated with prolonged stays in the intensive care unit: a retrospective cohort study.Clinical Drug Investigation2011;31:309–16.
5 Anthierens S, Tansens A, Petrovic M and Christiaens T. Qualitative insights into general practitioners views on polypharmacy.BMC Family Practice2010;11:65. 6 Fattinger K, Roos M, Verge`res Pet al.Epidemiology of
drug exposure and adverse drug reactions in two Swiss departments of internal medicine. British Journal of Clinical Pharmacology2000;49:158–67.
7 Zopf Y, Rabe C, Neubert A, Hahn EG and Dormann H. Risk factors associated with adverse drug reactions following hospital admission: a prospective analysis of 907 patients in two German university hospitals.Drug Safety2008;31:789–98.
8 Alaimo A, Provenzani A, Palazzo Uet al.Use of herbal remedies among cancer and transplant patients in the town of Palermo, Sicily. Acta Medica Mediterranea
2010;26(2):61–6.
9 Cupp MJ. Herbal remedies: adverse effects and drug interactions.American Family Physician1999;59:1239– 44.
10 Remirez D, Avila Pe´rez J, Jimenez Lopez G, Jacobo OL and O’Brien PJ. Interactions between herbal remedies and medicinal drugs – considerations about Cuba.Drug Metabolism and Drug Interactions2009;24:183–94. 11 Provenzani A, Notarbartolo M, Labbozzetta M et al.
Unusual high dose of tacrolimus in liver transplant patient, a case report.International Journal of Clinical Pharmacy2012;34:269–71.
12 Provenzani A, Notarbartolo M, Labbozzetta M et al.
Influence of CYP3A5 and ABCB1 gene polymorphisms and other factors on tacrolimus dosing in Caucasian liver and kidney transplant patient.International Journal of Molecular Medicine2011;28:1093–102.
drug–drug interactions in elderly outpatient: a prospec-tive cohort study. Journal of Pharmacy and Pharma-ceutical Sciences2012;15:332–43.
14 Sehn R, Camargo AL, Heineck I and Ferreira MBC. Interac¸o˜es medicamentosas potenciais em prescric¸o˜es de hospitalizados Pacientes.Infarma2003;15(9/10):77– 81.
15 Novaes MRC and Gomes KLG. Estudo de utilizac¸a˜o de medicamentos em Pacientes pedia´tricos.Infarma2006; 18(7/8):18–20.
16 Corsonello A, Pedone C, Corica Fet al.Concealed renal insufficiency and adverse drug reactions in elderly hospitalized patients. Archives of Internal Medicine
2005;165:790–5.
17 George J, Murray M, Byth K and Farrell GC (1995) Differentials of cytochrome P450 proteins in livers from patients with severe chronic liver disease. Hepatology
1995;21:120–8.
18 Adedoyin A, Arns PA, Richards WO, Wilkinson GR and Branch RA. Selective effect of liver disease on the activities of specific metabolizing enzymes: investigation of cytochromes P450 2C19 and 2D6.Clinical Pharma-cology & Therapeutics1998;64:8–17.
19 Franz CC, Egger S, Born C, Ra¨tz Bravo AE and Krahenbuhl S. Potential drug–drug interactions and adverse drug reactions in patients with liver cirrhosis.
European Journal of Clinical Pharmacology2012;68:179– 88.
20 Bates BW. CPOE and clinical decision support in hos-pital.Archives of Internal Medicine2010;70:1583–4. 21 Metzger J, Welebob E, Bates DW, Lipsitz S and Classen
DC. Mixed results in the safety performance of com-puterized physician order entry. Health Affairs2010; 29:655–63.
22 Braden BJ, Corritore C and McNess P. Computerized decision support systems: implications for practice.
Studies in Health Technology and Informatics1997;46: 300–4.
23 Teich JM, Osheroff JA, Pifer EA, Sitting DF, Jenders RA and the CDS Expert Review Panel. Clinical decision support in electronic prescribing: recommendations and an action plan: report of the joint clinical decision support workgroup.JAMA2005;12:365–76.
24 Kuperman GJ, Bobb A, Payne THet al. Medication-related clinical decision support in computerized pro-vider order entry systems: a review. Journal of the American Medical Informatics Association2007;14:29– 40.
25 Van der SIjs H, Aarts J, Vulto A and Berg M. Overriding of drug safety alerts in computerized physician order entry.Journal of the American Medical Informatics As-sociation2006;13:138–47.
26 Seidling HM, Storch CH, Bertsche T et al.Successful strategy to improve the specificity of electronic statin-drug interaction alerts. European Journal of Clinical Pharmacology2009;65:1149–57.
27 Feldstein AC, Smith DH, Parrin N et al. Reducing warfarin medication interactions: an interrupted time series evaluation. Archives of Internal Medicine 2006; 166:1009–15.
28 Lapane KL, Waring ME, Schneider KL, Dube` C and Quilliam BJ. A mixed method study of merits of e-prescribing drug alerts in primary care. Journal of General Internal Medicine2008;23:442–6.
29 Vaziri A, Connor E, Shepherd I, Jones RT, Chan T and de Lusignan S. Are we setting about improving the safety of computerised prescribing in the right way? A workshop report.Informatics in Primary Care2009;17:175–82. 30 van der Sijs H, Aarts J, Vulto A and Berg M. Overriding
of drug safety alerts in computerized physician order entry.Journal of the American Medical Informatics As-sociation2006;13:138–47.
31 Perna G. Clinical alerts that cried wolf. As clinical alerts pose physician workflow problems, healthcare IT leaders look for answers.Healthcare Informatics2012; 29:18, 20.
ADDRESS FOR CORRESPONDENCE
Piera Polidori Via E. Tricomi n. 5 90127 Palermo, Italy Email: [email protected]