Open Access
Review
Malignant hyperthermia
Henry Rosenberg*, Mark Davis, Danielle James, Neil Pollock and
Kathryn Stowell
Address: Department of Medical Education and Clinical Research, Saint Barnabas Medical Center, Livingston, NJ 07039, USA
Email: Henry Rosenberg* - [email protected]; Mark Davis - [email protected]; Danielle James - [email protected]; Neil Pollock - [email protected]; Kathryn Stowell - [email protected]
* Corresponding author
Abstract
Malignant hyperthermia (MH) is a pharmacogenetic disorder of skeletal muscle that presents as a hypermetabolic response to potent volatile anesthetic gases such as halothane, sevoflurane, desflurane and the depolarizing muscle relaxant succinylcholine, and rarely, in humans, to stresses such as vigorous exercise and heat. The incidence of MH reactions ranges from 1:5,000 to 1:50,000–100,000 anesthesias. However, the prevalence of the genetic abnormalities may be as great as one in 3,000 individuals. MH affects humans, certain pig breeds, dogs, horses, and probably other animals. The classic signs of MH include hyperthermia to marked degree, tachycardia, tachypnea, increased carbon dioxide production, increased oxygen consumption, acidosis, muscle rigidity, and rhabdomyolysis, all related to a hypermetabolic response. The syndrome is likely to be fatal if untreated. Early recognition of the signs of MH, specifically elevation of end-expired carbon dioxide, provides the clinical diagnostic clues. In humans the syndrome is inherited in autosomal dominant pattern, while in pigs in autosomal recessive. The pathophysiologic changes of MH are due to uncontrolled rise of myoplasmic calcium, which activates biochemical processes related to muscle activation. Due to ATP depletion, the muscle membrane integrity is compromised leading to hyperkalemia and rhabdomyolysis. In most cases, the syndrome is caused by a defect in the ryanodine receptor. Over 90 mutations have been identified in the RYR-1 gene located on chromosome 19q13.1, and at least 25 are causal for MH. Diagnostic testing relies on assessing the in vitro contracture response of biopsied muscle to halothane, caffeine, and other drugs. Elucidation of the genetic changes has led to the introduction, on a limited basis so far, of genetic testing for susceptibility to MH. As the sensitivity of genetic testing increases, molecular genetics will be used for identifying those at risk with greater frequency. Dantrolene sodium is a specific antagonist of the pathophysiologic changes of MH and should be available wherever general anesthesia is administered. Thanks to the dramatic progress in understanding the clinical manifestation and pathophysiology of the syndrome, the mortality from MH has dropped from over 80% thirty years ago to less than 5%.
Published: 24 April 2007
Orphanet Journal of Rare Diseases 2007, 2:21 doi:10.1186/1750-1172-2-21
Received: 20 March 2007 Accepted: 24 April 2007
This article is available from: http://www.OJRD.com/content/2/1/21 © 2007 Rosenberg et al; licensee BioMed Central Ltd.
Disease name and synonyms
Malignant hyperthermia
Malignant hyperpyrexia
Definition
Malignant hyperthermia (MH) is a hypermetabolic response to potent inhalation agents (such as halothane, sevoflurane, desflurane), the depolarizing muscle relaxant succinylcholine, and rarely, in humans, to stresses such as vigorous exercise and heat. The majority of patients with Central Core Disease (CCD), an inherited myopathy char-acterized by muscle weakness, are susceptible to MH. Multi-Minicore Disease (MmCD) also predisposes to epi-sodes of MH.
As almost all patients who are MH susceptible have no phenotypic changes without anesthesia, it is impossible to diagnose susceptibility without either the exposure to the "trigger" anesthetics or by specific diagnostic testing. The key diagnostic features include an unexplained elevation of expired carbon dioxide, muscle rigidity and rhabdomy-olysis, hyperthermia, acidosis and hyperkalemia.
Diagnostic criteria
The diagnosis of MH is based on clinical presentation or laboratory testing (see the section on diagnostic meth-ods).
The principal diagnostic features of MH are unexplained elevation of end-tidal carbon dioxide (ETCO2)
concentra-tion, muscle rigidity, tachycardia, acidosis, hyperthermia, and hyperkalemia. The variability in the order and time of onset of signs often makes the clinical diagnosis rather dif-ficult.
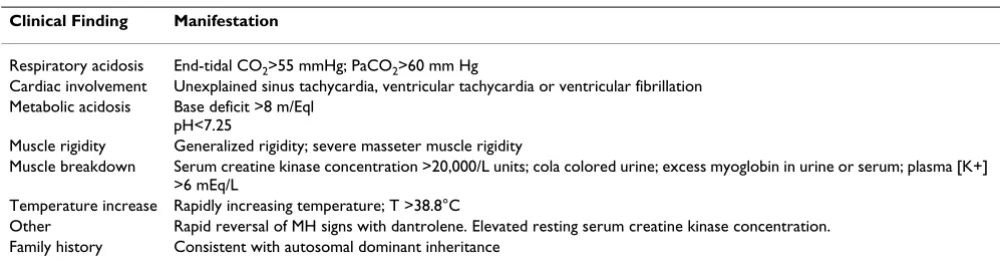
A clinical grading scale was developed by Larach and col-leagues [1] in order to assist in clinical diagnosis. The ele-ments of the scale are given in the Table 1. Differential weighting is given to each of the manifestations of the syn-drome. However, the scale lacks sensitivity since not all tests may be performed in an individual episode.
The value of the grading scale is mainly in identifying those subjects with the most convincing episodes of MH for subsequent evaluation of the sensitivity and specificity of the diagnostic tests. The clinical grading scale is useful in evaluating clinical episodes in those cases in which the subject is rated a 6 (almost certainly MH), but lower scores should not be considered for actual diagnosis.
Epidemiology
The incidence of MH episodes during anesthesia is between 1:5,000 and 1:50,000–100,000 anesthesias. Even though a MH crisis may develop at first exposure to
anesthesia with those agents known to trigger an MH epi-sode, on average, patients require three anesthesias before triggering. Reactions develop more frequently in males than females (2:1). All ethnic groups are affected, in all parts of the world. The highest incidence is in young peo-ple, with a mean age of all reactions of 18.3 years. It has been found that children under 15 years age comprised 52.1% of all reactions. Although described in the new-born, the earliest reaction confirmed by testing is six months of age [2]. The oldest is 78 years.
Genetically, MH is an autosomal dominant condition; the estimated prevalence of the genetic abnormalities may be as great as one in 3,000 individuals (range 1:3,000 to 1:8,500).
Numerous factors could be involved in triggering MH – age, type of anesthetic, environmental temperature, miti-gating drugs administered simultaneously, and degree of stress [3]. Mauritz et al. [4] found an incidence of 1:37,500 in patients who had been diagnostically tested, which was similar to the incidence estimated by Robinson et al. (1:30,000) [5], although wide variability has been reported. A recent report suggested that the MH suscepti-ble (MHS) trait may be present in 1:2,000–3,000 of the French population [6]. Bachand and colleagues examined the incidence of MH in Quebec, Canada, where many families had been biopsied [7]. They traced the pedigrees of the patients to the original immigrants from France and found an incidence of MH susceptibility of 0.2% in this province. However, that represented only five extended families.
MH crises develop not only in humans but in other spe-cies, particularly pigs, which have been a valuable source for research. Reactions have also been described in horses, dogs and other animals [8].
Clinical description
MH may occur at any time during anesthesia and in the early postoperative period. The earliest signs are tachycar-dia, rise in end-expired carbon dioxide concentration despite increased minute ventilation, accompanied by muscle rigidity, especially following succinylcholine administration. Body temperature elevation is a dramatic but often late sign of MH. Nevertheless, core temperature should be monitored in all patients undergoing general anesthesia for periods lasting more than 20 minutes, as temperature elevation may be an important confirmatory sign.
or more slower and not become manifest until after sev-eral hours of anesthesia.
All inhalation anesthetics except nitrous oxide are triggers for MH. The muscle relaxant succinylcholine is also a ger for MH. No other anesthetic drugs appear to be trig-gers, including propofol and ketamine. Neither are catecholamines, nondepolarizing muscle relaxants, cate-chol congeners, digitalis or similar agents [9].
Although ETCO2 is a sensitive early sign of MH, in recent years, with a decline in the use of succinylcholine, rather than an abrupt rise in C02, a more gradual rise is often noted. Indeed, by increasing minute ventilation it is pos-sible to mask this rise [10].
Hyperthermia, when it occurs, is marked by increase in core temperature at a rate of 1–2°C every five minutes. Severe hyperthermia (core temperature greater than 44°C) may occur, and lead to a marked increase in oxygen consumption, carbon dioxide production, widespread vital organ dysfunction, and disseminated intravascular coagulation (DIC) [11].
Uncontrolled hypermetabolism leads to cellular hypoxia that is manifested by a progressive and worsening meta-bolic acidosis. If untreated, continuing myocyte death and rhabdomyolysis result in life-threatening hyperkalemia; myoglobinuria may lead to acute renal failure. Additional life-threatening complications include DIC, congestive heart failure, bowel ischemia, and compartment syn-drome of the limbs secondary to profound muscle swell-ing, and renal failure from rhabdomyolysis. Indeed, when body temperature exceeds approximately 41°C, DIC is the usual cause of death.
Succinylcholine induced masseter muscle rigidity
Succinylcholine induced masseter muscle rigidity (MMR) occurs in 1 in 100 children with anesthesia induced by halothane and given succinylcholine [12]. The incidence
is probably the same following induction with sevoflu-rane, but much less following induction with thiopental [13]. The clinical incidence of MH as defined by arterial blood gas changes is about 15% after MMR. However, muscle biopsy reveals that 50% of patients experiencing MMR are MH susceptible [14]. Patients with generalized rigidity along with MMR are at much greater risk for MH. Kaplan (personal communication, 1995) has hypothe-sized that children with "jaws of steel" after succinylcho-line as opposed to mild rigidity are at greater risk for MH. He has hypothesized that the children with the more dra-matic masseter rigidity are more often referred for biopsy and hence the high incidence of positive biopsies. Since MMR may presage MH, it is most advisable to dis-continue the anesthetic after MMR. In an emergency, the anesthesia may continue with "non-trigger" drugs. Fol-lowing MMR, patients should be admitted to an intensive care unit and monitored for signs of MH. Rhabdomyoly-sis occurs in virtually all patients experiencing MMR and the creatine kinase (CK) values should be checked regu-larly. Dantrolene should be administered if the other signs of MH occur along with MMR. Muscle biopsy for definitive diagnosis should be carefully considered.
Central Core Disease and other myopathies
Central Core Disease (CCD) is a rare non progressive myopathy with autosomal dominant inheritance, pre-senting in infancy and characterized by hypotonia and proximal muscle weakness. A few families demonstrate autosomal recessive inheritance. Histological examina-tion of affected muscles shows a predominance of type I fibres containing clearly defined areas (cores) lacking oxi-dative enzyme activity [15].
An important feature of CCD is its close association with MH susceptibility. CCD patients are often susceptible to MH by in vitro contracture testing (IVCT), but MH and CCD phenotypes do not always co-segregate within fami-lies. Patients with MH may present with cores despite
Table 1: Criteria used in the Clinical Grading Scale for Malignant Hyperthermia
Clinical Finding Manifestation
Respiratory acidosis End-tidal CO2>55 mmHg; PaCO2>60 mm Hg
Cardiac involvement Unexplained sinus tachycardia, ventricular tachycardia or ventricular fibrillation Metabolic acidosis Base deficit >8 m/Eql
pH<7.25
Muscle rigidity Generalized rigidity; severe masseter muscle rigidity
Muscle breakdown Serum creatine kinase concentration >20,000/L units; cola colored urine; excess myoglobin in urine or serum; plasma [K+] >6 mEq/L
Temperature increase Rapidly increasing temperature; T >38.8°C
being clinically asymptomatic and with some RYR1 muta-tions (specifically some of those in the 3' transmembrane domain of the gene) specific to CCD. A recent study showed that RYR1 mutations are found in over 93% (25 out of 27) of Japanese patients with CCD [16]. While this is of importance, it may not reflect the incidence of RYR1
mutations in other populations. A more recent study indi-cated that the distribution and frequency of RYR1 muta-tions differed markedly in the Japanese MH susceptible population as compared to the North American and Euro-pean MH susceptible population [17]. Although RYR1
mutations are the most common identified cause of CCD, it does show genetic heterogeneity, with several rare sus-ceptibility loci known (the ACTA1 gene, in association with nemaline myopathy, and the MYH7 gene, in associ-ation with hypertrophic cardiomyopathy), with further loci yet to be identified [18].
At least 44 mutations have been reported in the RYR1
gene in association with CCD (reviewed in [18]). In gen-eral terms, single point RYR1 mutations can cause (a) CCD only, (b) MH only, (c) MH with variable CCD pen-etrance. In this latter case, the likelihood of an RYR1
mutation resulting in both MH and CCD depends on a number of factors including sensitivity of mutant protein to agonists, size of the intracellular Ca2+ pool and the level
of abnormality in channel-gating (reviewed in [19]). All individuals with the mutation should be MH susceptible, while they may or may not have CCD. If a mutation spe-cific to CCD is identified in a family, MH is not automat-ically excluded as a second mutation may be present and MH susceptibility needs to be assessed by IVCT [20]. If the mutation has no functional studies performed it is of no use clinically. A MH negative parent eliminates suscepti-bility in the children.
Other myopathies that have been associated with MH sus-ceptibility include some sodium channel forms of myoto-nia (myotomyoto-nia fluctuans), MmCD and hypokalemic periodic paralysis [21] and Multiminicore myopathy [22]. Guis et al., 2004 found multiminicores in 16 out of 17 MHS patients [23]. The multiminicores correlated with two missense RYR1 mutations on the same allele resulting in the amino acid changes R2656W and T2787S [23]. More recently, recessive mutations in RYR1 have been associated with MmCD, some of which result in altered Ca2+ release from intracellular stores and others that do
not [24]. Taken together, these observations suggest that there may be a subset of RYR1 mutations that result in both MH and MmCD and a subset that are associated only with MmCD, similar to the situation with MH and CCD. Consequently, it will be important to distinguish between
RYR1 mutations that result in MmCD, and those that do not.
King (or King Denborough) syndrome is a rare myopathy characterized by dysmorphic facies, ptosis, down-slanting palpebral fissures, hypertelorism, epicanthic folds, low-set ears, malar hypoplasia, micrognathia, high-arched palate, clinodactyly, palmar simian line, pectus excavatum, wing-ing of the scapulae, lumbar lordosis and mild thoracic scoliosis. The patents with King Denborough syndrome also present congenital hypotonia, slightly delayed motor development, diffuse joint hyperextensibility and mild proximal weakness. Such patients are MH susceptible.
Etiology
Experimental evidence from a variety of sources, in vitro,
in vivo, isolated cells, transfected cells and mice who's DNA has been altered to express one of the MH causative mutations clearly indicates that the signs and symptoms of MH are related to an uncontrolled release of intracellu-lar calcium from skeletal muscle sarcoplasmic reticulum (SR). In MH susceptible swine and in "knock-in" mice, a variety of environmental conditions can trigger the accel-erated calcium release such as environmental heat, exer-cise and stress. In humans, however, MH results most often from exposure to potent inhalation anesthetics +/-succinylcholine. The enhanced intracellular calcium results in activation of muscle contraction, oxygen con-sumption, carbon dioxide production, ATP breakdown and heat. The normal sequestration of released calcium is inadequate and energy is expended in a futile manner, in an attempt to lower intracellular calcium. Presumably, the declining levels of ATP lead to failure of membrane integ-rity and release of potassium and creatine kinase, although the exact steps in the process have not been definitively demonstrated.
dis-played typical MH changes and raised environmental heat led to typical MH changes [26].
In addition, dantrolene sodium (known to reverse signs of MH) has been found to bind to a specific ryanodine protein site [27].
Although mutations in the ryanodine receptor are undoubtedly important in the pathophysiology of MH, it is also clear that not all families demonstrate linkage to this gene. At least six other genetic loci have been impli-cated in MH, including one that elaborates the sodium channel [21,28] although only one other gene,
CACNL1A3, encoding the main subunit of the dihydropy-rodine receptor (DHPR), have been shown to be altered by an MH-linked mutation [29].
The clinical expression of MH is also poorly understood. Genotype-phenotype correlations are weak for both the clinical expression of MH and the response of isolated muscle to caffeine or halothane. It therefore seems clear that a variety of modulators influence the manifestations of the syndrome. The fatty acids represent one set of mod-ulators that has been studied in this respect [30,31]. Cer-tain unsaturated fatty acids have been demonstrated to increase the sensitivity of halothane-induced calcium release in vitro. Such an increase in fatty acids may result from breakdown of triglycerides as a result of enzymatic abnormalities.
In addition, in cultured muscle cells from MH susceptible patients there is a shift of subtypes of sodium channels leading to a longer membrane depolarization and an increased calcium release from the terminal cisternae [32]. Changes in sodium channel function, either through sodium channel mutations or through effects of fatty acids may influence the phenotypic expression of MH, especially muscle rigidity.
Laboratory diagnostic methods
The "gold standard" for diagnosis of MH is currently the
in vitro contracture test (IVCT), which is based on contrac-ture of muscle fibres in the presence of halothane or caf-feine. Two widely used forms of this test have been developed; one by the European Malignant Hyperthermia group (EMHG) and the other by the North American Malignant Hyperthermia Group, Caffeine Halothane Contracture Test-CHCT (NAMHG) [33,34]. While simi-larities exist in performing and interpreting the results of these tests, there are significant differences. Using the EMHG protocol, an individual is considered susceptible to MH (MHS) when both caffeine and halothane test results are positive. A normal MH diagnosis (MHN) is obtained when both tests are negative. A third diagnosis, MH equivocal (MHE), is obtained when only one of the
halothane or caffeine test is positive. Using the NAMHG protocol, an individual is diagnosed as MHS when either of the halothane or caffeine test is positive, and MNH when both tests are negative. The EMHG protocol may reduce the possibility of false positive and negative results when compared to the NAMHG protocol but overall sim-ilar results are obtained [35]. Sensitivity of 99% and a spe-cificity of 94% are obtained with the EMHG protocol [36], while figures of 97% sensitivity and 78% specificity are reported for the NAMHG. The specificity of either proto-col may be affected by neuromuscular disorders unrelated to MH which have an associated increase in myoplasmic calcium concentration. However, studies based on results from monozygote twins indicate that the IVCT has accept-able reproducibility [37]. A third variation of the IVCT, the caffeine skinned fibre test, does not appear to be used diagnostically outside of Japan, and has lower specificity and sensitivity than either the EMGH or NAMHG proto-cols.
IVCT is expensive, confined to specialized testing centers, it requires a surgical procedure and can yield equivocal as well as false positive and negative results. Modifications of the EMHG protocol include the use of ryanodine [38] (which binds selectively to the calcium release channel) or 4-chloro-m-cresol [39] but to date these agents have not been included in the standard protocol. Future supplies of halothane may be limited. A possible alternative testing agent is the fluorinated ether, sevoflurane. Trials with this agent are to be commenced soon. Other biochemical, hematological and physical tests have been used in the past but, without exception, these lack significant sensitiv-ity and specificsensitiv-ity to be used diagnostically.
DNA analysis, however, offers an alternative to the IVCT, requiring only a blood specimen, which can be sent to an accredited diagnostic laboratory. DNA testing for MH was first suggested in 1990, when a mutation within the ryan-odine receptor gene (RYR1) encoding the skeletal muscle calcium release channel was identified [40]. Since then, about 50% of MH have been linked to RYR1 with over 100 mutations associated with MH, identified within this gene [41].
MH is, however, a heterogeneous genetic disorder with at least five other susceptibility loci being identified. Amongst these loci, mutations with a clear association with MH have been identified in only one gene,
CACNA1S, encoding the alpha subunit of the dihydropy-ridine receptor, the voltage sensor of the skeletal muscle calcium release channel [29,42,43]. Early studies sug-gested that mutations cluster within three regions of RYR1
coding regions of RYR1 has, however, revealed that muta-tions occur in almost all regions of the gene [17,41].
While the majority of mutations lead to a single amino acid change in the receptor [44], deletions or truncations have also been reported [45-47]. A number of recessive mutations have also been reported to result in either MH or CCD [48].
The identification of causative mutations suggests the widespread use of DNA testing for MH, however, this is confounded by the metabolic complexity and genetic het-erogeneity of the disorder. Moreover, discordance between MHS diagnosed by IVCT and the presence of causative mutations has been shown within individual families [49-55]. In most cases, genotype-phenotype dis-cordance where MHS has been diagnosed by IVCT is likely to be due to the presence of a separate mutation either in
RYR1 or at a separate locus [6,56]. False positive results for the IVCT cannot be ruled out however, and probably account for a small proportion of such discordance. False positive results could be expected as the IVCT is not 100% specific and could be due to an unrelated myopathic con-dition. Until a greater understanding of the pathophysiol-ogy of these other conditions and their relationship to the MH phenotype is known, these patients would need to be treated as MHS. Discordance in patients with a causative mutation but who have been diagnosed MHN by IVCT has also been reported by some testing laboratories [55]. As causative mutations clearly show altered calcium release from intracellular stores, these rare instances of discordance are likely to be due to a false negative diagno-sis in the IVCT. Taken together, these observations suggest that DNA testing should always be used in selected, genet-ically characterized families, as well as within the guide-lines for DNA testing identified by the EMHG [57] or the NAMHG [58]. Using both IVCT and genetic diagnosis, a higher proportion of true positives are likely to be identi-fied than by simply relying on one or other test.
The guidelines set down by the EMHG requires contrac-ture testing prior to genetic testing in a family. Once a causative mutation is found in a family member, others may be tested for susceptibility by seeking out that muta-tion in the DNA. The predictive value of the genetic test has been suggested to be ~50% based on correlation between an MHS diagnosis by IVCT and presence of a causative mutation [58]. Using the same criteria, 62% of MHS patients in one family (36/58) were diagnosed MHS by genetic testing [56]. Another study reported the predic-tive value of genetic testing to be ~80% in a total of 10 families [55]. The sensitivity of the DNA test clearly varies within populations but will likely increase as more muta-tions are identified especially for those families where a significant level of discordance has been observed.
In summary, because of the heterogeneity of the disorder, as well as discordance within families, a negative DNA result cannot be used to rule out MH susceptibility. In addition, only those mutations that have been biochemi-cally characterized to affect SR calcium release can be used to test for MH susceptibility. Approximately 28 mutations within RYR1 have been shown to cause an alteration in calcium release from intracellular stores. A number of functional tests have been used successfully to assess the role of RYR1 mutations in calcium release. These include the use of lymphoblastoid cell lines generated from MHS individuals [59-61]. COS-7 or HEK293 cells transfected with the cDNA for rabbit RYR1 carrying point mutations introduced by site-directed mutagenesis [19,62,63], myo-tubes generated from muscle biopsy tissue [44,64-66] and 1B5 dyspedic myotubes transduced with wild type and mutated RYR1 cDNA [67]. Calcium release can be moni-tored and quantified using calcium-specific indicators like fluo-4 and fura-2 [68], [3H] ryanodine binding assays
amount of caffeine will elicit an enhanced release of car-bon dioxide from the muscle tissue, which can be meas-ured by capnography [71].
Differential diagnosis
A variety of unusual conditions may resemble MH during anesthesia. These include sepsis, thyroid storm, pheochro-mocytoma, and iatrogenic overheating. Hence, a high index of suspicion for these disorders as well as the ability to measure ETCO2 and obtain arterial and venous blood gas analysis is essential in order to differentiate MH from these disorders. Particularly problematic is the unex-plained hyperthermia following anesthesia. Since anes-thetic gases generally inhibit the febrile response, the first sign of sepsis may be marked hyperthermia on emergence from anesthesia. Response to antipyretics as well the clin-ical setting is often helpful in differentiating this response from MH.
The differential diagnosis of unexplained increased ETCO2 includes hyperthermia secondary to sepsis, or iatrogenic warming, machine valve malfunction, rebreathing, as well as faulty equipment.
Outside the operating room, MH-like syndrome may occur following injection of ionic contrast agents into the cerebrospinal fluid, cocaine overdose, and the neurolept-malignant syndrome(NMS).
NMS is a potentially fatal hyperthermic syndrome that occurs as a result of ingestion of drugs used in the treat-ment of treat-mental and nervous conditions such as schizo-phrenia. The incidence is approximately 0.01–0.02% of those being treated with these drugs such as older as well as newer antipsychotics and haloperidol, a sedative agent often used in the ICU to treat agitation. Other dopamine antagonists also have been reported to cause NMS.
The signs of NMS include muscle rigidity, acidosis, high fever, rhabdomyolysis. The pathophysiology is thought to result from dopamine receptor blockade. Treatment includes benzodiazepines, bromocriptine and even dant-rolene. There does not appear to be any cross over suscep-tibility to MH or vice versa. There is no laboratory diagnostic test for the syndrome either [72].
If a high ionic, water-soluble radiologic contrast agent is injected intrathecally, usually as a result of drug mixup, a characteristic progression of signs occurs. After the injec-tion, the patient appears to recover normally, but within thirty minutes involuntary jerking movements begin in the lower extremities and ascend to the upper body, finally resulting in seizures and hyperthermia. This is the result of the contrast agent entering the cerebral ventricles and requires a rapid symptomatic treatment of the muscle
activity, hyperthermia, and acidosis (cooling, nondepo-larizing neuromuscular blockers, ventilation, and seda-tion) [73]. The response of signs of hyperthermia, tachycardia and tachypnea to dantrolene in such syn-dromes is non-specific. In other words, the response to dantrolene does not per se prove MH susceptibility. In many countries, a "hotline" has been established to provide emergency assistance in the management of MH. Many are listed on the web site of the Malignant Hyper-thermia Association of the US [74].
Hyperkalemic cardiac arrest in patients with muscular dystrophy
A syndrome often confused with MH is sudden hyperka-lemic cardiac arrest during or shortly after anesthesia in young males. Following sporadic reports of such arrests, Larach and colleagues identified that patients with an occult myopathy, especially a dystrophinopathy such as Duchenne's muscular dystrophy, are at risk to dramatic life-threatening hyperkalemia upon administration of succinylcholine [75]. More recently, it has been shown that administration of potent volatile agents to such patients may produce a similar syndrome [76].
Since the most common muscular dystrophy (Duch-enne's) is found with a frequency of 1 in 3500 live male births, and the onset of symptoms of muscle weakness may be as late as 6–8 years of age, some apparently healthy children may really be at risk of succinylcholine induced hyperkalemia. Hence, when a young child or young adult experience a sudden and apparently unex-pected cardiac arrest, think of hyperkalemia, document and treat it in the standard fashion (calcium, bicarbonate, glucose and insulin, and hyperventilation). Muscle tissue should be obtained and preserved for testing for a myop-athy, specifically a dystrophinopathy.
In general, the patient with a dystrophinopathy that develops these anesthetic-related complications does not also exhibit classic signs of MH, such as hypethermia or marked muscle rigidity. They do, however, develop rhab-domyolysis. Therefore, this reaction is not malignant hypethermia per se, since the dystrophinopathies are caused by mutations on the X chromosome.
Rhabdomyolysis
Rhabdomyolysis refers to the breakdown of skeletal mus-cle which is associated with excretion of myoglobin in the urine. Classically, MH presents with hypercarbia, tachy-cardia, cardiac arrhythmias, pyrexia, rigidity and meta-bolic acidosis, and rhabdomyolysis as a late sign. Several reports of isolated rhabdomyolysis apparent immediately following anesthesia or developing up to 24 hours post anesthesia have been published [77,78]. Increased creat-ine kinase (CK) measurement and a positive IVCT have been obtained in these patients, indicating MH suscepti-bility. However, MH-like muscle responses can represent false positive diagnoses and an underlying myopathic process may produce a positive IVCT [79], so there must remain some doubt on the validity of this feature i.e. rhab-domyolysis as an expression of MH. Burns et al. however stated that MH should be considered in all patients pre-senting with rhabdomyolysis where the degree of muscle necrosis exceeds that expected for the severity of the accompanying disorder [80]. The most prudent diagnostic course, therefore, is contracture testing for MH suscepti-bility.
Genetic counseling
Genetic testing can be defined as an analysis or test that confirms the presence or the absence of a genetic condi-tion; this does not necessarily involve the analysis of DNA as there are still many clearly genetic conditions where the gene has not yet been identified. In the context of MH, the IVCT could be considered to be just as much a genetic test as the analysis of the RYR1 gene.
Genetic testing is different to the traditional medical test in that not only will the result have potential ramifica-tions for the current health of that individual, but it may also have ramifications for the future health of that indi-vidual and the future health of their immediate relatives [81,82]. Depending on the test being performed, results may leave the individuals disadvantaged in terms of their ability to access health insurance or life insurance, employment opportunities and, in some cultures, may even affect marital opportunities [83,84]. For this reason it is recommended that each individual accessing any form of genetic testing and indeed each individual under-going IVCT or RYR1 analysis should be fully informed of all the implications of each potential result and should be able to provide informed consent [85,86]. The process of imparting this information and discussing any questions the patient may have, is known as genetic counseling. This discussion with a clinician or genetic counselor should include the following points of information (Am. Soc. Hum. Gen. 1975):
- Potential implications the result may have on their abil-ity to obtain health/life insurance [87,88].
- Potential psychological effects of the result. Some par-ents feel guilty that they may have passed MH sensitivity on to their children, others may feel anxious about the implications of a MH sensitivity result and experience an increased fear of surgery, others may even feel guilty if they have not inherited MH when their brother or sister has [89-91].
- Inheritance pattern of the disorder and what implica-tions their test result may have for their children and the extended family.
If there is also a family history of CCD, it is important that the potential diagnosis of this condition is not lost in the discussions regarding MH. CCD is an extremely variable condition within families and while some individuals may only be very mildly affected, other family members may have a more severe phenotype [15].
Interpreting risk for other family members
MH is an autosomal dominant condition. When initiating genetic analysis in a branch of a known family, it is impor-tant to test the individual at the highest risk first.
Parents of a proband
The large majority of times, an affected proband will have inherited MH sensitivity from one of the parents. Clarifi-cation of which parent may also be MHS is useful for iden-tifying which side of the extended family (i.e. aunts and uncles) may be at risk.
Siblings of a proband
The risk to the siblings depends of the genetic status of the parents. If a parent is identified as MHS, then each of the proband's siblings have a 1 in 2 or 50% chance of also being MHS. If both parents receive an MHN result on IVCT and RYR1 analysis – suggesting the mutation is de novo in the proband – then the proband's siblings are at no greater risk than the general population.
Offspring of a proband
The risk for offspring of each individual with proven MHS also has a 50% chance of being MHS. The proband's grandchildren would be considered to be at 25% risk until their parent's genetic status is clarified.
Note: An individual who is MHN cannot pass MH sensi-tivity on to the next generation, however, if they have an affected parent, their siblings may still be at risk.
Interpretation of risk for other family members in the context of RYR1 analysis
dis-cordance between IVCT and mutation analysis in some families, current protocols state that a negative mutation result is not sufficient to identify a person as being MHN. In the event of a normal (negative) mutation result, IVCT is still recommended to confirm MHN status, and the individual and his/her offspring are still considered to be potentially MHS unless IVCT proves otherwise [54]. However, it is important to remember that in the event of a normal (negative) mutation result, the offspring of the individual are no longer at risk of inheriting the character-ized family mutation. As the tested individual does not carry the mutation, he cannot pass it on to his offspring. Therefore, if an individual is mutation negative but IVCT positive, the only useful test available to the offspring is IVCT.
Final note on autonomy in clinical testing for MH
Some individuals may wish to delay IVCT or RYR1 analy-sis, while they consider the information they have been given and/or make the necessary preparations. Others may decide that they do not want their risk clarified by clinical testing. These decisions should be respected and these individuals considered being MHS until proven oth-erwise.
Care should then be taken when arranging testing for the offspring of these individuals as a positive result in the next generation will generate a result for the individual who did not want to know (the individual must have car-ried the gene mutation in order to pass it on).
Management and treatment
Acute MH crisis
The essential points in the treatment of acute MH crisis are the immediate discontinuation of trigger agents, hyper-ventilation, administration of dantrolene in doses of 2.5 mg/kg repeated prn (pro re nata) to limit MH, cooling by all routes available (especially nasogastric lavage), and treating hyperkalemia in a standard fashion. Calcium blockers should not be used along with dantrolene, since hyperkalemia may occur with such a drug combination. The steps in the treatment of acute MH are as follows: 1. Stop potent inhalation agents and succinylcholine.
2. Increase minute ventilation to lower ETCO2. 3. Get help.
4. Prepare and administer dantrolene: - 2.5 mg/kg initial dose;
- Titrate dantrolene to tachycardia and hypercarbia;
- 10 mg/kg suggested upper limit, but more may be given as needed.
5. Begin cooling measures:
- If hyperthermic, use iced solutions, i.e. Ice Packs to groin, axilla, and neck;
- Nasogastric lavage with iced solution; - More aggressive measures as needed; - Stop cooling measures at 38.5°C.
6. Treat arrhythmias as needed. Do not use calcium chan-nel blockers.
7. Secure blood gases, electrolytes, creatine kinase, blood and urine for myoglobin;
- Coagulation profile check values every 6–12 hours;
- Treat hyperkalemia with hyperventilation, glucose and insulin as needed;
- Once crisis is under control, an MH hotline should be contacted for further guidance.
8. Continue dantrolene at 1 mg/kg every 4–8 hours for 24–48 hours.
9. Insure urine output of 2 ml/kg/hour with mannitol, furosemide, and fluids as needed.
10. Evaluate need for invasive monitoring and continued mechanical ventilation.
11. Observe patient in Intensive Care Unit for at least 36 hours.
12. Refer patient and family to MH Testing Center for con-tracture or DNA testing.
Patients experiencing MH should receive dantrolene and be monitored closely for 48–72 hours, since (even despite dantrolene treatment) 25% of patients will experience a recrudescence of the syndrome. Tests for disseminated intravascular coagulation (DIC) should be included, as well as observation of the urine for myoglobinuric renal failure. DIC is most frequent when body temperature exceeds about 41°C.
Preventive measures
member having experienced an MH episode. When suspi-cion of MH exists, family members should not be given trigger anesthetic agents, i.e. potent volatile anesthetic agents such as halothane, sevoflurane, desflurane, enflu-rane, isoflurane and succinylcholine, and testing is recom-mended.
Patients with any form of myotonia should not receive succinylcholine. Patients with hypokalemic periodic paralysis, CCD, Duchenne or Becker muscular dystrophy, paramyotonia, or myotonia fluctuans should not receive trigger agents.
All patients receiving more than a brief general anesthetic should have their core temperature monitored.
Young patients (below age 12 approximately) should not receive succinylcholine for elective procedures, in order to avoid the possibility of hyperkalemic response in a patient with undiagnosed muscular dystrophy.
Patients who are MH susceptible should be cautioned regarding the remote, but conceivable possibility of heat stroke in environments in which exposure to high heat and humidity is possible.
Management of the MH susceptible for anesthesia
Patients who are known to be MH susceptible may be anesthetized with regional anesthesia or local anesthesia without problems. If general anesthesia or sedation is required, the potent volatile agents and succinylcholine should be avoided.
The anesthesia machine should be prepared by flowing 100% oxygen through the machine at 10 L/min for at least 20 minutes. The ventilator should also be included in purging the machine by cycling the ventilator at the time of the oxygen flow. Vaporizers should be disabled, drained or removed if possible. All intravenous agents and nondepolarizing relaxants are safe to use.
Once the patient has undergone such an anesthetic with-out incident, he/she may be treated similar to any other patients. It is no longer felt to be necessary to monitor such patients in the post-anesthesia care unit for four hours routinely. Pretreatment with dantrolene is also not necessary.
Unresolved issues
Discordance
Given the confidence provided by functional analysis of
RYR1 mutations, the problem of discordance between
RYR1 mutations and MHS and MH equivocal (MHE) diagnosis still remains the largest problem associated with genetic diagnosis of susceptibility to MH. The MHE
diag-nosis is the most problematic and exhibits a much higher level of discordance than does MHS. Correlation between
RYR1 mutations and IVCT is greater for the caffeine (c) than the halothane (h) response [92] suggesting that the MHE(c) has greater diagnostic potential. The NAMHG protocol does not allow the MHE diagnosis; the potential for discordance between IVCT phenotype and RYR1 geno-type is therefore much greater. In a large UK study investi-gating the relationship between RYR1 genotype and IVCT phenotype, discordance was identified in seven families (nine individuals), with five positives and four false-negatives [20]. Mutation negative MHS individuals have also been observed [20,55] (Recent unpublished data give an approximate 2.5% discordance rate of this type in a large series of UK patients). Clear evidence of the involve-ment of genes as well as RYR, has been shown in a New Zealand Maori pedigree where MHS correlates with a T4826I mutation [56]; but three branches of the family possess unrelated chromosome 19 haplotypes, without the T4826I mutation in unambiguous MHS individuals spanning three or four generations. While some discord-ance may be explained by the existence of other yet uni-dentified mutations, false positive IVCT tests [93] and weak contracture mutations [20] have also been impli-cated. Clearly, while genetic diagnosis can be used selec-tively, a greater knowledge of the molecular mechanisms resulting in susceptibility to MH is required before the IVCT can be dispensed with.
Awake MH
In 1966 the Porcine Stress Syndrome was identified as an "awake" malignant hyperthermia episode. Stresses such as fighting cause a rapid death in these animals. In 1974 Wingard described an MH susceptible family with exercise and emotional induced pyrexia, in sudden deaths unre-lated to surgery. He considered that MH was part of a human stress syndrome. Subsequently, a number of reports of MH reactions in patients given trigger-free anes-thetics appeared. None of these reactions were totally con-vincing.
However, Gronert and Denborough, both reported patients with "awake" MH episodes, the latter being patients with exercise-induced heat stroke who responded to dantrolene [94-96]. Perhaps the most convincing, though unfortunate, episode of exercise induced MH was reported by Tobin et al., a fatal episode in a 13-year-old boy who had experienced a clinical episode of MH and developed signs of MH following exercise some months later. He and other family members were found to have a causative RYR 1 mutation [97]. Brown et al. reported a possible viral trigger [56].
recov-ering from violent exercise [98]. The sympathetic nervous system appears to be only secondarily involved [99], but serotonin (5HT) agonists may cause an MH-like syn-drome in susceptible pigs [100]. These agents can also cause MHS contractures in susceptible muscle [101]. Does serotonin have a role in the stress-induced episodes? There is limited support for this [102,103]. Recent research in mice with the Y522S mutation indicates abnormal sensitivity to increased environmental temper-atures associated with abnormal calcium release. This lat-est report, however, should be considered with some caution as the homozygous Y522S mutation in mouse is embryonic lethal, which is a different phenotype to that observed with the homozygous R615C mutation in pigs and the small number of homozygous RYR1 mutations in humans which clearly do not cause embryonic lethality. A more recent study, however, reports that a "knock-in" mouse heterozygous for the R163C RYR1 mutation is more representative of the human phenotype and thus may provide an important model system for further study of awake-MH [104].
Wappler et al. described a 34-year-old male with recurrent fever, fatigue, muscle cramping, and aching with mild exercise and emotional stress [105]. IVCT demonstrated an MHS response and a "causative" mutation. Others have reported similar findings [106,107]. A possible con-clusion is that a small subset of MH patients may display muscle damage and perhaps more ominous signs with the stress of exercise, and may be other stresses. It is recom-mended that MH is excluded in patients who have had episodes of exert ional heat stroke [108]. Despite possible links between exertional heat stroke and MH however, treatment with dantrolene has had limited results, thus this drug should not be used routinely in the management of heat stroke.
Resources
Many anesthesia textbooks, web sites and articles contain very thorough descriptions of MH and related syndromes. However, these sources often fail to provide information for patients (patient-specific information). Various volun-tary organizations throughout the world are dedicated to assisting patients, physicians, anesthesia providers of all types and any one else in managing the MHS and keeping these individuals up to date with the latest information regarding MH.
In the United States, the Malignant Hyperthermia Associ-ation of the United States (MHAUS) provides newsletters, printed information, an informative website [75] to meet the needs of the various groups interested in MH. In addi-tion, a hotline provides direct consultation for providers in real time management of MH episodes or questions related to specific patient as to their likelihood of
develop-ing MH and the optimum management of an episode. MHAUS, similar to other MH patient advocacy organiza-tions is not for profit supported by voluntary contribu-tions. The North American MH Registry supports a patient-specific database with detailed information as to the phenotypic presentations as well as diagnostic test results. The Registry is a subsidiary of MHAUS and is located at Children's Hospital of Pittsburgh [109]. The European MH group [110] coordinates testing proce-dures throughout Europe and is made up of professionals investigating MH. Patient supported MH associations exist in France, Germany, Switzerland, Japan, United Kingdom and several other countries. In South Africa, issues related to MH are subsumed under the Muscular Dystrophy Association of that country. These organiza-tions have been crucial to the education of anesthesia pro-viders in diagnosing and managing MH and helping patients better understand the disorder.
References
1. Larach MG, Localio AR, Allen GC, Denborough MA, Ellis FR, Gronert GA, Kaplan RF, Muldoon SM, Nelson TE, Ording H, et al.: A clinical grading scale to predict malignant hyperthermia susceptibil-ity. Anesthesiology 1994, 80(4):771-779.
2. Chamley D, Pollock AN, K.M. S, Brown RL: Malignant Hyperther-mia in Infancy and Identification of a novel RYR1 mutation. British journal of Anaesthesia 2000, 84:500-504.
3. Ording H: Incidence of malignant hyperthermia in Denmark. Anesth Analg 1985, 64(7):700-704.
4. Mauritz W, Hackl W, Winkler M, Sporn P, Steinbereithner K:
Anesthesia in malignant hyperthermia susceptible patients. Acta Anaesthesiol Belg 1990, 41(2):87-94.
5. Robinson RL, Curran JL, Ellis FR, Halsall PJ, Hall WJ, Hopkins PM, Iles DE, West SP, Shaw MA: Multiple interacting gene products may influence susceptibility to malignant hyperthermia. Ann Hum Genet 2000, 64(Pt 4):307-320.
6. Monnier N, Krivosic-Horber R, Payen JF, Kozak-Ribbens G, Nivoche Y, Adnet P, Reyford H, Lunardi J: Presence of two different genetic traits in malignant hyperthermia families: implica-tion for genetic analysis, diagnosis, and incidence of malig-nant hyperthermia susceptibility. Anesthesiology 2002,
97(5):1067-1074.
7. Bachand M, Vachon N, Boisvert M, Mayer FM, Chartrand D: Clinical reassessment of malignant hyperthermia in Abitibi-Temis-camingue. Can J Anaesth 1997, 44(7):696-701.
8. Britt BA: Malignant hyperthermia. Can Anaesth Soc J 1985,
32(6):666-678.
9. Hopkins PM: Malignant hyperthermia: advances in clinical management and diagnosis. Br J Anaesth 2000, 85(1):118-128. 10. Karan SM, Crowl F, Muldoon SM: Malignant hyperthermia
masked by capnographic monitoring. Anesth Analg 1994,
78(3):590-592.
11. Nelson TE: Porcine malignant hyperthermia: critical temper-atures for in vivo and in vitro responses. Anesthesiology 1990,
73(3):449-454.
12. Schwartz L, Rockoff MA, Koka BV: Masseter spasm with anesthe-sia: incidence and implications. Anesthesiology 1984,
61(6):772-775.
13. Lazzell VA, Carr AS, Lerman J, Burrows FA, Creighton RE: The inci-dence of masseter muscle rigidity after succinylcholine in infants and children. Can J Anaesth 1994, 41(6):475-479. 14. O'Flynn RP, Shutack JG, Rosenberg H, Fletcher JE: Masseter muscle
rigidity and malignant hyperthermia susceptibility in pediat-ric patients. An update on management and diagnosis. Anesthesiology 1994, 80(6):1228-1233.
pathological, and genetic features. Arch Dis Child 2003,
88(12):1051-1055.
16. Wu S, Ibarra MC, Malicdan MC, Murayama K, Ichihara Y, Kikuchi H, Nonaka I, Noguchi S, Hayashi YK, Nishino I: Central core disease is due to RYR1 mutations in more than 90% of patients. Brain
2006, 129(Pt 6):1470-80 Epub 2006 Apr 18.
17. Ibarra MC, Wu S, Murayama K, Minami N, Ichihara Y, Kikuchi H, Noguchi S, Hayashi YK, Ochiai R, Nishino I: Malignant hyperther-mia in Japan: mutation screening of the entire ryanodine receptor type 1 gene coding region by direct sequencing. Anesthesiology 2006, 104(6):1146-1154.
18. Shepherd S, Ellis F, Halsall J, Hopkins P, Robinson R: RYR1 muta-tions in UK central core disease patients: more than just the C-terminal transmembrane region of the RYR1 gene. J Med Genet 2004, 41(3):e33.
19. McCarthy TV, Quane KA, Lynch PJ: Ryanodine receptor muta-tions in malignant hyperthermia and central core disease. Hum Mutat 2000, 15(5):410-417.
20. Robinson RL, Brooks C, Brown SL, Ellis FR, Halsall PJ, Quinnell RJ, Shaw MA, Hopkins PM: RYR1 mutations causing central core disease are associated with more severe malignant hyper-thermia in vitro contracture test phenotypes. Hum Mutat
2002, 20(2):88-97.
21. Marchant CL, Ellis FR, Halsall PJ, Hopkins PM, Robinson RL: Muta-tion analysis of two patients with hypokalemic periodic paralysis and suspected malignant hyperthermia. Muscle Nerve 2004, 30(1):114-117.
22. Mathews KD, Moore SA: Multiminicore myopathy, central core disease, malignant hyperthermia susceptibility, and RYR1 mutations: one disease with many faces? Arch Neurol 2004,
61(1):27-29.
23. Guis S, Figarella-Branger D, Monnier N, Bendahan D, Kozak-Ribbens G, Mattei JP, Lunardi J, Cozzone PJ, Pellissier JF: Multiminicore dis-ease in a family susceptible to malignant hyperthermia: his-tology, in vitro contracture tests, and genetic characterization. Arch Neurol 2004, 61(1):106-113.
24. Ducreux S, Zorzato F, Ferreiro A, Jungbluth H, Muntoni F, Monnier N, Muller CR, Treves S: Functional properties of ryanodine receptors carrying three amino acid substitutions identified in patients affected by multi-minicore disease and central core disease, expressed in immortalized lymphocytes. Bio-chem J 2006, 395(2):259-266.
25. Sambuughin N, Holley H, Muldoon S, Brandom BW, de Bantel AM, Tobin JR, Nelson TE, Goldfarb LG: Screening of the entire ryan-odine receptor type 1 coding region for sequence variants associated with malignant hyperthermia susceptibility in the north american population. Anesthesiology 2005,
102(3):515-521.
26. Chelu MG, Goonasekera SA, Durham WJ, Tang W, Lueck JD, Riehl J, Pessah IN, Zhang P, Bhattacharjee MB, Dirksen RT, Hamilton SL:
Heat- and anesthesia-induced malignant hyperthermia in an RyR1 knock-in mouse. Faseb J 2006, 20(2):329-330.
27. Paul-Pletzer K, Yamamoto T, Bhat MB, Ma J, Ikemoto N, Jimenez LS, Morimoto H, Williams PG, Parness J: Identification of a dantro-lene-binding sequence on the skeletal muscle ryanodine receptor. J Biol Chem 2002, 277(38):34918-34923.
28. Vita GM, Olckers A, Jedlicka AE, George AL, Heiman-Patterson T, Rosenberg H, Fletcher JE, Levitt RC: Masseter muscle rigidity associated with glycine1306-to-alanine mutation in the adult muscle sodium channel alpha-subunit gene. Anesthesiology
1995, 82(5):1097-1103.
29. Monnier N Procaccio, V., Stieglitz, P. and Lunardi, J.: Malignant-Hyperthermia Susceptibility is Associated with a Mutation of the a1-Subunit of the Human Dihydropyridine-Sensitive L-Type Voltage-Dependent Calcium-Channel Receptor in Skeletal Muscle. American Journal of Human Genetics 1997, 60:1316 -11325.
30. Fletcher JE, Tripolitis L, Rosenberg H, Beech J: Malignant hyper-thermia: halothane- and calcium-induced calcium release in skeletal muscle. Biochem Mol Biol Int 1993, 29(4):763-772. 31. Fletcher JE, Mayerberger S, Tripolitis L, Yudkowsky M, Rosenberg H:
Fatty acids markedly lower the threshold for halothane-induced calcium release from the terminal cisternae in human and porcine normal and malignant hyperthermia sus-ceptible skeletal muscle. Life Sci 1991, 49(22):1651-1657.
32. Wieland SJ, Fletcher JE, Rosenberg H, Gong QH: Malignant hyper-thermia: slow sodium current in cultured human muscle cells. Am J Physiol 1989, 257(4 Pt 1):C759-65.
33. Larach MG: Standardization of the caffeine halothane muscle contracture test. North American Malignant Hyperthermia Group. Anesth Analg 1989, 69(4):511-515.
34. Larach MG, Landis JR, Bunn JS, Diaz M: Prediction of malignant hyperthermia susceptibility in low-risk subjects. An epidemi-ologic investigation of caffeine halothane contracture responses. The North American Malignant Hyperthermia Registry. Anesthesiology 1992, 76(1):16-27.
35. Ording H, Bendixen D: Sources of variability in halothane and caffeine contracture tests for susceptibility to malignant hyperthermia. Eur J Anaesthesiol 1992, 9(5):367-376.
36. Ording H, Brancadoro V, Cozzolino S, Ellis FR, Glauber V, Gonano EF, Halsall PJ, Hartung E, Heffron JJ, Heytens L, Kozak-Ribbens G, Kress H, Krivosic-Horber R, Lehmann-Horn F, Mortier W, Nivoche Y, Ranklev-Twetman E, Sigurdsson S, Snoeck M, Stieglitz P, Tegazzin V, Urwyler A, Wappler F: In vitro contracture test for diagnosis of malignant hyperthermia following the protocol of the European MH Group: results of testing patients surviving ful-minant MH and unrelated low-risk subjects. The European Malignant Hyperthermia Group. Acta Anaesthesiol Scand 1997,
41(8):955-966.
37. Islander G, Ranklev Twetman E: Results of in vitro contracture tests for the diagnosis of malignant hyperthermia suscepti-bility in monozygote twins. Acta Anaesthesiol Scand 1997,
41(6):731-735.
38. Bendahan D, Guis S, Monnier N, Kozak-Ribbens G, Lunardi J, Ghattas B, Mattei JP, Cozzone PJ: Comparative analysis of in vitro con-tracture tests with ryanodine and a combination of ryanod-ine with either halothane or cafferyanod-ine: a comparative investigation in malignant hyperthermia. Acta Anaesthesiol Scand 2004, 48(8):1019-1027.
39. Rueffert H, Olthoff D, Deutrich C, Meinecke CD, Froster UG: Muta-tion screening in the ryanodine receptor 1 gene (RYR1) in patients susceptible to malignant hyperthermia who show definite IVCT results: identification of three novel muta-tions. Acta Anaesthesiol Scand 2002, 46(6):692-698.
40. McCarthy TV, Healy JM, Heffron JJ, Lehane M, Deufel T, Lehmann-Horn F, Farrall M, Johnson K: Localization of the malignant hyperthermia susceptibility locus to human chromosome 19q12-13.2. Nature 1990, 343(6258):562-564.
41. Robinson R, Carpenter D, Shaw MA, Halsall J, Hopkins P: Mutations in RYR1 in malignant hyperthermia and central core disease. Hum Mutat 2006, 27(10):977-989.
42. Melzer W, Dietze B: Malignant hyperthermia and excitation-contraction coupling. Acta Physiol Scand 2001, 171(3):367-378. 43. Vainzof M, Muniz VP, Tsanaclis AM, Silva HC, Rusticci MS: Does the
A3333G mutation in the CACNL1A3 gene, detected in malignant hyperthermia, also occur in central core disease? Genet Test 2000, 4(4):383-386.
44. Wehner M, Rueffert H, Koenig F, Olthoff D: Functional character-ization of malignant hyperthermia-associated RyR1 muta-tions in exon 44, using the human myotube model. Neuromuscul Disord 2004, 14(7):429-437.
45. Lyfenko AD, Ducreux S, Wang Y, Xu L, Zorzato F, Ferreiro A, Meiss-ner G, Treves S, Dirksen RT: Two central core disease (CCD) deletions in the C-terminal region of RYR1 alter muscle exci-tation-contraction (EC) coupling by distinct mechanisms. Hum Mutat 2007, 28(1):61-68.
46. Sambuughin N, McWilliams S, de Bantel A, Sivakumar K, Nelson TE:
Single-amino-acid deletion in the RYR1 gene, associated with malignant hyperthermia susceptibility and unusual con-traction phenotype. Am J Hum Genet 2001, 69(1):204-208. 47. Rossi D, De Smet P, Lyfenko A, Galli L, Lorenzini S, Franci D, Petrioli
F, Orrico A, Angelini C, Tegazzin V, Dirksen R, Sorrentino V: A trun-cation in the RYR1 gene associated with central core lesions in skeletal muscle fibres. J Med Genet 2007, 44(2):e67. 48. Kossugue PM, Paim JF, Navarro MM, Silva HC, Pavanello RC,
Gurgel-Giannetti J, Zatz M, Vainzof M: Central core disease due to reces-sive mutations in RYR1 gene: Is it more common than described? Muscle Nerve 2007.
vitro contracture-test phenotypes and haplotypes for the MHS1 region on chromosome 19q12-13.2, comprising the C1840T transition in the RYR1 gene. Am J Hum Genet 1995,
56(6):1334-1342.
50. Fagerlund TH, Ording H, Bendixen D, Islander G, Ranklev Twetman E, Berg K: Discordance between malignant hyperthermia sus-ceptibility and RYR1 mutation C1840T in two Scandinavian MH families exhibiting this mutation. Clin Genet 1997,
52(6):416-421.
51. Fortunato G, Carsana A, Tinto N, Brancadoro V, Canfora G, Salva-tore F: A case of discordance between genotype and pheno-type in a malignant hyperthermia family. Eur J Hum Genet 1999,
7(4):415-420.
52. MacLennan DH: Discordance between phenotype and geno-type in malignant hyperthermia. Curr Opin Neurol 1995,
8(5):397-401.
53. Pollock AN, Langton EE, Couchman K, Stowell KM, Waddington M:
Suspected malignant hyperthermia reactions in New Zea-land. Anaesth Intensive Care 2002, 30(4):453-461.
54. Robinson R, Hopkins P, Carsana A, Gilly H, Halsall J, Heytens L, Islander G, Jurkat-Rott K, Muller C, Shaw MA: Several interacting genes influence the malignant hyperthermia phenotype. Hum Genet 2003, 112(2):217-218.
55. Robinson RL, Anetseder MJ, Brancadoro V, van Broekhoven C, Car-sana A, Censier K, Fortunato G, Girard T, Heytens L, Hopkins PM, Jurkat-Rott K, Klinger W, Kozak-Ribbens G, Krivosic R, Monnier N, Nivoche Y, Olthoff D, Rueffert H, Sorrentino V, Tegazzin V, Mueller CR: Recent advances in the diagnosis of malignant hyperther-mia susceptibility: how confident can we be of genetic test-ing? Eur J Hum Genet 2003, 11(4):342-348.
56. Brown RL, Pollock AN, Couchman KG, Hodges M, Waaka R, Lynch P, McCarthy TV, Stowell KM: A novel ryanodine receptor muta-tion and genotype-phenotype correlamuta-tion in a large malig-nant hyperthermia New Zealand Maori pedigree. Human Molecular Genetics 2000, 9(10):1515-1524.
57. Urwyler A, Deufel T, McCarthy T, West S: Guidelines for molec-ular genetic detection of susceptibility to malignant hyper-thermia. Br J Anaesth 2001, 86(2):283-287.
58. Girard T, Treves S, Voronkov E, Siegemund M, Urwyler A: Molecu-lar genetic testing for malignant hyperthermia susceptibility. Anesthesiology 2004, 100(5):1076-1080.
59. Girard T, Cavagna D, Padovan E, Spagnoli G, Urwyler A, Zorzato F, Treves S: B-lymphocytes from malignant hyperthermia-sus-ceptible patients have an increased sensitivity to skeletal muscle ryanodine receptor activators. J Biol Chem 2001,
276(51):48077-48082.
60. Sei Y, Brandom BW, Bina S, Hosoi E, Gallagher KL, Wyre HW, Pudi-mat PA, Holman SJ, Venzon DJ, Daly JW, Muldoon S: Patients with malignant hyperthermia demonstrate an altered calcium control mechanism in B lymphocytes. Anesthesiology 2002,
97(5):1052-1058.
61. Tilgen N, Zorzato F, Halliger-Keller B, Muntoni F, Sewry C, Palmucci LM, Schneider C, Hauser E, Lehmann-Horn F, Muller CR, Treves S:
Identification of four novel mutations in the C-terminal membrane spanning domain of the ryanodine receptor 1: association with central core disease and alteration of cal-cium homeostasis. Hum Mol Genet 2001, 10(25):2879-2887. 62. Treves S, Larini F, Menegazzi P, Steinberg TH, Koval M, Vilsen B,
Andersen JP, Zorzato F: Alteration of intracellular Ca2+ tran-sients in COS-7 cells transfected with the cDNA encoding skeletal-muscle ryanodine receptor carrying a mutation associated with malignant hyperthermia. Biochem J 1994, 301 ( Pt 3):661-665.
63. Querfurth HW, Haughey NJ, Greenway SC, Yacono PW, Golan DE, Geiger JD: Expression of ryanodine receptors in human embryonic kidney (HEK293) cells. Biochem J 1998, 334 ( Pt 1):79-86.
64. Wehner M, Rueffert H, Koenig F, Neuhaus J, Olthoff D: Increased sensitivity to 4-chloro-m-cresol and caffeine in primary myo-tubes from malignant hyperthermia susceptible individuals carrying the ryanodine receptor 1 Thr2206Met (C6617T) mutation. Clin Genet 2002, 62(2):135-146.
65. Wehner M, Rueffert H, Koenig F, Olthoff D: Calcium release from sarcoplasmic reticulum is facilitated in human myotubes derived from carriers of the ryanodine receptor type 1
mutations Ile2182Phe and Gly2375Ala. Genet Test 2003,
7(3):203-211.
66. Wehner M, Rueffert H, Koenig F, Meinecke CD, Olthoff D: The Ile2453Thr mutation in the ryanodine receptor gene 1 is associated with facilitated calcium release from sarcoplas-mic reticulum by 4-chloro-m-cresol in human myotubes. Cell Calcium 2003, 34(2):163-168.
67. Yang T, Ta TA, Pessah IN, Allen PD: Functional defects in six ryanodine receptor isoform-1 (RyR1) mutations associated with malignant hyperthermia and their impact on skeletal excitation-contraction coupling. J Biol Chem 2003,
278(28):25722-25730.
68. Grynkiewicz G, Poenie M, Tsien RY: A new generation of Ca2+ indicators with greatly improved fluorescence properties. J Biol Chem 1985, 260(6):3440-3450.
69. Richter M, Schleithoff L, Deufel T, Lehmann-Horn F, Herrmann-Frank A: Functional characterization of a distinct ryanodine recep-tor mutation in human malignant hyperthermia-susceptible muscle. J Biol Chem 1997, 272(8):5256-5260.
70. Klingler W, Baur C, Georgieff M, Lehmann-Horn F, Melzer W:
Detection of proton release from cultured human myotubes to identify malignant hyperthermia susceptibility. Anesthesiol-ogy 2002, 97(5):1059-1066.
71. Anetseder M, Hager M, Muller CR, Roewer N: Diagnosis of suscep-tibility to malignant hyperthermia by use of a metabolic test. Lancet 2002, 359(9317):1579-1580.
72. Strawn JR, Keck PEJ, Caroff SN: Neuroleptic malignant syn-drome. Am J Psychiatry 2007, (in press):.
73. Rosenberg H, Grant M: Ascending tonic-clonic syndrome sec-ondary to intrathecal Omnipaque. J Clin Anesth 2004,
16(4):299-300.
74. mhaus: www.mhaus.org. .
75. Larach MG, Rosenberg H, Gronert GA, Allen GC: Hyperkalemic cardiac arrest during anesthesia in infants and children with occult myopathies. Clinical Pediatrics 1997, 36:9-16.
76. Nathan A, Ganesh A, Godinez RI, Nicolson SC, Greeley WJ: Hyper-kalemic cardiac arrest after cardiopulmonary bypass in a child with unsuspected duchenne muscular dystrophy. Anesth Analg 2005, 100(3):672-4, table of contents.
77. McKenney KA, Holman SJ: Delayed postoperative rhabdomyol-ysis in a patient subsequently diagnosed as malignant hyper-thermia susceptible. Anesthesiology 2002, 96(3):764-765. 78. Fierobe L, Nivoche Y, Mantz J, Elalaoui Y, Veber B, Desmonts JM:
Perioperative severe rhabdomyolysis revealing susceptibility to malignant hyperthermia. Anesthesiology 1998, 88(1):263-265. 79. Lehmann-Horn F, Iaizzo PA: Are myotonias and periodic paraly-ses associated with susceptibility to malignant hyperther-mia? Br J Anaesth 1990, 65(5):692-697.
80. Burns AP, Hopkins PM, Hall G, Pusey CD: Rhabdomyolysis and acute renal failure in unsuspected malignant hyperpyrexia. Q J Med 1993, 86(7):431-434.
81. Halsted CH: Pitfalls of genetic testing. New England Journal of Medicine 1996, 334(18):1192-1194.
82. Juengst ET: Genetic testing and the moral dynamics of family life. Public Understanding of Science . Public Understanding of Sci-ence 1999, 8(9):193-207.
83. Burke W, Pinsky LE, Press NA: Categorizing genetic tests to identify their ethical, legal, and social implications. Am J Med Genet 2001, 106(3):233-240.
84. Fisher NL: Cultural and Ethnic Diversity - A guide for Genetics Professionals. 1996.
85. Grover S: The psychological dimension of informed consent: dissonance processes in genetic testing. J Genet Couns 2003,
12(5):389-403.
86. Skene L, Smallwood R: Informed consent: lessons from Aus-tralia. Bmj 2002, 324(7328):39-41.
87. Harper PS: Insurance and genetic testing. Lancet 1993,
341(8839):224-227.
88. Light DW: The practice and ethics of risk-rated health insur-ance. Jama 1992, 267(18):2503-2508.
89. Jacobs LA, Deatrick JA: The individual, the family, and genetic testing. J Prof Nurs 1999, 15(5):313-324.
Publish with BioMed Central and every scientist can read your work free of charge "BioMed Central will be the most significant development for disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
91. Marteau TM, Croyle RT: The new genetics. Psychological responses to genetic testing. Bmj 1998, 316(7132):693-696. 92. Manning BM, Quane KA, Ording H, Urwyler A, Tegazzin V, Lehane M,
O'Halloran J, Hartung E, Giblin LM, Lynch PJ, Vaughan P, Censier K, Bendixen D, Comi G, Heytens L, Monsieurs K, Fagerlund T, Wolz W, Heffron JJ, Muller CR, McCarthy TV: Identification of novel muta-tions in the ryanodine-receptor gene (RYR1) in malignant hyperthermia: genotype-phenotype correlation. Am J Hum Genet 1998, 62(3):599-609.
93. Serfas KD, Bose D, Patel L, Wrogemann K, Phillips MS, MacLennan DH, Greenberg CR: Comparison of the segregation of the RYR1 C1840T mutation with segregation of the caffeine/ halothane contracture test results for malignant hyperther-mia susceptibility in a large Manitoba Mennonite family. Anesthesiology 1996, 84(2):322-329.
94. Denborough MA: Heat stroke and malignant hyperpyrexia. Med J Aust 1982, 1(5):204-205.
95. Gronert GA: Dantrolene in malignant hyperthermia (MH)-susceptible patients with exaggerated exercise stress. Anesthesiology 2000, 93(3):905.
96. Gronert GA, Thompson RL, Onofrio BM: Human malignant hyperthermia: awake episodes and correction by dantro-lene. Anesth Analg 1980, 59(5):377-378.
97. Tobin JR, Jason DR, Challa VR, Nelson TE, Sambuughin N: Malignant hyperthermia and apparent heat stroke. Jama 2001,
286(2):168-169.
98. Ellis FR, Green JH, Campbell IT: Muscle activity, pH and malig-nant hyperthermia. Br J Anaesth 1991, 66(5):535-537.
99. Haggendal J, Jonsson L, Carlsten J: The role of sympathetic activ-ity in initiating malignant hyperthermia. Acta Anaesthesiol Scand
1990, 34(8):677-682.
100. Loscher W, Witte U, Fredow G, Ganter M, Bickhardt K: Pharma-codynamic effects of serotonin (5-HT) receptor ligands in pigs: stimulation of 5-HT2 receptors induces malignant hyperthermia. Naunyn Schmiedebergs Arch Pharmacol 1990,
341(6):483-493.
101. Wappler F, Roewer N, Kochling A, Scholz J, Loscher W, Steinfath M:
Effects of the serotonin2 receptor agonist DOI on skeletal muscle specimens from malignant hyperthermia-susceptible patients. Anesthesiology 1996, 84(6):1280-1287.
102. Isbister GK, Whyte IM: Serotonin toxicity and malignant hyper-thermia: role of 5-HT2 receptors. Br J Anaesth 2002, 88(4):603; author reply 603-4.
103. Wappler F, Fiege M, Schulte am Esch J: Pathophysiological role of the serotonin system in malignant hyperthermia. Br J Anaesth
2001, 87(5):794-798.
104. Yang T, Riehl J, Esteve E, Matthaei KI, Goth S, Allen PD, Pessah IN, Lopez JR: Pharmacologic and functional characterization of malignant hyperthermia in the R163C RyR1 knock-in mouse. Anesthesiology 2006, 105(6):1164-1175.
105. Wappler F, Fiege M, Antz M, Schulte am Esch J: Hemodynamic and metabolic alterations in response to graded exercise in a patient susceptible to malignant hyperthermia. Anesthesiology
2000, 92(1):268-272.
106. Davis M, Brown R, Dickson A, Horton H, James D, Laing N, Marston R, Norgate M, Perlman D, Pollock N, Stowell K: Malignant hyper-thermia associated with exercise-induced rhabdomyolysis or congenital abnormalities and a novel RYR1 mutation in New Zealand and Australian pedigrees. Br J Anaesth 2002,
88(4):508-515.
107. Wappler F, Fiege M, Steinfath M, Agarwal K, Scholz J, Singh S, Mat-schke J, Schulte Am Esch J: Evidence for susceptibility to malig-nant hyperthermia in patients with exercise-induced rhabdomyolysis. Anesthesiology 2001, 94(1):95-100.
108. Grogan H, Hopkins PM: Heat stroke: implications for critical care and anaesthesia. Br J Anaesth 2002, 88(5):700-707. 109. mhreg: www.mhreg.org. .