EXPERIENCE & REASON
Not Everything in the Maxillary Sinus Is Sinusitis:
A Case of a Dentigerous Cyst
Richard Haber, MA, MD, FRCPS
Department of Pediatrics, McGill University, Montreal, Quebec, Canada
The author has indicated he has no financial relationships relevant to this article to disclose.
ABSTRACT
A 4-year-old girl presented to a medical clinic with a painless right facial swelling. The treating physician ordered a radiograph of the sinuses and received a report of “maxillary sinusitis.” After appropriate antibiotic treatment, the facial swelling increased, and the mother took the child to her community pediatrician. After a period of observation and additional imaging, the diagnosis of dentigerous cyst was made. After appropriate surgical intervention, the cyst was removed, and over the ensuing 6 weeks the facial swelling gradually diminished. Dentigerous cysts, although uncommon, need to be considered in the differential diagnosis of children with painless facial swelling.
T
HIS CASE REPORTis one of the very few in the pedi-atric medical literature that remind us that not ev-erything in the maxillary sinus is acute sinusitis. Because dentigerous cysts are rarely reported in the pediatric medical literature, the purpose of this report is to alert pediatricians to their possibility in children with facial swelling.CASE REPORT
A 4-year-old girl presented to a medical clinic because of a slight right facial swelling. Although there was no fever or sinus tenderness, the attending physician or-dered sinus films and the radiologist reported “acute bilateral maxillary and right ethmoid sinusitis . . . the facial bones are radiologically normal.” A 10-day course of cefprozil (250 mg twice daily) was pre-scribed. Two months later, the child presented to her pediatrician because of a sore right ear, and a diagnosis of otitis media was made; the child was treated with a 3-day course of azithromycin. At the visit, the mother expressed concern that there was still some facial swelling overlying the right maxillary sinus. Physical examination revealed a slight right facial swelling, which was nontender and firm, with no warmth, fluc-tuation, or discoloration of the overlying skin. The child was afebrile, and the rest of her physical exam-ination was within normal limits. The physician de-cided to observe her. Six weeks later, the mother called because she was alarmed that the facial swelling was increasing. On examination, her physician noted that the right facial swelling was indeed increasing, and there was some watery discharge from the right eye with no conjunctival injection or redness (Fig 1). Again, the swelling was found to be painless, with no warmth, fluctuation, or discoloration overlying it. The
swelling felt firm and “bony.” The child underwent additional imaging (Figs 2– 4). The radiologic diagnosis was 2 large dentigerous cysts each associated with dental structures. A surgical procedure was performed (Caldwell-Luc excision of cyst and right functional endoscopic sinus surgery, as well as maxillary
antros-tomy). A cyst-like mass measuring 6.0⫻6.0⫻0.5 cm
was excised, along with 2 aberrant tooth-like struc-tures. Multiple sections revealed a cyst lined by a nonkeratinized layer of stratified squamous epithe-lium (Fig 5). Also present were small tooth-like struc-tures consisting of enamel, dentin, and dental follicle (Fig 6). Therefore, the final diagnosis was a dentiger-ous cyst arising from an odontoma. The child did well postoperatively, and 6 weeks after the procedure, the facial swelling had decreased considerably. A repeat computed tomography scan has shown no recurrence of the dentigerous cyst. Eighteen months later, there was no recurrence, and there has been complete res-olution of the facial swelling.
DISCUSSION
Dentigerous cysts are not usually aggressive. In this child, however, the lesion was quite aggressive, elevat-ing the orbital floor and depresselevat-ing the hard palate (Fig 2). This raises the issue of more serious diagnoses, in-cluding ameloblastoma and odontogenic keratocyst.
Ameloblastoma is rare in the pediatric age range, and in a classic review of 1036 cases of ameloblastoma, the
Key Words:ambulatory care, community pediatrics, diagnostic errors, sinus disease
www.pediatrics.org/cgi/doi/10.1542/peds.2006-1940
doi:10.1542/peds.2006-1940
Accepted for publication Jun 24, 2007
average age was 38.9 years. Ameloblastoma occurs rarely in the maxilla (7% of pediatric cases), with most occurring in the mandible either at the angle of the mandible or the symphysis. The majority of these cases present radiologically as a dentigerous cyst, and it is necessary to examine the lining of the cyst to make the correct diagnosis. This is important, because the treat-ment is different, if controversial, in children, with some oral surgeons recommending radical resection to
pre-vent recurrence.1 A unicystic ameloblastoma may
present, like in our subject, but the histologic features did not support the diagnosis. Ameloblasts present were associated with enamel formation (Fig 5).
The odontogenic keratocyst is a result of a cystic change within the enamel organ before calcification, and expansion of this lesion results from rapid proliferation
of the squamous epithelial lining and not from the ac-cumulation of fluid as in a dentigerous cyst. This is an aggressive lesion, and recurrence is common.
In this patient, histologic examination confirmed the diagnosis of an odontoma, which is a radiolucent lesion consisting of multiple tiny, malformed, tooth-like structures in various stages of development. Usu-ally this is a slow-growing lesion, but in our patient, it was associated with a follicular or dentigerous cyst, which arose from 1 of these tooth-like structures in the odontoma (Fig 6).
Dentigerous cysts in a child are extremely uncom-mon. A dentigerous cyst is a “benign expansive lesion derived from hydrostatic expansion of a dental follicle
and surrounds the crown of an unerupted tooth.”2In
our patient, the tooth remained close to the alveolar
FIGURE 1
bone with the cyst extending upward. One usually expects to see the tooth at the superior part of the cyst as the cyst develops between the crown and the epi-thelium pushing the tooth upward (Fig 3). The typical dentigerous cyst arises from the enamel organ after amelogenesis is finished and is a result of the accumu-lation of fluid between the crown and the enamel
organ pushing the crown away from the alveolar bone. Dentigerous cysts are associated with unerupted teeth and are usually found by the dentist during routine dental radiology.
Dentigerous cysts accounted for 14% to 20% of all jaw cysts referred to oral surgeons in 1 series; of the 40
referred, 14 cysts were in children ⱕ12 years of age.
Most are found in the mandible.3 Another series from
Brazil reviewing 2356 oral biopsies of patientsⱕ14 years
of age over a 15-year period revealed that 6.5% had
dentigerous cysts.4Dentigerous cysts, especially bilateral
or multiple, have been reported in patients with basal cell nevus syndrome, mucopolysaccharidosis, and clei-docranial dysplasia; they have also been associated with
FIGURE 3
Computed tomography scan showing abnormal tooth (black arrow) with attenuated bony septum and normal tooth on the left (white arrow).
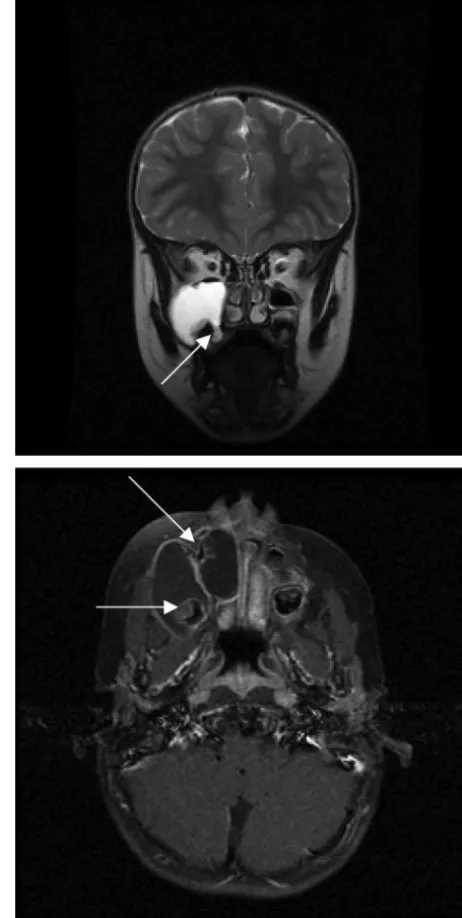
FIGURE 2
Two large expansile cystic lesions are seen within the right facial region occluding the ostiomeatal complex, obliterating the maxillary antrum, elevating the orbital floor, and depressing the hard palate (white arrows). Note the thin bony plate representing floor of maxillary sinus between the cystic expansile lesion and the maxillary antrum of 1 of the cysts (black arrow).
FIGURE 4
cyclosporine use and calcium channel blockers.3 Treat-ment is always surgical, requiring excision and patho-logic examination to rule out other more aggressive lesions.5,6
CONCLUSIONS
Our patient presented with a painless right facial swelling initially felt to be an acute sinusitis. Over a period of several
weeks, the expanding lesion in the right maxillary sinus, with additional imaging and histologic examination, re-vealed itself to be a dentigerous or follicular cyst associated with an odontoma. Although dentigerous cysts are more often found in the mandible, they may occur, as in our patient, in the maxilla. Histologic examination of the cyst lining is essential to differentiate this relatively benign le-sion from a more aggressive lele-sion, such as an
ameloblas-FIGURE 5
Medium-power view of cyst lining consist-ing of nonkeratinized stratified squamous epithelium (hematoxylin and eosin stain; original magnification:⫻200).
FIGURE 6
Low-power view of a tooth-like structure consisting of enamel and dentin (hematox-ylin and eosin stain; original magnification:
toma or an odontogenic keratocyst, both of which require aggressive resection to prevent recurrence. Most reports of dentigerous cysts are found in the surgical literature (den-tal, oral/facial, or otolaryngology), with no reports in the general pediatric literature. Our patient is a reminder to general pediatricians to include the dentigerous cyst in the differential diagnosis of painless facial swelling.
ACKNOWLEDGMENT
I acknowledge the assistance of Dr Peter Chauvin, associate professor and director of the Division of Oral Diagnostic Sciences, Faculty of Dentistry, McGill Uni-versity, for providing the histology slides and their descriptive text.
REFERENCES
1. Ord RA, Blanchaert RH, Nikitakis NG, Sauk JJ. Ameloblastoma in children.J Oral Maxillofac Surg.2002;60:762–770
2. Mehra P, Murad H. Maxillary sinus disease of odontogenic origin.Otolaryngol Clin N Am.2004;37:347–364
3. Ustuner E, Fitoz, S, Atasoy C, Erden I, Akyar S. Builateral maxillary dentigerous cysts: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.2003;95:632– 635
4. Sousa FB, Etges A, Correa L, Mesquita RA, de Araujo NS. Pediatric oral lesions: a 15 year review from Sao Paulo, Brazil. J Clin Pediatr Dent.2002;26:413– 418
5. Motamedi MHK, Talesh, KT. Management of extensive denti-gerous cysts.Br Dent J.2005;198:203–206
DOI: 10.1542/peds.2006-1940
2008;121;e203
Pediatrics
Richard Haber
Not Everything in the Maxillary Sinus Is Sinusitis: A Case of a Dentigerous Cyst
Services
Updated Information &
http://pediatrics.aappublications.org/content/121/1/e203
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/121/1/e203#BIBL
This article cites 6 articles, 0 of which you can access for free at:
Subspecialty Collections
ub
http://www.aappublications.org/cgi/collection/dentistry:oral_health_s
Dentistry/Oral Health following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2006-1940
2008;121;e203
Pediatrics
Richard Haber
Not Everything in the Maxillary Sinus Is Sinusitis: A Case of a Dentigerous Cyst
http://pediatrics.aappublications.org/content/121/1/e203
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.