Lung Function at 8 and 16 Years
After Moderate-to-Late Preterm
Birth: A Prospective Cohort Study
Per Thunqvist, MD, a, b Per M. Gustafsson, MD, PhD, c, d Erica S. Schultz, MD, e Tom Bellander, PhD, e, f Eva Berggren-Broström,
MD, PhD, a, b Mikael Norman, MD, PhD, g, h Magnus Wickman, MD, PhD, a, e Erik Melén, MD, PhD, a, e Jenny Hallberg, PhDa, e
abstract
BACKGROUND AND OBJECTIVE: Knowledge regarding lung function after moderately preterm birthis limited. We therefore investigated lung function at early school age and adolescence among children born moderately preterm.
METHODS: Data were used from the Swedish prospective birth cohort BAMSE (Swedish abbreviation for Children, Allergy, Milieu, Stockholm, Epidemiology study; N = 4089), with a 4.8% prevalence of moderate to late preterm birth defined as a gestational age of 32 to 36 weeks. Participants underwent spirometry at ages 8 and 16 years, and impulse oscillometry additionally at age 16 years. In total, 2621 children (149 preterm and 2472 term) provided lung function data.
RESULTS: At age 8 years, adjusted forced expiratory volume in 1 second was lower in preterm female subjects (–64 mL [95% confidence interval (CI): –118 to –10]) compared with term female subjects but not in preterm male subjects. At age 16 years, both genders in the preterm group demonstrated lower forced expiratory volume in 1 second (female subjects: –116 mL [95% CI: –212 to –20]; male subjects: –177 mL [95% CI: –329 to –25]) compared with the term group. For the preterm group, impulse oscillometry demonstrated higher adjusted resistance at 5 Hz (female subjects: 31.3 Pa·L–1·s−1 [95% CI: 6.3 to 56.3]; male
subjects: 34.9 Pa·L–1·s−1 [95% CI: 12.0 to 57.7]) and frequency dependence of resistance
(resistance at 5 and 20 Hz) for male subjects (20.9 Pa·L–1·s−1 [95% CI: 9.8 to 31.9]) compared
with the term group.
CONCLUSIONS: Measures of airway function assessed in adolescence were reduced in children born moderate to late preterm, and no catch-up in lung function between ages 8 and 16 years was observed.
aDepartment of Pediatrics, Sachs' Children and Youth Hospital, Stockholm, Sweden; Departments of bClinical
Science and Education, and gClinical Science, Intervention and Technology, and eInstitute of Environmental
Medicine, Karolinska Institutet, Stockholm, Sweden; cThe Sahlgrenska Academy at the University of Gothenburg,
Gothenburg, Sweden; dDepartment of Pediatrics, Central Hospital, Skövde, Sweden; fCentre for Occupational and
Environmental Medicine, Stockholm County Council, Stockholm, Sweden; and hDepartment of Neonatal Medicine
K78, Karolinska University Hospital, Stockholm, Sweden
Drs Thunqvist and Hallberg were responsible for the hypothesis generation, study design, data acquisition, analysis, interpretation, and article writing; Dr Gustafsson was responsible for the analysis, interpretation, and article writing; Dr Schultz was responsible for data acquisition, analysis, and interpretation; Dr Bellander was responsible for hypothesis generation, study design, and interpretation; Drs Berggren-Broström and Norman were responsible for the hypothesis generation, analysis, and interpretation; Dr Wickman was responsible for study design, analysis, and interpretation; Dr Melén was responsible for hypothesis generation, study design, analysis, interpretation, and article writing; and all authors drafted, reviewed, and gave fi nal approval to the manuscript as submitted.
The funding sources had no role in planning, conducting or the interpretation of this study. DOI: 10.1542/peds.2015-2056
To cite: Thunqvist P, Gustafsson PM, Schultz ES, et al. Lung Function at 8 and 16 Years After Moderate-to-Late Preterm Birth: A Prospective Cohort Study. Pediatrics. 2016;137(4):e20152056
WHAT’S KNOWN ON THIS SUBJECT: Moderate to late preterm birth (ie, at 32–36 weeks’ gestation) is associated with increased risk of reduced lung function during childhood. Follow-up reports in adolescence and adulthood are sparse but have indicated normalization of airway function.
Infants born preterm (ie, before 37 weeks’ gestation) will exhibit different stages of respiratory immaturity at birth, including incomplete deposition of the parenchymal elastic network of the lungs, as well as acute respiratory morbidity.1, 2 Following increased
survival after preterm birth, long-term lung recovery and health have become important issues. Most follow-up studies on lung function have focused on subjects born very preterm (ie, born at <32 weeks’ gestation). Far less is known about lung function in children born moderate to late preterm (ie, at 32–36 weeks’ gestation). This group constitutes the vast majority of preterm deliveries, with birth rates ∼10% worldwide, ranging from 5% to 15%; only 1% to 2% are born very preterm.3, 4
Available studies on moderate to late prematurity in relation to airway obstruction in infants and toddlers report increased respiratory morbidity during early childhood.5–11 Few studies
are available on lung function at school age and adolescence in this group, however, and the results are somewhat conflicting.12, 13
Furthermore, although spirometry is a well-established method to assess lung function by measuring expiratory flow rates and volumes, other lung function techniques aiming to assess peripheral airway function and mechanics, such as forced oscillation, have been shown to be more sensitive than spirometry for detection of airway obstruction in children with lung disease, including follow-up studies of children born very preterm.14–18
We hypothesized that being born moderate to late preterm would have a negative effect on lung function through childhood and adolescence. Therefore, the aim of the present study was to determine associations between moderate to late preterm birth and various aspects of later
lung function (measured by using spirometry at ages 8 and 16 years, and by using impulse oscillometry [IOS] at 16 years) with data from a large, prospective birth cohort.
METHODS
Study Design and Study Subjects
The BAMSE (Swedish abbreviation for Children, Allergy, Milieu, Stockholm, Epidemiology) study is a prospective birth cohort that included 4089 Swedish children.19
Parents of all infants born between 1994 and 1996 in predefined areas of Stockholm (including inner city, urban, and suburban districts) were asked to participate in the study. The original cohort consists of 75% of eligible children. Exclusion criteria were: the family planned to move within 1 year of the study start; insufficient knowledge of the Swedish language; the family had a seriously ill child; or an older sister or brother was already included in the study. Data on detailed residential characteristics, environmental factors, and allergic heredity were collected from the parental questionnaires when the children were ∼2 months of age (time of inclusion). At age 8 and 16 years, all subjects were invited to attend a follow-up visit, including lung function measurements. The Supplemental Information provide additional details.
Registry Data and Defi nition of Gestational Groups
Gestational age (GA) in complete weeks was obtained from the Swedish Medical Birth Registry or, when registry data were not available, by parental reporting. GA was categorized into 2 groups: moderate to late preterm (32–36 weeks) and term (37–41 weeks).
Small for GA was defined as birth weight ≥2 SDs below the mean according to a Swedish gender- and
GA-specific reference for normal fetal growth.20
Defi nition of Respiratory Symptoms
Asthma was defined as fulfilling at least 2 of the following 3 criteria: (1) symptoms of wheeze during the 12-month period before the date of questionnaire; (2) physician-diagnosed asthma (from birth to the date of the questionnaire); and (3) asthma medication taken occasionally or regularly during the past 12 months before the date of the questionnaire.21 Wheeze was defined
as at least 1 episode of wheeze during the 12 months before the date of the questionnaire.
Measurements of Lung Function
At 8 years of age, patients underwent lung function testing, performed by using the 2200 Pulmonary Function Laboratory (SensorMedics, Anaheim, CA), and at 16 years of age, using the Jaeger MasterScreen–IOS system (Carefusion Technologies, San Diego, CA).22 At both occasions, spirometry
was performed according to
American Thoracic Society/European Respiratory Society criteria.23 The
highest values of forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) were used for analysis. FEV1/FVC ratios were expressed as percentages. Mid-expiratory flow rate was extracted from the curve with the highest sum of FEV1 and FVC.
At 16 years, lung function was further assessed according to IOS.24
The IOS system has been described in detail elsewhere, 25–27 and a
examination by visual inspection of the waveforms. Given that coherence, which is a measure of testing
reliability, was >0.80 at 10 Hz, the mean value of resistance at 5 Hz (R5), resistance at 20 Hz (R20), frequency dependence of resistance (ie, R5–20), and reactance area (AX) were used for analysis. AX may boost the assessed response inappropriately compared with the R5–20 response because it multiplies 2 partly
independent reactions of the airways. We therefore “linearized” AX by reporting its square root as well (ie, AX0.5). The spirometer was calibrated
each day by using a 3-L precision syringe. The IOS system was checked for accuracy daily using a reference resistance (0.20 kPa·L−1·s−1).
Statistical Analysis
Demographic data were compared between groups of children by using Student’s t tests or the Pearson χ2
test. The associations between term/ preterm groups and spirometry variables were assessed by using linear regression analysis for male and female subjects separately, adjusting for age and height at the time of measurement. The mother’s smoking habits during pregnancy and the first months of the child’s life, small for GA, socioeconomic status, allergic heredity, air pollution exposure (particulate matter with aerodynamic diameter <10 μm and nitrogen oxides)28 in the first
year of life, BMI, pubertal staging, and personal smoking at 16 years were evaluated as confounders. The associations between preterm birth and z scores of FEV1 according to the Global Lung Initiative reference values were also evaluated.29
The distribution of the IOS values was skewed to the right. Quantile regression, 30, 31 also called regression
on the median, was used to estimate associations between prematurity and IOS variables while adjusting for height, age, and maternal smoking in male and female subjects separately.
This regression method is more robust to outliers or skewness of the distribution of the dependent variable than ordinary regression on the mean. The interpretation of the quantile regression coefficients is similar to that of linear regression, except that the parameter describes the difference in the medians, rather than means.
To assess the importance of preterm birth on the change in lung function over time (ie, from 8 to 16 years of age), lung function was assessed longitudinally by using a general estimating equations model. Time-dependent covariates included in the model were height and age. Term/preterm birth group, gender, and maternal smoking were fixed covariates. To assess the change over time, a preterm/term group– by–time interaction term was used. A significant interaction term would indicate that the change over time was different in the preterm group compared with the term group. Analyses were performed by using Stata version 12.1 (Stata Corp LP, College Station, TX).
Ethics
The BAMSE study was approved by the ethical committee of Karolinska Institutet (Stockholm, Sweden). All
parents provided consent for their child to participate in the study.
RESULTS
Overall, 222 subjects (5.4%) in the original BAMSE cohort (N = 4089) were reportedly born preterm, and 198 subjects (4.8%) were born moderate to late preterm (32–36 weeks’ gestation). The term (control) group consisted of 3494 (85% of total cohort) children born in gestational weeks 37 through 41. An overview of the participants and number of successful lung function test results in each group tests is presented in Fig 1 and the Supplemental Information. With respect to population
characteristics, the group of children who provided lung function data did not differ to any major extent from the original BAMSE cohort (Supplemental Table 4).
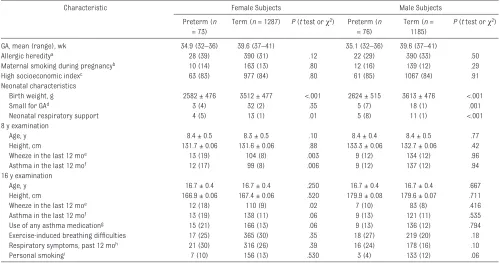
Characteristics of term and moderate to late preterm children are
presented in Table 1. The moderate to late preterm groups required more respiratory support in the neonatal period than those born at term. Small for GA was more common among the moderate to late preterm male subjects. Wheeze at 8 and 16 years, and asthma at 8 years, was reported more often among children born
FIGURE 1
moderate to late preterm compared with term female children.
Lung Function After Moderate to Late Preterm Birth
Unadjusted lung function values and z scores are presented in Supplemental Table 5. The z scores obtained with the Global Lung Initiative reference equations were outside the expected range at 8 years (mean ± SD z score in the term group: 0.50 ± 0.94 for female subjects, 0.36 ± 0.93 for male subjects) but showed a good fit at 16 years (mean: –0.01 ± 0.88 for female subjects and –0.01 ± 0.95 for male subjects).
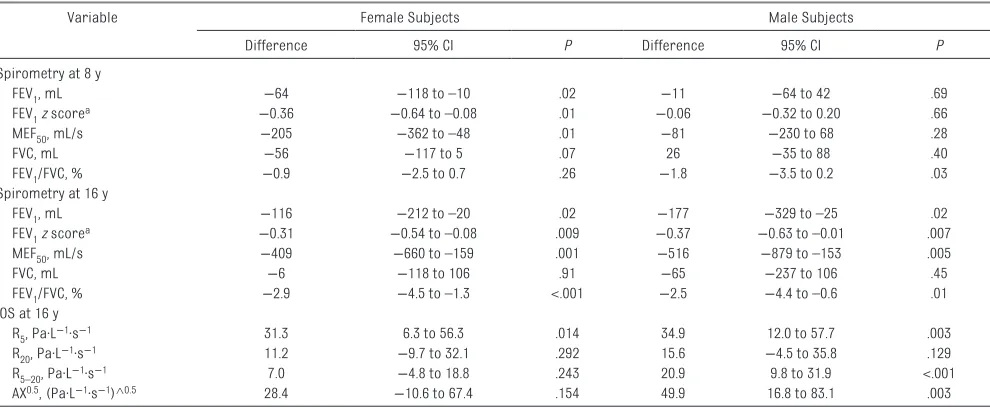
Lung function differences between moderate to late preterm and term children adjusted for height, age, the mother’s smoking habits during
pregnancy, and the first months of the child’s life are presented according to gender as differences in absolute values in Table 2. Small for GA, socioeconomic status, allergic heredity, air pollution exposure (particulate matter with aerodynamic diameter <10 μm and nitrogen oxides) in the first year of life, BMI, pubertal staging, and personal smoking at 16 years were evaluated as potential confounders. These variables showed no such effects, however, and were therefore not included in the final models. At 8 years of age, moderate to late preterm birth was associated with lower FEV1 (–64 mL [95% CI: –118 to –10] or –3.8%), mid-expiratory flow rate, and FEV1/FVC (–0.9% [95% CI: –2.5 to 0.7]) in female subjects
compared with the term group. For male subjects, the corresponding value for FEV1/FVC was –1.8% (95% CI: –3.5 to 0.2). At 16 years, negative associations between preterm birth and all spirometric indices except FVC were observed for both genders. In male subjects, FEV1 demonstrated a reduction of –177 mL (95% CI: –329 to –25), or –4.0%, for the moderate to late preterm group compared with term control subjects. In female subjects, the corresponding number was –116 mL (95% CI: –212 to –20) or –3.4%. Expressed as z scores using the Global Lung Initiative reference values for FEV1, the corresponding differences between moderate to late and term groups were, at 8 years, as follows: z scores of –0.36 (95% CI: TABLE 1 Characteristics of Term and Preterm Adolescents Who Contributed With Lung Function Data at 8 and/or 16 Years, According to Gender (N = 2621)
Characteristic Female Subjects Male Subjects
Preterm (n = 73)
Term (n = 1287) P (t test or χ2) Preterm (n
= 76)
Term (n = 1185)
P (t test or χ2)
GA, mean (range), wk 34.9 (32–36) 39.6 (37–41) 35.1 (32–36) 39.6 (37–41)
Allergic hereditya 28 (39) 390 (31) .12 22 (29) 390 (33) .50
Maternal smoking during pregnancyb 10 (14) 163 (13) .80 12 (16) 139 (12) .29
High socioeconomic indexc 63 (83) 977 (84) .80 61 (85) 1067 (84) .91
Neonatal characteristics
Birth weight, g 2582 ± 476 3512 ± 477 <.001 2624 ± 515 3613 ± 476 <.001
Small for GAd 3 (4) 32 (2) .35 5 (7) 18 (1) .001
Neonatal respiratory support 4 (5) 13 (1) .01 5 (8) 11 (1) <.001
8 y examination
Age, y 8.4 ± 0.5 8.3 ± 0.5 .10 8.4 ± 0.4 8.4 ± 0.5 .77
Height, cm 131.7 ± 0.06 131.6 ± 0.06 .88 133.3 ± 0.06 132.7 ± 0.06 .42
Wheeze in the last 12 moe 13 (19) 104 (8) .003 9 (12) 134 (12) .96
Asthma in the last 12 mof 12 (17) 99 (8) .006 9 (12) 137 (12) .94
16 y examination
Age, y 16.7 ± 0.4 16.7 ± 0.4 .250 16.7 ± 0.4 16.7 ± 0.4 .667
Height, cm 166.9 ± 0.06 167.4 ± 0.06 .520 179.9 ± 0.08 179.6 ± 0.07 .711
Wheeze in the last 12 moe 12 (18) 110 (9) .02 7 (10) 83 (8) .416
Asthma in the last 12 mof 13 (19) 138 (11) .06 9 (13) 121 (11) .535
Use of any asthma medicationg 15 (21) 166 (13) .06 9 (13) 136 (12) .794
Exercise-induced breathing diffi culties 17 (25) 365 (30) .35 18 (27) 219 (20) .18
Respiratory symptoms, past 12 moh 21 (30) 316 (26) .39 16 (24) 178 (16) .10
Personal smokingi 7 (10) 156 (13) .530 3 (4) 133 (12) .06
Unless otherwise indicated, data are presented as n (%) or mean ± SD.
a Mother and/or father with physician-diagnosed asthma and asthma medication and/or physician-diagnosed hay fever in combination with furred pet allergy and/or pollen allergy at the
time of baseline questionnaire.
b The mother smoked at least 1 cigarette per day at the time of basline questionnaire and/or smoked at least 1 cigarette per day in any point of time during the pregnancy.
c Socioeconomic index at birth for the household according to dominance order in 2 classes (low: blue collar vs. high: white collar worker).
d Indicates birth weight less than –2 SDs of the Swedish standard population.20
e Defi ned as at least 1 episode of wheeze during the 12 months before the date of the questionnaire.
f Defi ned as fulfi lling at least 2 of the following 3 criteria: (1) symptoms of wheeze during the 12-month period before the date of the questionnaire; (2) physician-diagnosed asthma (from
birth to the date of the questionnaire); and (3) asthma medication taken occasionally or regularly during the past 12 months before the date of the questionnaire.
g Regular or periodic use of short-acting β-agonists, inhaled corticosteroids, combination therapies, and/or leukotriene antagonists in the last 12 months. h Diffi culty breathing, chest tightness, wheezing, or raspy breathing.
–0.64 to –0.08) for female subjects and –0.06 (95% CI: –0.32 to 0.20) for male subjects. At 16 years of age, the corresponding numbers were –0.37 (95% CI: –0.63 to –0.10) for male subjects and –0.31 (95% CI: –0.54 to –0.08) for female subjects. However, no significant interactions between gender and preterm group were found for any of the lung function variables (Supplemental Table 6).
The proportion of subjects with an FEV1 below the lower limit of normal (z score: less than –1.64) was significantly larger in male subjects in the moderate to late preterm group compared with the term group (14.9% vs 3.7% [χ2 test for
difference, P < .001]), whereas the corresponding difference was smaller for female subjects (5.0% vs 2.3%; P = .19). Given the unsatisfactory fit of data observed at 8 years, proportions were not assessed for this time point.
The IOS results at age 16 years revealed significantly higher estimated medians for R5, R5–20, and AX0.5 in moderate to late preterm
male subjects compared with term male subjects (Table 2). Although a similar trend was seen for female
subjects, a significant difference was recorded only for R5.
To evaluate if the observed differences were driven by individuals with asthma or very low lung function in the preterm group, an analysis was performed excluding individuals who fulfilled the asthma criteria or had z scores of FEV1 less than –1.96 at age 16 years. The negative association for FEV1 between preterm birth and lung function at 16 years remained present for the nonasthmatic individuals: –185 mL (95% CI: –346 to –24) for male subjects, and –120 mL (95% CI: –226 to –14) for female subjects. Few subjects (moderate to late preterm, n = 5 [4.75%]; term, n = 269 [1.5%]; χ2 test for difference, P = .012) presented with z scores less than –1.96. After excluding these subjects, however, the mean group z scores remained lower for the preterm groups compared with the term groups, although statistical significance was only reached for female subjects (z score for female subjects, –0.24 [95% CI: –0.47 to –0.01]; z score for male subjects, –0.22 [95% CI: –0.5 to 0.06]).
Lung Function From Age 8 to 16 Years
To compare how the levels of lung function changed over time in the moderate to late preterm and term groups, a general estimating equations model with an interaction term between the moderate to late preterm/term group and period (ie, 8- or 16-year follow-up) was used. There was an increasingly negative trend over time for FEV1 in preterm male subjects compared with term male subjects (–185 mL [95% CI: –320 to –51]) or FEV1z score (–0.3 [95% CI: –0.58 to –0.03]). In female subjects, there was a further negative effect seen on FEV1/FVC for female subjects born moderate to late compared with those born term (–1.74% [95% CI: –3.3 to –0.2]) (Table 3).
DISCUSSION
In this large prospective longitudinal birth cohort study, we found that subjects born moderate to late preterm had lower lung function as measured by spirometry at 8 and 16 years of age compared with children born term. We found no evidence of TABLE 2 Differences in Adjusted Lung Function Between Moderate to Late Preterm and Term Groups (Adjusting for Maternal Smoking During Pregnancy
and Height and Age at Examination)
Variable Female Subjects Male Subjects
Difference 95% CI P Difference 95% CI P
Spirometry at 8 y
FEV1, mL −64 −118 to –10 .02 −11 −64 to 42 .69
FEV1z scorea −0.36 −0.64 to –0.08 .01 −0.06 −0.32 to 0.20 .66
MEF50, mL/s −205 −362 to –48 .01 −81 −230 to 68 .28
FVC, mL −56 −117 to 5 .07 26 −35 to 88 .40
FEV1/FVC, % −0.9 −2.5 to 0.7 .26 −1.8 −3.5 to 0.2 .03
Spirometry at 16 y
FEV1, mL −116 −212 to –20 .02 −177 −329 to –25 .02
FEV1z scorea −0.31 −0.54 to –0.08 .009 −0.37 −0.63 to –0.01 .007
MEF50, mL/s −409 −660 to –159 .001 −516 −879 to –153 .005
FVC, mL −6 −118 to 106 .91 −65 −237 to 106 .45
FEV1/FVC, % −2.9 −4.5 to –1.3 <.001 −2.5 −4.4 to –0.6 .01
IOS at 16 y
R5, Pa·L−1·s−1 31.3 6.3 to 56.3 .014 34.9 12.0 to 57.7 .003
R20, Pa·L−1·s−1 11.2 −9.7 to 32.1 .292 15.6 −4.5 to 35.8 .129
R5–20, Pa·L−1·s−1 7.0 −4.8 to 18.8 .243 20.9 9.8 to 31.9 <.001
AX0.5, (Pa·L−1·s−1)^0.5 28.4 −10.6 to 67.4 .154 49.9 16.8 to 83.1 .003
Spirometry data were analyzed by linear regression on the mean and IOS data by linear regression on the median. P values were obtained from the regression models. MEF50,
mid-expiratory fl ow rate.
catch-up in spirometric indices for either gender from school age until adolescence; the negative effects were instead augmented between age 8 and 16 years in male subjects. IOS measures at age 16 years confirmed the negative effects on airway function and further indicated possible small airway involvement, particularly in male subjects born moderate to late preterm. As a clinical measure, we found that female subjects born moderate to late preterm report respiratory wheeze and asthma symptoms and tend to use asthma medications more often compared with term female subjects.
Although reports of lung function at school age and adolescence are sparse in subjects born moderate to late preterm, a study by Kotecha et al12 reported similar results as in our
study, with significantly lower lung function at 8 to 9 years of age for children born after 33 to 34 weeks of gestation, compared with term control subjects. However, they found no significant negative effects among those born after 35 to 36 weeks of gestation. When assessing lung function over time, the investigators reported significant increases in FEV1z scores from age 8–9 years to 14–17 years in the 33- to 34-week GA subgroup, and no significant changes in those born after 35 to 36 weeks of gestation. Nevertheless, the FEV1/ FVC ratios were consistently lower in the 33- to 34-week subgroup compared with the control subjects, which is in line with our findings of
a persisting negative effect of late premature birth on airway function. Narang et al13 reported reduced
expiratory flow rates (measured as FEV at 0.75 second) at 7 to 9 years of age in a study of children born from 27 to 37 weeks’ gestation, but no differences between the study group and control subjects for FEV1 in adulthood were reported. It should be noted that this study group primarily included children with low birth weight (<2000 g) who were born ∼15 years before our cohort was initiated, which makes direct comparisons difficult due to population differences. Hence, although all studies reported reduced lung function at school age in individuals born moderate to late preterm, the potential for catch-up growth seems less certain.
The results from the IOS recordings performed in the present study at age 16 years confirm the negative effect of moderate to late prematurity on airway function observed using spirometry findings. Increases in frequency dependency of resistance (ie, R5–20) and AX have been suggested as indicating increased peripheral airway involvement. This outcome was observed only among preterm male subjects in the present study. Although no significant interactions between preterm birth and gender were found, these results indicate that the preterm male and female groups may differ in the type of impairment, severity of bronchial obstruction,
or other developmental effects on lung tissue. Associations between preterm birth and lung function measured by using IOS, although not gender specific, have previously been reported in follow-up studies on bronchopulmonary dysplasia after very preterm or extremely preterm birth.18, 32, 33 To our knowledge,
no other studies have used IOS or methods other than spirometry to characterize lung function after moderate to late preterm birth.
We also found that female subjects born moderate to late preterm reported more respiratory symptoms at both 8 and 16 years of age than female subjects born term. Positive associations between respiratory symptoms and preterm birth have been previously reported, including 1 study reporting a higher prevalence in female subjects compared with male subjects in young adulthood.6, 7, 34 No significant interactions between
gender and preterm group for any lung function indices were observed; however, the findings that the proportion of preterm adolescents with an FEV1 below the lower limit of normal was more pronounced in male subjects (and symptoms were more pronounced in preterm female subjects) indicate that there is a need for a broader investigation into the origins of the pattern of symptoms after moderate to late preterm birth.
A major strength of the present study is that we used prospective data from a large unselected birth cohort. GA was reported by the TABLE 3 Difference in Mean Adjusted Lung Function Change From 8 to 16 Years of Age Between the Preterm and Term Groups Using a Longitudinal Effects
Model With an Interaction Term Between Term/Preterm Groups and Time
Variable Female Subjects Male Subjects
Difference 95% CI P Difference 95% CI P
FEV1, mL −76 −171 to 18 .11 −185 −320 to –51 .007
FEV1z scorea −0.02 −0.27 to 0.24 .90 −0.30 −0.58 to –0.03 .03
MEF50, mL/s −241 −490 to 9 .06 −494 −809 to -180 .002
FVC, mL 16 −90 to 122 .77 −103 −253 to 47 .18
FEV1/FVC, % −1.74 −3.3 to –0.2 .03 −0.92 −2.7 to 0.8 .30
Time-dependent covariates included in the model were height and age. Term/preterm group was included as a fi xed covariate. In this model, the numbers of subjects contributing data comprised 1272 female subjects and 1149 male subjects (number of observations: 1897 in the female group, 1642 in the male group). P values were obtained from the longitudinal effects model. MEF50, mid-expiratory fl ow rate.
Swedish Medical Birth Registry, and in >90% of the pregnancies, was determined by using ultrasound. The proportion of prematurely born children in the cohort is comparable to other European reports, 3 but it
should be noted that the narrow border between 36+6 days and
37+1 poses a risk of nondifferential
misclassification that would likely result in an underestimation of the true differences in lung function between the groups. Another important point of discussion is loss to follow-up, with only 34% of the original preterm group in the study having undergone spirometry at both occasions. However, follow-up rates were similar in the term group and were also comparable to other studies.12, 13 Examination
after bronchodilation was not performed, making it difficult to exclude increased airway smooth muscle tone disclosed as reversible airway obstruction as the cause of the differing airway function (as opposed to impaired airway growth and development). Nevertheless, because restricting the analysis to those not reporting asthma did not change the main results, reactive airways apparently do not explain the differences seen in lung function between the groups in the present study. In addition, excluding
individuals with FEV1z scores less than –1.96 at 16 years did not change the main results, indicating that the difference between the moderate to late preterm and term groups is not explained by a few subjects with very poor lung function.
At 8 years of age, mean FEV1z scores were not centered at zero, whereas there was a good fit at 16 years. We speculate that this outcome could be due to a slightly different growth pattern during childhood in Swedish children compared with those included in the reference population. Although the effect is likely to be similar for term and preterm children and not affect comparisons between groups, we have refrained from estimating proportions of the population below the lower limit of normality at 8 years of age.
A recent study has suggested that low FEV1 in early adulthood is important in the genesis of chronic obstructive pulmonary disease.35 Concern has
also been raised as to whether chronic lung disease after extremely premature birth is a precursor of a chronic obstructive pulmonary disease–like phenotype later in life, given the markedly reduced airway function in early adulthood shown in this group.36–38 Although our findings
suggest that children born moderate
to late preterm are at risk of reaching adulthood with a modest reduction in lung function, the future clinical importance of these findings remains to be evaluated. Nevertheless, a larger proportion than expected of the moderate to late preterm population had a FEV1 below the lower limit of normal, indicating that this relatively large subgroup of the general population could benefit from lung function follow-up in adulthood.
CONCLUSION
Measures of airway function assessed in adolescence by spirometry and IOS are reduced in females and males born moderate-to-late preterm. Further, there was no catch-up of lung function between 8 and 16 years of age.
REFERENCES
1. Merkus PJ, ten Have-Opbroek AA, Quanjer PH. Human lung growth: a review. Pediatr
Pulmonol. 1996;21(6):
383–397
2. Henschen M, Stocks J, Brookes I, Frey U. New aspects of airway mechanics in pre-term infants.
Eur Respir J. 2006;27(5):
913–920
3. Buitendijk S, Zeitlin J, Cuttini M, Langhoff-Roos J, Bottu J. Indicators of fetal and infant health outcomes.
Eur J Obstet Gynecol Reprod Biol.
2003;111(suppl 1):S66–S77
ABBREVIATIONS
AX: reactance area AX0.5: square root of the
reactance area CI: confidence interval
FEV1: forced expiratory volume in 1 second
FVC: forced vital capacity IOS: impulse oscillometry R5: resistance at 5 Hz R20: resistance at 20 Hz
Accepted for publication Jan 5, 2016
Address correspondence to Per Thunqvist, MD, Sachs' Children and Youth Hospital, Department of Pediatrics, Södersjukhuset, 118 83 Stockholm, Sweden. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2016 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no fi nancial relationships relevant to this article to disclose.
FUNDING: Supported by the Swedish Research Council, the Swedish Heart-Lung Foundation, the Freemason Child House Foundation in Stockholm, the Stockholm County Council, and the Strategic Research Programme in Epidemiology at the Karolinska Institutet.
4. Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications.
Lancet. 2012;379(9832):2162–2172
5. Pulver LS, Guest-Warnick G, Stoddard GJ, Byington CL, Young PC. Weight for gestational age affects the mortality of late preterm infants. Pediatrics. 2009;123(6). Available at: www. pediatrics. org/ cgi/ content/ full/ 123/ 6/ e1072
6. McIntire DD, Leveno KJ. Neonatal mortality and morbidity rates in late preterm births compared with births at term. Obstet Gynecol. 2008;111(1):35–41
7. Been JV, Lugtenberg MJ, Smets E, et al. Preterm birth and childhood wheezing disorders: a systematic review and meta-analysis. PLoS Med. 2014;11(1):e1001596
8. McEvoy C, Venigalla S, Schilling D, Clay N, Spitale P, Nguyen T. Respiratory function in healthy late preterm infants delivered at 33-36 weeks of gestation. J
Pediatr. 2013;162(3):464–469
9. Hoo AF, Dezateux C, Henschen M, Costeloe K, Stocks J. Development of airway function in infancy after preterm delivery. J Pediatr. 2002;141(5):652–658
10. Friedrich L, Pitrez PM, Stein RT, Goldani M, Tepper R, Jones MH. Growth rate of lung function in healthy preterm infants. Am J Respir Crit Care Med. 2007;176(12):1269–1273
11. Kotecha SJ, Edwards MO, Watkins WJ, et al. Effect of preterm birth on later FEV1: a systematic review and meta-analysis. Thorax. 2013;68(8):760–766 12. Kotecha SJ, Watkins WJ, Paranjothy
S, Dunstan FD, Henderson AJ, Kotecha S. Effect of late preterm birth on longitudinal lung spirometry in school age children and adolescents. Thorax. 2012;67(1):54–61
13. Narang I, Rosenthal M, Cremonesini D, Silverman M, Bush A. Longitudinal evaluation of airway function 21 years after preterm birth. Am J Respir Crit
Care Med. 2008;178(1):74–80
14. Quanjer PH, Weiner DJ, Pretto JJ, Brazzale DJ, Boros PW. Measurement
of FEF25-75% and FEF75% does not contribute to clinical decision making.
Eur Respir J. 2014;43(4):1051–1058
15. Stocks J, Hislop A, Sonnappa S. Early lung development: lifelong effect on respiratory health and disease. Lancet
Respir Med. 2013;1(9):728–742
16. Keen C, Olin AC, Wennergren G, Gustafsson P. Small airway function, exhaled NO and airway hyper-responsiveness in paediatric asthma.
Respir Med. 2011;105(10):1476–1484
17. Shi Y, Aledia AS, Tatavoosian AV, Vijayalakshmi S, Galant SP, George SC. Relating small airways to asthma control by using impulse oscillometry in children. J Allergy Clin Immunol. 2012;129(3):671–678
18. Vrijlandt EJ, Boezen HM, Gerritsen J, Stremmelaar EF, Duiverman EJ. Respiratory health in prematurely born preschool children with and without bronchopulmonary dysplasia. J Pediatr.
2007;150(3):256–261
19. Kull I, Melen E, Alm J, et al. Breast-feeding in relation to asthma, lung function, and sensitization in young schoolchildren. J Allergy Clin Immunol. 2010;125(5):1013–1019
20. Marsál K, Persson PH, Larsen T, Lilja H, Selbing A, Sultan B. Intrauterine growth curves based on ultrasonically estimated foetal weights. Acta
Paediatr. 1996;85(7):843–848
21. Pinart M, Benet M, Annesi-Maesano I, et al. Comorbidity of eczema, rhinitis, and asthma in IgE-sensitised and non-IgE-sensitised children in MeDALL: a population-based cohort study. Lancet Respir Med. 2014;2(2):131–140
22. Schultz ES, Hallberg J, Bellander T, et al. Early life exposure to traffi c-related air pollution and lung function in adolescence. Am J Respir Crit Care Med. 2016;193(2):171–177
23. Miller MR, Hankinson J, Brusasco V, et al; ATS/ERS Task Force. Standardisation of spirometry. Eur
Respir J. 2005;26(2):319–338
24. Hallberg J, Thunqvist P, Schultz ES, et al. Asthma phenotypes and lung function up to 16 years of age—the BAMSE cohort. Allergy. 2015;70(6):667–673
25. Malmberg LP, Pelkonen A, Poussa T, Pohianpalo A, Haahtela T, Turpeinen M. Determinants of respiratory system input impedance and bronchodilator response in healthy Finnish preschool children. Clin Physiol Funct Imaging. 2002;22(1):64–71
26. Goldman MD. Clinical application of forced oscillation. Pulm Pharmacol Ther. 2001;14(5):341–350
27. Goldman MD, Saadeh C, Ross D. Clinical applications of forced oscillation to assess peripheral airway function. Respir Physiol Neurobiol. 2005;148(1-2):179–194
28. Schultz ES, Gruzieva O, Bellander T, et al. Traffic-related air pollution and lung function in children at 8 years of age: a birth cohort study. Am J Respir Crit Care Med. 2012;186(12):1286–1291
29. Quanjer PH, Stanojevic S, Cole TJ, et al; ERS Global Lung Function Initiative. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the Global Lung Function 2012 equations. Eur Respir J. 2012;40(6):1324–1343 30. Bottai M, Frongillo EA, Sui X, et
al. Use of quantile regression to investigate the longitudinal association between physical activity and body mass index. Obesity (Silver Spring). 2014;22(5):E149–E156
31. Bottai M, Pistelli F, Di Pede F, et al. Percentiles of inspiratory capacity in healthy nonsmokers: a pilot study. Respiration. 2011;82(3):254–262
32. Broström EB, Thunqvist P, Adenfelt G, Borling E, Katz-Salamon M. Obstructive lung disease in children with mild to severe BPD. Respir Med. 2010;104(3):362–370
33. Malmberg LP, Mieskonen S, Pelkonen A, Kari A, Sovijärvi AR, Turpeinen M. Lung function measured by the oscillometric method in prematurely born children with chronic lung disease. Eur Respir J. 2000;16(4):598–603
34. Vrijlandt EJ, Gerritsen J, Boezen HM, Duiverman EJ; Dutch POPS-19 Collaborative Study Group. Gender differences in respiratory symptoms in 19-year-old adults born preterm.
35. Lange P, Celli B, Agustí A, et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. N Engl
J Med. 2015;373(2):111–122
36. Doyle LW, Faber B, Callanan C, Freezer N, Ford GW, Davis NM. Bronchopulmonary dysplasia in very
low birth weight subjects
and lung function in late adolescence.
Pediatrics. 2006;118(1):
108–113
37. Filippone M, Bonetto G, Cherubin E, Carraro S, Baraldi E. Childhood course of lung function in survivors of
bronchopulmonary dysplasia. JAMA. 2009;302(13):1418–1420
DOI: 10.1542/peds.2015-2056 originally published online March 23, 2016;
2016;137;
Pediatrics
Hallberg
Berggren-Broström, Mikael Norman, Magnus Wickman, Erik Melén and Jenny
Per Thunqvist, Per M. Gustafsson, Erica S. Schultz, Tom Bellander, Eva
Prospective Cohort Study
Lung Function at 8 and 16 Years After Moderate-to-Late Preterm Birth: A
Services
Updated Information &
http://pediatrics.aappublications.org/content/137/4/e20152056 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/137/4/e20152056#BIBL This article cites 37 articles, 10 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/asthma_sub
Asthma
ub
http://www.aappublications.org/cgi/collection/allergy:immunology_s
Allergy/Immunology
http://www.aappublications.org/cgi/collection/pulmonology_sub
Pulmonology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2015-2056 originally published online March 23, 2016;
2016;137;
Pediatrics
Hallberg
Berggren-Broström, Mikael Norman, Magnus Wickman, Erik Melén and Jenny
Per Thunqvist, Per M. Gustafsson, Erica S. Schultz, Tom Bellander, Eva
Prospective Cohort Study
Lung Function at 8 and 16 Years After Moderate-to-Late Preterm Birth: A
http://pediatrics.aappublications.org/content/137/4/e20152056
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2016/03/22/peds.2015-2056.DCSupplemental Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.