A
DAMB
UCIŃSKI1, T
OMASZB
ĄCZEK2, J
ERZYK
RYSIŃSKI3, B
EATAZ
IEMBA4,
E
MILIAF
ILIPCZYK−C
ISARŻ4, M
AŁGORZATAR
YCHLICKA1Evaluation of Selected Prognostic Factors
in Patients with Ovarian Cancer Applying
Artificial Neural Network Analysis*
Analiza wybranych czynników rokowniczych metodą sztucznych sieci
neuronowych u chorych na raka jajnika
1Department of Biopharmacy, Faculty of Pharmacy, CM, Nicolaus Copernicus University, Bydgoszcz, Poland 2Department of Biopharmaceutics and Pharmacodynamics, Medical University of Gdańsk, Poland
3Department of Marketing and Pharmaceutical Law, Faculty of Pharmacy, CM, Nicolaus Copernicus University,
Bydgoszcz, Poland
4Low−Silesian Oncology Center, Wrocław, Poland Adv Clin Exp Med 2007, 16, 4, 527–532
ISSN 1230−025X
ORIGINAL PAPERS
© Copyright by Silesian Piasts University of Medicine in Wrocław
Abstract
Background.Artificial neural network (ANN) analysis, an advanced multivariate data processing method, was demonstrated to provide an objective evaluation of medical strategy by making use of large collections of routine clinical parameters of patients with ovarian cancer. The ANN method allowed the detection of complex systemat− ic relationships between diverse patient, disease, and treatment variables. It was revealed with ANN that it is pos− sible to perform correct classification of patients with regard to their surviving five years after treatment.
Material and Methods. Three hundred twenty patients with ovary cancer were the subjects of the study, for whom thirty−five disease and treatment variables were determined. The patients’ data were distributed into data sets for training (160), validation (80), and testing (80) of the model.
Results.The classification coefficients for the training, validation, and testing data sets were 95.6%, 86.2%, and 86.2%, respectively.
Conclusions.By means of ANN, systematic information which is useful in practice may be extracted from large sets of data otherwise hardly interpretable in comprehensive physical terms. This information can be of value for general prognosis and appropriate adjustment of the treatment (Adv Clin Exp Med 2007, 16, 4, 527–532).
Key words: artificial neural network, ovarian cancer.
Streszczenie
Wprowadzenie.Zaawansowana metoda analizy danych za pomocą sztucznych sieci neuronowych (SNN), zosta− ła zastosowana do obiektywnej oceny skuteczności postępowania terapeutycznego z wykorzystaniem złożonych danych klinicznych dotyczących pacjentów chorych na raka jajnika. Metoda SNN pozwoliła na wykrycie złożo− nych zależności między wskaźnikami charakteryzującymi pacjentów, chorobę i zastosowane postępowanie tera− peutyczne. Wykazano, że SNN umożliwia przeprowadzenie prawidłowej klasyfikacji pacjentów ze względu na ich przeżycie w okresie pięciu lat po wykonaniu danego postępowania terapeutycznego.
Materiał i metody.Przedmiotem analizy z wykorzystaniem sztucznych sieci neuronowych były dane retrospek− tywne dotyczące 320 pacjentek leczonych z powodu raka jajnika, dla których określono 35 zmiennych opisujących stan choroby i postępowania terapeutycznego.
Wyniki.Otrzymano satysfakcjonujące współczynniki klasyfikacji SNN obejmujące grupę danych uczących, wali− dacyjnych i testujących na poziomie odpowiednio 95,6; 86,2 i 86,2%.
Wnioski.Z wykorzystaniem zaprojektowanej SNN otrzymano praktycznie użyteczną informację, analizując złożony zbiór danych, trudnych do interpretacji podczas indywidualnej oceny. Ta informacja może mieć wartość prognostycz− ną podczas ustalania odpowiedniego postępowania terapeutycznego (Adv Clin Exp Med 2007, 16, 4, 527–532).
Słowa kluczowe:sztuczne sieci neuronowe, rak jajnika.
Although the prognosis of patients with ovari− an cancer has improved over the last 20–30 years, it remains a challenging task [1–3]. Five−year sur− vival does not exceed 40% [2–4], which is a reflection of late detection and this can− cer’s propensity to recur despite complete remis− sion after the first treatment [3, 4]. The disease is often diagnosed (up to 80%) [3, 5] in advanced stage because it does not provide any specific symptoms and there are no effective methods enabling early detection [6].
Artificial neural network (ANN) analysis is a sophisticated method of data analysis which is based on emulating the brain’s way of working. Neural networks exhibit the way in which arrays of neurons probably function in biological processes such as learning and memory. ANNs differ from classical computer programs in that they “learn” from a set of examples rather than being programmed to get the right answer. The information is encoded in the strength of the net− work’s “synaptic” connections [7, 8]. In chem− istry and related fields of research, interest in neural−network computing has been noted since 1986 [9, 10]. Because of their ability to mimic a number of relationships, ANNs are also used to process clinical data. Confirmation of this can be found in literature, including ANNs’s usefulness in oncology and studies on tumors [16–22]. ANNs have been proposed as decision support systems in dentistry [11] and urology [12–14] and to assess HIV/AIDS−related health perfor− mance [15].
The goal of this study was to prove that ANN analysis is a convenient and reliable prognostic tool in predicting survival within a five−year peri− od after treatment of ovarian cancer.
Material and Methods
Data on 320 patients with ovarian cancer from 1987–2001 were retrospectively collected and analyzed. The variables considered in this study are presented in Table 1. A total of 35 variables were subjected to ANN analysis. The final matrix of data subjected to ANN analysis was 320 patients times 35 variables.
The degree of advancement of tumor develop− ment was established in each case according to FIGO criteria. In the searching group, the follow− ing degrees were set: 73 patients with degree I, 27 with degree II, 187 with degree III, and 33 with degree IV. The median age was 49 years (range: 22–75 years). All patients were residents of the province of Lower Silesia: 152 from the former Wroclawskie, 42 from the former Jeleniogorskie,
45 from the former Legnickie, and 81 from the for− mer Walbrzyskie voivodeship.
The following treatments were applied after surgery:
1) CP Program: cisplatin/carboplatin + cyclo− phosphamid in 176 patients,
2) CA Program: cisplatin/carboplatin + dox− orubicin + cyclophosphamid in 73 patients,
3) Program with paclitaxel + cisplatin in 71 patients.
The response to treatment was evaluated according to WHO criteria (CR, PR, SD, PD).
ANN Analysis
Artificial neural network analysis was run on a personal computer using STATISTICA NEURAL NETWORKS v.7.1 software (StatSoft, Tulsa, OK, USA). An artificial neural network based on a multilayer perceptron consisting of 35 artificial neurons in the input layer, 12 neurons in the hid− den layer, and 1 neuron in the output layer was used. The architecture of the model utilized is depicted in Figure 1. The method of supervised learning with the back−propagation strategy and conjugate gradient descent method was used [23, 24]. The patient data were divided into three sets: a learning set with 160 patients, a validating set with 80 patients, and a testing set with 80 patients. The learning process was completed when the artificial neural network showed a small− er RMS error with regard to the validating data set. In the case of this network, learning was complet− ed in 1000 epochs by the Back Propagation (BP) method and 11 epochs by the Conjugate Gradient Descent (CGD) method. Data from the learning set were presented in randomized manner during the learning process. The changes in RMS error were recorded for the learning and validating data sets during the learning process (Fig. 1a). For fur− ther considerations, the ANN was taken which showed the least RMS error.
Results
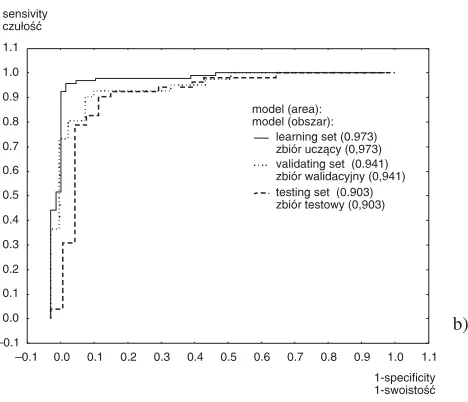
Figure 1 presents the architecture of the ANN model used for predictions of survival within a five−year period after treatment of ovarian cancer based on the input data from the training, validat− ing, and testing data sets. In Table 2, classification statistics are collected for the training, validating, and testing sets. Receiver operating characteristic (ROC) curves are shown on Figure 1b.
Table 1.Variables considered in the analysis by the artificial neural network (ANN)
Tabela 1. Zmienne rozważane w analizie metodą sztucznych sieci neuronowych (SSN)
Variable No. Variable Name Error Rank
(Zmienna nr) (Nazwa zmiennej) (Błąd) (Ranga)
1 Age (years): < 40 (1); 41–50 (2); > 50 (3) 1.013 24
2 Inhabitant of: city > 10000 (1); city < 10000 (2); village (3) 0.997 32
3 Time between the first and the last menstruation – years 0.981 34
4 Menopause: before (1); after (2) 1.064 12
5 Number of births: 0 (1); 1 (2); 2 (3); ≥3 (4) 1.092 6
6 Occurrence of ovarian cancer in the first and second generation: yes (1); no (2) 1.013 23
7 Detection of the second cancer: yes (1); no (2) 0.977 35
8 Professional activity: pensioner (0), employed (1), unemployed (2) 0.997 31 9 Previous voivodeship: wrocławskie (1); jeleniogórskie (2); legnickie (3); 1.076 9
wałbrzyskie (4); other (5)
10 Size of the ovarian tumors/the sum of maximal length: < 10 cm (1); 11–30 cm (2); 1.095 5 total infiltration of pelvis minoris (3)
11 Stage: I (1); II (2); III (3); IV (4) 1.114 3
12 Histology type: serous (1); mucinous (2); endometrious (3); clear−cell (4); 1.014 22 not diversified (5); solid (6); unknown (7)
13 Degree of histological differentiation: G1 (1); G2 (2); G3 (3); not classified (4) 1.040 15
14 OB before chemotherapy 0.998 30
15 OB at the last course 1.124 2
16 Initial Ca 125: normal (1); 35–150 (2); 150–500 (3); 501–1000 (4); > 1000 (5) 1.019 19 17 Ca 125 after 3 courses /decrease of %: normal (1); 0–25% (2); 26–50% (3); 1.067 11
51–75% (4); > 75% (5); increase (6)
18 Ca125 before the last course: normal (1); 35–150 (2); 151–500 (3); > 500 (4); 1.012 25 > 1000 (5)
19 The kind of recurrence: progress (1); increase in Ca125 (2); local recurrence (3); 1.662 1 ascites (4); metastasis (5); Ca125 + recurrence (6); Ca125 + dis. (7); lack (8)
20 The kind of surgery procedure: radical (1); rests < 2 cm (2); 1 without appendix (3); 1.017 21 1 without omemtectomy (4); 1 without 3 and 4 (5); cytoreductive (6);
explorative (7); lack (8)
21 The kind of surgery cut: transversal (1); Phanenstiela (2); lack (3) 1.006 27 22 The kind of the first chemotherapy: CP/Carbo+CTX (1); CAP (2); 1.053 14
paclitaxel + DDP (3)
23 Time from surgery to chemotherapy – weeks 1.024 17
24 Number of courses of the first chemotherapy: 1–3 (1); 4–6 (2); > 6 (3) 1.035 16 25 Response to the first chemotherapy: CR (1); PR (2); SD (3); PD (4) 1.019 20 26 Second chemotherapy after the first surgery: lack (1); ifosfamide (2);
other alkylating agents (2); platinum derivative (3); VP 16 (4); taxane (5); 1.007 26 other (6); RT–Th (7)
27 Result of “second−look” treatment: lack (1); positive (2); negative (3) 1.077 8 28 Chemotherapy after the second surgery: lack (1); CAP (2); CP/Carbo + CTX (3); 1.070 10
other alkylating agents (4); VP16 (5); ifosfamide (6); paclitaxel (7); RT−Th (8)
29 Inductive chemotherapy: yes (1); no (2) 1.053 13
30 Second surgery after chemotherapy: radical (1); cytoreductive (2); explorative (3); 1.101 4 second−look (4); lack (5); further chemotherapy
31 Changes during the second surgery: to remove (1); not to remove (2); lack (3); 1.024 18 without operation (4)
32 Total time of the first treatment – months 0.999 28
33 Achievement of CR in the first treatment: yes (1); no (2) 1.085 7
34 Total time of chemotherapy in the first treatment – months 0.998 29
group as with or without five−year survival with a prognostic potency on the level of more than 82%. The prognostic potency of ANN regarding the set of test patients is reasonably good and proves the appropriate choice and shape of the net− work proposed. Sixty−nine of the 80 patients in the testing set were correctly classified, which means that one is able to predict five−year survival utiliz− ing the selected variables with a high probability of more than 85%.
Parallel with the statistics for ANN analysis, sensitivity analysis for the input variables was also carried out (Table 1). Sensitivity analysis gives insight into the usefulness of individual variables. With this kind of analysis it is possible to judge which parameters are the most significant (with rank close to 1) and the least significant (with rank close to 35) to generate the proposed ANN. According to sensitivity analysis, the kind of recurrence is the most significant parameter distin−
Table 2.Classification statistics
Tabela 2. Statystyki klasyfikacyjne
Statistics Learning set – 5−year survival Validating set – 5−year survival Testing set – 5−year survival (Statystyki) (Zbiór uczący – 5−letni (Zbiór walidacyjny – 5−letni (Zbiór testowy – 5−letni
okres przeżycia) okres przeżycia) okres przeżycia)
yes no yes no yes no
Total
(Suma) 67 93 39 41 28 52
Correct
(Poprawnie) 64 89 35 34 24 45
Incorrect
(Niepoprawnie) 3 4 4 7 4 7
Correct (%)
(Poprawnie %) 95.52 95.70 89.74 82.93 85.71 86.54
Incorrect (%)
(Niepoprawnie %) 4.48 4.30 10.26 17.07 14.29 13.46
Fig. 1. Architecture of the artificial neural network used for predicting five−year survival: a) training Error Graph, b) Receiver Operating Characteristic (ROC) curves for the training, validating, and testing sets
Ryc. 1. Architektura sztucznej sieci neuronowej użytej do przewidywania 5−letniego okresu przeżycia: a) wykres zmiany błędu dla procesu uczenia, b) krzywe ROC dla zbioru uczącego, walidacyjnego i testowego
error błąd learning set zbiór uczący validating set zbiór walidacyjny
0.0 0.1 0.2 0.3 0.4 0.5 0.6 error RMS błąd RMS
0 100 200 300 400 500 600 700 800 900 1000 1100
epoche epoka
–0.1 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 1.1
1−specificity 1−swoistość –0.1
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 1.1
model (area): model (obszar):
learning set (0.973) zbiór uczący (0,973) validating set (0.941) zbiór walidacyjny (0,941) testing set (0.903) zbiór testowy (0,903) sensivity
czułość
guishing patients with and without five−year sur− vival. Highly significant are also OB at the last course of chemotherapy, the degree of advance− ment, and second surgery after chemotherapy. Less significant appear to be the total time of the first treatment, the time between the first and the last menstruation (in years) and the detection of a second cancer.
Discussion
Favorable prognostic factors in ovarian cancer include the degree of disease development, the size of the tumor, the size of residual changes, and the number of births [5]. The results presented in Table 1 confirm these literature data, because high sensitivity coefficients were obtained for these variables. The high sensitivity coefficients obtained for the variables “kind of recurrence”, “OB at the last course”, and “achievement of CR in the first treatment” are obvious from the clinical point of view. The high sensitivity coefficients
obtained for the variables “second surgery after chemotherapy” and “second−look treatment” justi− fy the favorable prognoses of patients treated with second surgery to remove changes remaining after chemotherapy. This also indicates chances to pro− long the lives of patients who failed with the first surgery. A surprisingly high sensitivity coefficient was also obtained for the variable “former voivodeship”. This is probably associated with the fact that patients with good prognosis were noted for the treatment from the former voivodeships of the Lower Silesia Province. Patients with advan− ced disease were given palliative care.
The authors conclude that this study is one of the first applications of ANN to estimate the sur− vival of patients with ovarian cancer. It is largely methodological in character and involves a limited number of cases. It may help in identifying a com− bination of factors which provide effective treat− ment and good prognosis, especially since ANN analysis allows for testing a virtually unlimited number of either mutually related or apparently unrelated factors and cases.
References
[1] Błaszczyk J, Pudełko M, Cisarż K:Nowotwory złośliwe na Dolnym Śląsku w roku 2003. Dolnośląski Rejestr Nowotworów, Wrocław 2005.
[2] Christian J, Thomas H:Ovarian cancer chemotherapy. Cancer Treat Rev 2001, 27, 99–109.
[3] Markowska J:Rak jajnika. Springer PWN, Warszawa 1997.
[4] Kristensen GB, Trope C:Epithelial ovarian carcinoma. Lancet 1997, 349, 113–117.
[5] Granai CO, Gajewski WH, Legare RD, Gordinier M: Gynecologic Cancer. In: Handbook of Cancer Chemotherapy. Eds.: Skeel RT, Lippincott Williams & Wilkins, Philadelphia 2003, 294–326.
[6] Schwartz PE: Neoadjuvant chemotherapy for the management of ovarian cancer. Best Pract Res Clin Obst Gynecol 2002, 16, 585–596.
[7] Zupan J, Gasteiger J:Neural Networks for Chemists. An Introduction. VCH, Weinheim 1993.
[8] Zupan J, Gasteiger J:Neural networks: A new method for solving chemical problems or just a passing phase? Anal Chim Acta 1991, 248, 1–30.
[9] Kaliszan R: Structure and Retention in Chromatography. A Chemometric Approach. Harwood Academic, Amsterdam 1997.
[10] Schneider G, Wrede P:Artificial networks for computer−based molecular design. Prog Biophys Mol Biol 1998, 70, 175–222.
[11] Brickley MR, Shepherd JP, Armstrong RA:Neural networks: a new technique for development of decision sup− port systems in dentistry. J Dent 1998, 26, 305–309.
[12] Snow PB, Rodvold DM, Brandt JM:Artificial neural networks in clinical urology. Urology 1999, 54, 787–790.
[13] Wei JT, Tewari A:Artificial neural networks in urology: pro. Urology 1999, 54, 945–948.
[14] Krongrad A, Lai S:Artificial neural networks in urology: con. Urology 1999, 54, 949–951.
[15] Lee CW, Park JA:Assessment of HIV/AIDS−related health performance using an artificial neural network. Inform Manage 2001, 38, 231–238.
[16] Mian S, Ball G, Hornbuckle J, Holding F, Carmichael J, Ellis I, Ali S, Li G, McArdle S, Creaser C, Rees R:
A prototype methodology combining surface−enhanced laser desorption/ionization protein chip technology and artificial neural network algorithms to predict the chemoresponsiveness of breast cancer cell lines exposed to Paclitaxel and Doxorubicin under in vitroconditions. Proteomics 2003, 3, 1725–1737.
[17] Biganzoli E, Boracchi P, Coradini D, Grazia DM, Marubini E:Prognosis in node−negative primary breast can− cer: a neural network analysis of risk profiles using routinely assessed factors. Ann Oncol 2003, 14, 1484–1493.
[18] Lisboa PJ, Wong H, Harris P, Swindell R:A Bayesian neural network approach for modelling censored data with an application to prognosis after surgery for breast cancer. Artif Intell Med 2003, 28, 1–25.
[19] Jerez−Aragones JM, Gomez−Ruiz JA, Ramos−Jimenez G, Munoz−Perez J, Alba−Conejo E:A combined neur− al network and decision trees model for prognosis of breast cancer relapse. Artif Intell Med 2003, 27, 45–63.
[21] Buciński A, Bączek T, Kaliszan R, Nasal A, Krysiński J, Załuski J:Artificial neural network analysis of patient and treatment variables as a prognostic tool in breast cancer after mastectomy. Adv Clin Exp Med 2005, 14, 973–979.
[22] Buciński A, Bączek T, Waśniewski T, Stefanowicz M:Clinical data analysis with the use of artificial neural net− works (ANN) and principal component analysis (PCA) of patients with endometrial carcinoma. Rep Pract Oncol Radiother 2005, 10, 239–248.
[23] Rumelhart DE, Hinton GE, Williams RJ:Learning internal representations by error propagation. In: Parallel Distributed Processing. Eds.: Rumelhart DE, McClelland JL, MIT Press, Cambridge 1986, v. 1.
[24] Shepherd AJ:Second−Order Methods for Neural Networks. Springer, New York 1997.
Address for correspondence:
Adam Buciński
Department of Biopharmacy, Faculty of Pharmacy CM Nicolaus Copernicus University
M. Skłodowskiej−Curie 9 85−094 Bydgoszcz Poland
Tel.: +48 52 585 39 09
E−mail: [email protected] Conflict of interest: None declared Received: 8.12.2006