A Study of 43 Cases
Jacqueline C. Hijmans, M.D., and Norbert B. Enzer, M.D.
(N.B.E.) Duke University School of Medicine, Department of Pediatrics, Durham, North Carolina, and
(J.C.H.) University of North Carolina School of Medicine, Department of Medicine,
Chapel Hill, North Carolina
T N 1923,Helmholtzcalledattentionto the
.1. fact that ulcerative colitis, though well
recognized in adults for many years, occurs
also in children.1 Since that time a number
of reports have demonstrated that no age group is exempt and that approximately 10% of all cases occurs in the pediatric age group.2'3
In children as well as adults, ulcerative colitis is manifested by frequent loose stools with blood and mucus, cramping abdomi nal pain, abdominal distention, anorexia, and frequently fever. Physical findings are
usually nonspecific and related to the de gree of diarrhea, the intra-abdominal com
plications, or the obscure secondary sys temic manifestations often seen with this disease. The etiology is unknown. Patho logically the disease is characterized pri marily by acute and chronic nonspecific in flammatory changes of varying severity in the large intestine.4'5 The clinical course is punctuated by remissions and exacerba tions. The natural history of the disease is only partially known, as the diagnosis sel dom is made if symptoms improve or dis appear spontaneously in a short period of time. Patients who recover quickly and have no recurrences may be given an in correct diagnosis of common infectious di arrhea. This is probably particularly true in the childhood age group. Diagnosis is diffi cult and is established by the characteristic proctoscopic and roentgenographic signs and by exclusion of other diarrheal diseases. Characteristically the disease is present for a prolonged period of time before it is sus pected.6'7
This review was undertaken to study the
nature, course, and outcome of this disease in children as exemplified by 43 patients who have been seen at the Duke University Medical Center between 1932 (when the hospital opened) and the end of 1960. We have attempted to include all cases of ul cerative colitis occurring between birth and the age of 16 years. Emphasis has been placed on the correlation between the clini cal and laboratory features of the disease and its course and prognosis. In each pa tient the clinical history and examination led to the suspicion of disease of the large intestine. Patients with microscopic, cultu ral, or serologic evidence of parasitic or bacteriologic disease were not included in this series. We have also excluded all pa tients for whom repeated microscopic and bacteriologic examinations of the stools were not performed.
Diagnosis required direct visualization of the intestine and/or roentgenographic studies compatible with the diagnosis of idiopathic nonspecific chronic ulcerative colitis.
METHODS
Proctoscopic Findings
By sigmoidoscopy the physician may es tablish the diagnosis of ulcerative colitis, except in the rare individual with “¿right sided― colitis and a normal rectosigmoid.8 Contrary to popular opinion, a thorough ex amination can be performed safely and without undue discomfort at all ages if proper physiological and psychological preparation has been made and the exam iner is experienced in the pediatric age group. Before the sigmoidoscope is inserted,
ADDRESS: (N.B.E.) Duke Hospital, Durham, North Carolina.
P@wrmcs, March 1962 389
vening mucosa between ulcerations may appear as “¿pseudopolyps.―As healing takes place the mucosa may appear finely granu lar, and in late stages the entire colon may become narrowed. A cicatricial stricture ap pearing as a whitish fibrous ring also may be present. Carcinomatous degeneration occurs as a late complication.―
Materials should be taken directly from tileulcerated areas, to he examined cul
turally and microscopically for bacteria and
parasites (ameba) in order to rule out these
diseases.
Roentgenographic Examination of the Colon8'12
During fluoroscopic examination of the colon with a barium enema, tile colon may appear normal or perhaps slightly irritated.
In the early stages of tile disease, one finds
a fine, serrated appearance of the niliCosa
(“feathering―, Fig. 1). Later the pattern be
comes irregular and distorted as a result of
partial destruction of tile mucosa. Hyper
trophied islands of mucosa between the
areas of destruction may project into tile
FIG. 2. Case 14. “¿Leadpipe―appearance of the
colon in a 3-month-old boy with ulcerative colitis.
*
@‘¿.SC -J
Fic. 1. Case 26. “¿Feathering―of the cecal region in a 14—year—oldgirl with ulcerative colitis.
tile anus should be carefully examined for
the presence of fissures, periproctitis and
perianal abscesses, fistulas, and chronic in
flammatory changes.9 These may lead to the
suspicion of ulcerative colitis, wilich can tilen be confirmed by examination of tile rectosigmoid. Great care must be taken in advancing the sigmoidscope, as the intes tine may be diffusely ulcerated, friable,
and easily perforated. The changes in the
mucosa of tile colon depend upon the stage of tile attack and may include edema, hy peremia, friability, submucosal petecilial
hemorrhages, exudate, ulcerations, “¿pseu dopolyps―, or any combination of these
changes.4' 10,11
In tile acute stages tile mucosa is dif fusely inflamed, and gentle swabbing with
cotton will produce a small amount of
bleeding. Bloody purulent mucoid exudate
mixed with fecal material may be seen
trickling down from above and will obscure adequate visualization. Punctate submuco sal petechial hemorrhages and fine pinpoint ulcerations are characteristic. Later these ulcerations may coalesce, resulting in de
ARTICLES 391
lumen of the bowel as “¿pseudopolyps―.The wall becomes thickened, the haustral mark ings tend to disappear, the colon becomes shortened and the lumen narrowed (“lead pipe―appearance, Fig. 2).
In severe cases the ominous appearance of a “¿toxicmegacolon― may be observed.13 In this condition, possibly in a segmental
ileus of the colon, the large intestine be
comes markedly distended with gas. This condition may be diagnosed on a plain x-ray film of the abdomen. Gross perfora tions may occur through the weakened, friable intestinal wall.14
The roentgenographic examination may reveal also the numerous complications of the disease—strictures, fistulous tracts, ob struction, and carcinoma. It is important to include an ileal study in order to determine whether the disease has affected the ter minal ileum (back-wash ileitis) and as an aid in the differential diagnosis of tuber culous enteritis, regional enteritis, and other diseases.
CASE MATERIAL
Forty-three cases were found which met
the exacting criteria for inclusion in this
study (Table I).
Family History, Sex, and Race
Sixteen (37%) of the patients were first or only children. In only one case was there known ulcerative colitis in a relative (a pa ternal cousin). There were 24 boys (56%) and 19 girls (44%). Although approximately one-half of all children seen and admitted to Duke Hospital are Negro, the disease affected 38 Caucasian children (88%) and only 5 Negro children (12%).
Because of the rarity of Negro patients has received comment,15 our five cases will be briefly documented.
Case 12 was that of a Negro girl who was well until the age of 13% years, when she developed a chronic, severe diarrhea fol lowing large doses of laxatives. This per sisted with minor remissions for approxi mately 5 years. During this time procto scopic and roentgenographic findings were
characteristic of chronic ulcerative colitis. After 5 years of the disease she had a com plete remission, which has been present for 3 years.
Case 18 was that of a Negro girl with known sickle-cell disease. Ulcerative colitis began when she was 13 years old; it was active for 9 years. It has been quiescent for 3 years.
Case 25 was that of a 13-year-old Negro girl. The sudden onset of severe ulcerative colitis with hepatosplenomegaly, arthrop athy, and erythema nodosum occurred 6 months prior to her visit to Duke Hospi tal. In the subsequent 6 months she has had continuous symptoms, and follow-up studies have been continued.
Case 35 was that of a Negro male child who was hospitalized for 2 months at the age of 3 years. The disease was severe and responded only partially to therapy. He has not been seen since the original hospital
admission.
Case 40 was that of a 13-year-old Negro girl who had a relatively mild and inter mittent diarrhea for six months. She has not returned for further therapy.
Season
Of the 33 patients in whom the exact time of onset could be determined, 14 (43%) began in the summer months, 8 (24%) in the winter, 6 (18%) in the fall, and 5 (15%) in the spring. Onset in the summer months increases the difficulties of diagnosis be cause of the frequency of “¿summerdiar rhea―. On the other hand, exacerbation of a pre-existing mild ulcerative colitis by a “¿summerdiarrhea― infection may be mis construed as the onset of the disease. In view of the fact that 57% of cases begin in
seasons other than the summer, it is doubt
ful that there is a true causal relationship between the common diarrheas and ulcera
tive colitis.
Precipitating Factors and Pre-existing Disease
CaseSecRaceAge of Onset (yr)OnsetFinding after Barium Enema(‘our'eTotal Dura twa (yr)ComplicationsOutcome ‘¿@evere12
8 Insidious Reversed A'G, abnormal
urine, growth and sexual
retardation, pseudopolyps
Ecchymoses, stomatitis
Ilepatomegaly
Abnormal urine, rectal fissures Abnormal urine
1czematoid rasb,hepatomegaly, growth retardation, hydro ureter, toxic megacolon, rec tovaginal fistula, pseudo
polvps
Eczema
Arthropathy, hepatomegaly, reversed A/G, abnormal urine, stomatitis
Arthropathy
Petechiae, arthropathy, hepa tomegaly, abnormal urine, pseudopolyps
Arthropathy. hepatospleno megaly, growth and senual retardation, abnormal urine, reversed A/G, pseudopolyps Splenomegaly, liver abscesses
Growth retardation Macular rash, arthropathy,
growth and sexual retarda tion@ hepatosplenomegaly, hepatitis and cirrhosis, chol ecystitis, pancreatitis, ab normal urine, nephrosis, tes ticular atrophy, stomatitis, pseudopolyps
Papular rash, growth retarda
tion, hepatitis, reversed A/G, abnormal urine, renal vein thrombosis
Erythema nodosum, arthrop
athy, hepatomegaly, re
versed A/G
Total colectomy after 12
years of continuous symp toms; currently doing well Continuous symptoms Remission for 3.5 years; no
further follow-up Continuous symptoms Remission for 1 year; no fur
ther follow-up
Remissions (to 4 mo duration) Remissions (less than 4 nio
duration) Continuous symptoms
Remissions (less than 3 mo (luratioli)
Remissions (less than 4 mo duration)
Continuous, but mild symp toms
Jfemicolectomy; 6 months
later, total coleetomy and death
Remission for 1 year; no fur ther follow-up
Total colettomy and (leath
A 3-year remission after 19 years of continuous symp toms
Remission for 8 months; ni
furtherfollow—up
A 1-year remisskn after 9 years of continuous symp tonis
Remissions (to 18 mo dura tion)
Continuous, but mild symp toms
Remissions (to4 mo duration)
Unremitting course to death
Remissions (less than 2 mo duration) Continuous symptoms 10.5 11.5 (18 da) 9.5 5 12.5 7 Ft 14.5 13.5 Fulminating Insidious Fulminating Fulminating Insidious Insidious Fulminating Insi(lious Insidious Insidious Fulminating Univ Univ Rt Neg Lt 1-t Univ Neg Neg Univ Severe Severe Severe Severe Mild Mild Severe Severe Mild Mild Severe Severe 0.5 4 1.5 1.2 1.5 12 4.5 3.5 6 3.5 8.5 0.5 Pseudopolyps Ilepatosplenomegaly, pustular rash Ilepatosplenomegaly, growth retardation Erythemutous rash
Abnormal urine, arthropatliy, A 2-year remission after 5
edema, rash,pseudopolyp.s years of continuous symp toms
(2 wk) Fulminating
@ Insidious Univ Mild
8.5 Fulminating Univ Severe
Insidious Univ Mild 22
Fulminating Neg Severe 1.6
Fulminating Univ Severe 10
Insidious Insidious Insidious Insidious Univ Neg Neg Univ Mild Mild Mild Severe 3 10 13 8 U 12 18 2 3 4 3 6 7 8 9 10 11 12 13 11 1.5 16 17 18 19 20 21 22 23 24 F M M F M M M M M M F F F M F F M F M M F M M M F 3.5 0.3 9 0.5 3 1.2 w w w w. w w N ‘¿V w. ‘¿V N w 1@' ‘¿V w w w N
11.5 Insidious Lt Mild
10.5 Fulminating Lt Severe
13 Fulminating Neg Severe Continuous symptoms
Univ =universal involvement; Rt =right-sided involvement; Lt =left-sided involvement. ULCERATIVE COLITIS
TABLE I
CaseSczRaceAie of Onset (yr)OnsetFinding after Barium EnemaCourseTotal Dura tion (yr)ComplicationsOutcome 393 Fulminating Fulminating Fulminating Insidious Fulminating Insidious Insidious Fulminating Insidious Fulminating Insidious Insidious Insidious Insidious Insidious Fulminating Fulminating Insidious Seaualretardation,arthopathy.
reversed A/G, hemorrhage,
pseudopolyps
Erythematous rash,abnormal
urine, reversed A/G, rectal stricture, hemorrhage Arthropathy, rectovaginal fis
tula, rectal stricture, pseu
dopolyps
Abnormal urine
Stoinatitis,perireetalabsress,
perforation and peritonitis, fatty liver
Reversed A/G
Erythema nodosum, artlirop athy, hepatosplenomegaly, hepatitis, reversed A/G, growth and sexual retarda tion, clubbing, retarded bone age, abnormal urine, rectal stricture
Renal abscesses, fatty liver Growth retardation
Rectal prolapse, ulcerative ap
pendicitis, reversed A/G Sexual retardation
Growth retardation, stomatitis
Erythematousrash, growth re tardation, abnormal urine
Reversed A/G, toxic mega
colon, aortitis, fatty liver, pancreatitis Rectal stricture 26 27 28 29 so 31 32 33 34 55 36 57 38 39 40 41 42 45 2.3 2 9 12.5 13 0.3 1.2 3.5 12 0.3 0.8 3 0.8 0.5 0.5 13 0.2 Continuous symptoms Continuous symptoms
Remissions (to 1 yr duration)
A 7-year remission after 5 years of continuous symp toms
Remissions (to 4 yr duration)
l)eath
Remissions (lessthan 3 mo
duration) Continuous symptoms Remissions (to 2 yr duration)
Continuous symptoms Ileostomy and death Remissions (to 6 mo duration) Ileostomy and death
Remissions (less than S mo duration)
Continuous but mild symp toms
Remissions (to 5 yr duration)
Death
Remissions (to I mo duration)
F M 1'@ M M M M M F M F M F F' F M F F “¿-W ‘¿V ‘¿V N ‘¿V WI W W N w ‘¿V ‘¿V Severe @evere Severe Mild Severe Severe Mild Severe Severe Severe Severe Mild Severe Severe Mild Severe Severe Mild 14.8 15.5 15 5.5 13 13.5 14.3 11 1.5 3 4.5 9 6.5 14.5 13.5 1.5 (2 da) 8 Univ L'niv Neg Neg Univ Neg Univ Neg Neg Univ Univ Univ Lt. Neg Univ
tients (9%) dated the onset of their illness to respiratory infections, pharyngitis, or mea sles. In one patient, laxatives had been used excessively just prior to the onset of the disease. In one patient the onset of disease appeared to coincide with emotional upset, and in six patients (14%) the onset coincided with a change in family relationships.
Patient 5 was an infant whose symptoms began at 18 days of age, when his mother was hospitalized and breast feeding was suddenly interrupted. Three children (aged 10, 11%, and 15 years) developed initial symptoms when they went to summer camps. Patient 27, a 15%-year-old boy, had his onset shortly after going to a summer
music school. Patient 37, a 9-year-old boy, began to have diarrhea when he went to a boarding school.
Thirty-six (84%) patients were in good health prior to the onset of the disease. Seven patients (16%) had pre-existing ill
nesses. The latter included one instance each of asthma, eczema, herpetic stomatitis,
sickle-cell disease, rectal surgery for pro lapse, and chronic otitis requiring three mastoidectomies. One child is said to have been “¿neverstrong―. It is interesting that the outcome of the ulcerative colitis was fatal in three of these seven patients (her petic stomatitis, “¿neverstrong―, and the child with chronic otitis). The remainder, ARTICLES
with one exception (an infant with eczema), had rather severe forms of the disease.
Mode of Onset
Svmptonis were present for varying pe
nods of time, from 2 weeks to 12 years, prior to the first visit to Duke Hospital. Ap proximately half of the patients (22) were ill for 6 months or less; tile remainder, in general, had manifestations for prolonged periods of time.
The patients could be divided clinically
into two broad groups with regard to the mode of onset of the disease. When symp toms appeared gradually with little increase in tile number of stools per day, little or no
blood or mucus in the stools, and few (if
any) constitutional complaints, the mode of onset was termed insidious. The fulminat ing group included those showing a sudden marked increase in the number of stools per day, gross blood and/or mucus in the stools, and many, usually severe, constitu tional symptoms. The onset was insidious in 24 patients (56@) and fulminating in 19 (44%) cases.
Age of Onset
Figure 3 demonstrates the age distnibu tion taken in 2-year periods and indicates the mode of onset in each age group. It is noteworthy that in three of the five cases
in the O-to-2 year age group the onset was in
the first month of life. Diagnosis is less fre quently made in the preschool group. In
Fulm@notng p1
the pre-adolescent and adolescent ages, there is a marked increase in the frequency of diagnosis.
The onset was fulminating in the three newborn infants and the course, as will he noted below, was severe in these cases. During the preschool years, the mode of onset was usually insidious. From the age of 10 years on, the onset was again more
likely to be fulminating (58%).
Symptoms and Signs
Figure 4 shows tile incidence of the vari
ous symptoms and signs noted at the time
of the first visit to Duke Hospital. Diarrhea, stools with blood or mucus, abdominal pain
or tenderness, weight loss, anorexia, fever, malaise, and tile appearance of chronic ill ness were tile most common findings at tile time of the original visit to the hospital. Less frequently encountered signs and symptoms included abdominal distention, nausea and vomiting, various skin rashes, hepatospleno megaly, growth retardation, arthropathy, and sexual retardation. Figure 4 shows also
the correlation of the signs and symptoms
at admission with the subsequent course. Sixty-five per cent of the total series had severe courses. Tile course was more likely to he severe (more than 85% of the patients) in those patients llavmg an appearance of
chronic illness, nausea and vomiting, rash,
hepatosplenomegaly, arthropathy, or sexual
retardation at the first admission. On the
other hand the presence of diarrhea, 1)100(1
and mucus in the stools, abdominal pain
and tenderness, weight loss, anorexia, fever
or growth retardation was not of prognostic
value. None of these manifestations mdi cated a significantly different course than
would be anticipated from the diagnosis alone (65% severe).
Table II shows tile positive accessory clinical findings on admission. Correlation
of tilese tests with tile subsequent course of tile patients is shown in Table III. The
presence of leukocytosis, abnormal urine, reversed albumin-globulin ratio, eosino philia, and marked anemia indicates a more severe course; a normal hemoglobin value,
II —¿.
0 9..
8@
7..
a. @..
e 4..
D
Z 3..
2
0@
Ii@n
02 2.4 4-6 68 8-10 1012 2.14 14-16
AGE OF ONSET IN YEARS
FIG. 3. Bar graph showing relation of age of onset
ARTICLES
normal albumin-globulin ratio, and a nor mal sedimentation rate are indicative of a milder subsequent course.
Proctoscopy was performed in all but
three cases. In these three children, the
large intestine was visualized either at sur gery or in pathological material and found
to show changes compatible with tile diag
nosis of ulcerative colitis. One child (Case
3) had a negative proctoscopic examination. However a diagnosis of ulcerative colitis
had been made elsewhere, and tile child had been treated with steroids.
Barium contrast studies of the colon were
performed on 37 patients. Eighteen patients had universal involvement of the colon, 5 had involvement limited to the rectosig moid, 1 had disease on the right sidle only,
and 13 had apparently normal b(,wel pat
terns. It is interesting to note that the Se
395
verity of tile total course was very similar
in those patients who initially showed
positive findings on the barium enema and
TABLE IL
INCII)EN( E OF ABNORMAL AC(E@OltY CLINICAL
FINl)INGS ON FUIsT ADMISSION
Patients wit/s Positive Patients Test Results
flndinqs 1@xamsued
(no.) Number Per rent Diarrhea
AbnormalMucosa
Blood and Mucus in Stools
Abdominal Pain and Tenderness
Weight Loss
Anorexia
Fever
Malaise
Ill Appearing
Abdominal Distension
Nausea and Vomiting
Rash
Hepatosplenomegaly
Growth Retardation
Arthropathy
Sexual Retardation
Total Cases
(.)
_______________________________________________1
__
1
Ij@-@7
7
1111
Numberand % of Patients with Severe Courseof Disease
7 Number
ofPatients
______
with
amild
Disease
5 10 15 20 25 30 35 40 45
NUMBEROF CASES
Fic. 4. Relation between signs and symptoms at original hospital visit to subsequent course
ulcerative colitis. Tile total length of bar in(licates the number of patients having the particular manifestation. The solid bars and enclosed figures indicate numbers and percentages of patients
(with the particular sign or symptom) whose subsequent total course was severe.
Barium
enema37@465Anemia43@2763Increased
ESIt1910,53Reversed
A-G ratio@2l11&-2Left
shift of leuko
cvte
course of the disease except for early onset in the first month of life. Of the three pa
tients who had their onset (luring the first
month of life, two died of the disease. In
comparing Figures 3 and 5, it becomes ap
parent that mode of onset does not dictate tile course of the disease. Thus, all patients
in the 4-to-6 and 6-to-8-year-old groups had
insidious onsets (Fig. 3). Nevertheless, of these five patients, two died, two had a se vere and almost unremitting course, while only one could be considered mild (Fig. 5). Although not apparent in the charts, the converse is also true. Patients with a ful minating onset may ultimately fall into the mild to moderate group svith regard to the course of the disease.
In our series, the children had symptoms for an average of 2 years (2 weeks to 12 years) prior to their initial visit to tile hos pital. The average period of observation was 23-iyears (up to 14 years). Thus there was an average course by history and by
observation of 4% years (1 month to 22
years).
The duration of the disease was not nec essarily correlated with its severity. Patient 16 had been ill for 10 years but had few
clinical signs amid appeared normal in gen
eral growth and development. Patient 7
likewise had few positive findings despite
an illness of 12 years' duration. On the other hand, though Patient 34 had been ill for a similar period of time (12 years), she had
•¿ Death
Continued Symptom or Remission (4 mo 3
@ Remission
L.@J >4mo but(3yr
-@ ContinuedRemission
Over 3yr
TABLE III
I{E1.@TmON01 I NITIAL L.-tBo1t;@ToneFINI)INGS TO @1Iti—1EQLEXT CoIusF:*
Patients uit/t Patients with Positive Test Negative Test
Results and Results a ‘¿(et'ereCourse Severe Course
(%) (%)
63 61)
71 51)
71) 33
100 11)
63 72
82 60
100 53
80 63
1tndiny.s-liariiniieiictii@t
fleiflia
In(r(-as((l lit Reversed A—(rat Left shift of lenko
(yte (0(101 Leu(o(Vtosis
Abnormal urine
EOsino1)hulia
* Sixtv—fi@-e p@-r cent of all patients ha(l a Se\ere
course.
those showing negative findings (Table III). In view of the paucity of cases showing other than universal involvement, no at tempt was made to correlate the specific
localization of the disease with the course or outcome.
Course of the Disease
The 43 patients could be divided into two
groups on the basis of the total course of
the disease. The first group, SCUCTC,in cluded patients who died, who had almost continuous and severe symptoms with short remissions and severe fulminating exacerba tions, who required definitive surgery, or who had many or severe systemic manifes tations and/or complications. The mild to
moderate group included those patients
with mild symptoms and those in whom remissions were rather prolonged and the exacerbations benign. Few, if any, consti tutional symptoms or complications were present in this group. Twenty-eight patients (65%) were in the first group, with a severe course, while 15 patients (35%) had a mild to moderate disease.
Figure 5 shows the relationship between age of onset and total course of the disease. When grouped in 2-year periods, age of onset does not appear to determine the
fl'
‘¿Ii @i@@ii1t1
- Ci@ 2-4 4-6 6-8 8-10 10-12 12-14 14-16
AGE OF ONSET IN YEARS
397 ARTICLES
marked and severe findings (chronically ill appearance, rash, arthropathy, hepatosplen
omegaly, growth and sexual retardation,
anemia, elevated sedimentation rate, re versed albumin-globulin ratio, and abnor mal urine).
Relationship of Emotional Factors to Ulcerative Colitis
As has been previously mentioned, in only seven patients (16%) could emotional factors be considered as precipitating causes for the original appearance of symp toms. The fact that such a relationship was not apparent in the remainder, and the presence of three infants showing the dis ease in the first month of life, make it difficult to ascribe a causal role to emotional factors. In view of the known relationship between emotional factors and gastrointes tinal symptoms, it appears more likely that psychic disturbances can precipitate symp toms in individuals with mild but unrecog nized ulcerative colitis. There is also much evidence that psychic disturbances can cause serious exacerbations in the dis ease.lhilT However, similar exacerbations also may be precipitated by intercurrent illness, dietary indiscretions, and many other factors. None of these have apparent etiological significance. This does not imply that psychotherapy is unimportant in the management of the disease. As has been emphasized by Engel,@6 defective person ality patterns and restricted interpersonal relationships may be found. Careful atten tion to basic or precipitating psychic fac tors may be rewarded by a more benign course. In nine of our patients emotional disturbances were noted during the course of illness, but there was no consistent pat tern of behavior. As in any chronic disease, particularly one with a persistent diarrhea incompatible with normal human relation ships, secondary psychic disturbances may require therapy.
Colonic and Rectal Complications9'18
In our 43 patients the following local complications were noted: pseudopolyps,
8 patients; rectal stricture, 2; rectovaginal fistula, 2; toxic megacolon, 2; rectal fissure, 1; perforation and peritonitis, 1; ulcerative appendicitis, 1; massive bleeding, 1; (Table I). No instances of malignant degeneration were noted in this series.
Extra-colonic Manifestations
Ulcerative colitis may be associated with a large variety of extracolonic manifesta tions. These include anemia,19 skin rashes,2°'21 stomatitis, arthropathy,22-24 clubbed fingers, growth and sexual retarda tion,25 angiitis,26' 27 renal disturbances,28 cessation of menses, reversed albumin-glob ulin ratio, hepatosplenomegaly, hepatitis and cirrhosis,29-32 and pancreatitis.33 Many other complications have been reported in the literature.@@ These extra-colonic mani festations appear to be correlated with the severity rather than the duration of the dis ease. Eight patients had a wide variety of problems despite the fact that clinical symptoms had been present for less than six months.
Patient 5 was a 2%-month-old child who had anemia, leukocytosis, and abnormal urine, though the disease had been present only 8 weeks; Patient 12 was a 14-year-old girl who had the disease for 6 months and on admission showed rash, arthropathy, anemia, and abnormal urine. Patient 15, a 9-year-old girl, had arthropathy, stomatitis, hepatosplenomegaly, anemia, reversed al bumiri-globulin ratio, and abnormal urine, though the disease had been present only 6 months. Patient 21, a 12-year-old girl, had growth retardation and anemia, with symp toms present only 3 months. A 13-year-old girl (Case 25) had the disease for 6 months and showed erythema nodosum, hepato splenomegaly, anemia, elevated sedimenta tion rate, and reversed albumin-globulin ratio.
SourceTotal
)
flOPFree
of SymptomsActiveDiseaseDeceased
Number Per CentNumberPer CentNumberPer
CentJackman
et
al.2951111.66265.32223.2Lagercrantz371374432.274541913.8Plattetal.35623760203258Present
series4312282456716Total33710430180545316
ULCERATIVE COLITIS
and a fatty infiltration of the liver. Patient 24 was an 11-year-old boy who had had symptoms for 6 months. On admission he was found to have a papular rash, growth retardation, anemia, and a reversed albu min-globulin ratio. Because of the striking urinary findings of hematuria and protein
uria together with a mass on the left side,
operation was performed and the kidney removed. An extensive thrombosis of the renal vein was found. Patient 42 was a 4-week old infant whose symptoms dated to the age of 2 days. On admission she showed a toxic megacolon, anemia, leuko cytosis, and a reversed albumin-globulin ratio. The course was extremely fulminant, and the infant died at the age of 6 weeks. Autopsy showed acute aortitis, pancreatitis, and fatty infiltration of the liver, in addition to extensive typical changes of ulcerative colitis in the colon.
These cases are to be contrasted with 11 cases in patients who had the disease for 6 years or longer, sometimes with rather prolonged remissions (Cases 1, 7, 10, 16, 18, 22, 28, 29, 30, 34, and 41). In five of these patients (Cases 7, 10, 16, 29, and 30) the disease was essentially uncomplicated and without systemic manifestations. Two of the eleven (Cases 18 and 34) had serious extra-colonic manifestations—arthropathy, splenomegaly, growth retardation, sexual retardation, anemia, leukocytosis, reversed albumin-globulin ratio, abnormal urine, ele vated sedimentation rate, clubbing of the fingers, and retarded bone age. Patient 28 had the disease for 11 years in mild degree. She then completed two pregnancies but
developed a rectovaginal fistula at the time of the first delivery. Later, after a total course of 15 years, she developed periodi cally incapacitating arthralgia. One patient (Case 22) ultimately died of cirrhosis and bleeding from esophageal varices. Another patient (Case 1) had a reversed albumin globulin ratio, abnormal urine, pseudo poiyps, and growth and sexual retardation. Elective surgery of the large intestine was done, and the patient has been doing well since.
Five patients had stomatitis during the course of their illness—variously described as ulcerative, aphthous, or herpetiform. The stomatitis usually occurred during acute exacerbations of the disease and were in dicative of a more serious prognosis. Three of these patients ultimately died of the dis ease or its complications (Cases 15, 22, and 31). One child (Case 2), an 11-year-old white boy, had a severe exacerbation dur ing the course of which a herpetiform sto matitis appeared. However, this child im proved and was not seen again. The fifth patient (Case 40), a 14-year-old Negro girl, was the only one with a benign course of the disease.
Outcome
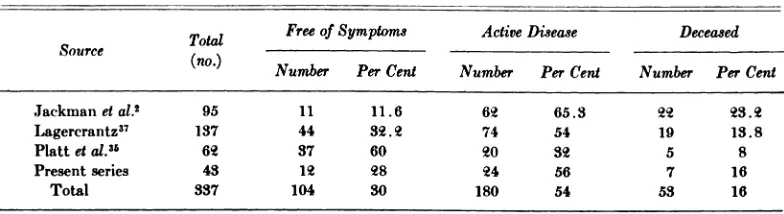
The outcome, at the time of this writing, is 12 (28%) prolonged remissions (one after colectomy), five patients (12%) who showed much improvement, 19 patients (44%) who remained symptomatic, and 7 deaths (16%).
These figures may be compared with those of Platt et
@ Hollowach and Thurs
ton,36 and Lagercrantz3T (Table IV). The
TABLE IV
ARTICLES 399
mortality in these series range from 8 to 23%; 12 to 50% of the children have re mained well with prolonged remissions, while another 10% in one series have been doing satisfactorily on corticoid therapy. The remainder have either come to surgery or are having a variable course. Thus, the disease is a most serious one both for life and for regaining normal health and ac tivity. We cannot agree with the statement of Lagercrantz37 that serious recurrences are rare after an asymptomatic remission of 2 years' duration. A number of our pa tients have had serious relapses after re missions lasting up to 5 years.
Fatalities
There were seven (16%) deaths in the en tire series. Deaths occurred either follow ing surgery (Cases 13, 15, 36, and 38) or as a result of complications of the disease, as in cirrhosis (Case 12), perforation and peri tonitis (Case 31), and aortitis (Case 42). The occasional extremely fulminating nature of the disease is documented by the latter two cases. Perforation and peritonitis occurred after a course of only 3 months in one child, while death from aortitis occurred 6 weeks after the onset in the other. The postopera tive deaths occurred between 6 months and
2 years following the onset of the disease,
indicating a very severe course since these operations were done on an emergency basis. The death from cirrhosis occurred 9 years after onset. It is to be noted that there were no deaths from carcinoma or obstruc tion in this series.
Therapy
The vast majority of our patients were treated with one of the “¿sulfa―drugs. Six teen received a corticoid or ACTH. It is im possible to evaluate the effects of therapy in our group of patients, as they occurred during a period of nearly 30 years and there were marked changes in the type of therapy administered. It was our impres sion that steroid therapy was helpful in causing remission of symptoms and reduc ing the time spent in the hospital. With
others we have seen exacerbations of the disease while patients were on adequate steroid therapy. The underlying cause of the disease did not appear to be effected.
Surgery was performed in five cases. In only one (Case 1) was this an elective pro cedure. This patient was operated upon approximately 12 years after the onset of her disease because of continuous symp toms, pseudopolyps, anemia, and growth and sexual retardation. Since surgery she has done quite well. In all other instances of surgery of the large intestine (Cases 13, 15, 36, and 38) the patients died shortly af ter operation. It should be noted that in these cases surgery was undertaken as an emergency measure to save life. Severe electrolyte disturbances were prominent post-operatively.
COMMENT
As again shown by this review, ulcerative colitis can occur at all ages in childhood. The disease is serious, the course variable, and the prognosis unpredictable. At all ages, but particularly in the very young, diagnosis is difficult. Of the multiple signs and symptoms only the bloody diarrhea with mucus, the abnormal colonic mucosa as seen through a sigmoidoscope, and, to a lesser extent, abdominal pain and tender ness have a high degree of consistency from case to case. Though abnormal findings of a barium enema study are helpful in estab lishing the diagnosis, normal findings may lead to unjustified complacency since the changes may not be present characteristi cally in the very early stages of the disease.
400
tient had a gradual onset of two to four stools per day with some blood and mucus. Except for a minimal weight loss she had no additional symptoms. Findings of the original general physical examination were unremarkable. Following a remission cf about 4 weeks' duration, she had a ful minating exacerbation characterized by anemia and 10 or more bloody stools per day. There was another brief remission for 2 weeks, followed by severe intestinal hem orrhage necessitating numerous transfu sions. An emergency ileostomy was per formed, and she died approximately 4 weeks later. By contrast, a fulminating on set must not be regarded as hopeless. Many of these patients who go into remission may continue to do well. Patient 12 was a 13-year-old girl who suddenly developed six to eight watery bloody stools daily. This was associated with abdominal pain and tenes mus. Shortly thereafter she developed arth ralgia, skin rash, edema, spiking fever, and anemia. Roentgenograms showed involve ment of the entire colon. After 5 years of frequent exacerbations, she had a complete
remission. Several protoscopic examinations
during this remission revealed normal ap pearing mucosa. Since then she has married and has had one successful pregnancy. No further symptoms were noted. However, even after prolonged remissions, each pa tient must be followed carefully, as exacer bations may occur at any time. Recent studies of rectal biopsy material indicate that histologic disease may persist in the face of clinical and sigmoidoscopic evi dence of remission.38 One of our patients (Case 41) was in remission for 5 years be fore having a severe relapse. A diagnosis of ulcerative colitis in childhood, therefore, predicates careful observation for many years—throughout the pediatric age period and into adult life.
In this disease it is unwise to venture a prognosis when the child is first seen or even after he has been followed for several years. In this disease, unlike many other chronic diseases, the severity of the most common findings does not seem to be im
portant prognostically. As mentioned, slight increase in the number of stools does not exclude a malignant course, nor does a pro fuse diarrhea, although alarming at the moment, predicate a fulminating disease and an ominous prognosis. Usually, how ever, a more severe illness is associated with certain signs and symptoms—severe malaise, chronically ill appearance, nausea and vomiting, skin rashes, hepatospleno megaly, arthropathy, sexual retardation, re versal of the albumin-globulin ratio, and an abnormal urinalysis.
Intestinal perforation, fistulas, abscesses, strictures, hemorrhage, pseudopolyps, and carcinoma occur as direct complications from the diseased intestine. Fortunately we did not encounter any malignancies in our group, but the incidence has been reported to be 6.3%, usually occurring many years after the onset of the disease itself.2'39
The disease has many extra-colonic mani festations, such as arthropathy, skin rashes, sexual and growth retardation, hepatomeg aly, splenomegaly, anemia, electrolyte dis turbances, alteration of protein patterns in serum, and changes in the urinary tract. Some of these are undoubtedly secondary to the disease, but others occur so fre quently and so early in the course that they seem to be associated rather than secondary features. In many ways, ulcerative colitis behaves as a systemic disease, with the colon as tile primary target organ.
Because of the seriousness of the disease,
it is imperative to eliminate all other possi
bilities in the differential diagnosis. Direct stool examination, cultures, and serologic tests are helpful in ruling out amebic dysen tery, bacillary dysentery, and typhoid and paratyphoid fever. Skin tests (tuberculin and Frei) will be helpful in diagnosing tu berculous enteritis or lymphopathia vene rea. It is particularly difficult to distinguish certain cases of regional enteritis from ul
cerative colitis, particularly as there may be
ARTICLES 401
ative colitis. Careful proctoscopic and roentgenographic examination of the intes tine may be helpful.
Since the etiology of ulcerative colitis is unknown,4 therapy is entirely sympto matic.4' During exacerbations the usual treatment for diarrhea should be pre scribed. A bland diet, antispasmodics, de mulsions, sedatives, blood transfusions, and parenteral fluids may be helpful. Habit forming drugs such as opium derivatives must not be given both because of the dan ger of drug addiction in a chronic disease and also because of the possibility of pro ducing serious abdominal distension. Many patients will complain that certain foods (milk, chocolate, tomatoes, potatoes, etc.) are not well tolerated and produce an in crease in the number of stools. Intolerance to foods should be carefully sought by his tory, skin testing, and elimination diets.
As has been reported many times, sulfon amides are a valuable adjunct in therapy.42 Salicylazosulfapyridine (Asulfidine) seems to be effective and should be employed in appropriate doses (100 mg/kg/day given at 4-to-6-hour intervals). This may be con tinued for prolonged periods, but the pa tient should be carefully followed for the appearance of toxic manifestations such as skin eruptions and agranulocytosis.
Adrenal corticoids and ACTH have been helpful in diminishing the severity of symp toms and in producing remissions.43 They do not appear to affect the underlying causes of the disease in that exacerbations may occur while the patient is on cortisone therapy. In other instances, corticoids have no effect on the acute manifestations. Fur thermore, relapses seem to occur as fre quently in those patients who have received corticoids as those who have not. In gen eral, tile use of corticoids will diminish the length of time necessary in the hospital and will allow the patient to lead a more nor mal life. Tile long-term benefit has yet to be evaluated. Analyses of the figures of Platt
et al.35 show no differences in the ultimate
outcome of patients who have received cor ticoids as compared with those who have
not. It should be kept in mind that corti coids may mask the complications of the disease, such as infection and perforation. Further, it has not been documented as to whether patients with ulcerative colitis are more prone to systemic infections and per foration if they are maintained on cortisone tilerapy.
Throughout the course of tile disease, tile
patient should receive psychological sup port. Attention should be paid in particular to the possibility of improving disturbed family patterns and interpersonal relation ships that may be deleterious to the child with ulcerative colitis. Secondary malad justments because of the chronicity of the disease and its disabling nature also require therapy.
Surgery, particularly in children, has usu ally been reserved for patients having se vere hemorrhage, intractable fulminating course, impending perforation, perforation with peritonitis, and the various complica tions such as stricture, abscess formation, fistulas, and malignancy. Operative mor tality has been excessively high because surgery usually has been performed as a terminal lifesaving measure. However, un der optimal conditions and with good sur geons, the mortality may be as low as 5 to
10%.@@As Ehrenpreis et
@ have shown in
a series of 23 cases, the majority will re quire total colectomy, removal of the rec tum, and a permanent ileostomy. If tile rec tum is not severely involved, an ileorectal anastomosis may be attempted, or an ileos
tomy may be done, preserving the rectum
for possible later anastomosis. Although one hesitates to subject a child to colectomy, especially with a permanent ileostomy, the seriousness of the disease indicates that
surgery perhaps should be used more fre
plicated by the signs previously mentioned might well he candidates for early surgery rather than, as at present, be considered for operation only in dire emergency. Total colectorny @5the procedure of choice al though some prefer to leave a rectal stump (if it is not seriously diseased) for later anastornosis.45
SUMMARY
Forty-three cases of ulcerative colitis in children, seen at Duke Hospital during a 28-year period, have been analyzed with regard to the nature, course and outcome of this disease in the pediatric age group. Emphasis has been placed on the correla tion of the clinical and laboratory features with the course and prognosis of the dis ease. Cases have been cited to demonstrate that the disease is serious, the diagnosis difficult, the course variable, and the prog nosis unpredictable. A diagnosis of ulcera tive colitis in childhood necessitates careful and continuous observation throughout the pediatric age and into adult life. Because of the chronicity, the complexity, and the seriousness of the disease, therapy demands the close co-operation of the pediatrician, the psychiatrist, and the surgeon.
REFERENCES
1. Helmholz, H. F.: Chronic ulcerative colitis in
children. Amer. J. Dis. Child., 26:418, 1923. 2. Jackman, R. J.,Bargen, J. A., and Helmholz,
H. F.: Life history of 95 children with chronic ulcerative colitis. Amer. J. Dis. Child., 59:459, 1940.
3. Cullinan, E. R., and MacDougall, J. P.: The natural history of ulcerative colitis. Castro
enterologia, 86:582, 1956.
4. Warren, S., and Sommers, S. C.: Pathology of regional ileitis and ulcerative colitis. J.A.M.A, 154:189, 1954.
5. Lumb, C., and Protheroe, R. H. B.: The early
lesionsin ulcerativecolitis.Gastroenterology,
33:457, 1957
6. Sloan, W. P., Jr., Bargen, J. A., and Gage, R. P:. The life histories of patients with chronic ulcerative colitis: a review of 2,000 cases. Gastroenterology, 16:25, 1950.
7. Waligren, A.: Ulcerative colitis in children. Deutsch. Med. J., 6:45, 1955.
8. Kirsner, J. B., Raskin, H. F., and Palmer,
W. L. : Ulcerative colitis in children. Amer.
J. Dis. Child., 90:141, 1955.
9. Sloan, W. P., Bargen, J. A., and Baggenstoss,
A. H. : Local complications of chronic ulcera
tive colitis based on the study of 2,000 cases.
Proc. Mayo Clin., 25:240, 1950.
10. Warren, S., and Sommers, S. C.: Pathogenesis
of ulcerativecolitis.Amer. J. Path.,25:657,
1949.
11. Buie, L. A.: Chronic ulcerative colitis. J.A.M.A.,87:1271, 1926.
12. Hodgson, J. R., and Kennedy, R. L. J.: The roentgenologic aspects of chronic ulcerative
colitis in children. Radiology, 65:671, 1955.
13. Wolf, B. S., and Marshak, R. H.: Toxic seg mental dilatation of the colon during the course of fulminating ulcerative colitis: roentgen findings, Amer. J. Roentgenol., 82: 985, 1959.
14. Roth, J. L. A., et at.: Toxic megacolon in ulcerative colitis. Gastroenterology, 37:239, 1959.
15. Reinhart, J. B.: Ulcerative colitis in Negro children (Letter to Editor).Amer. J. Dis. Child.,101:401, 1961.
16. Prugh, D. G.: The influence of emotional fac tors on the clinical course of ulcerative colitis in children. Castroenterology, 18:339, 1951. 17. Groen, J., and Van der Valk, J. M.: Psychoso
matic aspects of ulcerative colitis. Gastro
enterologia,86:591, 1956.
18. Wilcox, H. R., Jr., and Beattie, J. L:. Carci noma complicating ulcerative colitis during childhood. Amer. J. Clin. Path., 26:778, 1956.
19. Barr, ‘¿s-I.,Delava, S., and Zetterstrom, R.:
Studies an anemia in ulcerative colitis with
special reference to the iron metabolism. Acta. Pediat., 44:62, 1955.
20. Samitz, M. H., and Ringberg, M. S.: Skin
lesions in association with ulcerative colitis.
Gastroenterology, 19:476, 1951.
21. Jacobs, W. H.: Erythema nodosum in inflam matory diseases of the bowel. Gastroenterol
ogy, 37:286, 1959.
22. Bywaters, E. G. L., and Ansell, B. M.:
Arthritis associated with ulcerative colitis.
Ann. Rheum. Dis., 17:169, 1958.
23. Wright, V., and Watkinson, C.: Arthritis of
ulcerative colitis. Medicine, 38:243, 1959. 24. Friedman, E., and Kehoe, E. L.: Non-bacterial
suppurative arthritis as a complication of ulcerative colitis. New EngI. J. Med., 261:
288, 1959.
25. Benson, R. E., and Bargen, J. A.: Chronic ulcerative colitis as a cause of retarded sexual
and somatic development. Gastroenterology,
1:147, 1943.
ARTICLES 403
Necrotizing angiitis associated with chronic ulcerativecolitis.Amer. J. Med., 17:736, 1954.
27. Ihre, B. J. E.: Pathology of ulcerative colitis.
Gastroenterologia, 86:666, 1956.
28. Jensen, E. J., Baggenstoss, A. H., and Bargen,
J. A.: Renal lesions associated with chronic
ulcerative colitis. Amer. J. Med. Sci., 219:
281, 1950.
29. Jones, G. W., Baggenstoss, A. H., and Bargen,
J. A.: The liver in chronic ulcerative colitis,
Proc. Staff Meet. Mayo Clin., 25:251, 1950. 30. Kleckner,M. S.,et al: Hepatic lesionsin the
living patient with chronic ulcerative colitis as demonstrated by needle biopsy. Castro
enterology, 22:13, 1952.
31. Monto, A. S.: The liver in ulcerative disease of the intestinaltract:Functional and ana tomical changes. Ann. mt. Med., 50:1385, 1959.
32. Boden, R. W., et al.: The liver in ulcerative colitis.Lancet, 2:245, 1959.
33. Ball, P., Baggenstoss, A. H., and Bargen, J. A.:
The pancreas in ulcerative colitis. Proc. Mayo
Clin., 25:256, 1950.
34. Turell, R. (Editor): Diseases of the Colon and
Anorectum, Vol. II. Philadelphia and Lon don, Saunders, 1959, pp. 658.
35. Platt, J. W., Schlesinger, B. E., and Benson, P. F.: Ulcerative colitis in Childhood. Quart.
J. Med.,29:257,1960.
36. Hollowach, J.,and Thurston, D. L.: Chronic ulcerativecolitisin childhood.J.Pediat.,48: 279, 1956.
37. Lagercrantz, R.: Follow-up investigationof
childrenwith ulcerativecolitis,with special referenceto indicationsfor surgicaltherapy. Acta. Pediat., 44:302, 1955.
38. Dick, A. P., and Grayson, M. J.: Ulcerative colitis: a follow-up investigation with mu
cosal biopsy studies. Brit. Med. J., 1:160, 1961.
39. Kiefer, E. D., Eytinge, E. J., and Johnson, A. C.: Malignant degeneration in chronic ulcerativecolitis.Gastroenterology,19:51, 1951.
40. Warren, I. A., and Berk, J. E.: The etiology of chronic non-specificulcerativecolitis:a
criticalreview. Gastroenterology,33:395, 1957.
41. Bargen, J. A., and Kennedy, R. L. J.: Chronic ulcerativecolitisin children.Postgrad.Med., 17:127, 1955.
42. Kirsner,J. B.: Current concepts of the medi cal management of ulcerative colitis.
J.A.M.A., 169:433, 1959.
43. Kirsner,J. B., et al: Corticotropin(ACTH) and the adrenal steroidsin the management of ulcerative colitis: observations in 240 pa
tients. Ann. mt. Med., 50:891, 1959.
44. Lyons, A. S.: Ulcerative colitisin children. Pediat.Clin.N. Amer., 19:153, 1956. 45. Meeker, I. A., Jr., and Goff, P.: The surgical
signfficance of ulcerative colitis in infants and
children. Western J. Surg., 64:545, 1956.
46. Engel, C. L.: Studies of ulcerative colitis. Amer. J. Med., 19:231, 1955.
47. Ehrenpreis, T., et al: Surgical treatment of
1962;29;389
Pediatrics
Jacqueline C. Hijmans and Norbert B. Enzer
ULCERATIVE COLITIS IN CHILDHOOD: A Study of 43 Cases
Services
Updated Information &
http://pediatrics.aappublications.org/content/29/3/389
including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in its
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
1962;29;389
Pediatrics
Jacqueline C. Hijmans and Norbert B. Enzer
ULCERATIVE COLITIS IN CHILDHOOD: A Study of 43 Cases
http://pediatrics.aappublications.org/content/29/3/389
the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.