Common Variable Immunode
fi
ciency Presenting With
Persistent Parvovirus B19 Infection
abstract
Parvovirus B19 infection in healthy hosts is self-limited, but persistent infection has been described in patients with cellular immune defects. A 6-year-old boy presented with a 6-month history of weight loss and malaise and a 1-month history of fever and polyarticular arthritis. Parvovirus DNA was detected in plasma at 10 300 copies/mL. Levels of immunoglobulin (Ig)G, IgA, IgM, IgG-1, and IgG-2 were low, and anti-body responses to vaccine antigens were impaired. HIV antianti-body and DNA polymerase chain reaction were negative, and the patient had normal immunophenotype, mitogen stimulation response, CD40 ligand and inducible costimulator expression, transmembrane activator and CAML interactor sequencing, genomic analysis, andfluorescent in situ hybridization for deletions at 22q11.2. Common variable immunodefi -ciency was diagnosed and replacement therapy with immune globulin intravenous was initiated. The parvovirus DNA level declined by half over 3 months and was undetectable at 15 months. Constitutional symptoms improved but arthritis persisted and eosinophilic fasciitis eventually developed. This case demonstrates that persistent parvo-virus infection may be a presenting feature of humoral immune
de-ficiency and can mimic juvenile rheumatoid arthritis. The infection may respond to immune globulin intravenous therapy. Pediatrics
2012;130:e1711–e1715
AUTHORS:Sarah T.M. Adams, MD,aKara M. Schmidt, MD,a
Karen M. Cost, PhD,band Gary S. Marshall, MDa
aDepartment of Pediatrics, University of Louisville School of
Medicine, Louisville, Kentucky; andbClinical Immunology
Laboratory, Kosair Children’s Hospital, Louisville, Kentucky
KEY WORDS
human parvovirus B19, common variable immunodeficiency, juvenile idiopathic arthritis
ABBREVIATIONS
CVID—common variable immunodeficiency Ig—immunoglobulin
IGIV—immune globulin intravenous JIA—juvenile idiopathic arthritis RA—rheumatoid arthritis
Drs Adams, Schmidt, and Marshall provided medical care to the patient; Dr Adams abstracted the clinical data and contributed to its analysis and interpretation; Drs Schmidt, Cost, and Marshall contributed to analysis and interpretation of the clinical data; Dr Marshall conceived and designed the project; and all authors participated in review and substantive revision of the manuscript and approved thefinal version of the manuscript as submitted.
Dr Adams is currently in private practice with Greensboro Pediatricians, Inc, Greensboro, North Carolina.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-2556 doi:10.1542/peds.2011-2556
Accepted for publication Jun 26, 2012
Address correspondence to Gary S. Marshall, MD, Division of Pediatric Infectious Diseases, University of Louisville School of Medicine, 571 S. Floyd St, Suite 321, Louisville, KY 40202. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
tent infection, described in patients with HIV infection,2therapeutic
immu-nosuppression,3and primary cellular
immunodeficiency,4 is not classically
associated with humoral immune de-fects. This report describes a 6-year-old boy who presented with persistent par-vovirus infection and arthritis and was found to have common variable immu-nodeficiency (CVID).
PATIENT PRESENTATION
A 6-year-old white boy presented with a 6-month history of decreased energy and 5-pound (2.3-kg) weight loss. Other symptoms included cough, dyspnea, malaise, decreased appetite, and ab-dominal pain. For the preceding month he was pale, had night sweats associ-ated with temperatures to 101°F (38.3°C), and had swelling and stiffness in large and small joints that impaired his usual activities. Nine months before presen-tation, he began experiencing watery, nonbloody diarrhea, which lasted until 3 months before presentation.
On physical examination he appeared chronically ill (Fig 1), with weight, height, and BMI below the 10th percentile. He had pale conjunctivae, a 2/6 systolic murmur, multiple small, mobile, nonten-der anterior cervical lymph nodes, and
range of motion of his shoulders, elbows, wrists, and metacarpophalangeal, proxi-mal interphalangeal, knee, ankle, and metatarsophalangeal joints. There were no skin lesions or rash.
Laboratory investigation showed mi-crocytic anemia (hemoglobin 6.8 gm/dL, mean corpuscular volume 55.8 fL, re-ticulocyte count 1.3%), eosinophilia (22%, 1562 cells/mL), and thrombocy-tosis (691 000 cells/mL). Iron level was ,10mg/dL and iron saturation was 3%, but total iron-binding capacity, trans-ferrin, and ferritin were normal. Erythro-cyte sedimentation rate was 70 mm/h and C-reactive protein level was 139 mg/ L. Renal, hepatic, and muscle laboratory evaluation were normal; total protein was 5.4 mg/dL and albumin was 2.7 mg/dL.
Endoscopic gastric biopsy showed moderate chronic active gastritis, but biopsies of the esophagus, duodenum, terminal ileum, cecum, colon, and rectum were normal. Computed tomography demonstrated axillary and inguinal lymphadenopathy with a soft tissue mass abutting the head of the pancreas. Laparotomy revealed mesenteric lymph-adenopathy, with enlarged lymph nodes behind the head of the pancreas. Bi-opsies from these showed sinus his-tiocytosis with mild eosinophilia. Flow
phocytes (57% to 68% T cells, 29% to 38% B cells) without evidence of mono-clonality or aberrant antigen expression.
Radiographic studies revealed osteo-porosis, periarticular soft tissue swell-ing, and advanced bone maturation. Results of the following tests were normal or negative: rheumatoid factor; antinuclear antibody screen; C3 and C4 levels; antibodies to proteinase-3, myeloperoxidase, cyclic citrullinated peptide, dsDNA, RNP, Smith, SS-A (Ro), SS-B (La), Scl-70, thyroid peroxidase, mitochondria M2, myocardial cells, parietal cells, actin, striated muscle, and ribosomal P. The patient was se-ronegative for Epstein-Barr virus and cytomegalovirus but was not tested for mycoplasma. Stool culture was not done. Parvovirus B19 DNA was detected in whole blood by polymerase chain reaction at a copy number of 10 300 copies/mL (Fig 2). Both IgG and IgM antibodies to parvovirus B19 were detected (IgG 2.61 index value, IgM 2.20 index value).
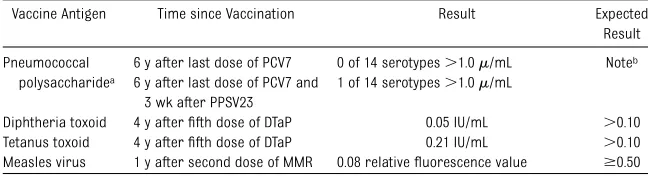
Immunologic evaluation revealed hypogammaglobulinemia with normal immunophenotype and lymphocyte function (Table 1) and abnormal anti-body responses to vaccination (Table 2). HIV antibody and HIV DNA polymerase chain reaction on blood were negative. CD40 ligand and inducible costimulator expression were normal. Fluorescent in situ hybridization showed no deletions at 22q11.2. Sequencing of the gene for transmembrane activator and CAML interactor, also known as TNFRSF13B, or tumor necrosis factor receptor super-family, member 13B, showed homozy-gosity for a synonymous mutation, c.81G.A, which is not associated with CVID. Microarray genome analysis failed to reveal major deletions in the genes for CD19, CD20, and CD81; dele-tions in B cell-activating factor re-ceptor, also known as TNFRSF13C, or FIGURE 1
tumor necrosis factor receptor super-family, member 13C, were not assessed by this method, and sequencing of CD19, CD20, CD81, and B cell-activating factor receptor was not done. No mutations were found in the X-linked lymphoproliferative syndrome gene baculoviral IAP repeat-containing pro-tein 4, also known as XIAP, or X-linked inhibitor of apoptosis. The diagnosis of CVID was made based on the demon-strated quantitative and qualitative humoral immune deficiency in the ab-sence of a defined cellular defect or syndrome. Interestingly, before the presenting illness he had had re-current episodes of acute otitis media.
Two months after presenting, the pa-tient was started on immune globulin intravenous (IGIV) replacement therapy at a dose of 400 mg/kg per month. Parvovirus DNA levels in the blood de-clined during the first 3 months of therapy and were consistently unde-tectable beginning at 15 months (Fig 2). The arthritis responded initially to corticosteroids and naproxen, and within a few months, the anemia, eo-sinophilia, and thrombocytosis re-solved; however, arthritis persisted, and methotrexate was started at 1 mg/ kg weekly. At 5 months, etanercept was added at a dosage of 0.4 mg/kg twice weekly. At 8 months, methotrexate was
discontinued because of transaminase elevation.
Fifteen months after starting IGIV, he was gaining weight (Fig 1) but still had active arthritis. Adalimumab 20 mg every 2 weeks was substituted for etanercept. Eighteen months into his disease course, he developed sclero-dermatous changes over both lateral ankles, with no peau d’orange, as well as recurrence of eosinophilia (1425 cells/mL). Interleukin-5 was slightly el-evated at 6 pg/mL. Repeat endoscopy showed mild gastritis and duodenitis with increased tissue eosinophils. Full-thickness skin biopsy revealed marked collagen deposition within the dermis and subcutis and sparse perivascular and interstitial chronic inflammation with lymphocytes and eosinophils, con-sistent with eosinophilic fasciitis. Echo-cardiogram, pulmonary function tests, and computed tomography of the chest were normal. Weekly and then monthly intravenous pulses of corticosteroids were started; adalimumab was dis-continued and abatacept was started.
Two years out from diagnosis and initia-tion of immune globulin replacement and disease-modifying antirheumatologic drugs, he had not experienced neurop-athies, myositis, weakness, Raynaud phenomenon, or ophthalmic involve-ment. Serial pulmonary function tests were normal and he had no unusual, recurrent, or opportunistic infections.
DISCUSSION
Human parvovirus B19 replicates in erythroid progenitor cells.5 In
immu-nocompetent patients, acute viremia resolves within 1 week, coincident with the appearance of specific IgM anti-body. Persistent parvovirus infection has been associated with deficient an-tibody responses to the capsid pro-tein.6 It is not surprising, therefore,
that a patient with humoral immune
de-ficiency, as the patient presented here, might develop persistent parvovirus FIGURE 2
Parvovirus genome copies in whole blood and serum IgG level over time.
TABLE 1 Immunologic Investigations at the Time of Presentation
Parameter Specimen Aa Specimen Ba Reference Rangeb
IgG, mg/dL 416 425 608–1229 IgG1, mg/dL 329 240 330–1065 IgG2, mg/dL 30 27 57–345 IgG3, mg/dL 135 107 8–126 IgG4, mg/dL 9 6 2–116 IgA, mg/dL 26 33 33–200 IgM, mg/dL 29 27 46–197 IgE, IU/mL ,5 ,5 0–70 T cells (CD3+), % of lymphocytesc 54 71 55–82
Helper T cells (CD4+), % of lymphocytes, (n/mm3) 37 (328) 48 (534) 31–59 (553–1359) Suppressor T cells (CD8+), % of lymphocytes (n/mm3) 17 (151) 23 (256) 14–29 (249–796) Activated T cells (HLA-DR+/CD3+), % of T cells 9 5 0–7 Naïve T cells (CD45RA+/CD4+), % of T cells (n/mm3) 26 (230) 36 (401) 3–38 (44–869) Memory T cells (CD45RO+/CD4+), % of T cells (n/mm3) 9 (80) 13 (145) 16–46 (92–1040) B cells (CD19+), % of lymphocytesc 40 (354) 26 (289) 6–25 (40–827)
Kappa:Lambda ratio (surface expression) 1.3:1 1.4:1 2:1 NK cells (CD56+/CD16+/CD32), % of lymphocytes (n/mm3) 3 (27) 4 (45) 3–10 (34–308) Lymphocyte stimulation with phytohemagglutinin (72 h)
CD25 expression, % — 80 70–90 S-phase, % — 30.2 19.3–36.9 aTwo specimens over a 2-wk period before immune globulin replacement was initiated.
bTwo SDs around the mean.
cThe following lymphocyte phenotypes were not assessed: T-regs, CD4+/CD95+, CD19+/CD21(low).
infection; however, to our knowledge, only 1 other case of persistent infection in the setting of CVID has been repor-ted. There, parvovirus infection man-ifested as erythema infectiosum with reticulocytopenia and was not the presenting feature of the immune
de-ficiency.7IGIV was started 2 weeks into
the illness, resulting in prompt re-covery of the reticulocyte count. Two months later, parvovirus DNA was not detectable.
We are unaware of other reports of persistent parvovirus infection leading to a diagnosis of CVID. In our case and the case cited in the preceding para-graph, the clinical and virologic response to IGIV, which contains antibodies to parvovirus,8 supports a
role for humoral immune deficiency in predisposing to persistent parvovirus infection (in the present case, the en-dogenous antibody response was quan-titatively or quanquan-titatively inadequate to clear the virus). There are 2 reports of persistent parvovirus infection in apparently healthy hosts who were treated with IGIV; in one, arthritis and viremia resolved, whereas in the other arthritis resolved but viremia persisted.9,10
Autoimmune diseases occur in about 20% of patients with CVID.11–13In those
with arthritis, synovial biopsy may demonstrate hyperplasia, as is typical of rheumatoid arthritis (RA), but with few B cells and no plasma cells.11 It
is possible that some cases of RA in patients with CVID are caused by un-recognized parvovirus infection. One report described 2 young children who presented with arthritis and anemia and were later diagnosed with CVID.14
They were treated with IGIV and both recovered; in light of the present case, one might wonder whether these patients might have had persistent parvovirus infection. It is worth noting here that a dermatomyositislike syn-drome has been described in patients with X-linked agammaglobulinemia in association with chronic enterovirus or adenovirus infection.15
Parvovirus causes chronic arthritis in adults.16 In children, parvovirus
in-fection can mimic juvenile idiopathic arthritis (JIA). In a series of 22 chil-dren with recent parvovirus infection and arthritis and/or arthralgia, 6 developed chronic arthritis that
ful-filled the diagnostic criteria of JIA.17
Another study of 50 children with JIA
pared with 0% of a control group. Similarly, in a study of 74 children with active RA, 30% had detectable amounts of parvovirus DNA in serum, as com-pared with 7% of 124 controls; 22% had parvovirus DNA in synovial fluid.19 It
is not clear whether the arthritis of persistent parvovirus viremia, which is presumably attributable to the for-mation of circulating antigen-antibody complexes, simply mimics that of JIA and RA, or whether parvovirus in-fection has a more direct role in the pathogenesis of rheumatic disease. It is possible that some of the im-provement seen in our patient resul-ted from the antiinflammatory effects of IGIV.
Our patient presented with polyarthritis and subsequently developed eosino-philic fasciitis, of which there are fewer than 35 reported pediatric cases.20
Eosinophilic fasciitis is a subtype of deep morphea with unclear etiology, and arthritis occurs in 40% of patients.21
Interestingly, patients can present with polyarthritis and subsequently develop eosinophilic fasciitis, as did our pa-tient.22 The few reported cases of
eosinophilic fasciitis in patients with CVID have been in adults,23 although
a 13-year-old child presented with pol-yarthritis and IgA deficiency and de-veloped eosinophilic fasciitis 4 months later.24
Persistent parvovirus infection can be a presenting feature of CVID, and im-mune globulin replacement can result in clearance of viremia. Chronic poly-articular arthritis or anemia in a pa-tient with CVID should prompt an evaluation for parvovirus infection.
REFERENCES
1. Brown KE, Young NS. Parvovirus B19 in human disease.Annu Rev Med. 1997;48(1): 59–67
2. Abkowitz JL, Brown KE, Wood RW, Kovach NL, Green SW, Young NS. Clinical relevance of parvovirus B19 as a cause of anemia in
patients with human immunodeficiency virus infection. J Infect Dis. 1997;176(1): 269–273
Pneumococcal polysaccharidea
6 y after last dose of PCV7 0 of 14 serotypes.1.0m/mL Noteb
6 y after last dose of PCV7 and 3 wk after PPSV23
1 of 14 serotypes.1.0m/mL
Diphtheria toxoid 4 y afterfifth dose of DTaP 0.05 IU/mL .0.10 Tetanus toxoid 4 y afterfifth dose of DTaP 0.21 IU/mL .0.10 Measles virus 1 y after second dose of MMR 0.08 relativefluorescence value $0.50
DTaP, diphtheria, tetanus, acellular pertussis vaccine; IU, international units; MMR, measles, mumps, rubella vaccine; PCV7, pneumococcal conjugate vaccine, 7-valent; PPSV23, pneumococcal polysaccharide vaccine, 23-valent.
aMeasured serotypes: 1, 3, 4*, 5, 6B*, 7F, 8, 9N, 9V*, 12F, 14*, 18C*,19
F*, 23F* (*included in PCV7; all measured serotypes included in PPSV23).
bAnamnestic responses to PCV7 serotypes, and de novo responses to non-PCV7 serotypes, are expected after immunization
3. Cavallo R, Merlino C, Re D, et al. B19 virus infection in renal transplant recipients.
J Clin Virol. 2003;26(3):361–368
4. Kurtzman G, Frickhofen N, Kimball J, Jenkins DW, Nienhuis AW, Young NS. Pure red-cell aplasia of 10 years’duration due to per-sistent parvovirus B19 infection and its cure with immunoglobulin therapy.N Engl J Med. 1989;321(8):519–523
5. Young NS, Brown KE. Parvovirus B19.N Engl J Med. 2004;350(6):586–597
6. Kurtzman GJ, Cohen BJ, Field AM, Oseas R, Blaese RM, Young NS. Immune response to B19 parvovirus and an antibody defect in persistent viral infection. J Clin Invest. 1989;84(4):1114–1123
7. Chuhjo T, Nakao S, Matsuda T. Successful treatment of persistent erythroid aplasia caused by parvovirus B19 infection in a patient with common variable immuno-deficiency with low-dose immunoglobulin.
Am J Hematol. 1999;60(3):222–224 8. Modrof J, Berting A, Tille B, et al.
Neutral-ization of human parvovirus B19 by plasma and intravenous immunoglobulins. Trans-fusion. 2008;48(1):178–186
9. Ogawa E, Otaguro S, Murata M, et al. In-travenous immunoglobulin therapy for se-vere arthritis associated with human parvovirus B19 infection. J Infect Chemo-ther. 2008;14(5):377–382
10. Bozzola E, Krzysztofiak A, Cortis E. Neurolog-ical impairment and arthritis in an immu-nocompetent child with human parvovirus B19 chronic infection.Infez Med. 2010;18(3): 187–190
11. Agarwal S, Cunningham-Rundles C. Auto-immunity in common variable immunode-ficiency. Curr Allergy Asthma Rep. 2009;9 (5):347–352
12. Knight AK, Cunningham-Rundles C. In-flammatory and autoimmune complications of common variable immune deficiency.
Autoimmun Rev. 2006;5(2):156–159 13. Conley ME, Park CL, Douglas SD. Childhood
common variable immunodeficiency with autoimmune disease. J Pediatr. 1986;108 (6):915–922
14. Salaria M, Singh S, Dutta U, Sehgal S, Kumar L. Arthritis in hypogammaglobulinemia. In-dian Pediatr. 1998;35(4):367–370
15. Lederman HM, Winkelstein JA. X-linked agammaglobulinemia: an analysis of 96 patients.Medicine (Baltimore). 1985;64(3): 145–156
16. Naides SJ, Scharosch LL, Foto F, Howard EJ. Rheumatologic manifestations of human parvovirus B19 infection in adults. Initial two-year clinical experience. Arthritis Rheum. 1990;33(9):1297–1309
17. Nocton JJ, Miller LC, Tucker LB, Schaller JG. Human parvovirus B19-associated
arthritis in children. J Pediatr. 1993;122 (2):186–190
18. Gonzalez B, Larrañaga C, León O, et al. Parvovirus B19 may have a role in the pathogenesis of juvenile idiopathic arthri-tis.J Rheumatol. 2007;34(6):1336–1340 19. Lehmann HW, Knöll A, Küster RM, Modrow S.
Frequent infection with a viral pathogen, parvovirus B19, in rheumatic diseases of childhood. Arthritis Rheum. 2003;48(6): 1631–1638
20. Ortega-Loayza AG, Merritt BG, Groben PA, Morrell DS. Eosinophilic fasciitis in a fe-male child.J Am Acad Dermatol. 2008;58(5 suppl 1):S72–S74
21. Varga J, Kähäri VM. Eosinophilia-myalgia syndrome, eosinophilic fasciitis, and re-latedfibrosing disorders.Curr Opin Rheu-matol. 1997;9(6):562–570
22. Olson NY, Lindsley CB, Kepes JJ. Eosinophilic fasciitis presenting as inflammatory poly-arthritis.Pediatrics. 1986;78(3):512–514 23. Di Gioacchino M, Masci S, Paolini F, et al.
Common variable immunodeficiency and eosinophilic fasciitis.Eur J Dermatol. 2002; 12(1):73–74
24. Ching DW, Petrie JP. Childhood eosinophilic fasciitis presenting as inflammatory poly-arthritis and associated with selective IgA deficiency.Ann Rheum Dis. 1991;50(9):647– 648
DOI: 10.1542/peds.2011-2556 originally published online November 5, 2012;
2012;130;e1711
Pediatrics
Services
Updated Information &
http://pediatrics.aappublications.org/content/130/6/e1711 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/130/6/e1711#BIBL This article cites 24 articles, 3 of which you can access for free at:
Subspecialty Collections
ub
http://www.aappublications.org/cgi/collection/allergy:immunology_s Allergy/Immunology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2011-2556 originally published online November 5, 2012;
2012;130;e1711
Pediatrics
Sarah T.M. Adams, Kara M. Schmidt, Karen M. Cost and Gary S. Marshall
B19 Infection
Common Variable Immunodeficiency Presenting With Persistent Parvovirus
http://pediatrics.aappublications.org/content/130/6/e1711
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.