Executive Function and Academic
Outcomes in Children Who
Were Extremely Preterm
Danielle S. Costa, MSc, a Débora M. Miranda, MD, PhD, b, c Alice C. Burnett, PhD, d, e Lex W. Doyle, MD, d, e, f, g
Jeanie L.Y. Cheong, MD, d, e, f Peter J. Anderson, PhD, e, h on behalf of the Victorian Infant Collaborative Study Group
OBJECTIVES: Cognitive and behavioral impairments of children born extremely preterm (EP)
(<28 weeks’ gestation) and extremely low birth weight (ELBW) (<1000 g) may change with
age. We assessed the individual stability of behavioral executive function (EF) from 8 to 18 years of age in children born EP or ELBW and their academic outcomes.
METHODS: Participants comprised 180 children born EP or ELBW from a large geographic
cohort. We investigated the frequency of 4 developmental groups (persistent, remitting, late-onset, and typical development) on the basis of dichotomized scores (typical versus elevated) at ages 8 and 18 years in 2 indices (the Behavioral Regulation Index [BRI] and the Metacognition Index [MCI]) of the parental form of the Behavior Rating Inventory of Executive Function. Adolescent academic outcomes were measured by using the word reading, spelling, and math computation subtests of the Wide Range Achievement Test, Fourth Edition.
RESULTS: Most participants had a typical EF (BRI 61%, MCI 53%), followed by persistent (BRI
15%, MCI 16%), late-onset (BRI 12%, MCI 19%), or remitting (BRI 12%, MCI 13%) executive difficulties. Groups with executive impairments at age 18 years (persistent and late onset) had poorer academic outcomes than the typical and remitting groups. Shifting impairment categories between 8 and 18 years old was relevant to later academic outcomes.
CONCLUSIONS: Most children showed stable and age-appropriate EF, although persistent and
transient difficulties were observed and related to uneven academic outcomes. Studying the origins and consequences of the developmental stability of EF may contribute to the development of interventions to decrease the adverse neurodevelopmental outcomes of preterm birth.
abstract
aCoordenação de Aperfeiçoamento de Pessoal de Nivel Superior, Ministry of Education of Brazil, Brasília, Brazil; bDepartment of Pediatrics, Federal University of Minas Gerais, Belo Horizonte, Brazil; cConselho Nacional de
Desenvolvimento Científico e Tecnológico, Ministry of Science, Technology, and Innovation of Brazil, Brasília, Brazil; dNeonatal Services, Royal Women’s Hospital, Parkville, Victoria, Australia; eClinical Sciences, Murdoch
Childrens Research Institute, Parkville, Victoria, Australia; fDepartment of Obstetrics and Gynecology, and gDepartment of Pediatrics, Melbourne Medical School, University of Melbourne, Parkville, Victoria, Australia;
and hMonash Institute of Cognitive and Clinical Neurosciences, School of Psychological Sciences, Monash
University, Clayton, Victoria, Australia
Ms Costa conceptualized and designed the study, conducted the initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript; Dr Miranda conceptualized and designed the study, contributed to the interpretation of data analysis, drafted the initial manuscript, and reviewed and revised the manuscript; Dr Burnett conceptualized and designed the study, contributed to the data collection and interpretation of data analysis, and reviewed and revised the manuscript; Drs Doyle, Cheong, and Anderson obtained funding, conceptualized and designed the study, contributed to the interpretation of data analysis, and reviewed and revised the
What’s KnoWn on this subject: Children born
extremely preterm are at risk for impairments in executive functioning (EF) and academics. The stability of executive impairments across childhood is not known, but it needs to be explored because developmental differences in EF may relate to academic outcomes.
What this study adds: Four distinct developmental
groups from 8 to 18 years of age were described in children born extremely preterm. Academic performance in adolescence was related to EF stability, with those with typical and remitting EF profiles showing better outcomes.
to cite: Costa DS, Miranda DM, Burnett AC, et al. Executive Function and Academic Outcomes in Children Who Were
Despite remarkable advances in medical care, children born extremely preterm (EP) (<28 weeks’
gestation) and extremely low birth weight (ELBW) (<1000 g) continue to be at risk for impairments in cognitive, social, behavioral, and educational functioning.1–3
However, the nature and severity of impairments may change with age, leading to uncertainty as to which developmental difficulties constitute a transient delay or a persistent deficit.4, 5 Whereas transient
impairments have been reported in cognition and behavior for preterm survivors, 6, 7 more severe and
persistent difficulties may be seen in children born EP.8, 9 It is also known
that specific behavioral and cognitive problems, such as emotional
regulation impairments, are unlikely to emerge until later in life.10–12
Executive function (EF) refers to a set of cognitive control processes, such as working memory, inhibition, shifting and control of attention, planning, reasoning, problem-solving, and impulse control.13, 14 These
higher-order skills of executive control emerge early in life, with ongoing maturation continuing into adolescence and early adulthood.15
Compared with term-born controls, children born EP or ELBW are at increased risk for EF deficits throughout development, 1, 16, 17 with a
tendency to show slower age-related progress in both performance-based and questionnaire measures of EF.1, 12
Difficulties in EF have been linked with reduced academic achievement of preterm survivors.18–20 However,
research to date has not explored differential EF stability within individuals born preterm. For example, some individuals may have persistent difficulties, whereas others display improved or deteriorating functioning with time.10, 21 Cognitive
performance in individuals born preterm is markedly variable,
22 yet most researchers will not
differentiate those with a dysfunction
from those with typical functioning. Disregard for individual differences may lead to an unbalanced focus on problematic development over the investigation of optimal human functioning.23 Importantly, it is also
unknown whether distinct stability subgroups in EF are related to different outcomes in children born EP or ELBW.
Our first aim in the current study was to assess the individual stability of behavioral EF from 8 to 18 years of age in a large geographic sample of children born EP or ELBW by assessing the frequency of the following 4 possible groups: persisting impairment, remitting impairment, late-onset impairment, and typical development. The second aim was to compare reading, spelling, and math computation at 18 years old among the different developmental subgroups,
hypothesizing that children born EP or ELBW with persisting executive dysfunction would exhibit poorer academic achievement than those with remitting executive dysfunction.
Methods Participants
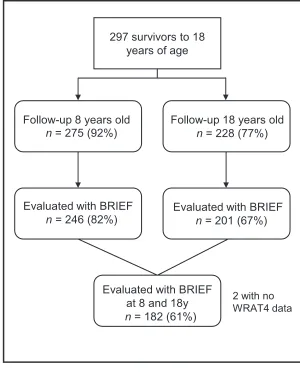
Participants comprised all infants born EP or ELBW in the state of Victoria, Australia, in 1991 and 1992. There were 298 survivors to 2 years of age and 297 survivors to 18 years of age, with follow-up assessments performed at ages 2, 5, 8, and 18 years and corrected for prematurity.8, 24–26
The recruitment and follow-up assessments were approved by the Human Research Ethics Committees of all participating sites (The Royal Women’s Hospital, Mercy Hospital for Women, Monash Medical Centre, and The Royal Children’s Hospital, Melbourne, Australia). Only participants with complete parental reports of the Behavior Rating Inventory of Executive Function (BRIEF)27 at ages 8 and 18
years and who completed the Wide
Range Achievement Test, Fourth Edition (WRAT4)28 at 18 years were
included. No exclusion criteria other than not having complete data sets were applied. Participants older than 17 years and the parents of those younger than 18 years gave written, informed consent for participation.
Measures
Behavioral EF
The parental form of the BRIEF27 was
used to assess everyday behavioral executive difficulties at 8 and 18 years of age. The BRIEF is valid, reliabile, 27 and is used extensively
in research and clinical settings to assess executive dysfunction at home, school, and social situations.29
It consists of 86 items, which generate 8 clinical scales (Inhibit, Shift, Emotional Control, Initiate, Working Memory, Plan and Organize, Organization of Materials, and Monitor) and 2 broader indices (the Behavioral Regulation Index [BRI] and the Metacognition Index [MCI]). For this study, the 2 broad indices were used. The BRI is a composite of the Inhibit, Shift, and Emotional Control scales, whereas the MCI is a composite of the Initiate, Working Memory, Plan and Organize, Organization of Materials, and Monitor scales. Scores were age- and sex-normed to a t-distribution (a mean of 50 and SD of 10).27 Scores
≥60 (ie, 1 SD from the mean) were classified as “elevated executive difficulties.”
Academic Achievement
The WRAT427 was used to measure
participants’ single-word reading, spelling, and math computation performance at 18 years old. The raw scores were converted to age-standardized scores with a mean of 100 and SD of 15 by using the WRAT4 normative data.27 For
with an integration aide or other intervention) at 8 years old.
Medical and Social Characteristics
Perinatal and neonatal variables such as gestational age, birth weight, major brain injury on cranial ultrasound (grades 3 and 4 intraventricular hemorrhage or cystic periventricular leukomalacia), postnatal corticosteroid treatment, and major neonatal surgery were collected. Social characteristics were collected at the 8-year follow-up wave and included social class (categorized as lower if the major income earner in the family had an unskilled occupation or was unemployed), maternal age and education (classified as low if the mother reported <12 years of schooling), and multilingual status (the family spoke languages other than English at home). Additionally, adolescents’ full-scale IQ was estimated with the Wechsler Abbreviated Scale of Intelligence.30
These variables were shown to influence preterm outcomes, including academic performance.8
data analysis
For each BRIEF Index (ie, BRI and MCI) participants were classified into 1 of 4 possible subgroups according to their EF at 8 and 18 years old. The typical subgroup consisted of participants with T-scores <60 at both time points, whereas the persistent subgroup consisted of participants with T-scores ≥60 at both time points. The remitting group consisted of participants with an elevated score (≥60) at 8 years but not 18 years of age, whereas the late-onset difficulties group was characterized by a T-score ≥60 at 18 years old only.
Baseline characteristics were compared among participants and nonparticipants born EP or ELBW as well as among the EF stability subgroups. For categorical data, when an χ2 test could not be
performed because of the sample size, comparisons were made by using the Fisher’s exact test with a Monte Carlo approach (confidence level = 99%, K (number of samples) = 10000). For continuous data, a multivariable analysis
of variance was performed for parametric data and the Kruskal–
Wallis test for nonparametric data. Differences in academic performance at 18 years old among the groups were calculated through generalized estimating equations (GEE) with a linear regression model, robust estimators, and an exchangeable structure for working correlation matrices. This strategy was chosen to allow for nonindependence of siblings from multiple pregnancies. For the GEE parameter estimates, the academic variables were transformed into z scores by using the means and SDs of the sample to facilitate the interpretation of effect sizes. Secondary GEE analyses were performed by removing participants with an IQ ≤70 at 18 years old and adjusting for any significant differences in perinatal and sociodemographic characteristics. We acknowledge that there are multiple comparisons, and thus, we interpreted the results by the magnitude of the difference among groups rather than adjusting the P value by the number of tests performed. The larger the difference among groups, the higher the chance that the results are clinically meaningful.31 In the current
study, effect sizes were interpreted by using Cohen’s conventions (small: d = 0.2, medium: d = 0.5, and large: d = 0.8).32 The analyses were
performed in SPSS 22.0.33
Results
sample Progression From 8 to 18 years of age
As shown in Fig 1, 180 of the original 297 participants born EP or ELBW had complete data sets to be included in the analyses.
Perinatal and sociodemographic characteristics were similar among participants and nonparticipants (Table 1).
developmental stability of behavioral eF in eP and elbW adolescents
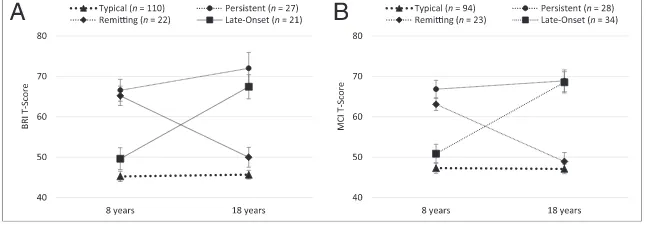
For the BRI, the majority of participants (n = 110, 61%) were classified as typical at both time points, whereas 15% (n = 27) had persistently elevated scores, 12% (n = 22) had remitting difficulties, and 12% (n = 21) had late-onset difficulties. Thus, most participants had a stable EF performance, with only 24% changing categories between 8 and 18 years old. For the MCI groups, 53% (n = 94) were classified as typical at both time points, 16% (n = 28) had persistent difficulties, 13% (n = 23) had remitting difficulties, and 19% (n = 34) had late-onset difficulties. Again, only a minority (32%) changed categories between 8 and 18 years old. These developmental groups are illustrated in Fig 2.
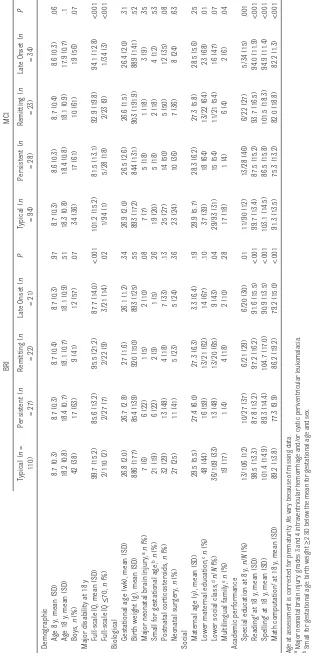
Demographic, biological (perinatal and neonatal variables), and social characteristics of the EF stability subgroups are presented in Table 2. There was evidence of group differences in sex, IQ, and social
FiGuRe 1
class. In general, the typical group for both the BRI and MCI had a higher proportion of girls, families of higher social class, and higher mean IQ scores than the persistent, late-onset, and remitting groups. Regarding the percentage of participants receiving special education at 8 years of age, children with typical development were less likely to receive additional support, whereas children with persistent EF difficulties were more likely to have an integration aide or other intervention.
eF stability and academic Performance
Reading, spelling, and math computation means and SDs for
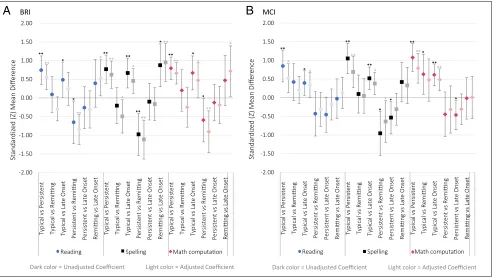
the EF development groups are displayed in Table 2, and Fig 3 shows comparisons among the groups. Adjusted results exclude participants with an IQ ≤70 at 18 years old and include significant confounders (eg, lower social class for the BRI and lower maternal education and multilingualism for the MCI). There was evidence of differences between some of the BRI and MCI stability subgroups, but not all of them (Fig 3). For both the BRI and MCI, the typical subgroup outperformed the persistent and late-onset subgroups for all academic outcomes. For the BRI, the persistent subgroup performed poorer than the remitting difficulties subgroup for all academic
outcomes, and the remitting subgroup performed better than the late-onset subgroup in reading and spelling in the adjusted analyses. For the MCI, the persistent subgroup had lower spelling scores than those with remitting difficulties.
discussion
We observed that most participants born EP or ELBW in this study had a stable development in parent-reported EF from 8 to 18 years of age. Importantly, more than half of our participants born EP or ELBW had an age-appropriate EF based on parental reports at 8 and 18 years, and by late adolescence, only 27% had elevated BRI scores, and 35% had elevated MCI scores. Only 12% to 13% of children had persisting problems, whereas 24% to 32% had transient difficulties. Thus, although it is well established that children born EP are at risk for executive dysfunction, 1, 12, 16, 17 based on
parental reports, the rates of children with persisting issues were low. Previous studies investigating parent-reported EF in the population born EP have reported significantly increased risk for behavioral problems.34–36 Behavioral and
emotional regulation have been suggested to be a special concern for parents, 18, 37 although in our
sample, a slightly higher proportion of parents reported MCI difficulties compared with BRI problems. Researchers in other studies using the BRIEF have also noted MCI problems, although the patterns are not identical. For example, Luu et al36 found that adolescents born
with low birth weight were at risk for behavioral problems comprised in the MCI but not in the BRI, and Ritter et al38 reported significant
differences between children born very preterm and controls only in the Working Memory subscale and not in BRI scales, such as Inhibition and Shift. Recently, we reported
table 1 Characteristics of Participants and Nonparticipants
Included (n = 180) Not Included (n = 118) P
Age 8 y, mean (SD) 8.7 (0.3) 8.7 (0.4)a .12
Age 18 y, mean (SD) 18.2 (0.8) 18.2 (0.8)b .71
Boys, n (%) 80 (44) 58 (49) .43
Gestational age (wk), mean (SD) 26.7 (2.0) 26.7 (1.8) .65
Birth weight (g), mean (SD) 886 (163) 890 (158) .76
Major neonatal brain injuryc, n (%) 16 (9) 16 (14) .20
Small for gestational aged, n (%) 30 (17) 16 (14) .47
Postnatal corticosteroids, n (%) 56 (31) 42 (36) .42
Neonatal surgery, n (%) 48 (27) 29 (25) .69
Maternal age (y), mean (SD) 29.0 (5.82) 27.8 (5.7) .07
Lower maternal educatione, n/N (%) 91/179 (51) 49/90 (54) .58
Lower social classf, n/N (%) 71/177 (40) 46/92 (50) .12
Multilingual familyg, n/N (%) 26/180 (14) 24/103 (23) .06
Age at assessment is corrected for prematurity. Ns vary because of missing data. aN = 95.
bN = 42.
c Major neonatal brain injury: grades 3 and 4 intraventricular hemorrhage and/or cystic periventricular leukomalacia. d Small for gestational age: birth weight ≥2 SD below the mean for gestational age and sex.
e Lower maternal education: <12 years of schooling.
f Lower social class: major income earner in the family has an unskilled occupation or unemployed. g Multilingual family: speaks languages other than English at home.
FiGuRe 2
table
2
BRI and MCI Subgroup Characteristics and Academic Performance
BRI MCI Typical ( n = 110) Persistent ( n = 27) Remitting ( n = 22)
Late Onset (
n = 21) P Typical ( n = 94) Persistent ( n = 28) Remitting ( n = 23)
Late Onset (
n
= 34)
P
Demographic Age 8 y, mean (SD)
8.7 (0.3) 8.7 (0.3) 8.7 (0.4) 8.7 (0.3) .97 8.7 (0.3) 8.6 (0.3) 8.7 (0.4) 8.6 (0.3) .06
Age 18 y, mean (SD)
18.2 (0.8) 18.4 (0.7) 18.1 (0.7) 18.1 (0.9) .51 18.3 (0.8) 18.4 (0.8) 18.1 (0.9) 17.9 (0.7) .1 Boys, n (%) 42 (38) 17 (63) 9 (41) 12 (57) .07 34 (36) 17 (61) 10 (61) 19 (56) .07
Major disability at 18 y Full-scale IQ, mean (SD)
99.7 (15.2) 85.6 (13.2) 95.5 (21.2) 87.7 (14.0) <.001 101.2 (15.2) 81.5 (13.1) 92.9 (19.8) 94.1 (12.8) <.001 Full-scale IQ ≤ 70, n (%) 2/110 (2) 2/27 (7) 2/22 (9) 3/21 (14) .02 1/94 (1) 5/28 (18) 2/23 (9) 1/34 (3) <.001
Biological Gestational age (wk), mean (SD)
26.8 (2.0) 26.7 (2.8) 27 (1.6) 26.1 (1.2) .34 26.9 (2.0) 26.5 (2.6) 26.6 (1.5) 26.4 (2.0) .31 Bir
th weight (g), mean (SD)
886 (177) 854 (139) 920 (150) 893 (125) .55 893 (172) 844 (131) 903 (191.9) 889 (141) .52
Major neonatal brain injury,
an (%) 7 (6) 6 (22) 1 (5) 2 (10) .08 7 (7) 5 (18) 1 (18) 3 (9) .35
Small for gestational age,
bn (%) 21 (19) 6 (22) 2 (9) 1 (5) .26 19 (20) 5 (18) 2 (18) 4 (12) .53 Postnatal cor ticosteroids, n (%) 32 (29) 13 (48) 4 (18) 7 (33) .13 25 (27) 14 (50) 5 (50) 12 (35) .08 Neonatal sur gery, n (%) 27 (25) 11 (41) 5 (23) 5 (24) .36 23 (24) 10 (36) 7 (36) 8 (24) .63
Social Maternal age (y), mean (SD)
29.5 (5.5) 27.4 (6.0) 27.3 (6.3) 3.3 (6.4) .19 29.9 (5.7) 28.3 (6.2) 27.3 (5.8) 28.5 (5.6) .25
Lower maternal education,
cn (%) 48 (44) 16 (59) 13/21 (62) 14 (67) .10 37 (39) 18 (64) 13/22 (64) 23 (68) .01
Lower social class,
dn / N (%) 36/109 (33) 13 (48) 13/20 (65) 9 (43) .04 29/93 (31) 15 (54) 11/21 (54) 16 (47) .07 Multilingual family, en (%) 19 (17) 1 (4) 4 (18) 2 (10) .28 17 (18) 1 (4) 6 (4) 2 (6) .04
Academic performance Special education at 8 y,
n / N (%) 13/106 (12) 10/27 (37) 6/21 (29) 6/20 (30) .01 11/90 (12) 13/28 (46) 6/22 (27) 5/34 (15) .001 Reading
f at 18 y, mean (SD)
98.5 (13.3) 87.8 (13.2) 97.2 (16.2) 91.6 (15.5) <.001 99.7 (13.4) 87.5 (15.2) 93.7 (16.5) 94.0 (11.9) <.001 Spelling
f at 18 y, mean (SD)
101.4 (14.9) 89.3 (14.4) 104.7 (17.0) 90.9 (13.5) <.001 103.1 (14.5) 86.5 (15.8) 101.5 (18.3) 94.9 (11.4) <.001 Math computation
f at 18 y, mean (SD)
89.2 (13.8) 77.3 (9.9) 86.2 (19.2) 79.2 (15.0) <.001 91.3 (13.5) 75.3 (13.2) 82.0 (18.8) 82.2 (1.3) <.001
Age at assessment is corrected for prematurity.
N
s vary because of missing data.
a Major neonatal brain injury: grades 3 and 4 intraventricular hemorrhage and/or cystic periventr
icular leukomalacia.
b Small for gestational age: bir
th weight
≥
2 SD below the mean for gestational age and sex.
c Lower maternal education: <12 years of schooling. d Lower social class: major income earner in the family has an unskilled occupation or unemplo
yed.
differences between children born EP and ELBW and children born at term in both the BRI and MCI, but the differences were stronger in the MCI domain for school-aged children.1
However, none of these previous studies examined developmental stability within individuals. Different responsiveness to environmental or biological risks might cause distinct behavioral courses and influence academic outcomes.39
Executive problems are thought to be related to academic achievement and learning skills, 34, 40 and the
current study provides additional evidence supporting this proposed relationship. In general, groups with executive difficulties at age 18 years tended to have poorer academic outcomes than those without concurrent executive difficulties. Our typical and remitting groups performed within 0.5 SD of the normative mean for the literacy measures but performed poorer
on the math computation subtest. Mathematics is an area of particular vulnerability for preterm children.41, 42
However, it is important to note that the reading and spelling subtests used in this study rely more on basic abilities of single-word recognition and coding, which are usually mature by late adolescence, whereas the math computation subtest includes complex arithmetic problems. The influence of core EFs, such as working memory, may decrease with time for reading but increase for mathematics.43 For the BRI,
shifting categories between 8 and 18 years of age was of extreme relevance for academic performance at 18 years old. Individuals with remitting difficulties performed comparably with individuals in the typical group, but in contrast, the late-onset group exhibited lower scores in all domains. Interestingly, for the MCI, the groups that changed categories between 8 and 18 years
old (ie, the remitting and late-onset groups) performed similarly on academic measures, intermediate between the typical and the persistent groups. As hypothesized, we observed that adolescents with remitting behavioral regulation difficulties performed better in all academic domains investigated when compared with adolescents with persistent behavioral problems. However, the same phenomenon was not as noticeable for the MCI, suggesting that early metacognitive difficulties may have a more lasting impact on later academic outcomes. Importantly, for some children born EP, executive difficulties are transient. Understanding the factors associated with improved functioning over time may inform intervention and management strategies for children with early EF difficulties. However, we also observed that for other children born EP, EF difficulties do not
FiGuRe 3
Standardized mean differences (SD) and 95% confidence intervals among the developmental subgroups in academic domains. Adjusted results are from
models excluding participants with an IQ ≤70 at 18 years old. A, includes lower social class for the BRI groups’ comparison. B, includes lower maternal
emerge until later in development, highlighting the need to monitor this population throughout childhood. Executive dysfunction is a common characteristic of several behavioral and emotional disorders, 3, 13 with
the clinical expression of many of these disorders changing during adolescence, 11 and the late-onset
group may help us understand the role of emerging EF problems on the adolescent onset of developmental disturbances such as emotional disorders.
Among the perinatal and sociodemographic variables investigated in the current study, differences in social background including maternal education, social class, and being in a multilingual family were observed among the developmental groups. Social disparities have a known effect on cognitive development, 44–46 and
in the population born preterm, socioeconomic factors seem to have an increasing influence over time.25, 47, 48 We were unable to
investigate this issue further in our sample because of a lack of statistical power. However, future studies are required to understand the factors influencing the variability of behavioral EF stability in children born preterm. The identification of individuals at risk, those who are particularly vulnerable to adversity, represents an opportunity to introduce targeted and timely interventions to ameliorate future outcomes.23 Interventions facilitating
child physiologic regulation, improving parent–child attachment, parenting style, maternal mental health, as well as elementary school programs enhancing self-regulation and planning skills, and working memory training are associated with higher levels of EF in children born preterm, particularly with early identification.49 Nevertheless,
variation in the effects of formal interventions is ubiquitous, and to acknowledge and understand factors
related to individual differences in development is of utmost importance for determining for whom and how specific interventions will work.23
This study was limited to participants born EP or ELBW. Although this is a group particularly at risk for developmental
impairments, research extending the spectrum of gestational age and birth weight is necessary. Cognitive and behavioral outcomes are inversely associated with the degree of prematurity.50
Therefore, it is reasonable to expect different rates of developmental stability according to the degree of prematurity. For example, the rate of persistent emotional and behavioral problems may be higher for children born EP, whereas the rate of children with remitting problems may be higher among those born moderately preterm.10 In
fact, little is known about individual changes of behavioral EF even for children with typical development. Cross-sectional studies have shown a decrease in reported EF problems with increasing age.51, 52 A previous
longitudinal study of our group showed a slight increase with age of BRI scores for children born preterm but not for term controls.1
Another limitation of our study is that we only used parental reports of behavioral EF. However, the demand for EFs varies according to environmental contexts (eg, home and school).18, 37 Also, cognitive
(performance-based) and behavioral measures of EF are probably covering distinct aspects of EF.53
For example, the association of the BRIEF with performance-based measures is generally modest.54
Cognitive measures of EF may uniquely explain a higher proportion of children’s academic performance, but behavioral measures of EF are complementary.53, 55 We did not
consider cognitive, educational, and behavioral interventions that the participants may have received
during childhood, which is a potential limitation because it has been proposed that EF can benefit from interventions targeting cognitive and behavioral enhancement.13 At
any rate, we observed that children with persistent EF difficulties were more likely to receive additional academic support at 8 years old. Strengths of the study include a geographically selected sample born EP or ELBW, with no significant differences between participants and nonparticipants (eg, children lost to follow-up) with regard to perinatal and sociodemographic characteristics. Moreover, the follow-up period of ∼10 years is associated with remarkable changes in human development related to self-control.56
There is an undeniable heterogeneity in individual responses to adversity, 35 and
outcomes after preterm birth are also characterized by
interindividual variability. In this study, we have demonstrated 4 stability subgroups for EF in children born EP or ELBW, which were associated with different academic outcomes in adolescence. Studying the origins and consequences of the distinct stability groups of children born preterm may contribute to the development of efficient interventions to decrease the adverse neurodevelopmental outcomes of preterm birth.
acKnoWledGMents
(in alphabetical order): Peter J. Anderson, PhD, Department of Pediatrics, University of Melbourne, and Murdoch Childrens Research Institute (Parkville, Victoria, Australia); Alice Burnett, PhD, Premature Infant Follow-up Program, Royal Women’s Hospital, and Murdoch Childrens Research Institute (Parkville, Victoria, Australia); Catherine Callanan, RN, Premature Infant Follow-up Program, Royal Women’s Hospital (Parkville, Victoria, Australia); Elizabeth Carse, FRACP, Monash Medical Centre (Melbourne, Victoria, Australia); Margaret P. Charlton, MEd, Psych, Monash Medical Centre (Melbourne, Victoria, Australia); Jeanie Cheong, MD, FRACP, Premature Infant Follow-up Program, Royal Women’s Hospital, Department of Obstetrics and Gynecology, University of Melbourne, and Murdoch Childrens Research Institute (Parkville, Victoria, Australia); Mary-Ann Davey, RN/RM, MEpi, DPH, Judith Lumley Centre, La Trobe University (Melbourne, Victoria, Australia); Noni Davis, FRACP, Premature Infant Follow-up Program, Royal Women’s Hospital (Parkville, Victoria, Australia); Cinzia R. De Luca, BSc, PhD, Premature Infant Follow-up Program, Royal Women’s Hospital (Parkville, Victoria,
Australia); Julianne Duff, FRACP, Premature Infant Follow-up Program, Royal Women’s Hospital (Parkville, Victoria, Australia); Marie Hayes, RN, Monash Medical Centre (Melbourne, Victoria, Australia); Esther Hutchinson, DPsych, Premature Infant Follow-up Program, Royal Women’s Hospital (Parkville, Victoria, Australia); Elaine Kelly, MA, Premature Infant Follow-up Program, Royal Women’s Hospital (Parkville, Victoria, Australia), and Mercy Hospital for Women (Melbourne, Victoria, Australia); Marion McDonald, RN, Premature Infant Follow-up Program, Royal Women’s Hospital (Parkville, Victoria, Australia); Carly Molloy, PhD, Murdoch Childrens Research Institute (Parkville, Victoria, Australia); Gillian Opie, FRACP, Mercy Hospital for Women (Melbourne, Victoria, Australia); Gehan Roberts, MPH, PhD, FRACP, Department of Pediatrics, University of Melbourne, Murdoch Childrens Research Institute, and Royal Children’s Hospital (Parkville, Victoria, Australia); Karissa Searle, BSc, Department of Psychiatry, University of Melbourne (Parkville, Victoria, Australia); Andrew Watkins, FRACP, Mercy Hospital for Women (Melbourne, Victoria, Australia); Amanda Williamson, Mercy Hospital for
Women (Melbourne, Victoria, Australia); Michelle Wilson-Ching, PhD, Premature Infant Follow-up Program, Royal Women’s Hospital (Parkville, Victoria, Australia); Stephen J. Wood, PhD, School of Psychology, University of Birmingham (Birmingham, United Kingdom); and Heather Woods, RN, Mercy Hospital for Women (Melbourne, Victoria, Australia). We gratefully acknowledge the contribution of the families who participated in this longitudinal study. This work is published on behalf of members of the Victorian Infant Collaborative Study Group, who were involved in data collection at the various study sites.
manuscript; and all authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work, including the accuracy and integrity of this study.
doi: https:// doi. org/ 10. 1542/ peds. 2017- 0257 Accepted for publication Jun 13, 2017
Address correspondence to Peter J. Anderson, PhD, School of Psychological Sciences, Monash University, 18 Innovation Walk, Clayton Campus, Clayton, VIC 3800, Australia. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2017 by the American Academy of Pediatrics
Financial disclosuRe: The authors have indicated they have no financial relationships relevant to this article to disclose.
FundinG: Funded in part by Centre of Clinical Research Excellence grant 546519, project grant 491246, and fellowship support (Dr Anderson: 1081288; Dr Cheong:
1053787) from the Australian National Health and Medical Research Council. Support was also provided by the Victorian Government’s Operational Infrastructure
Support Program. Ms Costa and Dr Miranda received financial support from the Brazilian foundations Coordenação de Aperfeiçoamento de Pessoal de Nivel
Superior and Conselho Nacional de Desenvolvimento Científico e Tecnológico, respectively. The funders had no role in study design, data collection and analysis,
decision to publish, or preparation of the manuscript.
Potential conFlict oF inteRest: The authors have indicated they have no potential conflicts of interest to disclose.
abbReviations
BRI: Behavioral Regulation Index BRIEF: Behavior Rating
Inventory of Executive Function
EF: executive function ELBW: extremely low birth
weight
EP: extremely preterm GEE: generalized estimating
equations
MCI: Metacognition Index
ReFeRences
1. Burnett AC, Scratch SE, Lee KJ, et al; Victorian Infant Collaborative Study Group. Executive function in adolescents born <1000 g or <28 weeks: a prospective cohort study.
Pediatrics. 2015;135(4). Available at:
www. pediatrics. org/ cgi/ content/ full/ 135/ 4/ e826
2. Hutchinson EA, De Luca CR, Doyle LW, Roberts G, Anderson PJ; Victorian Infant Collaborative Study Group. School-age outcomes of extremely preterm or extremely low birth weight children. Pediatrics. 2013;131(4). Available at: www. pediatrics. org/ cgi/ content/ full/ 131/ 4/ e1053
3. Johnson MH. Executive function and developmental disorders: the flip side of the coin. Trends Cogn Sci. 2012;16(9):454–457
4. Baron IS, Weiss BA, Litman FR, Ahronovich MD, Baker R. Latent mean differences in executive function in at-risk preterm children: the delay-deficit dilemma. Neuropsychology. 2014;28(4):541–551
5. Ritter BC, Nelle M, Perrig W, Steinlin M, Everts R. Executive functions of children born very preterm–deficit or delay? Eur J Pediatr. 2013;
172(4):473–483
6. Ment LR, Vohr B, Allan W, et al. Change in cognitive function over time in very low-birth-weight infants. JAMA. 2003;289(6):705–711
7. Tideman E. Longitudinal follow-up of children born preterm: cognitive development at age 19. Early Hum Dev. 2000;58(2):81–90
8. Doyle LW, Cheong JL, Burnett A, Roberts G, Lee KJ, Anderson PJ; Victorian Infant Collaborative Study Group. Biological and social influences on outcomes of extreme-preterm/low-birth weight adolescents. Pediatrics. 2015;136(6). Available at: www. pediatrics. org/ cgi/ content/ full/ 136/ 6/ e1513
9. Odd D, Evans D, Emond A. Preterm birth, age at school entry and long term educational achievement. PLoS One. 2016;11(5):e0155157
10. Hornman J, de Winter AF, Kerstjens JM, Bos AF, Reijneveld SA. Emotional and behavioral problems of preterm
and full-term children at school entry.
Pediatrics. 2016;137(5):e20152255
11. Pine DS, Fox NA. Childhood antecedents and risk for adult mental disorders.
Annu Rev Psychol. 2015;66:459–485
12. Taylor HG, Minich NM, Klein N, Hack M. Longitudinal outcomes of very low birth weight: neuropsychological findings. J Int Neuropsychol Soc. 2004;10(2):149–163
13. Diamond A. Executive functions. Annu
Rev Psychol. 2013;64:135–168
14. Johnson S, Marlow N. Growing up after extremely preterm birth: lifespan mental health outcomes. Semin Fetal
Neonatal Med. 2014;19(2):97–104
15. Romine CB, Reynolds CR. A model of the development of frontal lobe functioning: findings from a meta-analysis. Appl Neuropsychol. 2005;12(4):190–201
16. Anderson PJ, Doyle LW; Victorian Infant Collaborative Study Group. Executive functioning in school-aged children who were born very preterm or with extremely low birth weight in the 1990s. Pediatrics. 2004;114(1):50–57 17. Wilson-Ching M, Molloy CS, Anderson
VA, et al. Attention difficulties in a contemporary geographic cohort of adolescents born extremely preterm/extremely low birth weight. J Int Neuropsychol Soc. 2013;19(10):1097–1108
18. Farooqi A, Adamsson M, Serenius F, Hägglöf B. Executive functioning and learning skills of adolescent children born at fewer than 26 weeks of gestation. PLoS One. 2016;11(3):e0151819
19. Loe IM, Lee ES, Luna B, Feldman HM. Executive function skills are associated with reading and parent-rated child function in children born prematurely.
Early Hum Dev. 2012;88(2):111–118
20. Rose SA, Feldman JF, Jankowski JJ. Modeling a cascade of effects: the role of speed and executive functioning in preterm/full-term differences in academic achievement. Dev Sci. 2011;14(5):1161–1175
21. Gray RF, Indurkhya A, McCormick MC. Prevalence, stability, and predictors of clinically significant behavior
problems in low birth weight children at 3, 5, and 8 years of age. Pediatrics. 2004;114(3):736–743
22. Aylward GP. Cognitive function in preterm infants: no simple answers.
JAMA. 2003;289(6):752–753
23. Pluess M, Belsky J. Vantage sensitivity: individual differences in response to positive experiences. Psychol Bull. 2013;139(4):901–916
24. Anderson P, Doyle LW; Victorian Infant Collaborative Study Group. Neurobehavioral outcomes of school-age children born extremely low birth weight or very preterm in the 1990s.
JAMA. 2003;289(24):3264–3272 25. Doyle LW; Victorian Infant Collaborative
Study Group. Outcome at 5 years of age of children 23 to 27 weeks’ gestation: refining the prognosis. Pediatrics. 2001;108(1):134–141
26. The Victorian Infant Collaborative Study Group. Outcome at 2 years of children 23-27 weeks’ gestation born in Victoria in 1991-92. J Paediatr Child
Health. 1997;33(2):161–165
27. Gioia GA, Isquith PK, Guy SC, Kenworthy
L. Behavior Rating Inventory of
Executive Function: Professional
Manual. Lutz, FL: Psychological
Assessment Resources; 2000 28. Wilkinson GR, Robertson GJ. Wide
Range Achievement Test (WRAT4).
Lutz, FL: Psychological Assessment Resources, Inc; 2006
29. Roth RM, Erdodi LA, McCulloch LJ, Isquith PK. Much ado about norming: the behavior rating inventory of executive function. Child Neuropsychol. 2015;21(2):225–233
30. Wechsler D. Wechsler Abbreviated
Scale of Intelligence (WASI) Manual.
San Antonio, TX: Harcourt Assessment; 1999
31. Huberty CJ. A history of effect size indices. Educ Psychol Meas. 2002;62(2):227–240
32. Cohen J. Statistical Power Analysis
for the Behavioral Sciences. 2nd
ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 1998
33. IBM Corp. IBM SPSS Statistics for
Windows, Version 22.0. Armonk, NY:
34. Farooqi A, Hägglöf B, Serenius F. Behaviours related to executive functions and learning skills at 11 years of age after extremely preterm birth: a Swedish national prospective follow-up study. Acta Paediatr. 2013;102(6):625–634
35. Litt JS, Gerry Taylor H, Margevicius S, Schluchter M, Andreias L, Hack M. Academic achievement of adolescents born with extremely low birth weight.
Acta Paediatr. 2012;101(12):1240–1245
36. Luu TM, Ment L, Allan W, Schneider K, Vohr BR. Executive and memory function in adolescents born very preterm. Pediatrics. 2011;127(3). Available at: www. pediatrics. org/ cgi/ content/ full/ 127/ 3/ e639
37. McCann JP, Rider GN, Weiss BA, Litman FR, Baron IS. Latent mean comparisons on the BRIEF in preterm children: parent and teacher differences. Child
Neuropsychol. 2014;20(6):737–751
38. Ritter BC, Perrig W, Steinlin M, Everts R. Cognitive and behavioral aspects of executive functions in children born very preterm. Child Neuropsychol. 2014;20(2):129–144
39. Rutter M. Annual research review: resilience–clinical implications. J Child
Psychol Psychiatry. 2013;54(4):474–487
40. McAuley T, Chen S, Goos L, Schachar R, Crosbie J. Is the behavior rating inventory of executive function more strongly associated with measures of impairment or executive function? J Int
Neuropsychol Soc. 2010;16(3):495–505
41. Aarnoudse-Moens CS, Weisglas-Kuperus N, van Goudoever JB, Oosterlaan J. Meta-analysis of neurobehavioral outcomes in very preterm and/or very low
birth weight children. Pediatrics. 2009;124(2):717–728
42. Basten M, Jaekel J, Johnson S, Gilmore C, Wolke D. Preterm birth and adult wealth: mathematics skills count.
Psychol Sci. 2015;26(10):1608–1619
43. Geary DC. Cognitive predictors of achievement growth in mathematics: a 5-year longitudinal study. Dev Psychol. 2011;47(6):1539–1552
44. Farah MJ, Shera DM, Savage JH, et al. Childhood poverty: specific associations with neurocognitive development. Brain Res. 2006;1110(1):166–174
45. Noble KG, Houston SM, Brito NH, et al. Family income, parental education and brain structure in children and adolescents. Nat Neurosci. 2015;18(5):773–778
46. Sarsour K, Sheridan M, Jutte D, Nuru-Jeter A, Hinshaw S, Boyce WT. Family socioeconomic status and child executive functions: the roles of language, home environment, and single parenthood. J Int Neuropsychol Soc. 2011;17(1):120–132
47. Weisglas-Kuperus N, Baerts W, Smrkovsky M, Sauer PJ. Effects of biological and social factors on the cognitive development of very low birth weight children. Pediatrics. 1993;92(5):658–665
48. Wong HS, Edwards P. Nature or nurture: a systematic review of the effect of socio-economic status on the developmental and cognitive outcomes of children born preterm. Matern Child
Health J. 2013;17(9):1689–1700
49. Taylor HG, Clark CA. Executive function in children born preterm: risk factors
and implications for outcome. Semin
Perinatol. 2016;40(8):520–529
50. Johnson S. Cognitive and behavioural outcomes following very preterm birth. Semin Fetal Neonatal Med. 2007;12(5):363–373
51. Huizinga M, Smidts DP. Age-related changes in executive function: a normative study with the Dutch version of the Behavior Rating Inventory of Executive Function (BRIEF). Child
Neuropsychol. 2011;17(1):51–66
52. Fournet N, Roulin JL, Monnier C, et al. Multigroup confirmatory factor analysis and structural invariance with age of the Behavior Rating Inventory of Executive Function (BRIEF)–French version. Child Neuropsychol. 2015;21(3):379–398
53. Dekker MC, Ziermans TB, Spruijt AM, Swaab H. Cognitive, parent and teacher rating measures of executive functioning: shared and unique influences on school achievement.
Front Psychol. 2017;8:48
54. Toplak ME, West RF, Stanovich KE. Practitioner review: do performance-based measures and ratings of executive function assess the same construct? J Child Psychol Psychiatry. 2013;54(2):131–143
55. Gerst EH, Cirino PT, Fletcher JM, Yoshida H. [Formula: see text] Cognitive and behavioral rating measures of executive function as predictors of academic outcomes in children. Child Neuropsychol. 2017;23(4):381–407
56. Casey BJ. Beyond simple models of self-control to circuit-based accounts of adolescent behavior. Annu Rev
DOI: 10.1542/peds.2017-0257 originally published online August 30, 2017;
2017;140;
Pediatrics
Group
Cheong, Peter J. Anderson and on behalf of the Victorian Infant Collaborative Study
Danielle S. Costa, Débora M. Miranda, Alice C. Burnett, Lex W. Doyle, Jeanie L.Y.
Preterm
Executive Function and Academic Outcomes in Children Who Were Extremely
Services
Updated Information &
http://pediatrics.aappublications.org/content/140/3/e20170257 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/140/3/e20170257#BIBL This article cites 50 articles, 9 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neonatology_sub Neonatology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
rning_disorders_sub
http://www.aappublications.org/cgi/collection/cognition:language:lea Cognition/Language/Learning Disorders
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2017-0257 originally published online August 30, 2017;
2017;140;
Pediatrics
Group
Cheong, Peter J. Anderson and on behalf of the Victorian Infant Collaborative Study
Danielle S. Costa, Débora M. Miranda, Alice C. Burnett, Lex W. Doyle, Jeanie L.Y.
Preterm
Executive Function and Academic Outcomes in Children Who Were Extremely
http://pediatrics.aappublications.org/content/140/3/e20170257
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.