Persistent Infant Crying and Hyperactivity Problems
in Middle Childhood
Dieter Wolke, PhD; Patrizia Rizzo, BSc; and Sarah Woods, MSc
ABSTRACT. Objective. To investigate whether per-sistent infant crying is associated with an increased risk for externalizing behavior problems in childhood.
Methods. Sixty-four infants who were referred for persistent crying in infancy (PC; mean age: 3.8 ⴞ 1.3 months) were reassessed at 8 to 10 years of age and compared with 64 classroom controls (CC). The major outcome measure was pervasive hyperactivity or conduct problems defined as parent, child, and teacher ratings that across informants were within the borderline/clini-cal range according to the Strengths and Difficulties Questionnaire (SDQ). Ratings of other behavior prob-lems, parent ratings of temperament, and teacher assess-ment of academic achieveassess-ment were also obtained.
Results. Ten (18.9%) of 53 PC had pervasive hyperac-tivity problems (child, parent, and teacher reported) com-pared with 1 (18.9%) of 62 CC (odds ratio: 14.19 [1.75– 114.96]). Parents (29 [45.3%] of 64 vs 11 [17.2%] of 64; 4.00 [1.77–9.01]) and children (30 [46.9%] of 64 vs 17 [26.6%] of 64; 2.44 [1.16 –5.12]) but not the teachers reported more conduct problems. Parents of PC rated the temperament of their children to be more negative in emotionality (PC mean: 3.0ⴞ1.0; CC: 2.4ⴞ1.0; effect size: 0.6) and diffi-cult-demanding (PC mean: 5.2ⴞ1.3; CC: 6.3ⴞ0.9; effect size: 1.0). Academic achievement was reported by teach-ers to be significantly lower for PC than CC, in particular for those children with pervasive hyperactivity prob-lems.
Conclusions. Infants who are referred for PC prob-lems and associated sleeping or feeding probprob-lems are at increased risk for hyperactivity problems and academic difficulties in childhood.Pediatrics 2002;109:1054 –1060;
persistent crying, colic, hyperactivity, conduct disorder, academic achievement, temperament.
ABBREVIATIONS. PC, persistent crying; CC, classroom control subjects; D, dropout; NS, not significant;df, degrees of freedom; CA, Cronbach’s␣; SDQ, Strengths and Difficulties Questionnaire; TAAS, Total Academic Achievement Score; ES, effect size.
P
ersistent crying (PC), sometimes called colic and defined as fussing or crying for⬎3 hours per day on 3 days per week in the past 3 weeks,1,2 is found in approximately 10% to 15% ofinfants in the first 3 months of life.3,4 Unexplained
infant crying is among the most common complaints
for which parents seek professional advice in the first year of life.3,5There is some evidence that parental
perceptions of negative infant behavior persist be-yond the colic period.5–7 However, negative
conse-quences of colic on observed infant behavior or cog-nitive development, mother-infant interaction, or maternal coping with the child have been suggested, but few have been found.5,6 Colic in the first 3
months of life seems to be a transitory condition that is associated with temporary delays in certain devel-opmental tasks but no apparent long-term conse-quences.6,8 –12 Possible reasons are that previous
study samples were too small to detect such effects,8 – 11,13,14the follow-up period extended to only the first
months or year of life,15,16 or relied on maternal
perceptions of infant mood or temperament in infan-cy5,7,12,17,18rather than on reliable diary reports of PC
spanning several days.19,20
Others have speculated that not unexplained crying per se but persistent problems with behav-ioral control, such as the inability to stop crying and to regulate sleeping or feeding behavior in infancy, are precursors of behavior control diffi-culties such as hyperactivity or conduct problems in childhood.18,21–23 This study prospectively
in-vestigated a group of infants who persistently cried in the first 6 months of life and compared them for pervasive hyperactivity and conduct problems and other behavioral and academic dif-ficulties with classrooms control subjects (CC) at the age of 8 to 10 years.
METHODS
A total of 108 mothers of 2- to 6-month-old infants (mean age: 3.8⫾1.3 [standard deviation]) who either contacted the self-help group CRY-SIS (n⫽53) or came forward to a call in the national press (n⫽55) participated in a treatment trial of PC in infancy.24
More than 80% of the mothers had been in contact, often several times, with their primary health care providers regarding pro-longed crying before contacting CRY-SIS or the research team directly.24No organic problems on routine physical examination
were found to explain PC at baseline. The 108 mothers completed a standard and previously proven reliable 7-day 24-hour dia-ry19,20,25that required continuous and mutually exclusive
record-ings of 5 infant behaviors (sleeping, feeding, fussing, crying, and awake). A total of 101 of 108 infants fussed or cried⬎3 hours on 3 days in the week (modified Wessel criteria2) and 64 (63%) were
successfully traced and agreed to participate at 8 to 10 years of age (33 who had contacted CRY-SIS, 31 who had responded to the call in the national press). The 37 dropouts (D) were compared with the 64 participants (PC) according to mean fuss/cry duration in infancy (ttest for independent samples; baseline [mean⫾ stan-dard deviation] D: 381⫾177 minutes; PC: 391⫾170 minutes;t
(99)⫽ ⫺0.26;P⫽.798, not significant [NS]), cry bouts in 24 hours (D: 9.9 ⫾4.8; PC: 9.9⫾4.6;t(99)⫽ ⫺0.08;P ⫽.940, NS) and whether they had contacted a doctor/health visitor for PC
prob-From the University of Hertfordshire, Department of Psychology, Wolke Research Group, Hatfield Campus, Hatfield/Herts, United Kingdom. Received for publication Nov 28, 2001; accepted Dec 3, 2001.
lems (D: 81%; PC: 82.8%;2(degrees of freedom [df]: 1)⫽0.83;P⫽
.514, NS). Furthermore, D and PC were compared on 18 sociode-mographic factors (birth weight, marital status, family income, housing, employment, etc), 12 feeding variables, 3 sleeping vari-ables, 12 health problem items, total health problems, and infant weight at baseline.25No differences were found for all but the
following variables: dropouts had mothers who were in paid employment more often (9 [24.3%] of 37 vs 2 [3.1%] of 64;2(df:
1)⫽10.86;P⬍.001), and the infants were more often in regular day care (6 [16.2%] of 37 vs 3 [4.7%] of 64;2(df:1)⫽3.84;P⬍.05)
at baseline.
Of the 64 infants who were referred for PC, 5 (7.8%) of 64 had only a PC problem; 10 (15.7%) of 64 also had sleeping problems; 20 (31.2%) of 64 had additional feeding problems; and 29 (45.3%) of 64 had crying, sleeping, and feeding problems.
Twenty-four of the participating children (24 [37.5%] of 64) were referred before 12 weeks of age; 8 of 24 did not qualify anymore as persistent criers according to modified Wessel criteria at the follow-up 3 months later (baseline age: 73 ⫾ 10 days; baseline fuss/cry: 4 hours 41 minutes⫾1 hour 7 minutes; follow-up: 2 hours 9 minutes ⫾1 hour 14 minutes), whereas 16 of 24 remained persistent criers 3 months later (baseline age: 66⫾13 days; baseline: 6 hours 21 minutes⫾1 hour 37 minutes; follow-up: 4 hours 33 minutes⫾1 hour 18 minutes). Forty (62.5%) of 64 were referrals after the age of 12 weeks (baseline age: 136⫾27 days; baseline: 5 hours 26 minutes⫾1 hour 26 minutes; follow-up: 3 hours 13 minutes⫾1 hour 48 minutes). Of the 40 infants who were referred after 12 weeks, 19 were still persistent criers in the follow-up 3 months later (ie,⬎6 months of age). Thus, all but 8 infants were persistent criers after the age of 3 months.
Of the 64 PC, 31 had been assigned to a no-treatment control condition (received normal primary care) in infancy and 33 had received telephone contact with a parent volunteer from the self-help group CRY-SIS who herself had previously had an infant who persistently cried.24Fifteen of 33 shared their feelings and
coping strategies with the mother (empathy condition), and 18 of 33 were provided with behavioral management advice. The fol-low-up findings of the original trial indicated that infants reduced crying significantly more in the behavioral management than in the empathy or control condition.24However, fuss/cry amounts at
3 months’ follow-up were still substantially higher than expected in infants at this age in all 3 subgroups.24
The parents who had consented to participation in the fol-low-up study were asked to consent for the investigators to ap-proach their children’s teacher when the children were 8 to 10 years of age (9.7⫾0.6 years). The teachers were asked to select 2 children of the same gender in the class closest in age to the target child. Inclusion criteria for CC were same gender and that they had, according to retrospective parental reports, not cried ⬎3 hours per day on 3 days per week during any week in the first 6 months of life. Four CC were excluded because of PC in infancy. When both control parents agreed to participation and were suit-able, 1 was randomly selected to obtain a same size control sample (n⫽64). Parents and children were sent a set of standard ques-tionnaires for completion (the child questionnaire was in a sepa-rate envelope). When applicable, the reliability coefficients for scales (Cronbach’s␣[CA]26) as determined for the total sample
(N ⫽ 128) and the 64 PC and 64 CC separately are shown in brackets. The parent questionnaire included detailed questions about sociodemographic characteristics and current health,25
in-cluding 6 items on eating behavior (eg, eating too little, too much) and 7 items on current sleeping difficulties (eg, problems with falling asleep). Two questionnaires of child temperament, the Emotionality, Activity, Sociability Temperament Survey27 with
the subscales shyness (total sample CA: 0.73; PC: 0.73; CC: 0.65), emotionality (0.87; 0.87; 0.84), activity (0.78; 0.80; 0.76), and socia-bility (0.58; 0.60; 0.57) and the Childhood Temperament Impres-sion Scale (adapted from Wolke et al24) were also included.
Prin-cipal components analysis with varimax rotation28 of the 13
Childhood Temperament Impression Scale items rated on 9-cm visual analog scales (eg, mood: very bad tempered/irritable to very happy/cheerful) yielded 2 factors: Difficult-Demanding (items: mood, demanding, difficult, unhappy about child’s tem-perament, stressful; total sample CA: 0.92; PC: 0.92; CC: 0.89) and Adaptability (wariness, adaptability 0.64; 0.62; 0.69). The parents were also asked to complete the Strengths and Difficulties Ques-tionnaire (SDQ29), which consists of 5 subscales: Hyperactivity
(CA: 0.79; PC: 0.81; CC: 0.69), Conduct problems (0.67; 0.53; 0.71),
Emotional problems (0.81; 0.83; 0.81), Peer problems (0.73; 0.74; 071), and Prosocial behavior (0.76; 0.72; 0.78). A total score based on the first 4 subscales and scale scores for each subscale sepa-rately were computed. The SDQ has been shown to be a reliable and valid screening for identifying children who meetDiagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria and require psychiatric treatment.30,31 A child32 and teacher29
version of the SDQ was also completed by the child and teacher, respectively. The internal consistency coefficients were compara-ble to those reported for the parents. Furthermore, the total score and each subscale score were dichotomized into normal versus borderline/clinical (score ⬎80th percentile according to Good-man29,33[replicated by Wolke et al33for⬍11-year-olds]). Teachers
were also asked to rate the scholastic performance of the child compared with expected standards in the 11 national curriculum subjects English, math, science, technology, geography, history, information technology, art, music, physical education, and reli-gion on 5-point rating scales (1, very below average; 3, average; 5, very above average). Principal components analysis with varimax rotation indicated that the first 7 subjects (English, math, science, technology, geography, history, and information technology) loaded on 1 factor and were combined to give a Total Academic Achievement Score (TAAS; CA: 0.92; PC: 0.91; CC: 0.92). Further-more, mothers completed the Edinburgh Postnatal Depression Scale34when their children were 8 to 10 years of age.
Fully completed child and parent questionnaires were available for all PC and CC (N⫽128); however, teacher reports for 11 PC and 2 CC were not obtained as parents did not provide consent for completion of teacher ratings. Ethical permission for the study was provided by the University of Hertfordshire Ethical Commit-tee in accordance with the guidelines of the Helsinki Declaration, revised 1983.
Statistics
Comparisons between PC and CC were conducted using inde-pendent sample t test for interval-scaled dependent variables. Effect size (ES) for mean comparisons was computed as Cohen’s d35(ie, expressed as standard deviation unit differences using
g-power software).36Comparisons on categorical dependent
vari-ables were cross-tabulated, and crude odds ratio with 95% confi-dence interval were determined by logistic regression within SPSS version 10.Ttests, odds ratios, and 95% confidence intervals with
2statistics are presented with corresponding 2-sidedP values
(P⬍.05,⬍.01, or⬍.001). Post hoc analyses of mean differences in hyperactivity and conduct scale scores between treatment groups (behavior management, empathy, no-treatment control subjects) were conducted using 1 factorial analysis of variance.
RESULTS
PC and CC were comparable on a wide range of sociodemographic indices (nonsignificant differ-ences, Table 1). Furthermore, mothers did not differ in regard to depression scores (Edinburgh Postnatal Depression Scale mean 8.0 ⫾ 4.6 vs 7.4⫾ 5.3;t (df:
126) ⫽ 0.65;P ⫽ .52, NS). Twelve of 64 (18.8%) PC and 11 of 64 (17.2%) CC mothers scored within the clinical range (score ⬎12)34 (odds ratio: 1.11 [0.45–
2.74];2(df: 1)⫽ 0.05;P⫽.50, NS).
0.78, P ⬍ .001; child-teacher: r ⫽ 0.45, P ⬍ .001; parent-teacher: r⫽ 0.54, P⬍ .001). PC significantly more often had Hyperactivity scores in the border-line/clinical range than CC as reported by the chil-dren (26 [40.6%] of 64 vs 10 [15.6%] of 64; 3.69 [1.60 – 8.55]; 2 (df: 1) ⫽ 9.89; P ⬍ .01), the parents (25
[39.1%] of 64 vs 8 [12.5%] of 64; 4.49 [1.83–10.98];2
(df:1)⫽11.80;P⬍.001), and the teachers (13 [24.5%] of 53 vs 5 [8.1%] of 62; 3.71 [1.22–11.22];2(df:1) ⫽
5.87; P ⬍ .05; Fig 1). Ten of 53 PC (18.9%) had pervasive hyperactivity problems in the borderline/ clinical range (child, parent, and teacher reported) compared with 1 of 62 of the CC (1.6%; odds ratio: 14.19 [1.75–114.96];2(df:1) ⫽9.84;P⬍ .01). When
the stricter criterion of pervasive hyperactivity scores
⬎90th percentile was applied, it just failed to be significantly different between groups (5 [9.4%] of 53 vs 1 [1.6%] of 62; 7.8 [0.90 – 66.9];2(df:1)⫽3.54;P⬍
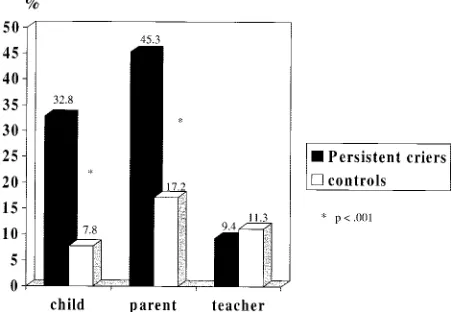
.07). Parents (29 [45.3%] of 64 vs 11 [17.2%] of 64; 4.00
[1.77–9.01];2(df:1) ⫽11.78;P⬍.001) and children
(21 [32.8%] of 64 vs 5 [7.8%] of 64; 2.44 [1.16 –5.12];2
(df:1)⫽12.36;P⬍.001) also reported more conduct problems in the borderline/clinical range (Fig 2).
Pearson’s correlations were computed between the minutes of fuss/cry at baseline (severity of fuss/cry problem) and hyperactivity and conduct scores in the SDQ within the PC group. None of the correla-tions was statistically significant (Hyperactivity: child SDQ r ⫽ 0.23, parent SDQ r ⫽ 0.24, teacher SDQ r⫽ 0.11; Conduct: child SDQr ⫽ 0.06, parent SDQr⫽ 0.09, teacher SDQr⫽ ⫺0.10).
No differences in Hyperactivity or Conduct scores were found according to treatment in infancy (Hy-peractivity: Behavioral management [M⫽4.7⫾3.2], Empathy [M⫽4.7⫾ 3.8], no-treatment control sub-jects [M ⫽ 4.7 ⫾ 2.7], F2,61 ⫽ 0.10; P ⫽ .91, NS;
Conduct problems: Behavioral management [M ⫽
TABLE 1. Sociodemographic Characteristics of PC and CC
Sociodemographic Characteristics PC (n⫽64;n[%]) CC (n⫽64;n[%])
Gender
Girls 32 (50%) 32 (50%)
Child’s age in y (M, SD) 9.7 (0.6) 9.5 (0.7)
Osborn Index (M, SD) 58.7 (6.5) 59.01 (7.2)
Mother’s age in years (M, SD) 36.9 (4.8) 37.8 (3.8)
Marital status
Married/cohabiting 52 (81.3%) 57 (93.4%)
Separated/divorced 9 (14.1%) 4 (6.6%)
No regular partner 3 (4.6%) 0 (0%)
Partner’s age (M, SD) 38.3 (5.7) 39.7 (5.7)
Number of children living in household
1 8 (12.5%) 8 (12.7%)
2 34 (53.1%) 30 (47.6%)
3 or more 22 (34.4%) 25 (39.7%)
Mother currently employed 41 (66.1%) 47 (74.6%)
Mother’s working h per wk
0–20 h 19 (47.5%) 24 (54.5%)
21–30 h 10 (25.0%) 8 (18.2%)
31–40 h 8 (20.0%) 11 (25.0%)
41⫹h 3 (7.5%) 1 (2.3%)
Age of child when went back to work (mo; M, SD) 8.4 (17.6) 8.0 (19.8)
Partner currently employed 52 (100%) 57 (98.3%)
Partner’s working h per wk*
0–20 h 0 (0%) 2 (3.4%)
21–30 h 2 (3.5%) 3 (5.1%)
31–40 h 25 (43.9%) 25 (42.4%)
41⫹h 30 (52.6%) 29 (49.1%)
Rent/own accommodation
Own 53 (82.8%) 57 (90.5%)
Council rented 7 (10.9%) 3 (4.8%)
Private rented 2 (3.2%) 0 (0%)
Mother’s educational qualification†
Left school with none 8 (12.7%) 7 (11.1%)
Vocational or O level 23 (36.5%) 24 (38.1%)
A level 16 (25.4%) 15 (23.8%)
Teacher certificate or degree 16 (25.4%) 17 (27.0%)
Partner’s educational qualification†
Left school with none 6 (9.5%) 7 (11.3%)
Vocational or O level 13 (20.6%) 7 (11.3%)
A level 17 (27.0%) 20 (32.3%)
Teacher certificate or degree 17 (27.0%) 26 (41.9%)
Gross family income (£ per annum)
⬍12 000 6 (9.5%) 7 (11.3%)
12 000–20 000 13 (20.6%) 7 (11.3%)
21 000–32 000 17 (27.0%) 20 (32.3%)
32 000 or more 17 (27.0%) 26 (41.9%)
SD indicates standard deviation.
* Mother reports include 4 recently separated partners.
2.2 ⫾ 1.7], Empathy [M⫽ 2.5 ⫾ 2.5], no-treatment controls [M ⫽2.4⫾1.7], F2,61⫽0.11;P ⫽.89, NS).
In the secondary outcome measure TAAS (N ⫽
112), 2 CC had a geography rating missing (CCn⫽
60) and 1 PC had a technology rating missing (PC
n ⫽ 52); the PC scored lower, on average, than CC (PC grand mean: 3.1⫾.8; CC grand mean: 3.4⫾.6;t
(110)⫽ ⫺2.41;P⬍.05; ES: 0.4). Comparisons on the individual items of the TAAS showed that persistent criers in infancy scored lower in science (PC mean: 3.2⫾ 0.9; CC mean: 3.6⫾0.7;t(113) ⫽ ⫺2.63;P ⬍
.01; ES: 0.5), English (PC mean: 3.1 ⫾1.1; CC mean: 3.5⫾.8;t(113)⫽ ⫺2.08;P⬍.05; ES: 0.4), geography (PC mean: 3.1 ⫾ .8; CC mean: 3.4 ⫾ 0.7; t (111) ⫽
⫺2.27;P⬍.05; ES: 0.4), and history (PC mean: 3.1⫾ 0.8; CC mean: 3.4⫾0.6;t(113)⫽ ⫺2.04;P⬍.05; ES: 0.4).
Higher SDQ Hyperactivity and Total Deviance scores of child, parent, and teacher ratings were con-sistently correlated with lower TAAS scores (Table 3). Furthermore, child and parent ratings of emo-tional problems, child ratings of peer problems, and teacher ratings of conduct problems were signifi-cantly correlated with lower academic achievement (Table 3). The PC with pervasive hyperactivity (10 of 52; 1 TAAS score missing) had much lower academic achievement scores (TAAS means: 2.5⫾0.8) than the
CC (n⫽60; 3.4⫾0.6;t(68)⫽4.58;P⬍.001: ES: 1.1) or PC without pervasive hyperactivity (n⫽42; 3.3⫾ 0.7;t(50)⫽3.16;P⬍ .01; ES: 1.1).
Significant differences were found in parent rat-ings of child temperament with case children rated as more negative in emotionality (Emotionality, Ac-tivity, Sociability Temperament Survey, PC mean: 3.0⫾1.0; CC mean: 2.4⫾1.0;t(126)⫽3.61;P⬍.001; ES: 0.6), more difficult-demanding (Temperament Impression Scale, PC mean: 5.2 ⫾ 1.3; CC mean: 6.3⫾1.0;t(126)⫽ ⫺5.49;P⬍.001; ES: 1.0), and less adaptable (Temperament Impression Scale: PC mean: 6.1⫾2.0, CC mean: 6.8⫾1.7;t(126)⫽ ⫺2.01;
P ⬍ .05; ES: 0.4). PC had more unregulated eating indicated by eating either too much or too little (PC: 15 [23.4%] of 64; CC: 5 [7.8%] of 64; 3.61 [1.23–10.64]; 2(df:1)⫽5.93;P⬍.05) or eating wrong foods more
frequently (PC: 15 [23.4%] of 64; CC: 6 [9.4%] of 64; 3.0 [1.07– 8.20];2(df: 1)⫽ 4.61;P⬍.05).
DISCUSSION
This study followed up infants who were identi-fied as being persistent criers in the first 6 months of life until school age. Persistent criers in infancy had more externalizing problems in childhood indicated by higher hyperactivity and conduct problems, neg-ative emotionality, being more difficult and
demand-Fig 1. Percentages for children who scored in the borderline/ clinical range for the hyperactivity SDQ subscale.
Fig 2. Percentages for children who scored in the borderline/ clinical range for the conduct problems SDQ subscale.
TABLE 2. Significant Mean Score Differences on the Scales of the SDQ Between PC and CC Rated by Child, Parent, or Teacher
Rater PC CC tValue Effect Size (d)
Mean SD Mean SD
Child
Hyperactivity* 5.0 2.4 3.5 2.0 3.8 0.7
Conduct problems* 2.8 1.9 1.4 1.4 4.6 0.9
Total deviance* 13.0 6.1 9.3 6.0 3.5 0.6
Parent
Hyperactivity* 4.6 3.1 2.9 2.1 3.7 0.7
Emotional symptoms† 3.0 2.7 1.8 2.2 2.6 0.5
Conduct problems* 2.4 1.9 1.1 1.5 4.4 0.8
Peer problems‡ 2.1 2.2 1.3 1.6 2.3 0.4
Total deviance* 11.7 7.0 7.1 5.6 4.0 0.7
Teacher
Hyperactivity* 3.6 2.9 1.9 2.3 3.6 0.7
Total deviance‡ 8.2 5.7 5.9 5.6 2.2 0.4
SD indicates standard deviation.
ing, and being less adaptable than CC. Most notable is that children with previous PC in infancy substan-tially more often had Hyperactivity scores in the borderline/clinical range than their peers as consis-tently reported by teachers, parents, and children themselves. Behavioral difficulties, in particular per-vasive hyperactivity problems, were related to lower academic achievement. The differences between PC and CC in middle childhood are unlikely to be ex-plained by differences in PC versus CC mothers or systematic bias in ratings. Dropouts did not differ from participants in any baseline measures apart from that mothers who returned to work earlier were less likely to participate when children were 8 to 10 years of age. The PC families at follow-up did not differ on a wide range of sociodemographic indices from CC and the mothers were not more often de-pressed, and multiple informants were required to define pervasive hyperactivity with a valid screening instrument.29 –31CC were selected on age and gender
only, and those with prolonged crying in infancy (6.5% of CC) on parent retrospective report were excluded. We found that for the prospectively stud-ied PC, the baseline reports on fussing/crying corre-lated r ⫽ 0.39 with the retrospective report 9 years later. The fuss/crying amounts were slightly overes-timated retrospectively. Thus, most prolonged in-fancy criers in the control group should have been excluded, if not, the reported findings are conserva-tive estimates of differences in hyperactivity.
Significant associations of difficult temperament in the second or third year of life with externalizing and hyperactivity problems have been reported previ-ously.23,37,38 These findings suggest that pervasive
problems of behavior regulation (hyperactivity) and poorer academic achievement are related to prob-lems of controlling behavioral states (eg, crying) de-tectable already in the first 6 months of life. This is in contrast to previous reports that found only small effects of prolonged crying in early infancy on be-havior in the toddler and preschool years.5,8,10,18,39
The differences in findings may be accounted for by differences in the populations studied. First, the in-fants with prolonged unexplained crying in previous studies were identified when they were well below 3 months of age at a time when cry amounts generally show an increase and mostly reduce spontaneously by 3 months (ie, colic crying40). In this study, all but
8 of the children were still fussing and crying ⬎3 hours a day after 3 months of age when the expected average fuss/cry amount is ⬍1 hour 15 minutes a day in UK infants of comparable age.3A comparison
of the 8 infants who ceased PC after 3 months to the rest with infants in the PC group was not meaningful
because of a lack of statistical power. Second, none of the previous longitudinal studies reported on co-associations of PC with sleeping or feeding prob-lems. This self-referred sample showed a high co-association with sleeping and feeding problems that has also been reported for other self-referred sam-ples.41,42Only 5 infants had just a PC problem, and
statistical comparison of these 5 with the 59 infants with multiple behavior problems lacked power. The prevalence of infants with multiple behavior difficul-ties in infancy is unknown. According to a commu-nity study of 5-month-olds, it may be approximately 2% in the infant population.18Third, although
behav-ioral management did lead to more reduction in fussing/crying in infancy compared with no or em-pathy intervention, all infants in this study still cried more than normative infants of 4 to 7 months of age.24 There were no differences on behavioral
out-come in childhood according to treatment in infancy. The sample thus consisted of infants with highly persistent crying and mostly multiple behavior prob-lems in infancy. The reduced variation in extreme groups may explain that the amount of fussing/ crying at baseline did not correlate significantly with Hyperactivity or Conduct scores at 10 years.
The pattern of previous findings and results here leads us to speculate that although colic that resolves by 3 months (ie, is transient) has no or few long-term adverse effects,6,8 –11,13,14 those infants with PC and
multiple behavior difficulties are at increased risk for externalizing and hyperactivity problems. This is consistent with findings from another recent study of infants who were referred in the first 6 months and had a history of several months of unexplained cry-ing.42 According to parent reports at 30 months,
be-havior problems were much more frequent in these infants than expected according to the scales norms. However, in the previous study, maternal bias in reporting on behavior could not be excluded. In con-trast, our follow-up extends into middle childhood and used several informants, including teachers. Un-fortunately, subgroup analysis in our study to test whether single versus multiple infant problems or the persistence of crying problems beyond 3 months of age are more strongly associated with hyperactiv-ity was not possible because of sample size restric-tions. Furthermore, although this study used multi-ple informants to define pervasive hyperactivity problems with a valid screening instrument,29 –31
more detailed clinical and neurobehavioral assess-ment would have been desirable for a firm diagnosis of attention-deficit/hyperactivity disorder according to theDiagnostic and Statistical Manual of Mental Dis-orders, Fourth Edition or hyperkinetic syndrome
ac-TABLE 3. Pearson’s Correlations Between SDQ Behavior Ratings (Child, Parent, Teacher) and Academic Achievement Score (TAAS)
SDQ Subscales
Hyperactive Emotional Conduct Peer Problems Total Deviance
Child rating and academic score ⫺0.39* ⫺0.31* NS ⫺0.24† ⫺0.37*
Parent rating and academic score ⫺0.44* ⫺0.30† NS NS ⫺0.36*
Teacher rating and academic rating ⫺0.50* NS ⫺0.19‡ NS ⫺0.35*
cording to the International Classification of Diseases, 10th Revision.
Alternative pathways may explain the association between infant difficulties in behavior regulation and childhood hyperactivity and warrant future ex-ploration. The heritability of hyperactivity is moder-ate to high43,44and has recently been linked to
spe-cific genes.45 We may speculate that the individual
characteristics of state regulation are stable over time as a result of genetic liability44 or, alternatively,
be-cause of underlying neurodevelopmental problems that were not detected in routine examination.46,47
For example, a higher rate of PC as well as more hyperactivity-attention problems have been reported in neurologic at-risk groups such as very low birth weight children.48,49 The neurobiological
underpin-nings for poorer state regulation may be sought in the biological targets of stimulants, the dopaminergic and noradrenergic system. Alternatively, the early problems with PC and state regulation are challeng-ing to parents. They form negative views5,6,16 that
maintain parenting difficulties and the problems that these infants have in state and behavior regulation.50
Thus, the behavior outcome may be a result of a self-fulfilling prophecy related to the earlier labeling. Whatever the reasons, health professionals should be aware that those with PC problems that last more than several months in infancy and often associated feeding or sleeping difficulties seem to be at in-creased risk for hyperactivity problems in childhood. Identification of infants and families that are slow to recover from colic and the development of appropri-ate interventions for these families remain important clinical challenges.22,41,51
ACKNOWLEDGMENTS
We give special thanks to Cerian Hughes, who contributed to the data collection, and to all of the children, parents, and teachers for participation.
REFERENCES
1. Wessel MA, Cobb JC, Jackson EB, Harris GS, Detwiler AC. Paroxysmal fussing in infancy, sometimes called “colic.”Pediatrics. 1954;14:421– 435 2. Barr RG, Rotman A, Yaremko J, Leduc D, Francoeur TE. The crying of infants with colic: a controlled empirical description.Pediatrics. 1992;90: 14 –21
3. St James-Roberts I, Halil T. Infant crying patterns in the first year: normal community and clinical findings.J Child Psychol Psychiatry. 1991;32:951–968
4. Wolke D. Probleme bei Neugeborenen und Kleinkindern. In: Margraf J, ed.Lehrbuch der Verhaltenstherapie. 2. vollstaendig ueberarbeitete und erwei-terte Auflage ed.Berlin, Germany: Springer; 2000:463– 480
5. Forsyth BWC, Canny PF. Perceptions of vulnerability three and a half years after problems of feeding and crying behavior in early infancy.
Pediatrics. 1991;88:757–763
6. Lehtonen L. From colic to toddlerhood. In: Barr RG, St James-Roberts I, Keefe M, eds.New Evidence on Unexplained Early Crying: Its Origin, Nature and Management. Skillman, NJ: Johnson & Johnson Pediatric Institute; 2001:259 –271
7. Herrle J, Laucht M, Esser G, Dinter-Joerg M, Schmidt MH. Dyspho-rische Saeuglinge: Fruehe Mutter-Kind-Interaktion und Entwicklung bis zum Vorschulalter.Kindheit Entwicklung. 1999;8:15–22
8. Stifter CA, Braungart J. Infant colic: a transient condition with no apparent effects.J Appl Dev Psychol. 1992;13:447– 462
9. Elliott MR, Pedersen EL, Mogan J. Early infant crying: child and family follow-up at three years.Can J Nurs Res. 1997;29:47– 67
10. Lehtonen L, Korhonen T, Korvenranta H. Temperament and sleeping patterns in colicky infants during the first year of life.Dev Behav Pediatr. 1994;15:196 –206
11. Sloman J, Bellinger DC, Krentzel CP. Infantile colic and transient de-velopmental lag in the first year of life.Child Psychiatry Hum Dev. 1990;21:25–36
12. Rautava P, Lehtonen L, Helenius H, Sillanpaa M. Infantile colic: child and family three years later.Pediatrics. 1995;96:43– 47
13. Shaver BA.Maternal Personality and Early Adaptation as Related to Infantile Colic. Psychological Aspects of a First Pregnancy and Early Postnatal Adap-tation.New York, NY: Raven Press; 1974:209 –215
14. Keefe MR, Kotzer AM, Froese-Fretz A, Curtin M. A longitudinal com-parison of irritable and nonirritable infants.Nurs Res. 1996;45:4 –9 15. St James-Roberts I, Conroy S, Wilsher K. Links between maternal care
and persistent infant crying in the early months.Child Care Health Dev. 1998;24:353–376
16. Lehtonen L, Gormally S, Barr RG. Clinical pies, etiology and outcome in infants presenting with early increased crying. In: Barr RG, Hopkins B, Green J, eds.Crying as a Signal, a Sign, and a Symptom: Developmental and Clinical Aspects of Early Crying Behavior. London, United Kingdom: Mac Keith Press; 2000:67–95
17. Oberklaid F, Sanson A, Pedlow R, Prior M. Predicting school behavior problems from temperament and other variables in infancy.Pediatrics. 1993;91:113–120
18. Wolke D, Meyer R, Ohrt B, Riegel K. Co-morbidity of crying and feeding problems with sleeping problems in infancy: concurrent and predictive associations.Early Dev Parenting. 1995;4:191–207
19. Barr RG, Kramer MS, Boisjoly C, McVey-White L, Pless IB. Parental diary of infant cry and fuss behavior.Arch Dis Child. 1988;63:380 –387 20. St James-Roberts I, Hurry J, Bowyer J. Objective confirmation of crying
durations in infants referred for excessive crying.Arch Dis Child. 1993; 68:82– 84
21. DeGangi GA, DiPietro JA, Greenspan SI, Porges S. Psychophysiological characteristics of the regulatory disordered infant.Infant Behav Dev. 1991;14:37–50
22. Wolke D. Interventionen bei Regulationsstoerungen. In: Oerter R, von Hagen C, Ro¨per G, eds.Klinische Entwicklungspsychologie. Weinheim, Germany: Beltz PVU; 1999:351–380
23. Moffitt TE, Caspi A, Dickson N, Silva P, Stanton W. Childhood-onset versus adolescent-onset antisocial conduct problems in males: natural history from age 3 to 18 years.Dev Psychopathol. 1996;8:399 – 424 24. Wolke D, Gray P, Meyer R. Excessive infant crying: a controlled study
of mothers helping mothers.Pediatrics. 1994;94:322–332
25. Wolke D, Meyer R, Gray P. Validity of the crying pattern questionnaire in a sample of excessively crying babies.J Reprod Infant Psychol. 1994; 12:105–114
26. Cronbach LJ.Essentials of Psychological Testing. 2nd ed. New York, NY: Harper & Row; 1960
27. Buss AH, Plomin R.Temperament: Early Developing Personality Traits.
Hillsdale, NJ: Lawrence Erlbaum Associates; 1984
28. Tabachnik BG, Fidell LS.Using Multivariate Statistics.2nd ed. New York, NY: Harper & Row; 1989
29. Goodman R. The strengths and difficulties questionnaire: a research note.J Child Psychol Psychiatry. 1997;38:581–586
30. Goodman R, Scott S. Comparing the strengths and difficulties question-naire and the child behaviour checklist: is small beautiful?J Abnorm Child Psychol. 1999;27:17–24
31. Klasen H, Woerner W, Wolke D, et al. Comparing the German versions of the Strengths and Difficulties (SDQ-Deu) and the Child Behavior Checklist.Eur J Child Adolesc Psychiatry.2000;9:271–276
32. Goodman R, Meltzer H, Bailey V. The strengths and difficulties questionnaire: a pilot study on the validity of the self-report version.
Eur J Child Adolesc Psychiatry. 1998;7:125–130
33. Wolke D, Woods S, Bloomfield L, Karstadt L. The association between physical and relational bullying and behavior problems among primary school children.J Child Psychol Psychiatry.2000;41:989 –1002
34. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh post-natal depression scale.Br J Psychiatry. 1987;150:782–786
35. Cohen J.Statistical Power Analyses for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988
36. Erdfelder E, Faul F, Buchner A. A general power analysis program.
Behav Res Methods Instrum Comput. 1996;28:1–11
37. Guerin DW, Gottfried AW, Thomas CW. Difficult temperament and behavior problems: A longitudinal study from 1.5 to 12 years.Int J Behav Dev. 1997;21:71–90
38. Thomas A, Chess S. Temperament and Development. New York, NY: Brunner/Mazel; 1977
40. Barr RG. The normal crying curve: what do we really know?Dev Med Child Neurol. 1990;32:356 –362
41. von Hofacker N, Papousek M. Disorders of excessive crying, feeding, and sleeping: the Munich interdisciplinary research and intervention program.Infant Mental Health J. 1998;19:180 –201
42. Papousek M, Wurmser H, von Hofacker N. Clinical perspectives on unexplained early crying: challenges and risks for infant mental health and parent-infant relationships. In: Barr RG, St James-Roberts I, Keefe M, eds.New Evidence on Unexplained Early Crying: Its Origin, Nature and Management. Skillman, NJ: Johnson & Johnson Pediatric Institute; 2001: 289 –316
43. Rutter M, Silberg J, O’Connor T, Simonoff E. Genetics and child psychiatry: II. Empirical research findings.J Child Psychol Psychiatry. 1999;40:19 –56
44. Kuntsi J, Stevenson J. Psychological mechanisms in hyperactivity: II. The role of genetic factors.J Child Psychol Psychiatry. 2001;42:211–219 45. Faraone S, Biederman J, Weiffenbach B, et al. Dopamine D4 gene
7-repeat allele and attention deficit hyperactivity.Am J Psychiatry. 1999; 156:768 –70
46. Whitaker AH, Van Rossem R, Feldman JF, et al. Psychiatric outcomes in
low-birth-weight children at age 6 years: relation to neonatal cranial ultrasound abnormalities.Arch Gen Psychiatry. 1997;54:847– 856 47. Schachar R. Childhood hyperactivity.J Child Psychol Psychiatry. 1991;32:
155–191
48. Wolke D, Meyer R, Ohrt B, Riegel K. Prevalence and risk factors for infant excessive crying at 5 month of age. In: Koops W, Hopkins B, Engelen P, eds.Abstract of the 13th Biennial Meeting of the International Society for the Study of Behavioural Development. Leiden, the Netherlands: Logon Publications; 1994:152
49. Hille ETM, den Ouden AL, Saigal S, et al. Behavioural problems in children who weigh 1000 g or less at birth in four countries.Lancet.
2001;357:1641–1643
50. van den Boom DC, Hoeksma JB. The effect of infant irritability on mother-infant interaction: a growth-curve analysis.Dev Psychol. 1994; 30:581–590
51. Wolke D. Behavioral treatment of prolonged infant crying: evaluation, methods and a proposal. In: Barr R, St James-Roberts I, Keefe M, eds.
New Evidence on Early Infant Crying: Its Origin, Nature and Management. Skillman, NJ: Johnson & Johnson Pediatric Institute; 2001:187–207
HEALTH COSTS WONⴕT GO DOWN!
“Why do health care costs keep on rising? It’s not because doctors and hospitals are greedy; it’s because of medical progress. More and more conditions that once lay beyond doctors’ reach can now be treated, adding years to the lives of patients and greatly increasing the quality of those years— but at ever greater expense. A triple coronary bypass does a lot more for you than a nice bedside manner, but it costs a lot more, too.”
Krugman P.New York Times.March 19, 2002
DOI: 10.1542/peds.109.6.1054
2002;109;1054
Pediatrics
Dieter Wolke, Patrizia Rizzo and Sarah Woods
Persistent Infant Crying and Hyperactivity Problems in Middle Childhood
Services
Updated Information &
http://pediatrics.aappublications.org/content/109/6/1054 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/109/6/1054#BIBL This article cites 38 articles, 9 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.109.6.1054
2002;109;1054
Pediatrics
Dieter Wolke, Patrizia Rizzo and Sarah Woods
Persistent Infant Crying and Hyperactivity Problems in Middle Childhood
http://pediatrics.aappublications.org/content/109/6/1054
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.