A Randomized, Controlled Trial to Evaluate the Effects of the Newborn
Individualized Developmental Care and Assessment Program in a
Swedish Setting
Bjo¨rn Westrup, MD*‡; Agneta Kleberg, RN, BSN‡; Kristina von Eichwald, RN, BSN‡; Karin Stjernqvist, PhD§; and Hugo Lagercrantz, MD, PhD‡
ABSTRACT. Background and Objective. Family-centered developmentally supportive care of very low birth weight infants, provided by the Newborn Individ-ualized Developmental Care and Assessment Program (NIDCAP) has been reported to have positive medical and economic impacts. Our aim was to investigate its effect on need of ventilatory assistance, growth, and hos-pitalization in a Swedish setting.
Methods. Preterm infants born between September 1994 and April 1997 with a gestational age<32 weeks and with a need of ventilatory assistance at 24 hours were randomly assigned to either NIDCAP (n512) or conven-tional care (n513). The 2 groups were comparable (me-dian [range]) with respect to birth weight (1083 [630 –1411] vs 840[636 –1939 g]), head circumference (24.0 [22.3–26.5] vs 24.0 [21.1–30.0 cm]), gestational age (27.6 [24.0 –28.7] vs 26.1 [23.9 –30.3] weeks), female/male ratio (3/9 vs 9/8) and Clinical Risk Index for Babies (4.0 [0 –11] vs 6.0 [2–15]). The infants in the intervention group were cared for in a separate room by a group of specially trained nurses. Formal weekly observations of these in-fants starting within 3 days after birth and continuing until 36 weeks postconception were used to develop in-dividualized care plans. These plans provided recom-mendations as to how care might be attuned to the cur-rent developmental stage of the infant and how the family might be supported and stimulated to participate in this care. The treatment of the 2 groups was in all other respects identical.
Results. The duration of mechanical ventilation (me-dian [range] was 2.8 [0 –36.7] days in the intervention group vs 4.8 [.1–29.8] days; not significant [NS]) among the controls and continuous positive airway pressure was applied for 26.1 (6.9 –52.0) vs 43.9 (5.0 – 65.1) days. Supple-mentary oxygen was withdrawn at 33.0 (29.3–35.7) vs 38.1 (33.1– 44.9) weeks of postconceptional age (PCA). The weight gain up to 35 weeks of PCA was 13.0 (6.7–21.0) vs 9.8 (6.8 –16.6) g/day (NS). The head growth up to 35 weeks of PCA was .73 (.56 –1.3) vs .63 (.56-.77) cm/week (NS). The age of the infant at discharge was 38.3 (36.1–57.7) vs 41.0 (36.9 – 48.4) weeks of PCA (NS).
Conclusions. NIDCAP does not seem to have detri-mental effects on Swedish very low birth weight infants
in comparison with conventional care. Indeed, NIDCAP might even be advantageous.Pediatrics 2000;105:66 –72; infant, very low birth weight growth and development infant, low birth weight infant, newborn infant, premature growth and development infant, premature infant, prema-ture, diseases nursing infant, premaprema-ture, diseases preven-tion and control, intensive care units, neonatal standards intensive care units, neonatal utilization intensive care, neonatal methods intensive care, neonatal nursing meth-ods, neonatal nursing standards, patient care planning standards, bronchopulmonary dysplasia/prevention and control/therapy, human.
ABBREVIATIONS. VLBW, very low birth weight (,1500 g); BPD, bronchopulmonary dysplasia; NIDCAP, Newborn Individualized Developmental Care and Assessment Program; RCT, randomized controlled trial; PCA, postconceptional age; CPAP, continuous positive airway pressure; CRIB, Clinical Risk Index for Babies; IVH, intraventricular hemorrhage; PDA, persistent ductus arteri-osus; CLD, chronic lung disease; NS, not significant.
T
he survival of very low birth weight infants(VLBW;,1500 g) has increased from 50%1to
.80%2,3since the initiation of neonatal
inten-sive care in the early 1970s. However, a concomitant decrease in morbidity has not yet been conclusively shown to have taken place.
Long-term pulmonary morbidity has been an issue of great concern ever since Northway and associates4
first described bronchopulmonary dysplasia (BPD) in 1967. Nevertheless, its incidence seems to have remained unchanged at 25% to 30%, because of the increasing number of extremely low birth weight infants (,1000 g) who survive.5,6
Neurodevelopmental outcome is another major is-sue for VLBW infants. Follow-up studies have re-ported the incidence of disability to be 15% to 25%,7–9
a figure that has also remained fairly constant over time.7,10In addition, as an increasing number of
sur-vivors reach school age, more minor impairments cause great concern. Difficulties with attention, be-havior, visual–motor integration, language perfor-mance, and academic skills seem to demonstrate a prevalence of ;40%.11–15
Both animal and human studies have documented the manner in which the sensory input influences the structure and function of the central nervous system, as well as the behavior of the newborn.16 –18 Infants
born with a VLBW receive inadequate stimulation. Treatment and care-giving procedures cause pain From the *Department of Clinical Science, Pediatrics, Umeå University,
Umeå, Sweden; ‡Neonatal Programme, Department of Woman and Child Health, Astrid Lindgren Children’s Hospital, Karolinska Institute, Stock-holm, Sweden; and the §Departments of Pediatrics and Psychology, Uni-versity of Lund, Lund, Sweden.
Received for publication Feb 9, 1999; accepted Aug 23, 1999.
and discomfort, making it difficult for VLBW infants to experience restful and undisturbed periods of sleep. During a 24-hour observation period, such infants have been reported to be handled on the average .200 times.19 Furthermore, the care-giving
itself was found to be associated with three fourths of all hypoxemic episodes in a group of 15 preterm infants.20 Increased levels of stress hormones have
been observed to occur in association with routine nursing procedures.21
Family-Centered Developmentally Supportive Care The important role of the family in caring for VLBW infants has also been emphasized and the concept of family-centered care has been strongly advocated.22Minde et al23have shown that neonatal
illness may have a lasting negative effect on parent– infant interactions.
Als24has integrated findings from other scientific
disciplines with those from developmental psychol-ogy and formulated a new idea of care-giving, which puts the focus on respect for the very tiny human being. She developed a theoretical framework for family-centered, developmentally supportive care, the so-called Synactive Theory, which describes the infant as an organism displaying 5 subsystems, ie, the autonomic–physiologic, motor, state organiza-tional, attentional–interactive, and self-regulatory systems. These systems are described as interactive, with Als pointing out how the functional state of 1 system profoundly influences the others. Thus, the stability and efficient functioning of 1 of these sys-tems affects the functions of the other syssys-tems in a positive fashion. For example, helping an infant to calm down his/her movements results in improved autonomic function, with improved respiration and saturation, which in turn also promotes the infant’s ability to interact socially with the parent or care-giver. The 5 subsystems interact synergistically.
Based on this theoretical framework, Als devel-oped the program of intervention known as the Newborn Individualized Developmental Care and Assessment Program (NIDCAP). The major ap-proach used in this program is weekly, formalized, naturalistic observations of the infant before, during, and after a care-giving procedure, eg, feeding, changes of diaper, collection of a blood sample, re-positioning, etc. Behavioral and physiologic changes are monitored by 2-minute epochs. Subsequently the observer evaluates the infant’s current ability to or-ganize and modulate his/her 5 subsystems and notes the infant’s signals of well being and self-regulation, as well as signals of sensitivity and stress. The in-fant’s behavior, described as avoidance of or ap-proach toward stimuli, enables the observer to assess how the infant strives to cope with his/her environ-ment and continue his/her developenviron-ment. These ob-servations provide information concerning the in-fant’s strengths and weaknesses at the point of time in question. In addition, information is obtained con-cerning how well the environment, the caregivers, and family members are attuned to the current needs of the infant.
Subsequently, the observer writes a report
describ-ing in detail the behavior of the infant durdescrib-ing the entire observation. This report is then used to explain the behavior of the infant in guidance of the parents and caregivers by illustrating complex interactions among the infant’s different subsystems. For a trained observer, this entire procedure requires 3 to 4 hours.
Based on this procedure, recommendations with respect to care-giving designed to support the indi-vidual infant’s development are formulated. Such recommendations may include details on how to:
• adjust the infant’s physical environment by reduc-ing the levels of sound, light and activity;
• make it easier for the infant to assume a flexed position by making a nest in the incubator, thus facilitating self-soothing/-regulatory behavior; • concentrate care-giving to certain limited periods
to allow restful sleep; and
• help parents to understand their infant’s signals, enhance their ability to recognize the infant’s needs and encourage their early participation in care-giving.
The group of Als and others have reported sub-stantial positive effects of NIDCAP with respect to both the short-term medical and behavioral out-comes (eg, less requirement for assisted ventilation, fewer intracranial hemorrhages, faster weight gain, shorter hospitalization, and better behavioral scores at the time of discharge,25–32as well as improvements
in parent–infant interactions33and the child’s
devel-opment).25,27
During recent years, a rapidly growing interest in NIDCAP has been demonstrated by neonatal nurses in both North America and Sweden but the program has met more skepticism from physicians. Some neo-natologists recommend general use of the method,34
whereas others are skeptical, criticizing published studies as being conducted with inappropriate meth-odology and before the general use of prenatal ste-roids and surfactant. Furthermore, the intervention is believed to be cumbersome and time-consuming and the results too good to be true.35–37
The aim of the present randomized controlled trial (RCT) was to examine the effects of NIDCAP in a Swedish setting. In this report on short-term results, our primary hypothesis was that there would be no impact on the requirement for assisted ventilation, growth, or the period of hospitalization. Other as-pects of this study (eg, the impact of NIDCAP on physiologic variables, parental experience, the moth-er–infant relationship, and follow-up data) will be reported later.
METHODS
The number of infants required for this study was estimated using a nomogram for a 2-sample comparison for a continuous variable relating a power of 80%, a significance level of .05 and the standardized differences estimated from the findings of the pre-vious studies. An increased daily weight gain of 3 g, a decreased need of supplementary oxygen of 25 days, and a 2 weeks earlier discharge would yield to a sample size of 40, 56, and 48 infants, respectively.
Recruit-ment began in September 1994. It proceeded much more slowly than expected, because of a drop in the birth rate and political decisions about health care (including downsizing). There was also an increasingly strong opinion among the nursing staff that NIDCAP should be implemented throughout the unit. Thus, after having studied only 25 infants, we decided to terminate this study in April 1997.
Inclusion criteria consisted of: 1) inborn, 2) singleton, 3) postcon-ceptual age (PCA) of,32 weeks, 4) absence of severe malformation, 5) need of ventilatory support 24 hours after birth, at least in the form of continuous positive airway pressure (CPAP), 6) family residence in the geographical district of the hospital to ensure full hospital stays at the study hospital, and 7) Swedish language facility attributable to the design of the follow-up.
To assure the NIDCAP intervention onset at birth, the infants were randomized immediately using sealed envelopes in blocks of 4. Infants assigned to the intervention were admitted to a special room directly after delivery. Informed consent was obtained. This procedure resulted in the randomization of infants who did not fulfill all the criteria for selection 24 hours after birth, who were subsequently excluded from the study.
One of 3 preexisting nursing teams was assigned to the NIDCAP infants. This team had been specially trained and was additionally supported by 2 formally NIDCAP-certified nurses. The infants were received weekly formal NIDCAP observations, starting within 3 days after birth and continuing until 36 weeks of PCA. In all other respects, the treatment of the 2 groups was identical. The ethical committee of the hospital approved the study.
In all cases, gestational age was determined by ultrasound during early pregnancy. The severity of illness was analyzed using the Clinical Risk Index for Babies (CRIB),38which is calcu-lated from the birth weight and gestational age, as well as the levels of blood gases and fraction of the inspired oxygen during the first 12 hours.
CPAP treatment was administered to all infants demonstrating spontaneous respiration at birth. Surfactant installation and me-chanical ventilation was initiated when respiratory efforts were deemed inadequate, when frequent apneas occurred, and/or when CPAP with 5 to 6 cm H2O and Fio2..4-.6 produced a Po2,6 kPa, Pco2 .8.5 kPa, and/or pH ,7.25. CPAP treatment was terminated at pressures of 2 cm H2O and Fio2,.3. Transcutaneous oxygen saturation was maintained at 90% to 94%. The periods of mechanical ventilation and CPAP treatment were registered by the hour. In contrast, the use of supplementary oxygen, when supplied daily for.1 hour, was expressed in days.
BPD was assessed by chest radiograph at 36 weeks of PCA according to a modified version of the recommendations of Toce et al.39Interstitial parenchymal changes, overall lung expansion, and focal emphysema were given scores from 0 to 2. The severity of BPD was classified from the total score as follows: mild, 1 to 3; moderate, 4 to 5; severe, 6. Subsequently, the infants were grouped in 2 categories: none–mild and moderate–severe.
Apneas were quantified from the charts. Sepsis was concluded to be present when a blood culture result was positive and/or antibiotic treatment was administrated for.6 days in response to clinical symptoms and elevated C-reactive protein. The endpoint for the measurement of growth parameters was set at 35 weeks of PCA to include subjects discharged early from the hospital.
All the infants were subjected to a cranial ultrasound examina-tion within the first week after birth and weekly thereafter if clinically warranted. Intraventricular hemorrhage (IVH) was re-corded according to Papile et al.40Eye examinations were per-formed on all survivors after 32 weeks of PCA, following the guidelines of the International Committee for the Classification of Retinopathy of Prematurity.41
The continuous variables were compared statistically using the Mann-WhitneyU test. For categorical variablesx2with exactP values and Fisher’s exact test were used. An overallP value of ,.05 was obtained by sequential adjustment for multiple tests according to Holm.42The statistical analyses were performed em-ploying the SPSS Version 8.0 (SPSS Inc, Chicago, IL).
RESULTS
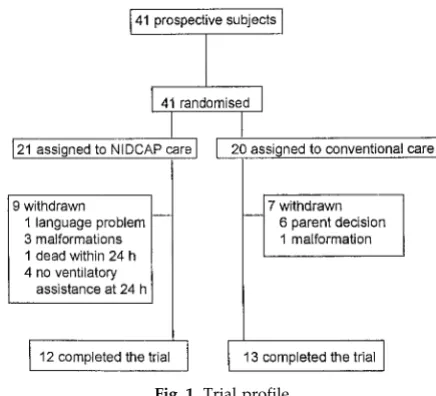
Between September 1994 and April 1997, all 41 prospective subjects for inclusion in this study were identified, ie,;20% of all infants admitted to the unit
with a gestational age ,32 weeks. Of these infants, 31 proved to be eligible for inclusion 24 hours after birth, the time for definitive enrollment. Twelve had been chosen randomly for the NIDCAP intervention and 19 for conventional care. The parents of 6 infants, all assigned to the control group, decided not to participate in the study (birth weight: 888 [199 g] mean [standard deviation]; gestational age: 26.7 [1.4] weeks; CRIB: 3.8 [3.4]; female/male: 3/3; SGA: 2/6). The investigation of the physiologic data (stress hor-mones in saliva, urine, and electroencephalogram— not reported in this article) could possibly have in-fluenced their decision. It is our impression that when the parents realized they had been allocated to the nonintervention group they lost their incentives to participate. Four of these 6 infants were later trans-ferred to other hospitals and thus received different treatment. Thus, the intervention group consisted of 12 infants and the control group of 13 subjects (Fig 1) with similar backgrounds (Table 1).
Our findings are summarized in Table 2. The in-fants receiving care according to NIDCAP required significantly less ventilatory support, compared with the control infants. Four infants in the intervention group never required mechanical ventilation. In the control group, there was 1 infant who was extubated already after 2 hours. None of these infants were given surfactant. The respective mean values (stan-dard deviation) for CPAP were 27.0 (12.0) versus 44.1 (16.5) days and for PCA at the time of oxygen with-drawal 32.9 (1.8) versus 38.1 (3.6) weeks. At 36 weeks of PCA, 6 of the infants in the NIDCAP group had mild signs of BPD on chest radiograph but none required supplementary oxygen. In the control group, there were 2 infants with mild, 4 with mod-erate, and 2 with more severe signs of BPD; all 8 needed extra oxygen. The mean head growth (stan-dard deviation) up to 35 weeks of PCA was .80 (.22) in the NIDCAP group, compared with .63 (.07) cm/ week among the controls.
In addition to the primary outcomes, clinical ob-servations of interest are summarized in Table 3. Hospital mortality for the NIDCAP group was 1/12 versus 2/13 for the controls. Furthermore, 1 infant in
the control group died of Sudden Infant Death Syn-drome at 8 months of age. No hydrocephalus, IVH of grade IV, or periventricular leukomalacia was ob-served in any of the subjects. There was 1 infant with IVH grade III in the NIDCAP group, compared with 3 such cases in the control group. There were 2 infants with symptomatic persistent ductus arterio-sus (PDA) in each group. None of the differences in these observations were statistically significant.
DISCUSSION
Our results indicate that intervention according to NIDCAP does not have a negative impact on the care of VLBW infants and might even be advantageous. The mean duration of CPAP treatment was short-ened by 17 days. None of the 11 infants in the NID-CAP group required supplementary oxygen at 36 weeks of PCA (ie, demonstrated chronic lung disease [CLD] of the premature), in comparison to 8/11 among the neonatal survivors of the controls.
The incidence of CLD in the control group could seem high. However, similar incidences in selective groups of VLBW infants have been documented in a recent report from our institution in which CLD was found to be associated with PDA and late-onset sep-sis.43 There were no group differences in the
inci-dences of these conditions, in the present study. There was an indication of enhanced head growth in the intervention group. Although this is in agree-ment with the findings of Stevens and collabora-tors,30this finding did not remain significant after the
correction for multiple comparisons. Other variables, eg, weight gain, number of apneas, requirement for antibiotic treatment, and retinopathy of prematurity tended to be positively influenced by NIDCAP as well.
Four of the 21 infants initially assigned to NIDCAP care and none of the 20 infants assigned to conven-tional care were withdrawn from the study because they were too healthy, ie, did not fulfill the criteria of inclusion at 24 hours of age (see Fig 1). It might be speculated that NIDCAP is especially effective if ap-plied immediately after birth.
This possible early effect was the reason for our randomization process. The parents were not blind to the allocation at the time of their final consent. Undoubtedly, it would have been preferable to ob-tain their decision before delivery or immediately at birth. Considering the acuteness of many premature births, this would not have been possible in all cases. Furthermore, we did not find it ethically correct to approach the parents in this psychological very hard moment, because the NIDCAP intervention very un-likely would cause the infants any discomfort or harm. This assumption was based on our earlier experience and the previous reports of others. The ethical board of the hospital approved this proce-dure.
There were 2 major reasons for terminating the trial before the desired number of subjects were ob-tained. Because the recruitment took a much longer time than anticipated, we noticed that the risk for a spillover effect to the control group increased. Nurses involved in NIDCAP care soon became con-vinced of its beneficial effects and, from time to time, exchanges of personnel between the 2 groups were necessitated by acute staffing problems. Further-more, the staff of the controls was increasingly ex-pressing feelings of discomfort and disloyalty, not being able to offer developmentally supportive care to their patients.
The introduction of NIDCAP is a multidisciplinary TABLE 1. Characteristics of the Two Study Groups
NIDCAP Groupn512 Control Groupn513
Mother’s age (y) 30.2 (24.2–36.3) 32.5 (18.3–39.4)
Maternal education* (,12/12/13–14/$15 y) 0/6/1/5 3/6/2/2
Prenatal steroids (none/,24 h/.24 h) 3/3/6 5/1/7
Gender (female/male) 3/9 5/8
Birth weight (g) 1083 (630–1411) 840 (636–1939)
Head circumference (cm) 24.0 (22.3–26.5) 24.0 (21.1–30.0)
Gestational age (wk) 27.6 (24.0–28.7) 26.1 (23.9–30.3)
Severity of illness (CRIB)† 4.0 (0–11) 6.0 (2–15)
Median (range), none of the differences were statistically significant. * 12 years indicates high school degree; 15 years, college degree. † According to the International Neonatal Network.38
TABLE 2. Ventilatory Assistance, Growth, and Hospitalization
Survivors NIDCAP Groupn51 Control Groupn510 P
Mechanical ventilation (d) 2.8 (0–36.7) 4.8 (.1–29.8) NS
CPAP (d) 26.1 (6.9–52.0) 43.9 (5.0–65.1) .045
PCA at oxygen withdrawal (wk) 33.0 (29.3–35.7) 38.1 (33.1–44.9) .007
BPD (no.)*
None-mild/moderate-severe 11/0 4/6 .024†
Weight gain up to 35 wk PCA‡ (g/d) 13.0 (6.7–21.0) 9.8 (6.8–16.6) NS
Head growth up to 35 wk PCA‡ (cm/wk) .73 (.56–1.3) .63 (.56–.77) NS
PCA at discharge (wk) 38.3 (36.1–57.7) 41.0 (36.9–48.4) NS
Median (range); Mann-WhitneyUtest if not otherwise indicated;Pvalues adjusted for multiple tests according to Holm.42 * Chest radiograph findings at 36 weeks’ PCA.
† Fisher’s exact test.
process involving not only medicine and nursing, but also developmental, family, and organizational
psychology. NIDCAP requires some physical
changes in the NICU, as well as considerable educa-tional efforts. Evaluation of its effects is complicated by the complexity of the intervention. In comparison to studies involving different drug treatments, it is more difficult to achieve an optimal experimental design.
Consequently, many previous studies25,30 –32,44,45on
NIDCAP have been using a historical design. This fact has given rise to certain methodological concerns and doubts about the results obtained.35–37 To our
knowledge, the present study is the first RCT outside of North America.
Despite our randomized design, certain problems were encountered. The attending neonatologists were not unaware of the infants’ status in the study. However, decisions concerning ventilatory support were made according to guidelines by several differ-ent neonatologists not directly involved in the study. The first author in this study was not working at the unit involved and the nursing staff for the NIDCAP group was not composed of volunteers. In contrast, after these nurses had received general NIDCAP training and experienced observations involving care-giving plans and the general support of the NIDCAP-certified nurses, they probably influenced the need for ventilatory support. By being aware of the cues provided by the infants, they could suggest an appropriate time for terminating CPAP treatment and subsequently provide competent support for the infant’s self-regulation of its different subsystems, including the autonomic system associated with re-spiratory regulation.
Our findings here are in line with previous studies. In an RCT from the era before surfactant treatment was used, Als et al27 reported positive effects of
NIDCAP in the form of a reduced requirement for ventilatory support, a reduced incidence of IVH and CLD, improved weight gain, cost-savings, improved self-regulatory abilities, and improved mental and psychomotor development at 9 months of age. In a repeat study, in which surfactant treatment was also used, the Fleisher et al29observed a reduced
require-ment for ventilatory support, improved behavioral performance and less chronicity in addition to
cost-savings. In the follow-up study at 2 years of age, another group of investigators46did not demonstrate
improved development. However one third of the original subjects were lost from the study, implying possible sample bias and renders their follow-up data less reliable.
Both of these RCTs included only infants with a birth weight of ,1250 g, ,28 weeks of PCA, and who were ventilated mechanically for .24 hours starting within 3 hours after birth. Interestingly, when Buehler and associates28 examined a low-risk
group of infants born between 30 and 34 weeks of PCA and not requiring mechanical ventilation, NIDCAP still improved behavioral, neurological, and electrophysiological maturation.
The complexity of developmentally supportive care and its demand for comprehensive training has caused some concern about its cost-effectiveness.35
However, several groups have reported that
NIDCAP actually reduces costs by $4000 to 120 000 per infant,26,27,29 –32depending on his/her birth weight
and initial illness.
Concerns have been expressed that the implemen-tation of this program would require extra nursing time. It is our experience45 that NIDCAP increases
the competence of both staff members and parents. Care-giving is specifically adjusted to the current medical and developmental status of the infant. It might be speculated that the caregivers become more skilled and detect changes in the infant’s status at an earlier stage. This might, in turn, lead to prompt intervention and prevention of additional deteriora-tion. Thus, the infants become more physiologically stable and actually require less nursing time, which is in line with the findings of others.30,32
Our earlier study45 also indicated that
environ-mental changes in the neonatal unit are not in them-selves sufficient to explain the improvement ob-served. During periods without NIDCAP observations, we have experienced an obvious decline in the qual-ity of care. Thus, to achieve improvements regular observations seem to be essential, although to what extent remains to be determined.
It is important to emphasize that not all personnel are suited to become NIDCAP observers. It requires a good deal of sensitivity to interpret the subtle signs of a premature infant and a great deal of psycholog-TABLE 3. Clinical Observations
NIDCAP Group Control Group
All subjects n512 n513
Survival (at discharge)
Alive/deceased 11/1 10/3
IVH*
None/grade I/grade II/grade III/grade IV 9/2/0/1/0 8/0/2/3/0
Neonatal survivors n511 n510
Antibiotic treatment (IV; d) 18 (6–53) 31 (18–55)
Sepsis† (none/1/$2) 1/3/7 0/2/8
Apneas (number) 33 (4–162) 49 (2–158)
Retinopathy of prematurity$stage 3ठ4/11 8/11
Median (range); none of the differences were statistically significant. * According to Papile.40
† A positive blood culture and/or antibiotic treatment for.6 days in combination with clinical symptoms and elevated C-reactive protein. ‡ According to the International Committee for the Classification of Retinopathy of Prematurity.11
ical skill to interact with the staff and parents in such a manner that they feel supported and not criticized. It should also be mentioned that implementation of developmental care in the hands of an unskilled person involves a potential risk of over-emphasizing the protection of the infant, ie, to forget the individ-ualized portion of the program. NIDCAP ought not be implemented unreflectively, eg, by completely covering the isolette of a not-yet-stabilized infant, thereby preventing its necessary surveillance; by building containment for the infant that is too rigid; and by over-protecting a stable, competent baby from visual, auditory, and social input, thus prevent-ing it from developprevent-ing its own ability to self-regulate and interact socially. Instead, intervention should be designed from the viewpoint of each individual in-fant, ie, by attempting to determine what is appro-priate for this particular infant at this particular time, considering all factors, including the infant’s medical status.
Care and intervention based on the infant’s own behavior seem attractive from an ethical point of view and, in addition, make good biological sense. Nurses and parents have implemented NIDCAP with great enthusiasm. Among neonatologists, there has been both praise and skepticism. Based on our own practical experience and on the findings in our limited study, we conclude that family-centered de-velopmentally supportive care seems to be beneficial in a Swedish setting. Larger multicenter studies with follow-up programs are now warranted to further confirm the indications of the positive impacts of NIDCAP on VLBW infants.
ACKNOWLEDGMENTS
This study was supported by the Vårdal Foundation, Dalarna Research Institute, Federation of County Councils, Smedby Foun-dation, Sa¨llskapet Barnavård, Sunnerdahls FounFoun-dation, First of Mayflower Annual Campaign, and Solstickan Foundation.
The assessment of the chest radiograph examinations by Hed-wig Wahlgren is gratefully acknowledged.
REFERENCES
1. Stewart AL, Reynolds EO, Lipscomb AP. Outcome for infants of very low birthweight: survey of world literature.Lancet. 1981;1:1038 –1040 2. Horbar JD, Wright EC, Onstad L. Decreasing mortality associated with
the introduction of surfactant therapy: an observational study of neo-nates weighing 601 to 1300 grams at birth.Pediatrics. 1993;92:191–196 3. Lagercrantz H, Katz-Salamon M, Forssberg H. The Stockholm neonatal
project: Neonatal mortality and morbidity at the Children’s Centre, Karolinska Hospital.Acta Paediatr Suppl. 1997;419:11–15
4. Northway WH Jr, Rosan RC, Porter DY. Pulmonary disease following respirator therapy of hyaline-membrane disease: bronchopulmonary dysplasia.N Engl J Med. 1967;276:357–368
5. Northway WH Jr. Bronchopulmonary dysplasia: twenty-five years later.Pediatrics. 1992;89:969 –973
6. Yeo CL, Choo S, Ho LY. Chronic lung disease in very low birthweight infants: a 5-year review.J Paediatr Child Health. 1997;33:102–106 7. Escobar GJ, Littenberg B, Petitti DB. Outcome among surviving very
low birthweight infants: a meta-analysis. Arch Dis Child. 1991;66: 204 –211
8. Cooke RW. Factors affecting survival and outcome at 3 years in ex-tremely preterm infants.Arch Dis Child. 1994;71:F28 –F31
9. Bylund B, Cervin T, Finnstrom O, et al. Morbidity and neurological function of very low birthweight infants from the newborn period to 4 y of age: a prospective study from the south-east region of Sweden.Acta Paediatr. 1998;87:758 –763
10. Pharoah PO, Platt MJ, Cooke T. The changing epidemiology of cerebral palsy.Arch Dis Child Fetal Neonatal Educ. 1996;75:F169 –F173
11. Sell EJ, Gaines JA, Gluckman C, Williams E. Early identification of learning problems in neonatal intensive care graduates.Am J Dis Child. 1985;139:460 – 463
12. Ornstein M, Ohlsson A, Edmonds J, Asztalos E. Neonatal follow-up of very low birthweight/extremely low birthweight infants to school age: a critical overview.Acta Paediatr. 1991;80:741–748
13. Hack M, Taylor HG, Klein N, Eiben R, Schatschneider C, Mercuri-Minich N. School-age outcomes in children with birth weights under 750 g.N Engl J Med. 1994;331:753–759
14. Hall A, McLeod A, Counsell C, Thomson L, Mutch L. School attainment, cognitive ability and motor function in a total Scottish very-low-birthweight population at eight years: a controlled study.Dev Med Child Neurol. 1995;37:1037–1050
15. Stjernqvist K, Svenningsen W. Ten-year follow-up of children born before 29 gestational weeks: health, cognitive development. behaviour and school achievement.Acta Paediatr. 1999;88:557–562
16. Wiesel TN, Hubel DH. Comparison of the effects of unilateral and bilateral eye closure on cortical unit responses in kittens.J Neurophysiol. 1965;28:1029 –1040
17. Philbin MK, Ballweg DD, Gray L. The effect of an intensive care unit sound environment on the development of habituation in healthy avian neonates.Dev Psychobiol. 1994;27:11–21
18. Rosenblum LA, Andrews MW. Influences of environmental demand on maternal behavior and infant development.Acta Paediatr. 1994;397: 57– 63
19. Murdock D. Handling during neonatal intensive care.Arch Dis Child. 1984;59:957–961
20. Long JG, Lucey JF, Philip AG. Noise and hypoxemia in the intensive care nursery.Pediatrics. 1980;65:143–145
21. Lagercrantz H, Nilsson E, Redham I, Hjelmdahl P. Plasma cat-echolamines following nursing procedures in a neonatal ward.Early Hum Dev. 1986;14:61– 65
22. Harrison H. The principles for family-centered neonatal care.Pediatrics. 1993;92:643– 650
23. Minde K, Whitelaw A, Brown J, Fitzhardinge P. Effect of neonatal complications in premature infants on early parent-infant interactions.
Dev Med Child Neurol. 1983;25:763–777
24. Als H. A synactive model of neonatal behavioral organization.Phys Occup Ther Pediatr. 1986;6:3–55
25. Als H, Lawhon G, Brown E, et al. Individualized behavioral and envi-ronmental care for the very low birth weight preterm infant at high risk for bronchopulmonary dysplasia: neonatal intensive care unit and de-velopmental outcome.Pediatrics. 1986;78:1123–1132
26. Becker PT, Grunwald PC, Moorman J, Stuhr S. Outcomes of develop-mentally supportive nursing care for very low birth weight infants.
Nurs Res. 1991;40:150 –155
27. Als H, Lawhon G, Duffy FH, McAnulty GB, Gibes-Grossman R, Blick-man JG. Individualized developmental care for the very low-birth-weight preterm infant: medical and neurofunctional effects.JAMA. 1994;272:853– 858
28. Buehler DM, Als H, Duffy FH, McAnulty GB, Liederman J. Effective-ness of individualized developmental care for low-risk preterm infants: behavioral and electrophysiologic evidence.Pediatrics. 1995;96:923–932 29. Fleisher BE, VandenBerg K, Constantinou J, et al. Individualized devel-opmental care for very low birthweight premature infants improves medical and neurodevelpmental outcome in the neonatal intensive care unit.Clin Pediatr. 1995;10:523–529
30. Stevens B, Petryshen P, Hawkins J, Smith B, Taylor P. Developmental versus conventional care: a comparison of clinical outcomes for very low birth weight infants.Can J Nurs Res. 1996;28:97–113
31. Petryshen P, Stevens B, Hawkins J, Stewart M. Comparing nursing costs for preterm infants receiving conventional vs. developmental care.Nurs Econ. 1997;15:138 –145, 150
32. Brown LD, Heermann JA. The effect of developmental care on preterm infant outcome.Appl Nurs Res. 1997;10:190 –197
33. Parker SJ, Zahr LK, Cole JG, Brecht ML. Outcome after developmental intervention in the neonatal intensive care unit for mothers of preterm infants with low socioeconomic status.J Pediatr. 1992;120:780 –785 34. Merenstein GB. Individualized developmental care: an emerging new
standard for neonatal intensive care units.JAMA. 1994;272:890 – 891 35. Lacy JB. Developmental care for very low-birth-weight infants.JAMA.
1995;273:1575–1576
36. Ohlsson A. Developmental care for very low-birth weight infants.
JAMA. 1995;273:1576
38. The International Neonatal Network. The crib (clinical risk index for babies) score: a tool for assessing initial neonatal risk and comparing performance of neonatal intensive care units.Lancet. 1993;342:193–198 39. Toce SS, Farrell PM, Leavitt LA, Samuels DP, Edwards DK. Clinical and
roentgenographic scoring systems for assessing bronchopulmonary dysplasia.Am J Dis Child. 1984;138:581–585
40. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm.J Pediatr. 1978;92:529 –534
41. The International Committee for the Classification of ROP. An interna-tional classification of retinopathy of prematurity.Arch Ophtalmol. 1987; 105:906 –912
42. Holm S. A simple sequentially rejective multiple test procedure.Scand J Stat.1976;6:65–70
43. Jonsson B, Katz-Salamon M, Faxelius G, Broberger U, Lagercrantz H. Neonatal care of very-low-birthweight infants in special-care units and neonatal intensive-care units in stockholm: early nasal continuous pos-itive airway pressure versus mechanical ventilation, gains and losses.
Acta Paediatr Suppl. 1997;419:4 –10
44. Becker PT, Grunwald PC, Moorman J, Stuhr S. Effects of developmental care on behavioral organization in very-low-birth-weight infants.Nurs Res. 1993;42:214 –220
45. Westrup B, Kleberg A, Wallin L, Lagercrantz H, Wikblad K, Stjernqvist K. Evaluation of the Newborn Individualized Developmental Care and Assessment Program (NIDCAP) in a Swedish setting.Prenat Neonat Med. 1997;2:366 –375
DOI: 10.1542/peds.105.1.66
2000;105;66
Pediatrics
Lagercrantz
Björn Westrup, Agneta Kleberg, Kristina von Eichwald, Karin Stjernqvist and Hugo
Setting
Individualized Developmental Care and Assessment Program in a Swedish
A Randomized, Controlled Trial to Evaluate the Effects of the Newborn
Services
Updated Information &
http://pediatrics.aappublications.org/content/105/1/66 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/105/1/66#BIBL This article cites 44 articles, 9 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/agency_abcs Agency ABC's
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.105.1.66
2000;105;66
Pediatrics
Lagercrantz
Björn Westrup, Agneta Kleberg, Kristina von Eichwald, Karin Stjernqvist and Hugo
Setting
Individualized Developmental Care and Assessment Program in a Swedish
A Randomized, Controlled Trial to Evaluate the Effects of the Newborn
http://pediatrics.aappublications.org/content/105/1/66
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.