SPECIAL ARTICLE
Perinatal Care at the Threshold of Viability: An
International Comparison of Practical Guidelines for
the Treatment of Extremely Preterm Births
Maria Serenella Pignotti, MD, Gianpaolo Donzelli, MD
Neonatal Medicine, A. Meyer Children Hospital, University of Florence, Florence, Italy
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
Over the last 2 decades, the survival rate of infants born atⱕ25 weeks of gestation has increased; however, significant morbidity and disability persist. The commitment for their care gives rise to a variety of complex medical, social, and ethical aspects. Decision-making is a crucial issue that involves the infant, the family, health care providers, and society. In a review of the existing guidelines, we investigated the different approaches in the care of extremely preterm births in various countries. We found that many scientific societies and professional organizations have issued guidelines that address the recommendations for the care of these fetuses/neonates although to varying degrees. In this article we compare different approaches and assess the scientific grounds of the specific recommendations. With current stan-dards, intensive care is generally considered justifiable atⱖ25 weeks, compassionate care atⱕ22 weeks, and an individual approach at 23 to 24 weeks, consistent with the parents’ wishes and the infant’s clinical conditions at birth.
W
ITH CONTINUAL PROGRESSin perinatal care, the limit of human viability has moved toward an increasingly younger gestational age. Thanks to modern care standards, the survival rate has risen, although for infants born between 22 and 25 weeks’ gestation, it is still very low,1–5and in our opinion the increased nonimpaired survivaldemonstrated with aggressive management at 23 to 24 weeks in Norway and Sweden by Markestad et al6 and
Serenius et al,7respectively, does not seem to have a great impact on the ethical dilemma regarding intensive care
in these infants. The threshold of human viability seems to be limited to the physiologic development of the lungs that takes place around weeks 22 to 24. Consequently, survival rate at this age is not expected to improve, at least with the current technologic resources.8–10 Moreover, the care of such tiny infants implies a variety of complex
medical, social, and economical aspects calling for ethical decisions, because the boundary between utility and futility is not clear. The infant’s best interests are far from being understood, and concern surrounding the ethical basis of providing such intensive, multidisciplinary, lifelong care is growing in the scientific world. The majority of these infants will die before, during, or after birth in the NICU.1For those who survive, there is further risk of death during
childhood, and approximately half will suffer from moderate-to-severe neurodevelopmental problems.2At the age of
6 years, some of those previously believed to be healthy will show some kind of disability.3To help parents and
physicians in the management of an extremely preterm birth, various forms of guidelines have been approved by many scientific societies in different countries. As defined by the Institute of Medicine,11clinical practice guidelines
are “systematically developed statements to assist practitioner and patient decisions about appropriate healthcare for specific clinical circumstances.” Their purpose is “to make explicit recommendations with a definitive intent to influence what clinicians do.”12Because of the ongoing discussion about the limit of viability, to compare different
approaches, if any, regarding the care of extremely preterm fetuses/neonates, we conducted a search in international literature to investigate the existing guidelines in this field of perinatal care.
METHODS
We searched (2005–2006) Pubmed, Embase, and Google, currently the most-used search engines,13 for practical
guidelines on perinatal care at an extremely preterm gestational age using “practice guidelines,” “newborn,” “withholding treatment,” “fetal viability,” and “perinatal care” as key words. We also sourced recent issues in relevant
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-0513
doi:10.1542/peds.2007-0513
Key Words
practice guidelines, newborn, withholding treatment, fetal viability, perinatal care
Accepted for publication Jun 19, 2007 Address correspondence to Maria Serenella Pignotti, MD, Neonatal Medicine, A. Meyer Children’s Hospital, University of Florence, via Luca Giordano 13, 50132 Firenze, Italy. E-mail: [email protected]
international journals and expanded our search by fol-lowing the references in the articles identified, obtaining specific information from personal knowledge and from referents of specialist perinatal societies of which the names were indicated on Web pages. Local institutional practical guidelines were excluded from the study. The guidelines published by scientific societies were com-pared. Each document was carefully examined, and spe-cific statements were independently noted and orga-nized into 2 coherent themes: specific treatment suggestions and practical care aspects. Extremely pre-term birth was defined in our study as the delivery of a stillborn or a live fetus before 26 completed weeks. Ges-tational age was defined as the postmenstrual age in weeks and days as per the International Classification of Diseases, 10th Revision.14 The time period between 230⁄7
and 236⁄7weeks is referred to as 23 completed weeks of
gestation (ie, the infant has completed the 23rd week of gestation and entered the 24th week).
RESULTS
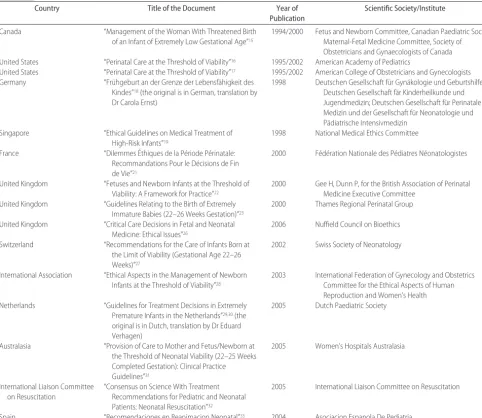
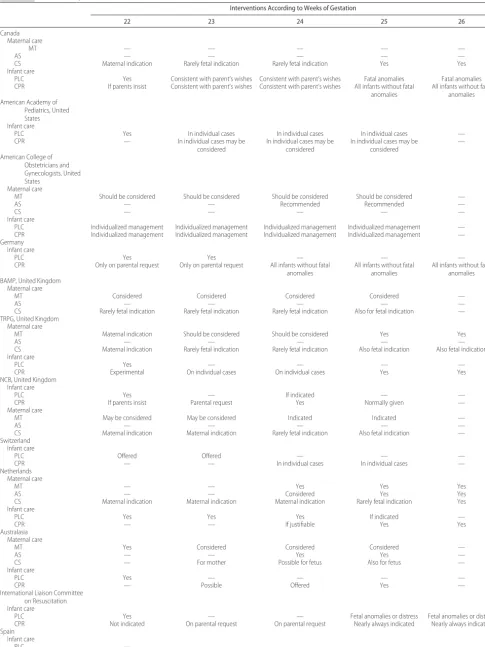
Guidelines for perinatal care at an extremely preterm gestational age have been formulated in different coun-tries over recent years. Fifteen documents were included in our study (Table 1). Practical aspects of care suggested in different countries are illustrated in Table 2.
The Canadian Paediatric Society and the Society of Obstetricians and Gynecologists of Canada emphasize15
the need for joint decision-making with fully informed parent and give detailed suggestions for information and the suitability of clinical audits of perinatal death and disability, including long-term outcome. Regular courses are recommended at hospitals in their catchment areas to inform the staff of advances in health care. The Amer-ican Academy of Pediatrics provides suggestions16 for
counseling but fails to give any specific recommenda-tions for treatment stratified on gestational age. How-ever, it does not recommend active intervention for infants under 23 weeks or with 400-g birth weight. The TABLE 1 Documents Taken Into Account
Country Title of the Document Year of
Publication
Scientific Society/Institute
Canada “Management of the Woman With Threatened Birth
of an Infant of Extremely Low Gestational Age”15
1994/2000 Fetus and Newborn Committee, Canadian Paediatric Society; Maternal-Fetal Medicine Committee, Society of Obstetricians and Gynaecologists of Canada United States “Perinatal Care at the Threshold of Viability”16 1995/2002 American Academy of Pediatrics
United States “Perinatal Care at the Threshold of Viability”17 1995/2002 American College of Obstetricians and Gynecologists Germany “Fru¨hgeburt an der Grenze der Lebensfa¨higkeit des
Kindes”18(the original is in German, translation by Dr Carola Ernst)
1998 Deutschen Gesellschaft fu¨r Gyna¨kologie und Geburtshilfe; Deutschen Gesellschaft fa¨r Kinderheilkunde und Jugendmedizin; Deutschen Gesellschaft fu¨r Perinatale Medizin und der Gesellschaft fu¨r Neonatologie und Pa¨diatrische Intensivmedizin
Singapore “Ethical Guidelines on Medical Treatment of High-Risk Infants”19
1998 National Medical Ethics Committee France “Dilemmes E´thiques de la Pe´riode Pe´rinatale:
Recommandations Pour le De´cisions de Fin de Vie”21
2000 Fe´de´ration Nationale des Pe´diatres Ne´onatologistes
United Kingdom “Fetuses and Newborn Infants at the Threshold of Viability: A Framework for Practice”22
2000 Gee H, Dunn P, for the British Association of Perinatal Medicine Executive Committee
United Kingdom “Guidelines Relating to the Birth of Extremely Immature Babies (22–26 Weeks Gestation)”23
2000 Thames Regional Perinatal Group United Kingdom “Critical Care Decisions in Fetal and Neonatal
Medicine: Ethical Issues”26
2006 Nuffield Council on Bioethics Switzerland “Recommendations for the Care of Infants Born at
the Limit of Viability (Gestational Age 22–26 Weeks)”27
2002 Swiss Society of Neonatology
International Association “Ethical Aspects in the Management of Newborn Infants at the Threshold of Viability”28
2003 International Federation of Gynecology and Obstetrics Committee for the Ethical Aspects of Human Reproduction and Women’s Health Netherlands “Guidelines for Treatment Decisions in Extremely
Premature Infants in the Netherlands”29,30(the original is in Dutch, translation by Dr Eduard Verhagen)
2005 Dutch Paediatric Society
Australasia “Provision of Care to Mother and Fetus/Newborn at the Threshold of Neonatal Viability (22–25 Weeks Completed Gestation): Clinical Practice Guidelines”31
2005 Women’s Hospitals Australasia
International Liaison Committee on Resuscitation
“Consensus on Science With Treatment Recommendations for Pediatric and Neonatal Patients: Neonatal Resuscitation”32
2005 International Liaison Committee on Resuscitation
TABLE 2 Practical Aspects of the Care of the Mother and Fetus/Neonate
Interventions According to Weeks of Gestation
22 23 24 25 26
Canada Maternal care
MT — — — — —
AS — — — — —
CS Maternal indication Rarely fetal indication Rarely fetal indication Yes Yes
Infant care
PLC Yes Consistent with parent’s wishes Consistent with parent’s wishes Fatal anomalies Fatal anomalies CPR If parents insist Consistent with parent’s wishes Consistent with parent’s wishes All infants without fatal
anomalies
All infants without fatal anomalies American Academy of
Pediatrics, United States Infant care
PLC Yes In individual cases In individual cases In individual cases —
CPR — In individual cases may be
considered
In individual cases may be considered
In individual cases may be considered
—
American College of Obstetricians and Gynecologists, United States
Maternal care
MT Should be considered Should be considered Should be considered Should be considered —
AS — — Recommended Recommended —
CS — — — — —
Infant care
PLC Individualized management Individualized management Individualized management Individualized management — CPR Individualized management Individualized management Individualized management Individualized management — Germany
Infant care
PLC Yes Yes — — —
CPR Only on parental request Only on parental request All infants without fatal anomalies
All infants without fatal anomalies
All infants without fatal anomalies BAMP, United Kingdom
Maternal care
MT Considered Considered Considered Considered —
AS — — — — —
CS Rarely fetal indication Rarely fetal indication Rarely fetal indication Also for fetal indication — TRPG, United Kingdom
Maternal care
MT Maternal indication Should be considered Should be considered Yes Yes
AS — — — — —
CS Maternal indication Rarely fetal indication Rarely fetal indication Also fetal indication Also fetal indication Infant care
PLC Yes — — — —
CPR Experimental On individual cases On individual cases Yes Yes
NCB, United Kingdom Infant care
PLC Yes — If indicated — —
CPR If parents insist Parental request Yes Normally given —
Maternal care
MT May be considered May be considered Indicated Indicated —
AS — — — — —
CS Maternal indication Maternal indication Rarely fetal indication Also fetal indication —
Switzerland Infant care
PLC Offered Offered — — —
CPR — — In individual cases In individual cases —
Netherlands Maternal care
MT — — Yes Yes Yes
AS — — Considered Yes Yes
CS Maternal indication Maternal indication Maternal indication Rarely fetal indication Yes
Infant care
PLC Yes Yes Yes If indicated —
CPR — — If justifiable Yes Yes
Australasia Maternal care
MT Yes Considered Considered Considered —
AS — — Yes Yes —
CS — For mother Possible for fetus Also for fetus —
Infant care
PLC Yes — — — —
CPR — Possible Offered Yes —
International Liaison Committee on Resuscitation Infant care
PLC Yes — — Fetal anomalies or distress Fetal anomalies or distress
CPR Not indicated On parental request On parental request Nearly always indicated Nearly always indicated Spain
Infant care
PLC —
CPR Not indicated
American College of Obstetricians and Gynecologists furnishes recommendations17split into levels concerning
counseling and treatment options: maternal transport to a tertiary center before delivery, an individualized treat-ment decision of the fetus/newborn, and a single course of corticosteroids between 24 and 34 weeks. In the Ger-man document,18 the principle outline states that “if
there is any chance, it is necessary to do everything to sustain survival,” and regardless of immaturity, every preterm neonate is a candidate for treatment. Below 22 weeks, compassionate care is indicated, although prena-tal assessment of gestational age must be confirmed after birth. The German doctors seem to prefer an individual approach as opposed to a statistical approach. In 1998, the National Bioethical Committee in Singapore pro-vided an ethical framework19outlining the definitions of
the treatment dilemma, the infant’s best interests, and the identification of high-risk infants including infants
⬍25 weeks of age. While failing to give specific recom-mendations, they consider it a medical duty, with the parents’ consent, to identify infants who could benefit from treatment: if there is good reason to treat, resusci-tation is mandatory, otherwise it should be withheld. Active termination of life is strictly prohibited. In the case of uncertain prognosis, provisional intensive care is indicated. Apart from the role of parents and the medical team, they also consider the role of medical ethics com-mittees to provide “ethical comfort” and legal protection for staff. The same concepts have recently been reviewed and analyzed20by one of the contributors to this
docu-ment. In 2000, the Federation Nationale des Pediatres Neonatologistes in France drew up general recommen-dations for perinatal end-of-life decisions21that provide a
framework helping caregivers to arrive at a humane, socially and ethically justifiable decision in the infant’s greatest interests while keeping the infant’s “quality of life” in mind. They consider the duties of doctors in-volved in the care of ill newborns, defining particular situations and relative ethical regulations, although they fail to give specific recommendations stratified according to gestational age. The limit of human viability is be-tween 22 and 24 weeks. Bebe-tween 24 to 26 weeks, sur-vival depends on numerous factors unique to each preg-nancy. Caring for neonates can mean withholding or withdrawing life-sustaining treatment and even arrest-ing life. The medical team is responsible for end-of-life decisions after arriving at a collegial agreement and speaking with the parents. The position of the parents seems to be different from the one assumed in other countries: doctors and parents have their own special roles in the care of the newborn, and parents do not ask to be decision-makers if they feel they can trust the doctor. The choice to withhold or withdraw medical treatment must be considered as a new medical decision, a new project for the child, and not simply the decision to do nothing. In the United Kingdom, the British Asso-ciation of Perinatal Medicine issued a number of practi-cal suggestions in 2000.22Neonates born between 22 and
28 weeks are within the viability limits, and counseling and involvement of the parents, interaction between senior perinatologists, and follow-up information are all
essential for their care. Emphasis is placed on planning and agreement between members of the perinatal team, communication, and the assessment of gestational age. In 2000, the Thames Regional Perinatal Group23
pro-posed a detailed management approach for infants be-tween 22 and 27 weeks. Resuscitation at ⱕ22 weeks should be considered experimental. In defining compas-sionate care, the Thames Regional Perinatal Group refers to the monograph of the Royal College of Pediatrics and Child Health,24 reviewed recently,25 where much
em-phasis is placed on palliative care. More recently in the United Kingdom, in 2006, the Nuffield Council on Bio-ethics proposed some week-by-week guidelines26 on
when to give intensive care to such infants. They con-sider the welfare of an infant inextricably linked with the ability of the parents to care for him or her; there-fore, the views of the parents are paramount. In the 3 documents from the United Kingdom, active termina-tion of life is not an acceptable choice. In 2002, the Swiss Society of Neonatology published recommendations for the care of infants born between 22 and 26 weeks.27Care
at ⬍24 weeks should generally be limited to palliative care. The administering of intensive care only if a high quality of life is possible could be regarded as discrimi-nation toward the disable. This problem is overcome with “the decision to withhold or withdraw therapies is motivated by the desire to protect the preterm infant from undue suffering and not by the wish to prevent survival with handicaps.”27Life support is continued as
long as there is reasonable hope of survival with an acceptable quality of life and if the burden of therapies is endurable for the infant. When this burden outweighs potential benefits, intensive care is no longer justified, and redirection of care to comfort measures could be acceptable. Active termination of life is strictly prohib-ited. With regard to the parents, the treatment decisions must be developed in an ongoing dialogue among all of the parties involved. The parents should not carry the full responsibility for the decision. The Swiss document also refers to health care resources in that economic considerations should never interfere with an individual case but must have their place at a society level and should refer not simply to economic costs but also to the emotional and physical burden of therapy. In 2003, the Committee for the Ethical Aspects of Human Reproduc-tion and Women’s Health of the InternaReproduc-tional Federa-tion of Gynaecologists and Obstetricians28 defined
in-fants between 22 and⬍28 weeks as having “threshold viability.” At this age, it is ethical to institute provisional intensive care at birth until attaining the clinical progress of the infant and consultation between an experienced staff member and the parents clarifies what is best for the child. The Dutch Pediatric Association guidelines, ap-proved in November 2005,29,30state that at 23 completed
and postnatal active treatment is recommended at 26 weeks.29,30Women’s Hospitals Australasia is a nonprofit
association that advocates the health care needs of women and infants in Australia and New Zealand. It represents many major women’s hospitals and health units throughout these countries. In their guidelines,31
they stress the information process, because they con-sider parental participation in planning and decision-making vital. At 240⁄7to 246⁄7weeks, medical support/
surgical support could be indicated. From 240⁄7to 256⁄7
weeks, the decision for surgical intervention should be addressed because of its implications for future pregnan-cies. Several recommendations are reaffirmed by the International Liaison Committee on Resuscitation32 in
the international guidelines on neonatal resuscitation. A “do-not-resuscitate” order is an evidence-based justified choice in a newborn of⬍23 weeks, 400 g, as well as with anencephaly and confirmed trisomy 13 and 18. With an uncertain or inaccurate diagnosis or prognosis, a thera-peutic trial with the option of subsequent withdrawal can be considered. In 2004, on reviewing the principles of resuscitation of the newborn,33 the Asociacion
Es-panola De Pediatria gives advice for the treatment of infants of an extreme gestational age, accepting the statement of the international guidelines mentioned above and published previously.
DISCUSSION
From an international point of view, there is the general agreement that atⱕ22 weeks there is no hope of sur-vival for the fetus/neonate. Week 220⁄7to 226⁄7is
con-sidered to be the cutoff of human viability: no scientific society recommends performing any kind of active treat-ment on the mother that is aimed at protecting the fetus or on the newborn except for offering compassionate care. A general agreement is also evident for week 250⁄7
to 256⁄7: antenatal steroids are recommended, prenatal
transport and cesarean section are also indicated to pro-tect the fetus, and resuscitation is offered to all infants without fatal anomalies. More caution is shown in Swit-zerland, where resuscitation is initiated on an individual basis, and also in the Netherlands, where cesarean sec-tion is rarely performed on fetal indicasec-tion and the op-tion for active treatment is subject to the consideraop-tion of the infant’s clinical conditions. On the other hand, in Australasia almost all infants of 240⁄7 weeks to 246⁄7
weeks are candidates for intensive care. From the re-viewed guidelines, it seems clear that 23 to 24 weeks are a sort of “gray zone,” where recommendations suggest resuscitation on an “individual basis” and “according to the parents’ wishes.” In some countries, this gray zone extends through 250⁄7to 256⁄7weeks. In all of the
state-ments, the gestational age is considered the best estimate of the infant’s maturation and, consequently, his or her possibility of survival, although many other fetal/neona-tal characteristics could play a role in the prognosis. In the case of uncertain gestational age, the guidelines rec-ommend a careful assessment of the infant’s condition at birth. In doubtful cases, resuscitation is appropriate until a further assessment of the infant’s clinical course clar-ifies the situation.19,23,24,28,29Although not influencing the
indications for care in terms of weeks of gestation,30the
modern concept of “provisional intensive care”19,28,29
re-mains a possibility, provided the parents understand the implications of aggressive treatment, and physicians are willing to withdraw ineffective or futile treatment if necessary. The concept of compassionate, comfort, or palliative care is strongly emphasized in the majority of the recommendations. All of the official guidelines in our research on perinatal care surrounding the threat of extremely preterm birth come from industrialized coun-tries, because we could not find any guidelines in devel-oping countries. This is not surprising considering the very high cost of intensive and long-term care for high-risk neonates and the ethical reasons that could lead to different treatment choices in different countries. An-other important issue regards how much the availability of such guidelines would affect the survival rate. Unfor-tunately, this availability may not automatically change the attitudes and behavior of physicians. Research is needed in these fields. From our study it is also evident that, despite being extremely useful, guidelines on this issue are intended as a general framework for helping health practitioners and parents in decision-making in the dramatic event of a threatened extremely preterm birth. Nevertheless, because of the uniqueness of every pregnancy and neonate, to protect mothers and infants from futile treatment, as well as incorrect withholding of life-sustaining treatment, the specific circumstances of every individual situation must always be kept in mind.
ACKNOWLEDGMENTS
We are greatly indebted to our colleagues who have provided information for our work: in Argentina, Nora Balanian, Gustavo Goldsmit, and Celia Lomuto; in Bel-gium, Dominique Haumont; in Denmark, Klaus Børch, Jesper Fenger-Gron, and Gorm Greisen; in Finland, Sture Andersson, Jukka Rajantie, and Outi Tammela; in France, Guy Putet; in Germany, Gabriele Olbrisch and Christian F. Poets; in Greece, Andreas Constantopoulos; in Hungary, Gyorgy Fekete; in Italy, Carola Hernst; in Norway, Thomas Moller and Ola Saugstad; in Singapore, Lai-Yun Ho; in Switzerland, Thomas M. Berger; in the Netherlands, Arend Bos; and in the United Kingdom, Philip Steer. We also give special thanks to Dr Eduard Verhagen for suggestions for the preparation of the ar-ticle and to Susan Cadby for her revision of the English-language aspects of the article.
REFERENCES
1. Costeloe K, Hennessy E, Gibson AT, Marlow N, Wilkinson AR. The EPICure study: outcomes to discharge from hospital for infants born at the threshold of viability.Pediatrics.2000;106: 659 – 671
2. Wood NS, Marlow N, Costeloe K, Gibson AT, Wilkinson AR. Neurologic and developmental disability after extremely pre-term birth.N Engl J Med.2000;343:378 –384
3. Marlow N, Wolke D, Bracewell M, Samara M. Neurologic and developmental disability at six years of age after extremely preterm birth.N Engl J Med.2005;352:9 –17
5. Larroque B, Breart G, Kaminski M, et al. Survival of very preterm infants: Epipage, a population based cohort study.Arch Dis Child Fetal Neonatal Ed.2004;89:F139 –F144
6. Markestad T, Kaaresen PI, Ronnestad A, et al. Early death, morbidity, and need of treatment among extremely premature infants.Pediatrics.2005;115:1289 –1298
7. Serenius F, Ewald U, Farooqi A, Holmgren PA, Hakansson S, Sedin G. Short-term outcome after active perinatal manage-ment at 23–25 weeks of gestation: a study from two Swedish tertiary care centers. Part 2: infant survival.Acta Paediatr.2004; 93:1081–1089
8. Rutter N. The extremely preterm infant. BJOG. 1995;102: 682– 687
9. Hack M, Fanaroff A. Outcome of children of extremely low birthweight and gestational age in the 1990s.Semin Neonatol.
2000;5:89 –106
10. Levene M. Is intensive care for extremely immature babies justified?Acta Paediatr.2004;93:149 –152
11. Field MJ, Logh MJ.Clinical Practice Guidelines: Directions for a New Program. Washington, DC: National Academy Press; 1990 12. Cluzeau F, Little Johns P, Grimshaw J, Feder G, Moran S. Development and application of a generic methodology to assess the quality of clinical guidelines.Int J Qual Health Care.
1999;11:21–28
13. Steinbrook R. Searching for the right search: reaching the medical literature.N Engl J Med.2006;354:4 –7
14. World Health Organization. International Classification of Dis-eases. 10th Revision. Vol 1. Geneva, Switzerland: World Health Organization; 1992
15. Fetus and Newborn Committee, Canadian Paediatric Society, Maternal-Fetal Medicine Committee, Society of Obstetricians and Gynaecologists of Canada. Management of the woman with threatened birth of an infant of extremely low gestational age. CMAJ. 1994;151:547–553. Available at: www.cps.ca/ english/statements/FN/fn94-01.htm. Accessed March 9, 2005 16. MacDonald H; American Academy of Pediatrics, Committee on
Fetus and Newborn. Perinatal care at the threshold of viability.
Pediatrics.2002;110:1024 –1027
17. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 38: perinatal care at the threshold of viability.Obstet Gynecol2002;100:617– 624
18. Pohlandt F. Premature delivery in borderline viability of the infant: a recommendation of the German Society of Gynecol-ogy and Obstetrics, the German Society of Pediatrics and Ad-olescent Medicine, the German Society of Perinatal Medicine and the Society of Neonatology and Pediatric Intensive Care Medicine [in German]. Z Geburtshilfe Neonatol. 1998;202: 261–263
19. National Medical Ethics Committee. Ethical guidelines on medical treatment of high-risk infants. Available at: www. moh.gov.sg/mohcorp/publicationsreports.aspx?id⫽2406. Ac-cessed November 11, 2007
20. Ho LY. Perinatal care at the threshold of viability: from prin-ciples to practice.Ann Acad Med Singapore.2003;32:362–375 21. Dehan M, Gold F, Grassin M, et al. Ethical dilemmas in the
perinatal period: guidelines for end-of-life decisions [in French].Arch Pediatr.2001;8:407– 419
22. Gee H, Dunn P; BAPM Executive Committee. Fetuses and newborn infants at the threshold of viability: a framework for practice. 2000. Available at: www.bapm.org/media/documents/ publications/threshold.pdf. Accessed October 10, 2005
23. Thames Regional Perinatal Group. Guidelines relating to the birth of extremely immature babies. Available at: www.bapm.org/ media/documents/publications/immature.pdf. Accessed October 10, 2005
24. Royal College of Pediatrics and Child Health.Withholding and Withdrawing Life Saving Treatment in Children: A Framework for Practice. London, United Kingdom: Royal College of Paediatrics and Child Health; 1997
25. Royal College of Paediatrics and Child Health. Withholding and withdrawing life sustaining treatment in children: a frame-work for practice. May 2004. Available at: www.rcpch.ac.uk. Accessed September 29, 2006
26. Nuffield Council on Bioethics. Critical care decisions in fetal and neonatal medicine: ethical issues. Available at: www. nuffieldbioethics.org/go/screen/ourwork/neonatal/publication㛭406. html. Accessed December 14, 2006
27. Swiss Society of Neonatology. Guidelines: care of infants born at the limit of viability (22 to 26 weeks of gestation). Available at: www.neonet.ch/assets/doc/Infants㛭born㛭at㛭the㛭limit㛭of㛭viability㛭-㛭 english㛭final.pdf. Accessed September 20, 2006
28. FIGO, Committee for the Ethical Aspects of Human Reproduc-tion and Women’s Health. RecommendaReproduc-tions on ethical issues in obstetrics and gynaecology: ethical aspects in the manage-ment of newborn infants at the threshold of viability. Novem-ber 2003. Available at: www.figo.org/about_guidelines.asp. Accessed November 11, 2007
29. Rijken M, Veen S, Walther FJ. Ethics of maintaining extremely preterm infants.Paediatr Child Health. 2007;17:58 – 63 30. Verloove-Vanhorick SP. Management of the neonate at the
limits of viability: the Dutch viewpoint.BJOG.2006;133(suppl 3):13–16
31. Women’s Hospitals Australasia Clinical Practice Guidelines. Provision of care to mother and fetus/newborn at the threshold of neonatal viability (22–25 weeks completed gestation). Avail-able at: www.wcha.asn.au/index.cfm/spid/1㛭47.cfm. Accessed October 10, 2006
32. International Liaison Committee on Resuscitation. The Inter-national Liaison Committee on Resuscitation (ILCOR) consen-sus on science with treatment recommendations for pediatric and neonatal patients: neonatal resuscitation.Pediatrics.2006; 117(5). Available at: www.pediatrics.org/cgi/content/full/117/ 5/e978
33. Grupo de Reanimacion Cardiopulmonar de la Sociedad Es-panola de Neonatologia. Recommendations in neonatal resus-citation [in Spanish].An Pediatr (Barc).2004;60:65–74 34. Desfrere L, Tsatsaris V, Sanchez L, Cabrol D, Moriette G.
Ex-tremely preterm infants: resuscitation criteria in the delivery room and dialogue with parents before birth [in French].J Gynecol Obstet Biol Reprod (Paris).2004;33(suppl 1):S84 –S87 35. Walther FJ. Withholding treatment, withdrawing treatment,
DOI: 10.1542/peds.2007-0513
2008;121;e193
Pediatrics
Maria Serenella Pignotti and Gianpaolo Donzelli
Practical Guidelines for the Treatment of Extremely Preterm Births
Perinatal Care at the Threshold of Viability: An International Comparison of
Services
Updated Information &
http://pediatrics.aappublications.org/content/121/1/e193 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/121/1/e193#BIBL This article cites 23 articles, 6 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/standard_of_care_sub Standard of Care
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2007-0513
2008;121;e193
Pediatrics
Maria Serenella Pignotti and Gianpaolo Donzelli
Practical Guidelines for the Treatment of Extremely Preterm Births
Perinatal Care at the Threshold of Viability: An International Comparison of
http://pediatrics.aappublications.org/content/121/1/e193
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.