M E E T I N G A B S T R A C T S
Open Access
ESICM LIVES 2017
30th ESICM Annual Congress. September 23-27, 2017
Published: 20 September 2017
Oral Sessions Monday, 25 September
2017
Acute respiratory failure and MV experimental
studies
0001
Comparison of three methods to measure lung compliance during a decremental PEEP trial in an experimental model of ARDS J.-C. Richard1, B. Louis2, C. Guérin1,2
1
Hopital de la Croix Rousse, Lyon, France;2IMRB INSERM 955, Créteil, France
Correspondence:J.-C. Richard
Intensive Care Medicine Experimental2017,5(Suppl 2):0001
INTRODUCTION.Optimal PEEP is still a matter of debate in ARDS pa-tients. PEEP is by nature an expiratory setting aiming at maintaining lung recruitment reached during the breathing cycle and/or during a recruitment manoeuver. Decremental PEEP trial after a recruitment manoeuver is an attractive method to detect optimal PEEP. This latter can be defined from different variables, lung compliance being one of them.
OBJECTIVES. To compare three methods to measure lung compli-ance and to find out which is associated with the optimal PEEP (max-imal compliance) during a decremental PEEP trial.
METHODS. Female piglets were anesthetized, paralyzed, tracheoto-mized and mechanically ventilated (Carestation, GE Healthcare) and acute lung injury was performed by saline lavage. Once PaO2 was lower than 100 mmHg under 100% FIO2, a recruitment manoeuver (sustained inflation to 40 cm H2O for 30 seconds) was performed followed by cycling mechanical ventilation in volume controlled mode, constant flow inflation, 100% FIO2, tidal volume 6 ml/kg body weight, respiratory rate 35 breaths/min. PEEP was initially set to 20 cmH2O then decreased by 2 cmH2O-steps lasting 2 minutes each to 2 cmH2O. At each PEEP step, airway pressure, esophageal pressure and airflow were acquired (Biopac 100), whole lung CT scan was per-formed during end-expiratory and end-inspiratory pause, and finally electrical impedance tomography (EIT) (Göttingen University) signal was acquired. Compliance was inferred using three methods: i) by fit-ting a R-C model on recorded pressure and flow signals using a least square method (Clung). ii) by using CT data (Cscan) as ratio of tidal vol-ume (sum of the difference between inspiration and expiration in volume of normally aerated, poorly aerated and overaerated lung compartments) to driving pressure (plateau pressure minus PEEP). iii) by computing ratio of change in electrical impedance to driving pressure (CEIT). The relationships between Clung, Cscanand CEITwere performed by using the coefficients of determination over the 10 PEEP steps in each pig.
RESULTS.Thirteen pigs were analyzed. The table shows for each pig the values of coefficient of determination between each pair of com-pliance and the resulting optimal PEEP that maximized comcom-pliance. CONCLUSIONS.Excellent correlation, except for pig B, was observed between Clung and Cscan and the resulting optimal PEEP were in agreement with a difference generally less than 2 cmH2O. Poor cor-relation (r2≤ 0.8) between CEITand Cscanwas observed in 4 pigs. Nevertheless, even iIn these cases the difference between optimal
PEEP computed from CEITand the two other methods were small (≤2 cmH2O).
REFERENCE(S)
Measurement of Clung, which is easy to manage in adults, strongly correlated to Cscanand should be used to titrate optimal PEEP in dec-remental PEEP trial. By contrast measurement of CEIT, which is the only method possible in neonates, seems less correlated to Cscan.
0002
Effect of external negative pressure versus positive end-expiratory pressure on respiratory mechanics during recruitment of
experimentally induced lung injury
A. Nestorowicz1, A. Fijalkowska-Nestorowicz2, J. Glapinski3, J. Wosko4 1
Medical University Lublin, Anaesthesiology and Intensive Therapy, Lublin, Poland;2Medical University Lublin, Anaesthesiological and Intensive Care Nursing, Lublin, Poland;3Wroclaw University of Science and Technology, Chair of Electronic and Photonic Metrology, Wroclaw, Poland;4University Hospital No 4, Anaesthesiology and Intensive Therapy, Lublin, Poland
Correspondence:A. Nestorowicz
Intensive Care Medicine Experimental2017,5(Suppl 2):0002
INTRODUCTION. Positive end-expiratory pressure (PEEP) improves gas exchange and respiratory mechanics in patients suffering from acute lung injury. However, it itself may also induce the risk of lung overdistension and their damage. Some data suggest that the use of external negative pressure (eNP) in damaged lungs is less injurious compared to positive pressure ventilation [1].
OBJECTIVES.To compare the effect of eNP versus PEEP on lung me-chanics in pigs with acute lung injury.
METHODS.Ten Large White pigs weighting 52 ± 5 kg were included in the study. Under general anaesthesia the animals were intubated and ventilation in a volume-controlled mode with FIO21.0, VT 8– 10 mL kg−1 and I:E ratio 1:2. Respiratory rate was adjusted to Table 1 (Abstract 0001)See text for description
maintain PaCO2 wthin 35–45 mm Hg. A continuous infusion of
Ringer´s lactate at the rate of 5–10 mL kg−1h−1was administered
throughout the study.
The acute lung injury was produced by repeated bronchoalveolar lavage using warm 0.9% NaCl until PaO2/FIO2 remainded stable
below 100. Thereafter, each animal was secured in a whole body size-chamber and endotracheal PEEP followed by eNP were created, while lung ventilation mode was held unchanged. Peak airway pres-sure (Pawpeak), airway resistance (R) and dynamic compliance (Cdyn)
were recorded before lung injury and after - at 0, 4, 8, 12, 16 cm H2O
of positive and negative pressure, respectively.
RESULTS.There were no significant differences in Cdyn and R when
either PEEP or eNP was applied. However, PEEP resulted in increase whereas eNP in decrease of Pawpeak and the obtained results
dif-fered significantly at the negative vs positive pressure of 12 and 16 cm H2O. Both mode of lung recruitment resulted in a spectacular
in-crease of oxygenation (Fig. 1).
CONCLUSIONS.This results demonstrate that both modes of lung
re-cruitment constitutes similar profile of respiratory mechanics, but eNP decrease whereas PEEP increase Pawpeak.
REFERENCE(S)
1. Grasso F. et al.: Am J Respir Crit Care 2008; 177: 412–18. GRANT ACKNOWLEDGMENT
NCN 2013/11/B/ST7/01173
0003
Dynamic changes on pulmonary artery flow caused by mechanical ventilation. Cyclic worsening of pulmonary artery function in acute respiratory distress syndrome
A. Santos1,2, M.I. Monge-García3, J.B. Borges1, E. Gomez-Peñalver4, J. Retamal5, L. Lucchetta6, G. Hedenstierna7, A. Larsson1, F. Suarez-Sipmann1
1
Uppsala University, Hedenstierna Laboratory. Surgical Sciences Department, Uppsala, Sweden;2CIBER de Enfermedades Respiratorias (CIBERES), Madrid, Spain;3Hospital SAS Jerez, Intensive Care Unit, Jerez de la Frontera, Spain;4Hospital General de Villalba, Villalba, Spain;5Pontificia Universidad Católica de Chile, Departamento de Medicina Intensiva, Santiago, Chile;6San Mateo Hospital, Pavia, Italy; 7
Uppsala University, Department of Medical Sciences. Clinical Physiology, Uppsala, Sweden
Correspondence:A. Santos
Intensive Care Medicine Experimental2017,5(Suppl 2):0003
INTRODUCTION. Mechanical ventilation (MV) induces cyclic
changes in RV preload and afterload. However, evaluation of MV
effects on RV and pulmonary circulation during the respiratory cycle and how these effects change after acute respiratory dis-tress syndrome (ARDS) is not well known.
OBJECTIVES.To evaluate the cyclic effects of MV on RV and
pul-monary artery function in a porcine model of ARDS.
METHODS.Continuous flow waveform analysis was applied beat
by beat during a period of three minutes in 10 mechanically ventilated pigs before and after a model of ARDS. The model was created by means of lung saline lavages followed by two hours of injurious MV. Applied analysis was based on the de-scribed effect of MV on RV stroke volume (SV) (Fig. 2), mainly attributed to preload modification. However, also variables re-lated with vascular function can be cyclically affected by MV (Fig. 3). We hypothesized that changes in RV and pulmonary ar-tery function are also related with the SV changes and that this relationship is affected by ARDS. To test this hypothesis, slope and correlation (r2) between variables related with vascular and
ventricle function and SV were calculated along the respiratory cycle (Fig. 4). Studied variables were pulmonary artery acceler-ation time (PAAT, time to reach maximum flow normalized to the ejection time, which is inversely related with pulmonary vas-cular resistance), flow amplitude (maximum - minimum flow), and the maximum flow to the time to reach maximum flow ra-tio (Qmax/Qmaxt), which has been described as a contractility index. Flow signal was obtained from a sensor placed around the main pulmonary artery.
RESULTS.After creation of ARDS, mean SV decreased (39 ± 12 ml
vs 30 ± 6 ml, p = 0.014) and its coefficient of variation increased (0.08 ± 0.03 vs 0.10 ± 0.03, p = 0.016), compared to baseline. Slopes between flow amplitude and SV (0.19 ± 0.05 vs 0.24 ± 0.09, p = 0.027), and between Qmax/Qmaxt and SV (1.6 ± 1.12 vs 2.9 ± 1.4, p = 0.008), as well as the correlation be-tween PAAT and SV (0.21 ± 0.21 vs 0.54 ± 0.28, p = 0.012) and between Qmax/Qmaxt and SV (0.37 ± 0.21 vs 0.61 ± 0.26, p = 0.026) increased during ARDS. A non-significant trend to in-crease in the correlation between flow amplitude and SV (0.73 ± 0.30 vs 0.86 ± 0.14, p = 0.050) and to a decrease in the slope between PAAT and SV (−0.004 ± 0.005 vs −0.006 ± 0.004, p = 0.325) was observed during ARDS.
CONCLUSIONS. ARDS modified the hemodynamic effects of MV
on RV and pulmonary vascular function: changes in SV during a respiratory cycle were more affected by pulmonary vascular function and RV contractility. These preliminary results could help to understand the tidal effects of MV on RV and pulmonary artery function.
Fig. 1 (abstract 0002)Respiratory mechanics and oxygenation
Fig. 2 (abstract 0003)See text for description
0004
Effects of prone positioning and ultra-low tidal volume on transpulmonary driving pressure in a porcine model of ards
F. Pino1,2, G. Scaramuzzo3, L. Ball1, M. Pinol Ribas4, J.B. Borges2,5, G. Hedenstierna6, A. Larsson2, C. Guerin7, P. Pelosi1, G. Perchiazzi2,8 1University of Genoa, Dep. of Surgical Sciences and Integrated
Diagnostics, Genova, Italy,2Hedenstierna Laboratory, Dep. of Surgical Science. Uppsala University, Uppsala, Sweden,3University of Ferrara, Ferrara, Italy,4Hospital La Fe, Valencia, Spain,5Hospital das Clínicas, Universidade de São Paulo, Sao Paulo, Brazil,6Hedenstierna Laboratory, Dep. of Medical Science. Uppsala University, Uppsala, Sweden,7Hopital de la Croix Rousse, Lyon, France,8Bari University, Bari, Italy
Correspondence:F. Pino
Intensive Care Medicine Experimental2017,5(Suppl 2):0004
INTRODUCTION.In ARDS patients:
1) prone positioning can reduce mortality, and
2) respiratory system driving pressure is associated with outcome. Therefore, a reduction in transpulmonary driving pressure (DPL) could
minimise ventilator-induced lung injury, yielding improved outcome in prone position.
OBJECTIVES.To test the effects of prone positioning on DPLduring
protective and ultra-low tidal volume (VT) ventilation. We
hypothe-sized that prone positioning can reduce DPLduring mechanical
ven-tilation at both VTsizes.
METHODS.We used a previously described two-hit porcine model of
ARDS, comprising saline lavage followed by injurious mechanical ventilation. After lung injury, pigs were ventilated in volume-controlled mode, VT 6 mL/kg and positive end-expiratory pressure
(PEEP) and FIO2titrated according to the ARDSnet table (PEEPARDSnet).
A decremental PEEP trial was performed from 20 cmH2O to 5 cmH2O
in supine and prone position at VTof 6 mL/kg and 3 mL/kg,
identify-ing the PEEP level with the lowest DPL(PEEPBDP). Each animal was
al-located, by random sequence and in crossover with a latin square design, to eight treatments: 6 and 3 mL/kg VT at constant minute
ventilation, with PEEPBDPor PEEPARDSnet,in prone and supine
pos-ition. Each change in ventilation settings was preceded by a recruit-ment manoeuvre[GC1].The primary endpoint was DPL, and secondary
endpoints included gas-exchange and PEEPBDP.
RESULTS.We analysed data from 8 pigs (32 ± 2 kg); after injury
PaO2/FIO2ratio was 136 ± 22 mmHg. DPLwas lower in prone than
supine position at both 6 mL/kg (3.7 ± 1.8 vs. 5.2 ± 1.1 cmH2O,
p= 0.006) and 3 mL/kg (1.6 ± 0.9 vs. 2.6 ± 0.6 cmH2O,p= 0.002)
VT. PEEPBDPwas also lower in prone than supine position: 10.3 ± 1.0
vs. 13.3 ± 3.0 cmH2O (p = 0.02) at 6 mL/kg and 10.4 ± 1.4 vs.
12.8 ± 2.1 cmH2O (p= 0.03) at 3 mL/kg. In prone and supine
posi-tions, PaO2was 266 ± 63 vs. 234 ± 62 mmHg (p= 0.17) at 6 mL/kg
and 219 ± 65 vs. 154 ± 39 cmH2O (p= 0.06) at 3 mL/kg,
respect-ively; PaCO2was 68 ± 10 vs. 68 ± 17 cmH2O (p= 0.99) at 6 mL/kg
and 90 ± 22 vs. 87 ± 24 cmH2O (p= 0.66) at 3 mL/kg, respectively.
CONCLUSIONS. In our ARDS animal model, prone positioning
allowed a reduction of DPLand PEEP level with the lowest DPL
dur-ing both protective and ultra-low VTventilation.
0005
Abnormal diaphragm fibers in patients undergoing mechanical ventilation: a pilot study
J. Marin-Corral1, I. Dot1, M. Boguñà1, C. Vilà1, A. Castellví1, S. Pascual-Guardia2, M.P. Gracia1, A. Zapatero1, Y. Díaz1, L. Cechini3, J.R. Masclans1,4
1Hospital del Mar-Parc de Salut Mar, GREPAC (Grupo de Investigación en
Patología Crítica), Institut Mar d'Investigaciones Médicas (IMIM), Critical Care Department, Barcelona, Spain;2Hospital del Mar-Parc de Salut Mar, Institut Mar d'Investigaciones Médicas (IMIM), Respiratory Department, Barcelona, Spain;3Hospital del Mar-Parc de Salut Mar, Urology Department, Barcelona, Spain;4Pompeu Fabra University (UPF), Barcelona, Spain
Correspondence:J. Marin-Corral
Intensive Care Medicine Experimental2017,5(Suppl 2):0005
INTRODUCTION. Several studies are concordant with animal
models of ventilator-induced diaphragm dysfunction (VIDD) in demonstrating ultrastructural injury and atrophy of diaphragmatic fibers, increased oxidative stress, activation of major proteolytic pathways and mitochondrial dysfunction, which are significantly correlated with mechanical ventilation (MV) duration. Area frac-tions of normal and abnormal diaphragm in patients undergoing MV have not been yet assessed.
OBJECTIVES.To assess and compare area fractions of normal and
ab-normal diaphragm and limb muscles of brain-dead organ donors (BD), type III Maastricht donors (MS), and stable patients who re-ceived mechanical ventilation during thoracic surgery (CT).
METHODS.Prospective and observational study in a polyvalent
Spanish ICU. All organ donors admitted in the ICU during 6 months (BD or MS) were included. There was a control group with patients undergoing resection of a suspected early lung malignancy. Demographic and temporary variables, comorbidi-ties, severity on admission and treatment were evaluated. Dia-phragm biopsy specimens were obtained from the anterior costal diaphragm lateral to the insertion of the phrenic nerve and limb muscle from the vastus lateralis as internal control. Muscle samples were fixed and paraffin embedded and they were cut and stained with hematoxylin and eosin (H&E). Quanti-tative evaluation of normal and abnormal (internal nucleus, in-flammatory cells, lipofuscin, abnormal viable and inflammed/ necrotic) muscle fibers in sections were done following previous methodologies. Differences between groups were assessed using chi-square for categorical variables and Student's t-test or Mann–Whitney test for continuous variables. We considered p < 0.05 to be significant.
RESULTS.Fifteen patients were included of which 5(33%) were CT,
4(27%) were BD and 6(40%) MS. There were no differences between groups in age, sex, BMI, and comorbidities. BD patients presented a lower number of hours of mechanical ventilation with a higher proportion of controlled modalities than MS [63hrs(33–92) vs 216hrs(107–396);p = 0.010 and 33%(0–46) vs 5%(0–20);p = 0.128]. Diaphragm of BD presented higher percentage of abnormal muscle fibers than MS donors [19.1%(9.2) vs 2.4(2.3);p = 0.024] and CT sub-jects [19.1%(9.2) vs 4.5(1.1);p = 0.036]. Diaphragm of BD had lower percentage of internal nucleus [0%(0) vs 2.4%(1.0);p = 0.036] and MS diaphragms showed lower percentage of inflammatory cells [0%(0) vs 0.4%(0.1);p = 0.004] both compared to CT subjects. No differences were found in limb muscles evaluation of normal/abnormal fibers be-tween different groups.
CONCLUSIONS. Diaphragm of BD donors presents an impaired
number of abnormal fibers. Although MS donors are undergone mechanical ventilation during more hours their percentage of ab-normal diaphragm fibers don't differ from CT subjects. It could be related with the ability of these patients to realise spontan-eous breathing efforts.
Insight into the pathophysiology of sepsis
0006
Characterization of metabolic signatures associated with early response to supportive therapy in patients with septic shock
A. Cambiaghi1, B. Bollen Pinto2, L. Brunelli3, F. Falcetta3, A. Federico1, K. Bendjelid2, R. Pastorelli3, M. Ferrario1
1
Politecnico di Milano, Dipartimento di Elettronica, Informazione e Bioingegneria (DEIB), Milan, Italy;2Geneva University Hospitals, Anaesthesia, Pharmacology and Intensive Care, Geneva, Switzerland; 3Istituto di Ricerche Farmacologiche Mario Negri, Milan, Italy
Correspondence:B. Bollen Pinto
Intensive Care Medicine Experimental2017,5(Suppl 2):0006
INTRODUCTION.Elucidation of early metabolic signatures associated
with the progression of septic shock and responsiveness to support-ive therapy could be useful in the development of a new therapeutic strategies.
OBJECTIVES.The primary aim of this study was to verify whether a
different response to therapy was associated with a particular trajec-tory in metabolite patterns.
METHODS. We examined the plasma metabolome of 21 septic
shock patients (pts) enrolled in the Shockomics clinical trial (NCT02141607). Responsiveness to therapy was assessed as change in organ dysfunction assessed by SOFA score, measured at ad-mission (T1, acute phase) and 48 hours after (T2, post-resuscitation). A patient was judged as non-responder if both SOFAT2 was >8 and Δ = SOFAT1- SOFAT2 < 5 (NR, 7 pts); the
remaining as responsive (R, 14 pts). We combined untargeted and targeted mass spectrometry-based metabolomics strategies to cover as much as possible the plasma metabolites repertoire. Firstly, a mass metabolic profiling, performed by direct flow injection-TOF-MS, was applied as untargeted screening. After-wards, we performed a targeted analysis using a mass spectrometry-based quantitative approach with the Biocrates plat-form coupled to Triple-Quad 5500 LC-MS/MS system, which allowed to measure specific metabolic classes and the magnitude of their variation. We built classification models to predict non-responsiveness to therapy based on sets of metabolites. Explora-tive analyses by probabilistic graphical models - i.e. Markov Net-work (MN) - were also performed.
RESULTS. At ICU admission, plasma metabolome was similar
between R and NR. In univariate analysis, NR presented less vari-ation in metabolite concentrvari-ation between T1 and T2. Different classification models using targeted metabolomics to predict NR status reproducibly reveled the presence of phosphatidylcholines (PCs) (e.g. lysoPC), alanine and Kynurenine (a metabolite of trypto-phan). We combined untargeted metabolomics with those metabo-lites, and the set of features selected from the integrated models was consistent in showing the importance of PCs and alanine. All models had good performance (AUC > 0.9). The MNs showed that the two groups were characterized by different dependencies among metabolites, and the main differences were represented by PCs, kynurenine and alanine.
CONCLUSIONS. These findings support the emerging evidence
that lipidome alteration plays an important role in response to in-fection. In addition, the identification of alanine as a consistent marker of NR to therapy could represent a possible shift in glu-cose‐alanine cycle in the liver thus providing a more detailed characterization of liver dysfunction than clinically available tests. These results were strengthened by the explorative analyses per-formed by MNs suggesting that lipid species and alanine are im-portant regulatory nodes.
GRANT ACKNOWLEDGMENT
This research is supported by the FP7 Health Programme (602706).
0007
Immune evasion mechanism ofE. colias a target for sepsis
treatment
M.D.T. Correia1, F.P. da Silva1, S.K. Ariga1
1Faculdade de Medicina da Universidade de São Paulo, Laboratory of
Medical Investigation - LIM 51, São Paulo, Brazil
Correspondence:M.D.T. Correia
Intensive Care Medicine Experimental2017,5(Suppl 2):0007
INTRODUCTION. Bacteria have evolved sophisticated strategies to
evade immune defense mechanisms. Since our group discovered that Escherichia coli binds in an opsonin-independent manner to FcγRIII receptor (CD16) to escape immune system, we have sought to identify the protein sequence from such bacteria that is able to mimic IgG1. Using a Phage Display Technique, we
re-cently identified and characterized a peptide of E. coliwhich is a ligand to CD16.
The peptide, called wzxe, is a translocase involved in the transbilayer movement of an trisaccharide-lipid (Lipid III) intermediate in the as-sembly of Enterobacterial Common Antigen (ECA). Peptide-receptor interactions induced CD16-mediated immunoreceptor ITAMi signal-ing, blocking the production of reactive species of oxygen(ROS) and bacterial killing. This CD16-mediated inhibitory signaling was abro-gated in a wzxe−/−mutant ofE. coliK12 restoring production of ROS and bacterial killing2.
OBJECTIVES.To evaluate the role ofE. colipeptide wzxe in a murine
sepsis model of bacterial injection.
METHODS.Two group of 20 males mice C57Bl/6, at 10 weeks of age,
were submitted to injection of 3 x 108E. coliK12 wild type or the
same amount ofE coliwzxe−/−mutant. Survival was observed during 96 hours then the mice were sacrificed for cytokines analysis. TNF alpha, IL-1beta, IL-6, MCP-1 and IL-10 were quantified by ELISA. In addition, control mice injected with saline were sacrificed in the 4th
day for cytokine dosing.
RESULTS.A higher mortality and increased production of cytokines
were observed in the group of mice injected withE. coliK12 wild type.
The Kaplan-Meier and log-rank methods were used to analyze mor-tality. Cytokine values were compared using the Mann–Whitney U-test. Differences were considered significant when P was < 0.05. All statistical analysis was performed using Prism 6.0 (GraphPad Soft-ware, USA).
CONCLUSIONS. In an era of growing resistance to antibiotics,
pre-venting bacteria innate immune evasion could be a good approach to control infections. RegardingE. coli, peptide wzxe apparently plays an important role during sepsis, being an interesting therapeutic tar-get to be explored.
REFERENCE(S).
1. Pinheiro da Silva F, Aloulou M, Skurnik D, Benhamou M, Andre-mont A, Velasco IT, et al. CD16 promotes Escherichia coli sepsis through an FcR gamma inhibitory pathway that prevents phagocyt-osis and facilitates inflammation. Nat Med. 2007;13(11):1368–74. 2. Beppler J, Mkaddem S Ben, Michaloski J, Honorato RV, Velasco IT, de Oliveira PSL, et al. Negative regulation of bacterial killing and inflammation by two novel CD16 ligands. Eur J Immunol. 2016;46(8):1926–35.
GRANT ACKNOWLEDGMENT
0008
Oxidant/antioxidant status of adult and pediatric ICU patients: a key role for sepsis and mortality
M. Miliaraki1, T. Tavladaki2, A.-M. Spanaki2, H. Dimitriou3, S. Ilia2, K. Vardas4, E. Briassouli5, E. Michalakakou6, T. Karakonstantakis6, E. Kondili7, I. Papasotiriou6, P. Papadopoulos8, A. Pistiki8, D. Georgopoulos7, G. Briassoulis2
1University of Crete, Medical School, Pediatric Intensive Care Unit,
Heraklion, Crete, Greece;2University of Crete, Medical School, Heraklion, Greece, Pediatric Intensive Care Unit, Heraklion, Crete, Greece;3University of Crete, Medical School, Heraklion, Greece, Pediatric Hamatology Oncology, Heraklion, Crete, Greece;4National and Kapodistrian University of Athens, First Critical Care Department, Athens, Greece;5National and Kapodistrian University of Athens, First Department of Internal Medicine - Propaedeutic, Athens, Greece;6National and Kapodistrian University of Athens, Biochemical Department, Children's Hospital 'Aghia Sophia', Athens, Greece;7University of Crete, Medical School, Heraklion, Greece, Adult Intensive Care Unit, Heraklion, Crete, Greece;8National and Kapodistrian University of Athens, 2nd ICU and 4th Internal Medicine Department, Athens, Greece
Correspondence:M. Miliaraki
Intensive Care Medicine Experimental2017,5(Suppl 2):0008
INTRODUCTION. Sepsis is a major health problem and much
em-phasis has recently been placed on the role of redox imbalance, oxi-dative stress, chaperone heat shock proteins (HSP) 72, 90, and interleukin 27 (IL-27), in intensive care unit (ICU) patients' clinical course and outcome. Oxidative/antioxidative screening methods might assist the clinicians in discriminating critically ill septic patients, or at risk of death, from those with systemic inflammatory response syndrome (SIRS), and facilitate therapeutic decision-making upon ad-mission of a patient.
OBJECTIVES. The present study seeks to ascertain whether the
ex-pected increased risk of mortality might be further determined by the presence of oxidant/antioxidant imbalance and altered IL-27 (a regulator T-cells having both pro and anti-inflammatory effects), Zn, glutamine, and HSP levels in septic ICU and pediatric ICU (PICU) pa-tients, compared to SIRS and healthy controls.
METHODS.This prospective observational study was performed in a
sample of critically ill adult (n = 180) and pediatric patients (n = 44) with sepsis or SIRS, compared to healthy controls (n = 116). Serum total oxidant status (TOS) and total antioxidant capacity (TAC) were measured on day 1 in ICU, using photometric test systems. Plasma glutamine (chromatography), serum zinc (Zn-Photometry), IL-27 (Elisa kits) and HSPs (Elisa and flow cytometry) were also analyzed. Clinical severity scores APACHE II and SOFA were calculated and ICU mortal-ity was recorded.
RESULTS.A total of 180 adult ICU patients were included in the study.
Mean APACHE II score was 22.5 ± 8 and ICU mortality rate 30.8% (PICU 4,3%). Septic patients had lower TAC, but higher TOS, glutamine, IL-6, IL-10, HSP72 and HSP90 levels, compared to SIRS and control individ-uals (p < 0.05). TOS was negatively related to TAS (r = 0.5, p < 0.05). Serum TOS correlated positively (p < 0.05) and TAS negatively (p < 0.05) with Zn, IL-27, HSP72/90 and clinical severity scores. For pdicting sepsis among critically ill patients, TAC and TOS achieved a re-ceiver operating characteristic curve (AUROC) >0.90 (95% CI 0,85-0,97, p < 0.05). In predicting mortality, TOS, IL-27, and Zn achieved an AUROC >0.68 (95% CI 0,50-0,85, p < 0.05). A pilot study of 44 pediatric patients showed the same trend of oxidant/antioxidant imbalance and lower Zn and glutamine levels in septic children (p < 0.05).
CONCLUSIONS.Oxidant/antioxidant status is significantly impaired in
septic patients compared to SIRS. Decreased antioxidant defense and increased oxidative stress system, along with alterations in innate im-mune system integrity and IL-27, may play an important role in sepsis-related mortality.
GRANT ACKNOWLEDGMENT
This research has been co-financed by the European Union (European Social Fund- ESF) and Greek national funds through the Operational Program ´´Education and Lifelong Learning´´ of the National Strategic Reference Framework (NSRF)- Research Funding Program: THALES.
0009 Withdrawn
0010
Mitochondrial dysfunction in a tissue slice model of septic acute kidney injury is caused by oxidative stress
S.J. Pollen, M. Singer
UCL, Bloomsbury Institute of Intensive Care Medicine, London, United Kingdom
Correspondence:S.J. Pollen
Intensive Care Medicine Experimental2017,5(Suppl 2):0010
INTRODUCTION.Mitochondrial modulation of cellular bioenergetics
is increasingly viewed as an explanation for the apparent paradox between clinical/biochemical acute kidney injury (AKI) that occurs during sepsis, despite a relative lack of cell death, maintenance of adequate tissue oxygenation and recovery of organ function.1
Previous in vitro studies from our lab show that exposing naïve kidney tissue to septic serum, thereby removing any haemodynamic influences, produces mitochondrial dysfunction.2
Fig. 6 (abstract 0007).Mice survival curves after bacterial injection
Fig. 7 (abstract 0007).Production of cytokines
OBJECTIVES. To determine if the mitochondrial dysfunction that occurs following exposure to septic serum is driven by the observed increase in reactive oxygen species (ROS), and, if so, whether these changes can be inhibited and/or reversed using a targeted mito-chondrial ROS scavenger.
METHODS.Live naïve kidney slices (200μm thick) were exposed to
serum from 24-hour sham operated or septic rats and imaged with a confocal microscope using fluorescent dyes to detect dynamic changes in mitochondrial function. Mitochondrial membrane poten-tial (MMP), ROS generation and redox state (NADH) were all probed over a 90-minute time course. In separate studies, septic (and sham) serum exposed slices were co-incubated with the mitochondrial ROS scavenger MitoTEMPO, either at time zero or as a delayed (50 min) treatment.
RESULTS.The decreases in MMP and NADH, and the increase in
ROS seen following exposure to septic serum were prevented by co-incubation with MitoTEMPO from time zero (Fig. 8).
Treating septic serum-exposed slices with MitoTEMPO at 50 min could partly reverse changes in mitochondrial function that had already begun, and prevent further progression (Fig. 9).
CONCLUSIONS.Ourin vitrofindings suggest that increased
produc-tion of mitochondrial ROS is a direct cause of mitochondrial dysfunc-tion in septic AKI, independent of circulatory changes, and this can be protected/reversed by ROS scavenging. Targeting mitochondrial ROS may provide therapeutic benefit.
REFERENCES
1 Singer, M. The role of mitochondrial dysfunction in sepsis-induced multi-organ failure. Virulence 5, 66–72, doi:10.4161/ viru.26907 (2014).
2 Pollen, S., Arulkumaran, N. & Singer, M. Septic serum alters mito-chondrial function in a kidney slice model of septic acute kidney in-jury. Intensive Care Medicine Experimental 4, A144, doi:10.1186/ s40635-016-0098-x (2016).
GRANT ACKNOWLEDGMENT
UCL Medical School MBPhD Programme, Astor Foundation and Inten-sive Care Society
Microcirculation and fluid responsiveness
0011
Influence of the different fluid on the vascular endothelial barrier permeability and glycocalyx layer in a rats model of the acute normovolemic hemodilution
B. Ergin1,2, P. Guerci3, Z. Uz1, Y. Ince1, C. Ince1,2
1Academic Medical Center, University of Amsterdam, Department of
Translational Physiology, Amsterdam, Netherlands;2Erasmus MC University Hospital, Department of Intensive Care, Rotterdam, Netherlands;3University Hospital of Nancy, Department of Anesthesiology and Critical Care Medicine, Nancy, France
Correspondence:B. Ergin
Intensive Care Medicine Experimental2017,5(Suppl 2):0011
INTRODUCTION.Intravenous fluid administration is the most
per-formed action in patients undergoing surgery. Hemodilution can be either intentional with the aim of limiting allogenic blood transfusions in elective surgery or used for correction of volume status of the patient. It has been suggested that colloidal solu-tions may preserve glycocalyx components, by maintaining the shear stress on endothelial due to an higher viscosity, osmotic pressure and also to the presence of macromolecules. We sought to evaluate the impact of hemodilution with either a balanced colloid, a balanced crystalloid or a normal saline solution on the glycocalyx components and the vascular barrier permeability.
MATERIAL AND METHODS. Experiments were conducted in 24
fully instrumented, mechanically ventilated and anesthetized rats. Acute normovolemic hemodilution (ANH) was induced by step-wise exchange of blood with the plasma expander according to the following ratio; 1:1 with balanced hydroxyethyl starch (HES 130/0.4), 1:3 with balanced crystalloid or normal saline 0.9%, untill targeted hematocrit (Hct) levels of Hct 30%, Hct 25%, Hct 20% and Hct 15% were achieved. An hand-held in vivo micro-scope, CytoCam was placed on the surface of the exposed biceps femoris. Plasma concentration-time curves of Dextran 40kD-Texas red, Albumin-Alexa 680 and Dextran 500kd-FITC were fitted for each experiment separately with a monoexponential function in order to assess both endothelial barrier function and plasma vol-ume. At the end of the experiment, the heart, brain, kidney, lung and liver were harvested to determine their water content using Fig. 8 (abstract 0010).See text for description
the wet/dry weighing technique. Hyaluronan, syndecan-1, and heparan sulfate as indirect makers of glycocalyx degradation were measured by the ELISA in plasma samples.
RESULTS. MAP significantly decreased during the hemodilution
process (p < 0.05) whereas CVP and femoral arterial blood flow (fABF) were maintained. At 15% of hematocrit, lactate levels in-creased significantly (p < 0.01), accompanied by changes in pH and bicarbonate levels for balanced crystalloid and normal saline groups (p < 0.01). Syndecan-1 levels were increased in all groups at the end of the experiment compared to baseline values re-spectively (p < 0.0001). Heparan sulfate increased only in saline group at the different hemodilution thresholds (p < 0.01) only in the normal saline group. Hyaluronan levels were increased in bal-anced crystalloid and normal saline groups compared to control (p < 0.01).
No significant alteration in power of the exponential decay-time of dyes were observed between the different fluid groups. Neither was any alteration in the microcirculation nor the presence of tissue edema measured.
CONCLUSION.ANH per se may jeopardize the endothelial
glyco-calyx layer without inducing significant alterations in vascular barrier permeability regardless of the fluid composition. Normal saline appears to be the most unsuitable fluid for use for hemodilution.
0012
Influence of fluid challenge administration rate on endothelial glycocalyx and major macrohemodynamic variables in surgical and septic patients
J. Pouska1,2, V. Tegl1,2, V. Cerny3,4,5, J. Benes1,2,6
1Fakultní Nemocnice Plzeň, Klinika Anesteziologie, Resuscitace a
Intenzivní Medicíny, Plzen, Czech Republic;2Lékařská Fakulta v Plzni, Univerzita Karlova, Klinika Anesteziologie, Resuscitace a Intenzivní Medicíny, Plzen, Czech Republic;3Fakultní Nemocnice Hradec Králové, Klinika Anesteziologie, Resuscitace a Intenzivní Medicíny, Hradec Kralove, Czech Republic;4Lékařská Fakulta v Hradci Králové, Univerzita Karlova v Praze, Hradec Kralove, Czech Republic;5Univerzita J. E. Purkyně, Masarykova Nemocnice Ústí Nad Labem, Klinika Anesteziologie, Perioperační a Intenzivní Medicíny, Usti nad Labem, Czech Republic; 6
Biomedicínské Centrum Lékařské Fakulty v Plzni, Univerzita Karlova, Plzen, Czech Republic
Correspondence:J. Pouska
Intensive Care Medicine Experimental2017,5(Suppl 2):0012
INTRODUCTION. Fluid challenge (FC) is test of cardiac preload
re-serve, but how FC is performed varies widely. Slow FC may decrease the hemodynamic effect and contrary fast FC may lead to temporary hypervolemia. Hypervolemia harms endothelial glycocalyx (EG), and hence the rate of FC may significantly alter FC macro- and microhe-modynamic effects.
OBJECTIVES.Major objectives of this study was to assess the influence
of fast and slow FC administration on hemodynamic variables and EG.
METHODS.Randomized prospective study performed in a University
hospital was approved by the local ethics committee. Patients under-going major spinal surgery (group A) and critically ill with septic shock (group B) in whom a FC was indicated were randomly (1:1 randomization by predefined scheme) assigned to receive either fast (5-10min) or slow (20-30min) 500ml balanced crystalloid FC. In group A only one FC per patient was performed, in group B more FC were allowed if response to previous FC was positive. Intraoperatively pre-load reserve and volume effect was assessed using standard hemodynamic variables and pleth-variability index (PVI). In septic patients the PiCCO2 device was used for hemodynamic monitoring. Effect on EG was assessed using the intravital microscopy of sublin-gual circulation using the Glycocheck software (Glycocheck BV, Netherlands). Hemodynamic (PVI, stroke volume - SV) as well as EG variables (PBR - perfused boundary region and CD - capillary density) were monitored before (T0), immediately after (T1), and in 20 mi-nutes intervals till the end of surgery (T2-4, group A) or after 1 and 2 hours (T2-3, group B). Microcirculatory parameters were assessed as absolute and relative change to baseline (%BL).
RESULTS.In 50 patients of group A 50 FC (25 fast and 25 slow) were
performed; 26 FC in 15 patients (12 fast and 14 slow) of group B. All but 6 FC (12%) were positive in group A, whereas 13 (50%) were posi-tive in group B equally distributed with 7 (54%) posiposi-tive in fast and 6 (46%) in slow FC. In group A both fast and slow FC increased CD (T1 CD %BL 104 ± 5% and 109 ± 4%), but the effect vanished rapidly in the slow FC (T2 CD%BL 112 ± 16% vs. 96 ± 19%; p = 0.02). Similar effect was observed on PBR - post FC increment (T1 PBR %BL 104 ± 19% vs. 108 ± 16%) with significantly prolonged effect in the fast FC (T3 PBR%BL 109 ± 16% vs. 99 ± 15%; p = 0.04). In group B, rate of infusion Fig. 10 (abstract 0011).No significant alteration in power of the
exponential decay-time of dyes were observed between the different fluid groups.
Fig. 11 (abstract 0011).Neither was any alteration in the microcirculation nor the presence of tissue edema measured.
have neither impact on PBR nor CD. Contrary, significantly higher PBR (1.9 ± 0.2 vs. 2.1 ± 0.3; p = 0.02) and lower CD (0.7 ± 0.1 vs. 0.6 ± 0.1; p = 0.02) values were observed in responders in T1.
CONCLUSIONS.In our study a fast 500ml balanced crystalloid FC had
prolonged microcirculatory and hemodynamic effects in surgical pa-tients than slow FC. In papa-tients with septic shock no changes in terms of EG were observed.
GRANT ACKNOWLEDGMENT
Supported by Ministry of Health of the Czech Republic, grant nr. 15-31881A.
0013
Glycocalyx degradation is independent of vascular barrier dysfunction in non-traumatic hemorrhagic shock
P. Guerci1,2,3, B. Ergin1, Z. Uz1, Y. Ince1, M. Heger4, C. Ince1 1
Academic Medical Center, University of Amsterdam, Department of Translational Physiology, Amsterdam, Netherlands;2Centre Hospitalier Universitaire de Nancy, Anesthesiology and Intensive Care Medicine, Nancy, France;3University of Lorraine, Nancy, France;4Academic Medical Center, University of Amsterdam, Department of Experimental Surgery, Amsterdam, Netherlands
Correspondence:P. Guerci
Intensive Care Medicine Experimental2017,5(Suppl 2):0013
INTRODUCTION.Glycocalyx shedding following traumatic hemorrhagic
or septic shock has been linked to increased vascular barrier per-meability (VBP) (1). Little is known regarding the VBP during non-traumatic hemorrhagic shock (NTHS). It is not yet elucidated whether or not there is positive correlation between the fluid resuscitation-mediated glycocalyx degradation and an increased VBP (2,3). It would be suggested that a colloidal solution would better preserve glycocalyx components, by maintaining the shear stress on endothelial due to an higher viscosity, osmotic pressure and also to the presence of macromolecules.
OBJECTIVES.The aim of this study was to determine the effects
of different resuscitation fluids on the glycocalyx barrier and its relation with the VBP in short term of severe hemorrhage.
METHODS. Fully instrumented and hemodynamically monitored
Wistar albino rats were subjected to a pressure-controlled NTHS for 60 min. Same spot of the microcirculatory unit of the biceps femoris muscle was monitored continuously with hand-held microscope. Rats were then fluid resuscitated with either Ringer's acetate or balanced starch solution or NaCl 0.9% till the MAP reaches 80 mmHg. Glycocalyx shed products (hyaluronan, syndecan-1, heparan) were determined at baseline and 60 min after fluid resuscitation by ELISA methods. VBP was assessed with 3 different techniques: plasma decay of 3 fluorescent dyes (Texas Red-40 KDa and FITC-500 kDa Dextrans and Alexa 680–70 kDa Albumin), tissue edema (wet/dry weight ratio) and intravital fluorescence microscopy.
RESULTS.NTHS and associated fluid resuscitation produced
signifi-cant amount of glycocalyx shed products (P< 0.05) partially damp-ened by the use of balanced colloid. Despite glycocalyx degradation and microcirculatory functional density alterations (P < 0.05) we did not show an increase in VBP regardless of the technique used (plasma decay of fluorescent dyes,).
CONCLUSIONS. In NTHS, even though microcirculation was
re-stored, fluid resuscitation was not associated with increased VBP despite the presence of glycocalyx degradation. This result chal-lenges the role of the glycocalyx as a significant contributor to VBP. Each fluid used has a different impact on the glycocalyx.
REFERENCE(S)
1. Kottke MA. Shock 2016; 46:20–36
2. Torres Filho IP. Am J Physiol Heart Circ Physiol 2016; 310:H1468–78
3. Weinbaum S. Annu Rev Biomed Eng 2007; 9:121–67 GRANT ACKNOWLEDGMENT
Dr Guerci was supported by a grant from the French Society of Anesthesiology and Intensive Care Medicine (SFAR).
Fig. 13 (abstract 0013).See text for description
0014
Limitations of using grid-based point-of-care assessment for scoring microcirculatory alterations
Y. Ince1,2, H. He2,3, G. Guven2,4, E. Boerma1,5, C. Ince1,2 1
Academic Medical Center, University of Amsterdam, Department of Translational Physiology, Amsterdam, Netherlands;2Erasmus MC-University Medical Center, Department of Intensive Care, Rotterdam, Netherlands;3Peking Union Medical College Hospital, Peking Union Medical College, Beijing, China;4Ankara University Faculty of Medicine, Department of Intensive Care, Internal Medicine, Ankara, Turkey; 5
Medical Centre Leeuwarden, Department of Intensive Care, Leeuwarden, Netherlands
Correspondence:Y. Ince
Intensive Care Medicine Experimental2017,5(Suppl 2):0014
INTRODUCTION.The semi-quantitative score method introduced by
Boerma and co-workers for measuring microcirculatory flow index (MFI) has been commonly used to evalute the microcirculatory alterations in critically ill patients using hand-held vital microscopes [1] and sugg-gested as use for point-of-care assessment [2].MFI is based on scoring a representative vessel in one of four quadrants of the field of view (FOV) and calculating the mean value over the four quadrants. There remains uncertainty, however, about the reliability of the numerical value ob-tained from this grid-based scoring system.
OBJECTIVES.The aim of this study was to determine if this MFIquadrants
would differ significantly from the MFI per vesselscore based on the
measurement of every vessel in the FOV.
METHODS.MFIquadrantsis the mean flow score for the four quadrants
of a representative vessel scored in each quadrant. MFIper vesselis the
mean flow scores measured for each vessel in the entire FOV (Fig. 16). Flow values are scored as 0 no flow, 1 (intermitent flow), 2 sluggish flow, 3 continuous flow [1]. The total vessel density (TVD), perfused ves-sel density (PVD), and percentage of perfused vesves-sel (PVD) was also cal-culated and compared. 126 videos of skeletal muscle from 24 rats in shock and resuscitation were analyzed to measure the relationship be-tween the MFIquadrantand MFIper vessel.
RESULTS.The MFIquadrantswas 2.29 + 0.74 (range from 0.5 to 3), and MFI-per vesselwas 2.13 + 0.74, range (0.17 to 3). A Bland-Altman plot showed
the mean difference between MFIquadrantsand MFIper vesselwas−0.16,
and limits of agreement (bias ± 1.96SD) is from 0.95 to−0.64 (Fig. 17).
Moreover, the absolute value of variation between MFIquadrantsand MFI-per vessel was significantly correlated with PPV (P < 0.001), PVD
(P = 0.002), MFIper vessel(P < 0.0001), but not with MFIquadrants(P = 0.085)
and TVD (P = 0.134). The PPV (ROC area 0.81) was the best predictor of a 15% difference between MFIquadrantsand MFIper vessel, significantly better
than PVD (ROC area 0.71), TVD(ROC area 0.6) (Fig. 18).
For predicting an 15% difference between MFIquadrantsand MFIper vessel,
a PPV threshold of 71% was identified with a sensitivity of 42% and a specificity of 95%.
CONCLUSIONS. Quantative values of the MFI based on quadrants
should be used with caution under conditions of low PPV (<71%). This finding is of importance if MFI values are to be used as thresholds for clinical decision making for point-of-care use at the bedside.
REFERENCE(S)
1. Boerma EC, Mathura KR, van der Voort PH, Spronk PE, Ince C: Quantify-ing bedside-derived imagQuantify-ing of microcirculatory abnormalities in septic patients: a prospective validation study. Crit Care 2005, 9: R601-R606. 2. De Backer D, Hollenberg S, Boerma C, Goedhart P, Büchele G, Ospina-Tascon G, Dobbe I, Ince C: How to evaluate the microcircula-tion: report of a round table conference. Crit Care 2007, 11:R101.
Fig. 16 (abstract 0014).See text for description
Fig. 15 (abstract 0013).See text for description
0015
The assessment of fluid responsiveness in undifferentiated shock using corrected flow time measured by Doppler ultrasound of carotid artery after passive leg raise maneuver
I. Barjaktarevic1, S. Hu2, S. Chang1, E. Aquije Montoya3, R. Buhr1, W. Toppen4, S. Ong3, T. Wang1, A. Chiem3, D. Berlin5, P. Paull4, A. Maller1, T. Rezayat6 1
David Geffen School of Medicine at UCLA, Pulmonary and Critical Care Medicine, Los Angeles, United States;2David Geffen School of Medicine at UCLA, Division on Pulmonary and Critical Care Medicine, Los Angeles, United States;3David Geffen School of Medicine at UCLA, Los Angeles, United States;4David Geffen School of Medicine at UCLA, Department of Medicine, Los Angeles, United States;5Weil Cornell University, Pulmonary and Critical Care Medicine, New York, United States;6David Grant Medical Center, Pulmonary and Critical Care, Travis, United States
Correspondence:I. Barjaktarevic
Intensive Care Medicine Experimental2017,5(Suppl 2):0015
INTRODUCTION.Adequate assessment of fluid responsiveness in
un-differentiated shock has substantial impact on patient outcomes. Sys-tolic flow time (FT) corrected for heart rate can be used to follow change in left ventricular preload. Recent data1,2suggests its possible value in predicting fluid responsiveness when combined with pre-load challenge maneuvers such as passive leg raise (PLR).
OBJECTIVES.Evaluation of PLR-induced change in carotid corrected
FT (ccFT) as a predictor of fluid responsiveness in patients with undif-ferentiated shock.
METHODS. Prospective, non-interventional study included patients
with newly diagnosed undifferentiated shock. Eligible subjects were adult patients with shock duration < 24 hours, resuscitated with >30cc/ kg of intravenous fluids who had no history of significant cardiovascular disease or contraindications to perform PLR. Subjects were evaluated with point-of care (POC) Doppler ultrasound (Logiq e, GE Healthcare, Wauwatosa, WI) imaging of carotid artery and with stroke volume (SV) assessment via non-invasive cardiac output monitoring system (NICOM, Cheetah Medical) before and after PLR maneuver. ccFT was calculated based on Doppler waveform analysis, andΔccFT was presented in milli-seconds (msec) or percent-change (%ΔccFT), Fig. 19. Fluid
responsive-ness was defined as >10%ΔSV as per NICOM protocol.
RESULTS.Presented is preliminary analysis of the first 70 patients. All patients required vasopressor support, with 40 patients (57.1%) being
on mechanical ventilation. Average length of stay prior to shock onset was 0.6 days, average age of patients 60.9 years with 51.4% of cohort being female,Table 2. Average cardiac index improved significantly with PLR from 3.75 to 4.24L/min/m2 with an averageΔSV 23.7 ± 23.0%, Table3. Average ccFT at baseline was 314.0 ± 37.2msec and was in-creased after PLR to an average 324.0 ± 43.8msec with an average increase of 10.9 ± 23.0msec in ΔccFT or 3.6 ± 7.6% change in %ΔccFT. The majority of patients, 49 (70.0%), were fluid responders based on ΔSV. Fluid responders had higher average ΔccFT 17.7 ± 23.6 msec compared to non-responders,ΔccFT−4.7 ± 10.7msec (p = 0.000047). ROC curve analysis demonstrated slight improvement ofΔccFT (AUC = 0.873 [95% CI: 0.86-0.88]) in comparison to%ΔccFT
(AUC = 0.860 [95% CI: 0.85-0.87]), Fig. 20. Using a ΔccFT cutoff of 9 msec, the test has positive predictive value of 95% with sensitivity 73% and specificity 90%, Table 4.
CONCLUSIONS.POC assessment of ccFT can be simple and broadly
available test that, combined with PLR maneuver, may offer ability to predict fluid responsiveness in undifferentiated shock.
REFERENCE(S)
1) Blehar et al.Correlation of corrected FT in the carotid artery with changes in intravascular volume status.J Crit Care.2014
2) Lafanechere et al.Changes in aortic blood flow induced by PLR predict fluid responsiveness in critically ill patients.Crit Care.2006 GRANT ACKNOWLEDGMENT
This study has been financially supported by GE Healthcare Fig. 18 (abstract 0014).See text for description
Fig. 19 (abstract 0015).See text for description
Table 2 (Abstract 0015).See text for description
Parameter Value
Number of patients enrolled, N 70
Sex (percent female subjects) 51.4
Age (years) 60.9
Heart rate, N (±SD) 89.1 (±19.5)
Baseline mean arterial pressure, mmHg (±SD) 70.6 (±11.4)
Vasopressor use, N (%) 70 (100)
Mechanical ventilation, N (%) Passively ventilated, N (%) -Positive end-expiratory pressure (PEEP) >5mmH2O, N (%)
40 (57.1) - 19 (27.1) - 16 (22.9)
Lactate at enrollment, mg/dl 34.2
Therapy and prognosis of acute brain injury
0016
Acute magnetic resonance imaging predicts neurocognitive outcome after aneurysmal subarachnoid haemorrhage
M. J. Rowland1,2, P. Garry1,2, M. Ezra1,2, R. Corkill2, I. Baker2, J. Westbrook2, G. Douaud1, K. T. Pattinson1,2
1
University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom;2Oxford University Hospitals NHS Foundation Trust, Neurosciences Intensive Care Unit, Oxford, United Kingdom
Correspondence:M. J. Rowland
Intensive Care Medicine Experimental2017,5(Suppl 2):0016
INTRODUCTION.Aneurysmal subarachnoid haemorrhage (SAH) is a
devastating disease often leading to death or poor functional out-comes. Damage to the brain in the first 72 hours following aneurysm rupture ("early brain injury") is likely to play a key role in determining the incidence of morbidity and mortality after SAH. Acute MRI scan-ning may offer greater insight into early brain injury and help de-velop novel diagnostic and therapeutic biomarkers.
OBJECTIVES. To detect and quantify the impact of SAH on brain
measurements of T1-structural and diffusion-weighted (DWI) MRI from the first 72 hours to 3 months post-SAH, and to correlate these with subsequent neurocognitive outcomes.
METHODS.27 patients with "good grade”SAH (World Federation of
Neurosurgeons Grade I and II) underwent T1-weighted structural and DWI MRI scanning at 3 time-points post-SAH: < 72 hours, 5–10 days and 3 months post-SAH. Patient MRI data was assessed longitudinally as well as being compared with data from age/gender-matched healthy controls. Patients underwent detailed assessment at 3 months post-SAH to quantify neurocognitive outcomes.
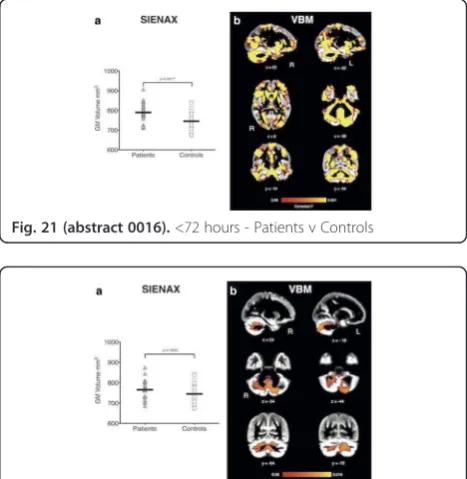
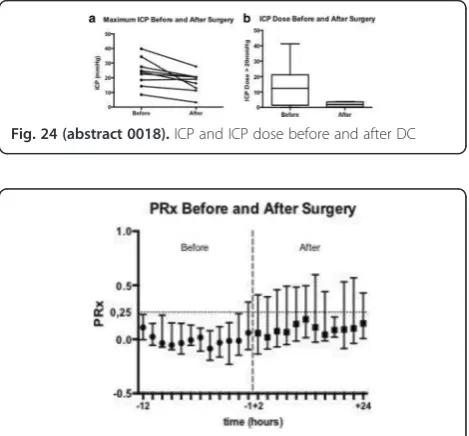
RESULTS.There was a significant global increase in grey matter (GM)
volume measured from T1-weighted MRI in the first 72 hours post-SAH compared with healthy controls (Fig. 21). These changes were associated with restricted diffusion, suggesting widespread cytotoxic cerebral oedema resulting in this apparent increase of GM volume. By 3 months, structural changes had resolved, except for higher GM volume in pa-tients compared with healthy controls in cognitive zones of the cerebel-lum (Crus I & II, and lobule VIIb–Fig. 22). This increase was negatively correlated with neurocognitive performance (r = 0.389, p = 0.006 Pear-son's correlation). Retrospectively, patients with subsequent neurocogni-tive impairment at 3 months already showed higher GM volume at < 72 hours post-SAH in the same cognitive cerebellar regions compared with patients who did not develop cognitive impairment (Fig. 23). Notably, cerebellar GM measure during the acute phase made it possible to pre-dict with 84% sensitivity and 86% specificity those patients who went on to develop poor neurocognitive outcomes post-SAH.
CONCLUSIONS.Structural and diffusion-weighted MRI are highly
sensi-tive to the global as well as regional impact of cerebral oedema that occurs acutely following aneurysm rupture and is often undiagnosed. Results from this study also demonstrate the crucial role of cerebellar injury in modulating neurocognitive outcomes after“good grade”SAH. Using an automated approach, a simple T1-weighted structural MRI scan in the first 72 hours post-SAH can predict subsequent neurocogni-tive outcome with high accuracy. Damage to the cerebellum acutely post-SAH may therefore underlie neurocognitive impairment after SAH and act as a therapeutic and diagnostic marker of early brain injury. Grant Acknowledgement
MRC (UK) Table 3 (Abstract 0015).See text for description
Parameter Baseline Value Post PLR challenge
NICOM cardiac index, L/min/m2 3.75 4.24
NICOM SV, ml (±SD) 62.1 (±24.5) 74.9 (31.4)
NICOMΔSV, % ±SD 23.7 (±23.0)
Fluid responsive, N (%) - NICOM ΔSV, % ±SD
49 (70) - 32.5 (21.8)
Fluid nonresponsive, N (%) - NICOM ΔSV, % ±SD
21 (30) - 3.1 (7.0)
Systolic time at baseline, msec (±SD) 263.92 (42.84) 272.70 (46.35)
Corrected FT at baseline, msec (±SD) 314.03 (37.23) 324.02 (43.78)
ΔccFT msec (±SD) and Percent ΔccFT, % (±SD)
10.94 (22.96) and 3.6 (7.6)
ΔccFT, fluid responsive vs. fluid non-responsive, msec (±SD)
17.65 (23.6) vs. -4.72 (10.68), p-value= 0.000047
Fig. 20 (abstract 0015).See text for description
Table 4 (Abstract 0015).See text for description ΔccFT
(msec)
Sensitivity Specificity Positive predictive value (PPV)
Negative predictive value (NPV)
1 0.88 0.70 0.88 0.70
3 0.84 0.70 0.88 0.64
5 0.78 0.80 0.91 0.64
9 0.73 0.90 0.95 0.56
11 0.65 0.95 0.97 0.51
13 0.61 0.95 0.97 0.49
15 0.51 0.95 0.96 0.44
17 0.51 0.95 0.96 0.42
19 0.43 1.00 1.00 0.41
Fig. 22 (abstract 0016).3 months - Patients v Controls
0017
Hypothermia to control intracranial pressure following traumatic brain injury is associated with significant differences in outcomes, management and physiology: results of additional data collection from the Eurotherm3235 trial
J. K. Rhodes1, I. Puddu2, F. S. Taccone3, M. van der Jagt4, A. Rodriguez5, C. Battison5, L. Sinclair5, P. Andrews1
1
University of Edinburgh/NHS Lothian, Edinburgh, United Kingdom, 2University of Turin/S. Giovanni Battista-Molinette Hospital, Turnin, Italy, 3
Université Libre de Bruxelles/Hôpital Erasme, Brussels, Belgium, 4Erasmus MC-University Medical Center, Rotterdam, Netherlands, 5
University of Edinburgh, Edinburgh, United Kingdom
Correspondence:J.K. Rhodes
Intensive Care Medicine Experimental2017,5(Suppl 2):0017
INTRODUCTION.The Eurotherm3235 trial [1] was a high quality
ran-domised controlled trial assessing the efficacy of therapeutic hypothermia, 32-35°C, (TH) to control intracranial pressure (ICP) fol-lowing traumatic brain injury (TBI) verses standard care (Control (CG)). TH was associated with increased mortality at 6 months. To better understand this result study centres collected additional data retrospectively.
METHODS.Additional data, including the patients' background,
man-agement and physiology in the 7 days following randomisation, was collected from medical notes, 24 hour charts and hospital informa-tion systems between January and July 2016. This was collated into a secure database and analysed. Data are given as number (%) or mean daily values (standard deviation) for TH vs. CG.
RESULTS.286 anonymised forms were received from 33 of 47
cen-tres (74% of the trial population). 143 patients received TH and 143 were in the CG. Mortality at 6 months was significantly increased with TH (46 vs. 32 deaths, Hazard ratio 1.624 CI 1.025 - 2.573, p = 0.039). The cause of death may have differed between the groups, with an excess of TH patients dying with multi-organ failure, systemic inflammation or acute lung injury (15 (35.7%) vs. 5 (19.2%)). The numbers receiving Midazolam (96.0(12.8) vs. 78.7(16.0), p = 0.046), Alfentanil (37.1(4.7) vs. 27.7(5.2), p = 0.004, Atracurium (31.1(6.8) vs. 22.0(4.5), p = 0.012) were significantly greater with TH. TH was associated with increased numbers receiving Vasopressin (5.7(2.4) vs. 1.9(0.9), p = 0.002) and Dobutamine (7.3(3.1) vs. 2.3(1.0), p = 0.002). The number of patients with a metabolic acidosis (45(36.9%) vs. 27(22.1%), p = 0.017) and receiving bicarbonate (17(13.7%) vs. 5(4.2%), p = 0.018) was greater with TH. Serum lactate was also greater (1.20(0.10) vs. 1.06(0.11) mmol/l, p = 0.027). Further-more, the number of patients receiving steroids was greater with TH (23(17.8%) vs. 9(6.7%), p = 0.01). Small but significant effects of TH on leucocytes (9.9(0.9) vs. 11.0(0.7) 10^9/l, p = 0.031), neutrophils (7.8(0.6) vs 9.0(0.7) 10^9/l, p = 0.005) and activated partial thrombo-plastin time (33.2(2.1) vs. 31.2(1.3) s, p = 0.046) were also found.
CONCLUSIONS.This post-hoc explorative study found significant
be-tween groups differences in outcome, management and physiology associated with TH. In light of Eurotherm3235´s principle finding that TH was associated with harm, these differences, which have previ-ously been regarded as simple consequences of TH, could have pathological significance. Correcting for these differences in future studies of TH could be important.
REFERENCE(S)
1. Andrews, P.J., et al.,Hypothermia for Intracranial Hypertension after Traumatic Brain Injury.N Engl J Med, 2015. 373(25): p. 2403–12. GRANT ACKNOWLEDGMENT
Supported by the National Institute for Health Research Health Tech-nology Assessment program, which funded the main phase of the study. The European Society of Intensive Care Medicine funded the pilot phase.
0018
Decompressive craniectomy after traumatic brain injury and brain monitoring
A. V. Ferreira1, J. Silva2, E. Monteiro3, A. Cerejo4, C. Dias3 1
Hospital Pedro Hispano, Matosinhos, Portugal;2Centro Hospitalar de Gaia, Neurosurgery, Gaia, Portugal;3Centro Hospitalar São João, Intensive Care, Porto, Portugal;4Centro Hospitalar São João, Neurosurgery, Porto, Portugal
Correspondence:A. V. Ferreira
Intensive Care Medicine Experimental2017,5(Suppl 2):0018
INTRODUCTION.Decompressive craniectomy (DC) is largely used as
treatment for refractory intracranial hypertension after traumatic brain injury (TBI). DC decision and its impact on clinical evolution has still unresolved controversies mainly regarding timing of intervention, patient selection and post-operative management.
OBJECTIVES. To characterize the before and after periods of DC
using multimodal brain monitoring.
METHODS.We retrospectivaly studied 9 TBI patients, admitted to
the Neurocritical Care Unit (NCCU) at Hospital São João, Porto that were submitted to primary or secondary DC and had brain monitor-ing durmonitor-ing 12 hours before and 24 hours after surgery. At NCCU, TBI patients admitted are managed with an autoregulation-oriented CPP protocol. Variables analyzed were Intracranial Pressure (ICP), ICP dose over 20 mmHg (ICPd > 20), Cerebral Perfusion Pressure (CPP), optimal CPP (CPPopt), Arterial Blood Pressure (ABP), End-Tidal CO2 (ETCO2), cerebrovascular pressure reactivity based on ICP (PRx) and volume-pressure compensatory reserve (RAP).
RESULTS.Data analyzed included seven males and two females
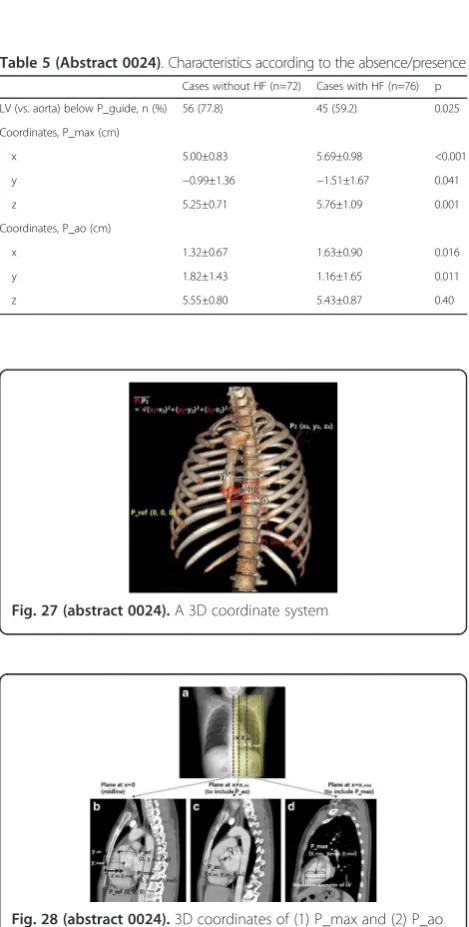
with mean age of 30.3 ± 11.1 years, with admission mean Glas-gow Coma Scale (GCS) of 6.1 ± 2.1 and Simplified Acute Physi-ology Score II (SAPSII) of 42.2 ± 14.6. Marshall classification of the first CT scan was predominantly grade III and before DC was IV. The mean period from hospital admission to DC was 3.3 ± 2 days. DC led to significantly decrease in ICP maximum values (p= 0.011) and lowered ICPd > 20 exposure (p = 0,038), in spite of non significant decrease of median ICP (Fig. 24). CPP before and after DC was significantly different (p = 0.038) as it was CPPopt (p = 0,021) (Fig. 25). Two hours before surgery PRx be-came positive indicating impairment of autoregulation (AR). The median values of PRx before and after DC show no statistically significant differences in spite of documented increase in its vari-ance (Fig. 26). Furthermore in some patients after DC, PRx remained >0.25 (used cut-off for AR). Before DC, RAP index was positive and closer to 1 expressing poor volume-pressure reserve. After DC RAP decreased with a trend towards to zero (p= 0.008) representing an improvement in brain compliance. Three months after hospital admission 67% of patients had Glasgow Outcome Scale (GOS)≥3. Mortality rate was 17%.
CONCLUSIONS.ICP, CPP and compensatory reserve improved
signifi-cantly as expected after DC. Sudden impairment of AR before DC may help to decide the timing of surgery. However, further studies are warranted to better understand DC influence on clinical decision and outcome.
REFERENCES
1. Kramer AH, Deis N, Ruddell S, et al. Decompressive Craniectomy in Patients with Traumatic Brain Injury: Are the Usual Indications Con-gruent with Those Evaluated in Clinical Trials? Neurocrit Care 2016 26:10–19.
2. Lazaridis C, Czosnyka M. Cerebral Blood Flow, Brain Tissue Oxygen, and Metabolic Effects of Decompressive Craniectomy.Neurocrit Care. 2012 16(3):478–484.
0019
Transfusion Requirements after Head Trauma (TRAHT): a randomized clinical trial
A. Gobatto1,2,3, M. L. Azevedo1, D. J. F. Solla1, W. S. Paiva1, L. M. Malbouisson1, E. B. Shu1
1Hospital da Clinicas - University of Sao Paulo Medical School, São Paulo,
Brazil;2Hospital São Rafael, Salvador, Brazil;3Hospital da CIdade, Salvador, Brazil
Correspondence:A. Gobatto
Intensive Care Medicine Experimental2017,5(Suppl 2):0019
INTRODUCTION.Anemia is frequent among traumatic brain
in-jured (TBI) patients, and it is associated with an increased risk of poor outcomes. The optimal hemoglobin (Hb) level to trigger red blood cell (RBC) transfusions in TBI patients is yet to be defined.
OBJECTIVE. To evaluate the feasibility and safety of creating a
hemoglobin gradient between TBI patients submitted to restrict-ive or liberal transfusion strategies in the ICU, as part of plan-ning a larger randomized clinical trial.
METHODS.From June 2015 to June 2016, all adult patients with
moderated or severe TBI were randomized either to a restrictive group, with an Hb transfusion threshold level of 7g/dL, or to a liberal group, with an Hb transfusion threshold level of 9g/dL. Transfusion strategies were maintained for up to 14 days or to ICU discharge. The primary outcome was the mean Hb differ-ence between groups. Secondary outcomes included transfusion requirements, intracranial pressure (ICP) management resources use, transcranial doppler (TCD) parameters, length of stay and mortality. Patients were followed for 6 months after hospital discharge.
RESULTS.A total of 44 patients were randomized, 21 patients to
the liberal group and 23 patients to the restrictive group. There was no baseline difference between the groups. The patients were predominantly male, 40 (90.9%) patients, mean age was 34.5 ± 13.4 years, and admission median Glasgow coma scale was 6 (quartiles 4–8). The mean CRASH score 14-day death risk was 40.7 ± 18.9% in the restrictive group and 39.3 ± 18.4% in liberal group (p = 0.818). The ICU admission Hb levels (g/dL) were 10.3 ± 1.6 in restrictive group and 10.1 ± 1.2 in liberal group (p = 0.550), and the average 14 days Hb level was 8.4 ± 1.0 and 9.3 ± 1.3 (p < 0.001), respectively. During ICU stay, RBC transfusion was administered to 13 (56.5%) patients in the restrictive group and to all 23 (100.0%) patients (p = 0.001) in the liberal group (a total of 35 and 66 RBC units, respectively; p = 0.022). There was an inverse correlation (−0.265) between Hb level and middle cerebral artery flow velocity (p < 0.001) at the side of trauma. This correlation was stronger on the liberal group (Hb range 7.1-12.6g/dL) when compared to the restrictive group (Hb 6.2-10.7g/dL). Hospital mortality was higher in the re-strictive group, seven (30.4%), versus one (4.8%) patient (p = 0.048).
CONCLUSION. Creating a hemoglobin gradient between the
groups was feasible. The restrictive group had lower hemoglobin levels and received less RBC transfusions. Mortality was higher in restrictive group.
REFERENCES
1. Lelubre C, Bouzat P, Crippa IA, Taccone FS. Anemia manage-ment after acute brain injury. São PauloCrit Care. 2016;20(1):152. 2. Robertson CS, Hannay HJ, Yamal JM, Gopinath S, Goodman JC, Tilley BC, et al. Effect of erythropoietin and transfusion threshold on neurological recovery after traumatic brain injury: a random-ized clinical trial. JAMA. 2014;312(1):36–47.
0020
Cumulative intracranial pressure and cerebral perfusion pressure burdens as determinants of early mortality after severe traumatic brain injury
H. S. Mangat1, X. Wu2, L. M. Gerber2, M. Fakhar1, S. B. Murthy1, P. E. Stieg3, J. Ghajar4, R. Härtl3
1
Weil Cornell University, Neurology, New York, United States;2Weil Cornell University, Healthcare Policy & Research, New York, United States; 3
Weil Cornell University, Neurological Surgery, New York, United States; 4Stanford University School of Medicine, Neurological Surgery, Palo Alto,
United States
Correspondence:H.S. Mangat
Intensive Care Medicine Experimental2017,5(Suppl 2):0020
INTRODUCTION.Increased Intracranial pressure (ICP) and low cerebral
perfusion pressure (CPP) remain the two main cerebral hemodynamic goals to improve outcomes after severe traumatic brain injury (TBI). Yet debate remains over the actual thresholds, and whether they need to be individualised based on autoregulation status or other criteria.1,2 Here, we used data from a large cohort to examine the association of cumulative ICP and CPP burden on outcome after severe TBI. Recent data from small cohorts has supported such an approach.3
Fig. 24 (abstract 0018).ICP and ICP dose before and after DC
Fig. 25 (abstract 0018).PRx before and after surgery