Dementia
Healthcare for London 2
Contents
Foreword
3
1 Introduction
5
1.1 What is dementia?
7
1.2 Who is affected and how?
8
1.3 Prevalence of dementia in the UK
9
1.4 Prevalence of dementia in London
9
1.5 Increasing prevalence and future need
12
1.6 Spending on dementia
14
1.7 Strategic context
18
1.8 The benefits of change
18
1.9 Key issues for London
20
2 Integrated care pathway
21
Introduction
22
2.1 Patient experience
22
2.2 Construction of the care pathway
23
2.3 Detailed description of the care pathway
25
2.4 Workforce competencies
43
2.5 Outcomes
44
3 General hospital care pathway
45
Introduction
46
3.1 Policy context
46
3.2 Construction of the general hospital care pathway
51
3.3 Action descriptions
55
3.4 General hospitals workforce competencies
66
3.5 Outcomes
66
3.6 Conclusions and recommendations for implementation
67
4 Memory services
69
Introduction
71
4.1 National and regional information
71
4.2 Specifying a memory service
73
4.3 Example commissioning specification for a memory service
75
Dementia services guide 3
Dementia can be an overwhelming and difficult diagnosis to hear, both for the person with dementia and for their carer. Dementia is surprisingly common, and given our ageing population and projections that the number of people with the condition will double in the next 30 years; providing dementia services to suit local communities will be a challenge. In London we are determined to respond to that challenge.
Nationally there have been some critical reports about the services available for people with dementia. Professor Lord Darzi’s Healthcare for London A Framework for Action
(2007) and the National Audit Office report Improving services and support for people with dementia(2007) highlighted that services were not provided consistently well across London.
The National Dementia Strategywas published in 2009 by the Department of Health and provides a framework of 17 objectives to help organisations develop dementia services. The strategy focuses on three key themes: improved awareness, early diagnosis and intervention, and high quality care and support.
Healthcare for London and its partners within the mental health project, recognise that people with dementia and their carers need improved access to early identification and diagnosis, better treatment in both primary and secondary care and good quality information. Providing dementia services for these components will significantly help to empower and support people with dementia and their carers so that they may make informed decisions as their condition progresses.
We welcome the Dementia services guide, which will assist London’s healthcare, social care and third sector organisations to commission services that will improve health outcomes and offer comprehensive support for people with dementia and their carers. We would like to thank those individuals and organisations that helped us develop the Dementia services guidethrough our consultation with primary and secondary healthcare professionals, social care experts and statutory, independent and third sector partners.
Joan Mager
Chief Executive, NHS Richmond, Healthcare for London Mental Health Senior Responsible Officer and Project Board Chair
Jenny Goodall
Director of Community and Children’s Services, City of London Corporation and Healthcare for London Dementia Task Group Chair
Healthcare for London
Dementia services guide 5
Intr
oduction
Introduction
Introduction
In July 2007, Professor Lord Darzi set out ambitious plans for improving the health and healthcare of Londoners in the report Healthcare for London: A Framework for Action. The report recognised that although mental healthcare provision is particularly strong in some areas of the capital, the service is not provided consistently well across London.
The Healthcare for London strategy was established by the capital’s 31 primary care trusts (PCTs) to change healthcare services and has been working to transform the way people with mental health conditions receive care. London has a high prevalence of people with mental health conditions compared with the national average, and levels are particularly high in boroughs with high levels of deprivation.
The number of people with dementia will increase as the population ages. Forecasts show a large increase in the numbers of people with dementia in London in future years. According to the Alzheimer’s Society’s report, Dementia UK, there will be a 14% increase in the numbers of people with dementia in London between now and 2021 but the effect of population change varies by PCT.
PCT level projections from Dementia UKare shown in the full needs assessment
(see appendix 1).
Mental illness is estimated to cost the capital £5 billion a year, taking into
account the cost of services, lost earnings and benefits1. Ensuring that services
for people with dementia and their carers are improved is a growing challenge and is becoming increasingly costly for the health service as a whole.
This guide aims to advise London commissioners and clinicians with local authority partners how to follow the integrated care pathway for dementia developed by Healthcare for London in order to:
• help all London commissioners plan services in partnership along with local
authority colleagues in social care
• provide a quality check against which they can benchmark services
• provide performance outcomes to help them review services.
Healthcare for London
6
1The London Assembly http://www.london.gov.uk/assembly/reports/health/mental-health.rtf
Intr
Dementia services guide 7
2Gupta et al. Rare and unusual dementias, Adv Psychiatric Treatment, 2009; 15: 364-371
Intr
oduction
1.1 What is dementia?
The term dementia is used to describe a collection of symptoms, including changes in memory, reasoning and communication skills, with a gradual loss of ability to carry out daily activities. These symptoms are caused by structural and chemical changes in the brain as a result of physical diseases such as Alzheimer’s disease.
There are a number of different types of dementia; with the most common being Alzheimer’s which accounts for about 60% of cases2.
• Alzheimer’s disease changes the chemistry and structure of the brain, causing brain cells to die. Over time the person will become increasingly dependent on others for help. They are likely to experience severe memory loss and become increasingly frail. They may have difficulty with eating, swallowing, continence and experience loss of communication skills such as speech.
• Vascular dementia is caused by strokes or small vessel disease which affects the supply of oxygen to the brain. Vascular dementia affects people in different ways. It can cause communication problems, stroke-like symptoms and acute confusion. This form of dementia progresses in a similar way to Alzheimer’s disease but progression is often ‘stepped’ rather than gradual.
• Frontotemporal dementia is a rare form of dementia affecting the front of the brain. It includes Pick’s disease and most commonly affects people under 65. In the early stages the memory may remain intact while the person’s behaviours and personality change.
• Dementia with Lewy bodies is caused by tiny spherical protein deposits that develop inside nerve cells in the brain. These interrupt the brain’s normal functioning, affecting the person’s memory, concentration and language skills. This type of dementia has symptoms similar to those of Parkinson’s disease such as tremors and slowness of movement.
Using this guide
Readers are asked to note, where reference is made to 'people with dementia and their carers' please read this as 'people with dementia and their informal or formal carers'.
The concept of personalisation underpins this Dementia services guide. This means that people with dementia and their carers will be empowered to shape their own lives and the services they receive.
1.2 Who is affected and how?
Dementia can affect anyone regardless of gender, ethnicity, socio-economic situation and residential status. Nearly two-thirds of people with the disorder live in the community, while the other third reside in a residential home. A small number of people with dementia are from black and minority ethnic (BME) groups. This is due to the current younger age profile in London’s BME communities. As this population ages, with a higher prevalence of physical conditions which may contribute to dementia, the rate of dementia is expected to increase.
A detailed analysis of the London population segments affected by dementia is available in appendix 1. This highlights that most cases of dementia are late-onset and therefore affect people aged 65 and over. Approximately one in 40 cases is early-onset dementia and occurs before the age of 65. Many factors, including age, genetic background, medical history and lifestyle can combine to lead to the onset of the disorder.
Key points to emerge from recent studies and consultations with people with dementia and their carers showed:
• Dementia is poorly understood, it remains a stigmatised condition and those affected often experience social exclusion and discrimination.
• Seeking help is frustrating; access to services typically includes contact with the NHS, local councils and the third sector; sometimes being referred elsewhere and often duplicating activities.
• Current services do not meet the needs of people with dementia.
• Services are fragmented and lack robust integration and strong partnership working. • There are gaps in provision and the quality of specialist services remains inconsistent. • Reliability and continuity of services are compromised because many staff lack
the requisite knowledge and skills to respond appropriately to those affected. • Most health and social care services are not delivering the outcomes that are
important to people with dementia: early diagnosis and treatment, easily accessible services, information and advice and high quality support.
Healthcare for London
8
Intr
Dementia services guide 9
3Source: Based on Dementia UK prevalence rates applied to GLA populations
Intr
oduction
1.3 Prevalence of dementia in the UK
According to Living Well with Dementia: A National Dementia Strategy, dementia is one of the most severe and devastating disorders faced by the NHS. Latest figures for the UK show:
• There are approximately 700,000 people with dementia.
• Within 30 years, the number of people with dementia is expected to double to 1.4 million.
• Dementia is predominantly a disorder of later life, but there are at least 15,000 people under the age of 65 who have the illness.
• The level of UK diagnosis and treatment of people with dementia is generally low, with a two-fold variation in population prevalence between the highest and lowest PCTs in London.
• International comparisons suggest that the UK is in the bottom third of European performance in terms of diagnosis and treatment, with less than half the activity of France, Sweden, Ireland and Spain.
1.4 Prevalence of dementia in London
Around 64,600 people have dementia in London including 1,560 people with early-onset and 63,019 people with late-onset dementia. Altogether the population with dementia makes up 1.4% of the total London population aged 30 years and over (see figure 1).
Figures 2 and 3 illustrate the rates for early and late-onset dementia in London PCTs and the range of overall numbers affected. In general the outer London boroughs have a higher prevalence than those in inner London but this pattern is not uniform and there will also be variations within each borough. Figure 4 indicates the estimated total numbers of people with dementia by PCT.
PCT Bromley Bexley Havering London Haringey Lambeth Relative position Highest Average Lowest
Proportion of people aged 30+ with dementia, 2007 2.0% 1.9% 1.9% 1.4% 1.0% 1.0%
47.7 to 53.6 (6) 46.2 to 47.7 (6) 43 to 46.2 (4) 37.8 to 43 (7) 33 to 37.8 (9) Early-onset dementia (30-64) Rate per 100,000 76.5 to 80 (7) 73 to 76.5 (5) 72 to 73 (6) 70.6 to 72 (5) 63.9 to 70.6 (8)
Late-onset dementia (over 65s) Rate per 1,000
Figure 2: Estimated prevalence of early-onset dementia by PCT, 2007
Figure 3: Estimated prevalence of late-onset dementia by PCT, 2007
Healthcare for London
10
Intr
2,780 to 3,810 (5) 2,290 to 2,760 (7) 1,770 to 2,290 (5) 1,470 to 1,770 (7) 1,170 to 1,470 (7) Early and late-onset dementia Numbers by PCT
Dementia services guide 11
4Source: Dementia UK and GLA populations 2007
Intr
oduction
Figure 4: Estimated total numbers of people with dementia by PCT, 2007
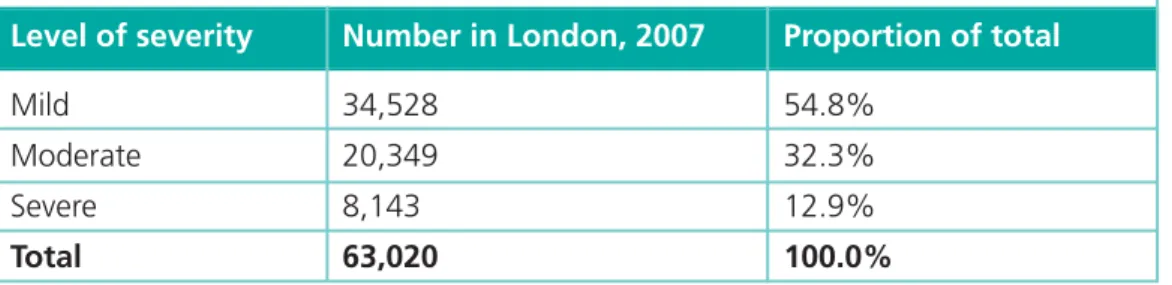
Figure 5 shows the numbers of new cases of dementia that occur each year. It also highlights a sharp rise with age.
Level of severity
Mild Moderate Severe Total
Figure 5: Number of people with mild, moderate and severe late-onset
dementia in London, 20074 Number in London, 2007 34,528 20,349 8,143 63,020 Proportion of total 54.8% 32.3% 12.9% 100.0%
1.5 Increasing prevalence and future need
Forecasts show a large increase in the number of people with dementia in London; however the effects of population change differ by PCT. The average annual increase in the number of people with the disease in London varies from 0.8% to 1.3% according to the projections used (see appendix 1). Specific attention will need to be paid to relatively high risk groups when developing local services. This includes ensuring that early identification and intervention services are equitably provided and meet the needs of different ethnic groups, homeless people, those with learning disabilities, people with HIV, travellers, substance misusers, prisoners, people who live alone, people in socially deprived areas and others who may have particular needs. It is also important that commissioning plans incorporate a sensitivity analysis by using more than one set of projections.
The above figures suggest that:
• There will be a 14% increase in the number of people with dementia in London over the 16 year period.
• The proportion of people with dementia who are female will reduce from 64% in 2005 to 59% in 2021.
• The proportion of people with dementia who are aged 75 and over will remain at 82%.
• The largest increase will be in males aged 75 and over (35% more).
Healthcare for London
12 5Source: Dementia UK Intr oduction Gender Male Female Persons
Figure 6: Projected increase in the number of people with dementia in
London by gender and age group, 2005 to 20215
Age group 30-64 65-75 75+ Total 30-64 65-75 75+ Total 30-64 65-75 75+ Total People with dementia 2005 855 4,912 15,009 20,776 657 3,981 32,301 36,939 1,512 8,893 47,310 57,715 People with dementia 2021 1,134 5,529 20,241 26,904 801 4,691 33,541 39,033 1,935 10,220 53,782 65,937 Percentage increase 33% 13% 35% 29% 22% 18% 4% 6% 28% 15% 14% 14%
Dementia services guide 13
6Source: Dementia UK
Intr
oduction
Figure 7: Projected increases in the number of people with dementia by PCT,
2005 to 20216
Different population projections have been used in this guide and have produced different prevalence rates. The Dementia UKprojections were quoted in the
Department of Health’s National Dementia Strategyand were calculated by applying census prevalence rates to Office of National Statistics (ONS) population projections. However the use of other population projections produces different results and two alternative scenarios should also be considered:
• Projections of dementia by Projecting Older People Population Information (POPPI) using more recent ONS population projections than those used in Dementia UK.
• Projections of dementia calculated by Healthcare for London for the needs assessment using GLA population projections.
The variances in using different population projections can be found in appendix 1.
22% to 54% (7) 14% to 22% (8) 0% to 14% (7) -7% to 0% (9)
1.6 Spending on dementia
Dementia accounts for the biggest proportion of mental health expenditure in the UK. Currently, access to early identification, assessment and treatment is inequitable with some people in the under 65 age group struggling to access services.
Early intervention will delay the speed of decline in a person with dementia and reduce the time patients spend in institutional settings. The level of service capacity required to improve outcomes is unknown, as service commission or provision of unmet need across London has not yet been mapped.
The economic costs of an illness can be calculated in different ways and can be hard to describe accurately. For example costs can be direct or indirect, can be examined from different perspectives (e.g. the NHS, the public sector or society as a whole), and can cover different time periods. The cost of dementia is substantial and it has been reported that ‘the direct costs of Alzheimer’s disease alone exceed the total cost of stroke, cancer and heart disease’7. One study quoted by the National Institute for Health and Clinical Excellence (NICE) calculated the direct costs of Alzheimer’s disease alone in the UK to be between £7.1 billion and £14.9 billion in 20008.
The Dementia UKreport calculated a total cost of £17.03 billion per annum for the UK in 2005/06. This equated to an average cost per person with dementia of £25,472 per annum. This only includes the cost of service provision and does not include the wider economic costs associated with issues such as lost employment and taxation and welfare benefits.
Costs of providing services increase with the progression of the disease. Direct costs are higher for people with severe dementia (figure 8).
Healthcare for London
14
7National Institute for Health and Clinical Excellence. Dementia Costing Report – implementing NICE SCIE
guidance in England, 2006 8Lowin et al. 2001 9Source: Dementia UK 2007 Intr oduction Service NHS Social services Informal care Accommodation Total cost
Figure 8: Annual costs of services used by people with late-onset dementia
(per person), 2005/069 Mild dementia, community £2,508 £4,935 £9,246 £0 £16,689 Moderate dementia, community £2,430 £6,224 £17,223 £0 £25,877 Severe dementia, community £2,639 £7,738 £27,096 £0 £37,473 Dementia in residential care setting £1,334 £378 £938 £28,646 £31,296
Dementia services guide 15
10Source: Personal Social Services Research Unit 2008 11QOF 2007/08
Intr
oduction
Costs in London are likely to be higher than those listed in figure 8 because of higher salaries and the cost of living. The ‘London effect’ will vary for each component, but some examples of additional staff costs are given below.
• Social worker salary: 10% extra in London.
• Approved social worker (mental health): 20% extra in London.
• Local authority day care (mental health) revenue cost: 30% higher in London. • Community nurse salary: 19% extra in London10.
Additional costs would also be incurred as a result of high staff turnover and use of agency staff in some areas.
Healthcare for London has investigated the cost of dementia in London and the savings needed to ensure investment in memory services is cost neutral. The impact of the introduction of Mental Health Payment by Results (PbR) has been considered (see appendices 6 and 7).
Impact on primary care
Overall, 23,871 patients are recorded on GP practice registers as having dementia across London11. This equates to about 37% of the total number of people estimated to have dementia in the capital. Figures for each London PCT are available in appendix 1. While it is not expected that everyone with dementia would appear on GP registers, the current coverage amounts to just over a third of the population affected. There are many reasons why primary care registers may under-record the level of dementia. This might be due to various factors relating to the overall level of services and infrastructure of the practice. Other reasons may include the level of dementia diagnosis and care in each area.
Across London 83% of those people with dementia on GP registers, who were eligible to be reviewed by the primary care practice, were reviewed over 15 months during 2007/08 (see appendix 1).
Some patients may be excluded from indicators for various reasons and guidance on this is available in the Quality and Outcomes Framework (QOF). Some reasons for exclusions include:
• Patients who have been recorded as refusing to attend a review who have been invited on at least three occasions during the preceding 12 months.
• Patients for whom it is not appropriate to review the chronic disease parameters due to particular circumstances e.g. terminal illness or extreme frailty.
• Patients newly diagnosed within the practice or who have recently registered with the practice.
Prescribing data
Over 90,000 prescriptions of dementia-related drugs were made in London during 2007/08 at a cost of £5.7 million. This equates to 1,406.9 prescriptions per 1,000 people estimated to have dementia over the 12 month period and the range between PCTs is shown in figure 9. Further information is provided in appendix 1.
Impact on carers
Eleven per cent of people over the age of 65 in London provide informal care to a family member, friend, neighbour or other individual who suffers with dementia. About two thirds of people with dementia, including some who have severe dementia, live in the community supported by informal carers. Most carers are spouses of a similar age to the person for whom they are caring; many will also have some degree of age related impairment or be in poor health. Where spouse care is not available, daughters or other female kin are often involved13.
Dementia can have a devastating effect on family relationships and in particular on the psychological stress, depression and physical strain experienced by the primary carers. This often increases as the severity of the disease progresses. One study14 found that the number of hours of informal care required also increased once the dementia progressed:
• people with mild dementia received an average of 13.1 hours a week • people with moderate dementia received an average of 39.4 hours a week • people with severe dementia received an average of 46.1 hours a week.
Healthcare for London
16
12Source: Healthcare for London, drawn from NHSBSA and EPACT (Prescription Pricing Authority) 13London Centre for Dementia Care (LCDM/UCL and LBS). London Borough of Sutton – older people with
dementia service redesign, 2008
14Langa KM et al. National estimates of the quantity and cost of informal care giving for the elderly with
dementia. Journal of General Internal Medicine, 16(11):770-78, 2001 (quoted in LCDC above).
Intr oduction Relative position Highest Average Lowest
Figure 9: Range in prescriptions for dementia related drugs per 1,000
estimated people with dementia, by PCT 2007/0812
PCT
Lambeth Tower Hamlets Lewisham
London
Hammersmith & Fulham Croydon
Ealing
Prescriptions for dementia related drugs per 1000 estimated people with dementia, 2007/08
2769.5 2369.8 2146.8 1406.9 291.5 236.8 200.0
Dementia services guide 17
15Banerjee S et al. Predictors of institutionalisation in people with dementia. Journal of Neurology Neurosurgery
and Psychiatry. 74:1315-1316, 2003 (quoted in LCDC).
16Eaker ED. Predictors of nursing homes admission and/or death on incident Alzheimer’s disease and other
dementia cases compared to controls: a population based study. Journal of Clinical Epidemiology 55:462-468, 2002 (quoted in LCDC).
17Department of Health. Care Services Improvement Partnership. Creative models of short breaks (respite care)
for people with dementia, 2008
Intr
oduction
These figures are likely to understate the support provided by carers as they are unlikely to include the long hours required to be spent with someone with severe dementia although not physically carrying out specific caring tasks.
Nevertheless, family care often enables people with dementia to continue living at home for a longer period of time, and overall those living with a family carer have been found to be 20 times less likely to be admitted to long-term care15. A study also found older people with dementia were more likely to move into a residential home if they were frequently active at night, immobile or had difficulty walking, incontinent, being cared for by a carer for more than 16 hours a week, and where
the primary carer was female16.
The need to offer more support for family carers has been recognised in the National Dementia Strategy. A Care Services Improvement Partnership (CSIP) report17on short breaks for carers of people with dementia suggests that:
• There is still limited access to short breaks.
• There is insufficient choice, in particular on in-home care and affordability. • The range of services available in many areas does not reflect the diversity of
the population it is commissioned for.
• Short breaks cannot be seen in isolation from other services supporting people with dementia.
There are various types of short breaks available: • day care
• support provided in the person’s own home • overnight care away from home
• host family care • adult placements • emergency breaks.
The CSIP report also includes a set of principles that should govern the provision of short breaks, and provides examples of good practice. It is important that this should be seen as part of a wider package of support for carers.
1.7 Strategic context
The National Dementia Strategyis a five year strategy designed to guide health and social care commissioners, strategic health authorities, health trusts, practice based commissioners and local authorities, the third sector and independent providers in planning, developing and monitoring services. Service integration and partnership with people with dementia and carers is key to achieving the objectives set out in the
National Dementia Strategy.
Besides the National Dementia Strategy, this guidance is set within the wider policy context which includes:
• Our health, our care, our say: a new direction for community services18. • High quality care for all: NHS Next Stage Review final report19.
• End of Life Care Strategy – promoting high quality care for all adults at the end of life20.
• Putting People First: A shared vision and commitment to the transformation of adult social care21.
• Carers’ Strategy: Carers at the heart of 21st century families and communities: a caring system on your side, a life of your own22.
• The NICE-SCIE guidelines on supporting people with dementia and their carers in health and social care23.
1.8 The benefits of change
The Healthcare for London integrated care pathway (section 2) is based on the
recommendations made in the National Dementia Strategyand highlights the benefits of change and the need to improve services for people with dementia and their immediate carer.
The National Dementia Strategy24provides a strategic quality framework to raise awareness of dementia, facilitate early diagnosis and improve services. It outlines 17 objectives to improve the quality of life for people with dementia and their carers under three key themes:
• raising awareness and understanding • early diagnosis and support
• living well with dementia.
Healthcare for London
18
18Department of Health. Our health, our care, our say: a new direction for community services, 2006 19Department of Health. High quality care for all: NHS Next Stage Review final report, 2008
20Department of Health. End of Life Care Strategy – promoting high quality care for all adults at the end of life,
2008
21Department of Health. Putting People First: A shared vision and commitment to the transformation of adult
social care, 2007
22Department of Health. Carers at the heart of 21st century families and communities: a caring system on your
side, a life of your own, 2008
23NICE-SCIE. Supporting people with dementia and their carers in health and social care, 2006 24Department of Health. Living well with dementia: A National Dementia Strategy, 2009
Intr
Dementia services guide 19
25Department of Health. Living well with dementia: A National Dementia Strategy, 2009
Intr
oduction
Raising awareness
and understanding
01 Public information campaign
02 Memory services
03 Information for people with dementia andcarers
Making the change
013 Workforce competencies, development and training
014 Joint local commissioning strategy and WorldClass Commissioning
015 Performance monitoring and evaluation including inspection
016 Research
017 Effective national and regional support for implementation of the strategy
04 Continuity of support for people with dementia andcarers
05 Peer support for people with dementia andcarers
06 Improvedcommunity personal support
07 Implementingcarers’ strategy for peole with dementia
08 Improvedcare in general hospitals
09 Improved intermediate care for dementia
010 Housing including telecare
011 Improvedcare home care
012 Improved end-of-life care
Early diagnosis
andsupport
Living well with
dementia
Figure 10: Delivering the National Dementia Strategy– joint commissioning
of services among a defined care pathway to enable people to live well
Healthcare for London
20
Intr
oduction
1.9 Key issues for London
Population size and composition varies widely. Some PCTs face substantial growth in the numbers of people with dementia while others will see relatively little change (see appendix 1). PCTs will see an increase in the ethnic diversity of their older populations, and many face challenges associated with diagnosing dementia and providing support for more high risk groups such as: people in areas of high deprivation, homeless people, those with learning disabilities, people with HIV, travellers, substance misusers, prisoners, and people who live alone – in some cases a long distance from other family members. While local models of care will need to be based on national guidelines and on evidence of clinical and cost effectiveness, specific service requirements will vary across the capital. These will be influenced by differences in populations and in service infrastructure between PCT areas.
Implementation of the Healthcare for London integrated care pathway for dementia offers the opportunity to develop a consistent care pathway while taking local differences into account. This will include local commissioning patterns of health and social care services for older people with mental health problems, as well as the availability of key staff, the critical mass required, cost effectiveness and accessibility for people who may have dementia and their carers.
Integrated care
pathway
2
Dementia services guide 21Integrated car
e
Introduction
This section contains the recommended service delivery model for providing dementia care. It includes access to services, the journey through the pathway and the recommended standards for service provision, as well as clinical principles and standards which underpin service delivery.
The integrated care pathway provides guidance about effective services and
interventions that deliver outcomes for people living with dementia and their carers. Its implementation is designed to:
• promote integration of care
• promote the principles of personalisation
• improve multi-agency working
• assist in the process of evaluating the quality of care
• clarify staff roles and responsibilities
• improve communication between professionals
• ensure people with dementia receive evidence based care
• ensure services are measured and continually improved.
Commissioners and providers should work together to develop local policies, protocols and practitioner networks which cross professional boundaries and focus on meeting the needs of the local community.
The integrated care pathway has been developed to support commissioners by providing best practice guidance and recommendations for efficient and effective care for people with dementia and their carers (figure 1). The pathway includes interventions and recommendations for carers’ services.
2.1 Patient experience
Following a diagnosis of dementia there are key principles and actions that need to be taken to ensure that appropriate support is always available. This support should respond to the changing needs of both the person with dementia and their carer, with the aim of avoiding unmanaged crises.
Commissioners and clinicians will need to consider the following issues:
Dignity and respect– all people with dementia and their carers should be treated as
valued individuals with respect for their dignity and privacy, and staff should be sensitive to the cultural needs of patients.
Continuity – services should be designed to maintain a key contact point who can
advocate on behalf of the person with dementia and their carer; for example a dementia adviser role.
Healthcare for London
22
Integrated car
e
Clear communications– processes should be in place to ensure that all people with dementia and their carers are able to communicate with staff and convey information in confidence.
Information sharing with other healthcare professionals– care planning should
be coordinated and consistent. This will improve transfers of care and help ensure vulnerability issues are considered.
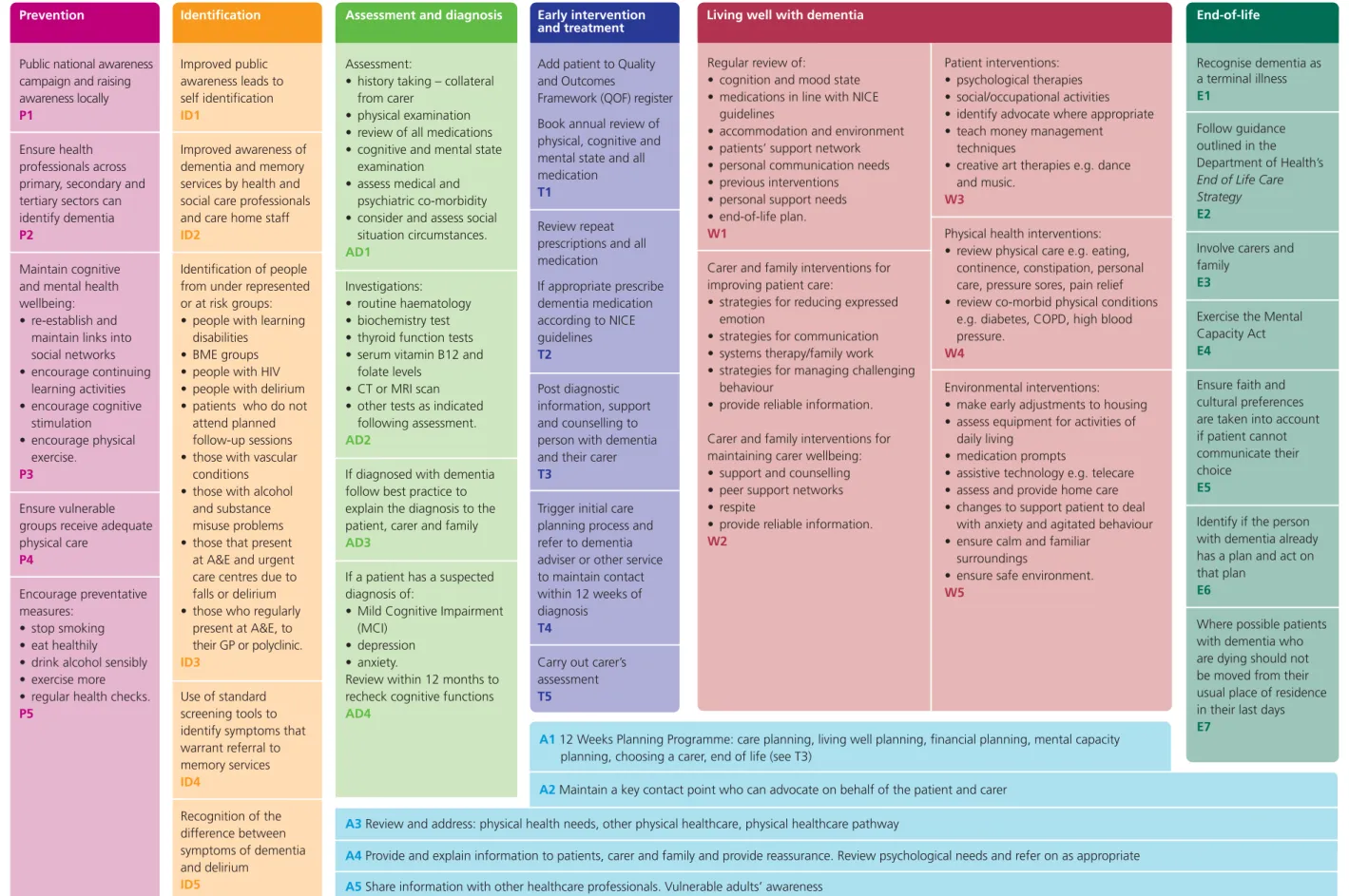
2.2 Construction of the care pathway
The integrated care pathway was developed along the principles of:
• prevention
• identification
• assessment and diagnosis
• early intervention and treatment
• living well with dementia
• end-of-life.
The integrated care pathway is a multi-disciplinary, multi-agency, planned approach to the delivery of high quality care and support for people with dementia and their carers. It is an age inclusive pathway that covers all people with dementia.
It sets out general guidance about services and interventions including effective treatment and therapies for delivering high quality care and support to people with dementia whenever they are in contact with health and social care systems, including those:
• worried about their memory and other psychological changes
• seeking a diagnosis of dementia
• newly diagnosed with dementia
• experiencing difficulties in activities of daily living
• living in the community with dementia
• patients in an acute hospital whose behaviour suggests they may have dementia
• living in a care home and experiencing difficulties in cognition
• with learning disabilities
• at the end of their life.
It is recommended that the integrated care pathway is continuously developed in response to feedback from people with dementia and their carers, and local quality and outcome findings.
Dementia services guide 23
Integrated car
e
The pathway has been set out as boxes that have been given letters and numbers. Each box contains a set of recommended actions and activities:
• A: actions that need to be undertaken across the pathway
• P: prevention
• ID: identification of dementia
• AD: assessment and diagnosis
• T: early interventions and treatments
• W: activities and tasks that enable people to live well with dementia
• E: end-of-life care.
At an individual level, services, interventions and support should:
• uphold the dignity of people with dementia
• respect and value diversity and promote equality
• acknowledge the central role of people with dementia and their carers in the process of planning and developing services
• ensure that the best and most effective pharmacological and non-pharmacological treatments are widely and consistently available
• provide the practical advice and information people with dementia and their carers need, as well as developing consistently high quality, comprehensive packages of care and support which enhance access to services
• include everyone and respond to people on the basis of need not age
• support the individual to live safely and well at home for as long as possible if desired
• provide joined up care as part of integrated services
• contribute to overall wellbeing
• ensure access to universal services.
Healthcare for London
24
Integrated car
e
Integrated
Prevention
Public national awareness campaign and raising awareness locally P1
Ensure health professionals across primary, secondary and tertiary sectors can identify dementia P2
Maintain cognitive and mental health wellbeing: • re-establish and
maintain links into social networks • encourage continuing learning activities • encourage cognitive stimulation • encourage physical exercise. P3 Ensure vulnerable groups receive adequate physical care P4 Encourage preventative measures: • stop smoking • eat healthily • drink alcohol sensibly • exercise more • regular health checks. P5
Assessment and diagnosis
Assessment:
• history taking – collateral from carer
• physical examination • review of all medications • cognitive and mental state
examination • assess medical and
psychiatric co-morbidity • consider and assess social
situation circumstances.
AD1
Investigations: • routine haematology • biochemistry test • thyroid function tests • serum vitamin B12 and
folate levels • CT or MRI scan • other tests as indicated
following assessment.
AD2
If diagnosed with dementia follow best practice to explain the diagnosis to the patient, carer and family
AD3
If a patient has a suspected diagnosis of:
• Mild Cognitive Impairment (MCI)
• depression • anxiety.
Review within 12 months to recheck cognitive functions
AD4
Early intervention and treatment Add patient to Quality and Outcomes
Framework (QOF) register Book annual review of physical, cognitive and mental state and all medication T1
Review repeat prescriptions and all medication If appropriate prescribe dementia medication according to NICE guidelines T2 Post diagnostic information, support and counselling to person with dementia and their carer T3
Trigger initial care planning process and refer to dementia adviser or other service to maintain contact within 12 weeks of diagnosis
T4
Carry out carer’s assessment T5
Regular review of:
• cognition and mood state • medications in line with NICE
guidelines
• accommodation and environment • patients’ support network • personal communication needs • previous interventions
• personal support needs
• end-of-life plan.
W1
Carer and family interventions for improving patient care:
• strategies for reducing expressed emotion
• strategies for communication • systems therapy/family work • strategies for managing challenging
behaviour
• provide reliable information. Carer and family interventions for maintaining carer wellbeing: • support and counselling • peer support networks • respite
• provide reliable information.
W2
Patient interventions: • psychological therapies • social/occupational activities • identify advocate where appropriate • teach money management
techniques
• creative art therapies e.g. dance and music.
W3
Physical health interventions: • review physical care e.g. eating,
continence, constipation, personal care, pressure sores, pain relief • review co-morbid physical conditions
e.g. diabetes, COPD, high blood pressure.
W4
Environmental interventions: • make early adjustments to housing • assess equipment for activities of
daily living
• medication prompts
• assistive technology e.g. telecare • assess and provide home care • changes to support patient to deal
with anxiety and agitated behaviour • ensure calm and familiar
surroundings
• ensure safe environment.
W5
A3Review and address: physical health needs, other physical healthcare, physical healthcare pathway
A4 Provide and explain information to patients, carer and family and provide reassurance. Review psychological needs and refer on as appropriate
A5Share information with other healthcare professionals. Vulnerable adults’ awareness
A6 Agree indicators for moving along pathway and implement Mental Capacity Act as appropriate
A1 12 Weeks Planning Programme: care planning, living well planning, financial planning, mental capacity planning, choosing a carer, end of life (see T3)
A2Maintain a key contact point who can advocate on behalf of the patient and carer
Figure 1: Integrated care pathway
Living well with dementia End-of-life
Recognise dementia as a terminal illness E1 Follow guidance outlined in the Department of Health’s
End of Life Care Strategy
E2
Involve carers and family
E3
Exercise the Mental Capacity Act
E4
Ensure faith and cultural preferences are taken into account if patient cannot communicate their choice
E5
Identify if the person with dementia already has a plan and act on that plan
E6
Where possible patients with dementia who are dying should not be moved from their usual place of residence in their last days
E7 Identification Improved public awareness leads to self identification ID1 Improved awareness of dementia and memory services by health and social care professionals and care home staff ID2
Identification of people from under represented or at risk groups: • people with learning
disabilities • BME groups • people with HIV • people with delirium • patients who do not
attend planned follow-up sessions • those with vascular
conditions • those with alcohol
and substance misuse problems • those that present
at A&E and urgent care centres due to falls or delirium • those who regularly
present at A&E, to their GP or polyclinic. ID3
Use of standard screening tools to identify symptoms that warrant referral to memory services ID4 Recognition of the difference between symptoms of dementia and delirium ID5
Dementia services guide 25 Integrated car e pathway A A2
2.3 Detailed description of the care pathway
Actions to be taken across the pathway
Following a diagnosis, people with dementia and their carers need good support along the pathway. Key actions (A1-A6) will ensure that support is always available.
Care plans should:
• be developed in partnership with people with dementia and their carers
• be shared between professionals and agencies involved in the care and treatment. It is important to ensure that vulnerable adults (P4) are identified and local protocols are followed
• include details of services; ensure financial and legal aspects are in place to meet the needs along the pathway; from living well to end of life care (A1)
• detail the patient’s psychological, psychiatric and physical health needs (A3), how these are to be met and by whom (A4)
• be regularly monitored and reviewed (A1). Part of the care planning process will include identification of a dementia contact point (A2) and information giving (A5).
12 Weeks Planning Programme:
• care planning • living well planning • financial planning
• mental capacity planning • choosing a carer
• end-of-life (see T3).
Maintain a key contact point who can advocate on behalf of the patient and carer
1Banerjee and Wittenberg. Clinical and cost effectiveness of services for early diagnosis and intervention in dementia, 2009 Planning needs to start early, as it will be beneficial for both the person with dementia and their carer. Early planning will also improve the likelihood that service capacity is available.
Research shows that a memory service provides a suitable setting to generate an early diagnosis, which can enable choice and forward planning while people have capacity1.
A consistent point of contact who can advocate on behalf of both the patient and their carer is required. A professional relationship should be developed with the person with dementia and their carer. The key contact should have a good understanding of their needs, condition and history.
The point of contact should be consistent and accessible.
Healthcare for London
26
Integrated car
e
pathway
It is important to ensure a joined up and coordinated care plan which meets the needs of the person with dementia and their carer.
Providing written information and websites to gain further information is useful to the person with dementia and their carer. It will help with the difficult process of acceptance and understanding, allowing people to access information at a speed that is right for them. Provide a place to discuss their diagnosis and the opportunity to ask questions.
.
It is essential to have a coordinated and consistent approach to care planning. This will help reduce delayed transfers of care and ensure that vulnerability issues are not overlooked. Vulnerable adults can suffer abuse, therefore local safeguarding protocols should be followed2.
Involving the person with dementia and their carer, as part of the care planning process, will give confidence that changing needs will be met appropriately along the pathway. It is good practice to discuss with the person with dementia and their carer, while they still have mental capacity, about the use of:
• advance statements (stating what is to take place if the person loses the capacity to communicate or make decisions)
• advance decisions to refuse treatment
• Lasting Power of Attorney
• A Preferred Place of Care Plan3.
As the person with dementia deteriorates, decisions about sharing information should be made in the context of the Mental Capacity Act 2005.
2Royal College of Psychiatrists., Institutional abuse of older adults, Council Report CR84 3NICE-SCIE. Dementia Quick Reference Guide, 2006
A3
A4
A5
A6
Review and address:
• physical health needs • other physical healthcare • physical healthcare
pathway.
Provide and explain information to patients, carer and family and provide reassurance
Review psychological or psychiatric needs and refer on as appropriate
Share information with other healthcare professionals Vulnerable adults’ awareness
Agree indicators for moving along pathway and
implement Mental Capacity Act as appropriate
Dementia services guide 27
Integrated car
e
pathway
P
Stigma, social exclusion, age discrimination and the attitudes of some professionals and care staff may prevent those who are worried about their memory from seeking help during the early stages of dementia. Reliable and good quality information, especially about the benefits of early diagnosis and living well with dementia, can overcome barriers to identification and encourage contact.
A national public information campaign, phased over a number of years, is being developed by the Department of Health. Engaging at a local level with the community will give a greater understanding of local needs.
All staff in contact with older adults must be provided with accessible and accurate information about dementia, and the health, social care and community services that are available.
Primary care trusts (PCTs), hospital trusts and local authority partners should ensure their front line staff have gained a basic competence in understanding the symptoms of dementia. The NICE-SCIE guidelines4 provide evidence to support the professional education and training needs of health and social care staff.
Achieving the standard related to prevention of dementia requires PCTs and local authorities to work with other health partners to:
• develop joint strategies for raising awareness about prevention of dementia in local communities
• promote cognitive, emotional, mental and physical wellbeing
• ensure responses to major national campaigns e.g.
Safe, Sensible, Social: The next steps in the National Alcohol Strategy(2007) include information about risks of alcohol-related brain damage and signpost sources of help
• promote the use of services such as leisure centres to enable people to maintain healthy lifestyles.
4NICE-SCIE. Dementia: Supporting people with dementia and their carers in health and social care, 2006
P1
P2
P3
Prevention
Public national awareness campaign and raising awareness locally
Ensure health professionals across primary, secondary and tertiary sectors can identify dementia
Maintain cognitive and mental health wellbeing:
• re-establish and maintain links into social networks • encourage continuing learning activities • encourage cognitive stimulation • encourage physical exercise.
Healthcare for London
28
Integrated car
e
pathway
Groups who are particularly vulnerable include:
• people with learning disabilities
• older adults, people aged over 85
• people with co-morbidities
• women living alone
• working/middle-aged adults with low health status and poor lifestyles.
Physical ill health and problems relating to physical functions can increase the risk of dementia. Encouraging a healthy lifestyle is important. It is
recommend by the Alzheimer’s Society that people take regular exercise; eat healthily, take part in social activities and make sure they get their blood pressure checked. It is important that people are made more aware that what is good for your heart is also good for your head.
New Horizons, Towards a shared vision for mental health
states that keeping physically healthy is good for all aspects of mental health and physically fit people have a lower rate of dementia. Up to half of all people with dementia may have a vascular component (i.e. vascular dementia or mixed dementia). Current health promotion messages on diet and lifestyle, and regular health checks are therefore likely to reduce this risk5.
5Department of Health. New Horizons, Towards a shared vision for mental health, 2009
P4
P5
Ensure vulnerable groups receive adequate physical care
Encourage preventative measures:
• stop smoking • eat healthily
• drink alcohol sensibly • exercise more
Dementia services guide 29
Integrated car
e
pathway
ID
People with dementia and their families are often reluctant to seek help, and can sometimes mask and deny difficulties, managing problems until a crisis occurs. Early identification of dementia offers those affected and their families the opportunity of an early diagnosis and the chance to make plans for living well with dementia. Good practice in breaking bad news of a diagnosis is sharing the information with the patient and carer at the speed of the individual’s understanding and willingness to listen.
Important points for identification are:
• proactive work by primary care e.g. case finding
• recognition by staff in generic services e.g. in general hospitals (see section 3 on general hospital care pathway and guidance) and social care settings. The benefits of early identification include:
• identification of treatable physical and psychiatric causes
• treatment of co-morbidity and other conditions
• medication in line with NICE-SCIE guidelines6
• reliable instigation of pharmacological treatments
• information for individuals and families to provide them with a better explanation and understanding of the diagnosis
• access to local support services and legal and financial advice
• identification of more socially vulnerable individuals (older adults over 85, living alone, poor housing) at greater risk of admission to care
• referral to psycho-social support
• help with daily living activities
• opportunity for people with dementia and their carers to plan for the future.
6NICE-SCIE. Dementia: Supporting people with dementia and their carers in health and social care, 2006
ID1
Identification
Improved public awareness leads to self identification
Healthcare for London
30
Integrated car
e
pathway
7Department of Health. Living well with dementia: A National Dementia Strategy, 2009 This group includes:
• primary care, general hospital and mental health staff
• care managers in adult care services and social care staff in the independent sector
• third sector and private providers.
Residential and nursing care home staff must be trained to recognise residents who may have dementia and ensure care plans take account of cognitive impairment and reflect person-centred care.
The setting for identifying those who are under represented or at risk is through GP practices and general hospitals.
Following the recommendations of the National
Dementia Strategy7professionals and care staff need to be able to identify individuals with possible dementia. They must also give good basic information and advice and refer appropriately to local memory services.
ID2
ID3
Improved awareness of dementia and memory services by health and social care professionals and care home staff
Identification of people from under represented or at risk groups:
• people with learning disabilities
• BME groups • people with HIV • people with delirium • patients who do not
attend planned follow-up sessions
• those with vascular conditions
• those with alcohol and substance misuse problems
• those that present at A&E and urgent care centres due to falls or delirium • those who regularly
present at A&E, to their GP or polyclinic.
Dementia services guide 31
Integrated car
e
pathway
8NICE-SCIE. Dementia: Supporting people with dementia and their carers in health and social care, 2006 9NICE-SCIE. Dementia: Supporting people with dementia and their carers in health and social care, 2006 10Department of Health. Living well with dementia: A National Dementia Strategy, 2009
Refer to the NICE-SCIE guidelines for standard screening tools, e.g. Mini Mental State Examination (MMSE) and Cambridge tools8.
Memory services for the early identification and care of people with dementia should be available for local people and should provide a single point of referral. Their functions are:
• early identification and referral of people with a possible diagnosis of dementia
• a high quality service for the assessment, diagnosis and management of dementia.
To recognise signs and symptoms of delirium refer to the NICE-SCIE guidelines9.
The guidelines define delirium as:
“Delirium (acute confusional state) is a common
condition in the elderly affecting up to 30% of all elderly medical patients. Patients who develop delirium have high mortality, institutionalisation and complication rates, and have longer lengths of stay than non-delirious patients. Delirium is often not recognised by clinicians, and is often poorly managed. Delirium may be prevented in up to a third of older patients. The aim of these guidelines is to aid recognition of delirium and to provide guidance on how to manage these complex and challenging patients”.
Health and social care staff need to:
• ensure all local services promote easy access to care and treatment
• support the individual’s journey from the early stages. Based on the National Dementia Strategy, Healthcare for London recommends that all complex cases and younger people with dementia are referred10to specialist services.
ID5
Use of standard screening tools to identify symptoms that warrant referral to memory services
Recognition of the difference between symptoms of
dementia and delirium ID4
Healthcare for London
32
Integrated car
e
pathway
Below is the process flow of a person with dementia:
Identification
Pr
evention and awar
eness
Person with memory pr
oblem • in community • primary car e • acute hospital.
Living well with dementia
Mild cognitive impairment r
eview
6-12 months
Assessment and diagnosis
Uncomplicated memory pr oblem • investigation/assessment • diagnosis • communications • tr eatments. Not having: • depr ession • delirium • lear ning dif ficulties.
*May need specialist
assessment End-of-life End-of-life Pr esent to primary car e Specialist memory service Memory pr
oblem complicated by:
1. Behavioural and psychological
symptoms of dementia, depr
ession.
Needs ar
e best met by mental
health services. 2. Complicated neur opsychiatric, neur opsychological, neuorlogical condition. 3 . Main concer n is physical health in the back dr op of dementia.
Dementia services guide 33
Integrated car
e
pathway
AD
11NICE-SCIE. Dementia: Supporting people with dementia and their carers in health and social care, 2006 12Royal College of Psychiatrists (2005)
As outlined in the NICE-SCIE11guidelines, these assessments need to be carried out for a diagnosis to be made.
Clinical examinations should be based on a standardised system in line with the NICE-SCIE guidelines using specified and agreed tools.
Investigations can include syphilis serology and HIV tests if indicated.
There is an increased likelihood that people with Mild Cognitive Impairment (MCI) may go on to develop dementia. It is estimated that about 15% will develop dementia every year and 90% of these will develop Alzheimer's disease12.
It is suggested that improved access to memory services will increase early identification and diagnosis.
AD1
AD2
AD3
Assessment:
• history taking – collateral from carer
• physical examination • review of all medications • cognitive and mental
state examination • assess medical and
psychiatric co-morbidity • consider and assess social
situation circumstances.
Investigations:
• routine haematology • biochemistry test • thyroid function tests • serum vitamin B12 and
folate levels • CT or MRI scan
• other tests as indicated following assessment.
If patient is diagnosed with dementia follow best practice to explain the diagnosis to the patient, carer and family
Healthcare for London
34
Integrated car
e
pathway
A systematic and supportive approach to providing diagnosis should be established. Locally agreed joint procedures should cover:
• pre-diagnosis counselling
• diagnosis and prognosis
• post diagnosis services and support including information in a range of formats
• care planning and management
• follow-up care arrangements.
AD4
If a patient has a suspected diagnosis of:
• Mild Cognitive Impairment (MCI) • depression • anxiety.
Review within 12 months to recheck cognitive functions
Dementia services guide 35
Integrated car
e
pathway
T1
13NICE-SCIE. Dementia: Supporting people with dementia and their carers in health and social care, 2006
Inclusion on the patient register as prescribed in the QOF will provide an additional mechanism to guarantee that the patient’s care is managed in a systematic way. Ensuring any changes are noted in the annual reviews provides a good record for the future management of the patient, either in a primary care setting or by a specialist. It is important to record the person on the QOF register under the appropriate code. Incorrect data cannot be removed.
The NICE-SCIE guidelines note that an appropriate diagnosis of dementia can be made in primary care13as most specialists undertake broadly similar assessments in terms of history, mental state and blood tests. The use of other diagnostic tests varies considerably.
The NICE-SCIE guidelines indicate it is good practice to share the diagnosis with the person with dementia. It must be acknowledged that there may be difficulties in accepting a diagnosis. Diagnosis and follow-up support sessions should be delivered at the individuals’ own pace. Local services should contribute to the resource pack. The information should be renewed regularly.
Information, services and the resource pack should meet the needs of the local community.
T1
T2
T3
Add patient to Quality and Outcomes Framework (QOF) register
Book annual review of physical, cognitive and mental state prescriptions and all medications
Review repeat prescriptions and all medication
If appropriate prescribe dementia medication
according to NICE guidelines
Post diagnostic information, support and counselling to person with dementia and their carer
Healthcare for London
36
Integrated car
e
pathway
14Mittelman et al. Improving caregiver well-being delays nursing home placement of patients with Alzheimer disease, 2006.
Neurology 67: 1592-1599
During the post-diagnosis period, a local multi-disciplinary dementia team will meet with the person with dementia and their carer, in order to devise a routine for that person which might include examining health issues (e.g. eyesight and hearing tests),
psychological wellbeing, exercise or interaction with social groups. This would also include consideration of home care assistance if necessary.
The carer’s assessment is as important to the process as the assessment for the person with dementia for ensuring the carer, who is often elderly, is able to provide the necessary care and support.
An example of this can be found in Mittelman14, where in a sample of 406 spouse carers’ there was a 28.3% reduction in the rate of nursing home placements where they received the combined intervention of individual, group and telephone counselling. It is worth noting that over 60% of the intervention’s beneficial impact was accounted for in terms of improvements in carers’ satisfaction with social support, their response to patient behavioural problems and improvements in their
demonstration of symptoms of depression.
T4
T5
Trigger initial care planning process and refer to
dementia adviser or other service to maintain contact within 12 weeks of diagnosis
Dementia services guide 37
Integrated car
e
pathway
W
15Oddy, R Age Concern England. Promoting Mobility for People with Dementia: a Problem Solving Approach, 2003 16http://www.hse.gov.uk/research/rrpdf/rr440.pdf
17http://www.psige.org/special_interest_challenging_behaviour.php
18Department of Health. Carers at the heart of 21st century families and communities: a caring system on your side, a life
of your own, 2008
The NICE-SCIE guidelines emphasise the importance of effective communication strategies in reducing the level of dependency of the person with dementia. It is recommended that commissioners and clinicians review examples of best practice outlined in the guidelines. There is evidence that written and pictorial
communication have an important role to play15.
Family carers may experience difficulty and be unable to continue to care for the person with dementia if they develop challenging behaviour. Previously the only option was to use medication to manage this type of behaviour. There are interventions to help with challenging behaviour such as Prevention and Management of Violence and Aggression (PMVA) trainers16. Professionals can help train carers, and speech and language therapists can provide advice to carers on how to better understand the communication needs of the person with dementia. The Newcastle Model17 provides a framework for understanding the cause of the person’s challenging behaviour and a process by which interventions are delivered.
Carers and family members should be made aware of the availability of local services to support them, such as respite care, peer support and the availability of carer grants and other provisions outlined in the Carers Strategy18. This is likely to vary considerably between boroughs and it should not be assumed that carers are aware of what is provided in their area. It is best practice that every borough should have access to an Admiral nurse.
W1
W2
Regular review of:
• cognition and mood state • medications in line with
NICE guidelines • accommodation and
environment
• patients’ support network • personal communication
needs
• previous interventions • personal support needs • end-of-life plan.
Carer and family
interventions for improving patient care:
• strategies for reducing expressed emotion • strategies for
communication
• systems therapy/family work
• strategies for managing challenging behaviour • provide reliable
information.