185-Perceptions
by
Parents:
Implications
for
Weight
Control
Intervention
Karen C.
Uzark,
RN,
PhD
Marshall H.
Becker, MPH,
PhD
T.E.
Dielman,
MA,
PhD
Albert P.
Rocchini,
MD
Victor
Katch,
EdD
Karen C. Uzark and Albert P. Rocchini are with the Division of Pediatric
Cardi-ology,
C.S. Mott Children’s Hospital,University
ofMichigan
Medical Center.Marshall H. Becker is with the Department of Health Behavior and Health Educa-tion,
University
ofMichigan
School of Public Health.TE Dielman is with the Department of
Postgraduate
Medicine,University
ofMichigan.
Victor Katch is with the Division of Physical Education, University of Michigan.
Address reprint requests to Karen C. Uzark, RN,
PhD,
Division of PediatricCardi-ology,
C.S. Mott Children’sHospital, University
ofMichigan,
AnnArbor,
MI 48109-0204.The study was
designed
toidentify
some of thepsychosocial
barriers tocompliance
in ahospital-based weight
control intervention program for adolescents. Forty obeseadolescents,
10 to 16 years of age, and their parents were surveyedprior
toparticipa-tion in a behavioral
change weight
control program at a majorteaching hospital.
Significant
correlations were obtained betweenweight
loss outcome and six factors. In obese adolescents,weight
loss wassignificantly
associated with their beliefsregarding:
(1) personal
control overweight, (2)
barriers ordifficulty
oflosing
weight,(3)
medicalproblems
as a cause of theirobesity, (4) family problems
as a cause of their obesity,and
(5) perceived
willingness offamily
members to diet. It issuggested
that greaterweight
loss in children whoperceived
morebarriers/difficulty
and lessfamily
willing-ness to diet may reflect theimportance
ofhaving
realisticexpectations
related to be-havioralcompliance.
Inaddition,
apositive parental
attitude orexpectation
that thechild was less
likely
to beoverweight
in the future was associated with greaterweight
loss
compliance.
Other parental healthbeliefs, however,
did notgenerally predict
the child’sweight
loss response to the intervention. Thefindings
lend support to thesig-nificance of the adolescent’s beliefs
regarding weight
andfamily
support inexplaining
weight
loss response to a behavioralchange
intervention program.Childhood
obesity
is aprevalent
healthproblem
associated with thedevelopment
ofconcluded
that,
aside from notsmoking,
&dquo;reduction ofoverweight
isprobably
themost
important
hygienic
measure ... available for the control of cardiovasculardis-ease&dquo;
(p.
140).~
Unfortunately,
data reveal that more than 80% of obese adolescentsbecome obese
adults,~ ’~
suggesting
that currentweight
control efforts for obese chil-dren are insufficientand/or
ineffective. While childhoodobesity
is a multifacetedproblem
affectedby
genetic,
physiologic,
social,
and economicvariableS.4
it is oftenthe direct result of
maladaptive
attitudes and behaviors which lead to over-consump-tionand/or
underactivity.
To understand and facilitatecompliance
with interventions directed atchanging
theeating
or exercise behaviors of obese children andadolescents,
it is necessary to examine the attitudes and beliefs which contribute to these be. haviors.Considerable research has been conducted on the
relationship
between the health beliefs and health-related behaviors of adults. A recent review of 46 studies relevant tothe Health Belief Model revealed that
&dquo;perceived
barriers&dquo; was the mostpowerful
health belief dimension across various
study designs
and behaviors ofadults.5
In astudy
of the model’sability
toexplain
andpredict
mothers’compliance
with adietary
regimen
for their obesechildren,
Becker andassociates’
foundsignificant
correlationsbetween
major
dimensions of the model andweight
loss. Researchby
Costanzo andWoody’
has also revealed thatparents’
preconceptions
about the nature of their child’sweight
problem
are influencedby
the sex of their children.Overweight
inboys
was seen as associated with less
exercise,
lessemotionality,
less socialinvolvement,
andpronounced
foodpreferences.
In contrast,greater
overweight
ingirls
was associatedwith
greater
influence of moods oneating,
moreparental
restraint ofeating,
moreemotionality,
and greater peerrejection.
It seems thatparents
of obesegirls
wererela-tively
more inclined to see the child’sobesity
behavior in terms ofproblematic
emo-tionally-driven
eating behavior,
and to assume an active role inrestraining
andredirect-ing
thatbehavior.’
In the
previously
citedstudy
which focused upon the mothers’ health motives andperceptions
aspredictors
of her child’sweight loss,
Becker etal.6
noted that mothers of older children were bettercompliers.
It wassuggested
that older children use theirextra control to adhere to the
diet,
possibly
in response to peer pressures and thesocial
desirability
oflosing weight. Perhaps
with older children and adolescents whohave somewhat greater control over their own
behavior,
there is moreopportunity
for their
personal
health beliefs to have animpact.
Natapoff8
reviewed considerableevidence
indicating
that children’s health beliefsbegin
to differentiate into a coherent belief system atapproximately
nine years of age, a time whichcorresponds
well withPiaget’s
concreteoperational
period.
Several studies have shown a stabilization of health beliefs around ten or eleven years ofage.9-’
Health is salient to manyadoles-cents 12
andGochman9
has shown that therelationship
between children’sperceptions
ofvulnerability
to health threats andpotential
health behavior was influencedby
thedegree
ofperceived
internal control and the salience of health to the child.While health beliefs are often
significant
predictors
of health behaviors in adultpopulations,
therelationship
between health beliefs andpreventive
health behaviors inyounger
populations
may be somewhatlimited. 11 ,13
This may be due to the amountof
parental
control and torelatively
less &dquo;future-orientation&dquo; whichonly gradually
increasesduring
later childhood and adolescence. Dielman andassociates&dquo;
found thattwo areas of children’s
preventive
healthbehavior, cigarette
smoking
andsnacking
lesser extent,
parental
health beliefs. While it issuggested
thatparental
health beliefsare a more distal
influence,
operating
via their influence onparental
behavior,
asig-nificant
relationship
wasreported
between theseparental
beliefs and the health beliefsof their children.
To understand adolescent
compliance
with a behavioralweight-control
interven-tion,
it isproposed
that thefollowing
important
psychosocial
factors be examined:parental
attitudes and beliefsregarding
health,
weight,
anddiet;
the obese adolescent’s attitudes and beliefsregarding
health,
weight,
anddiet;
andperceptions
orcharacteris-tics related to
family
support
of theweight-control
intervention.METHODS
This
prospective study
was conducted in the PediatricCardiology
Clinic at amajor
teaching hospital
over a two yearperiod
thatbegan
inApril,
1983. Datadescribing
the attitudes and beliefs of obese children and theirparents
were obtained inconjunction
with a
larger
researchproject
investigating
thephysiologic
effects of diet and exerciseon
weight
loss in obese children(NIH
No.AM30989).
Obesesubjects
were recruitedvia referral initiated
by
theparent, teacher,
physician,
nurse, or self in response to awritten notice
printed
in the local newspaper and mailed to local health care facilities.For admission to the program,
subjects
wererequired
tosatisfy
threeobesity
criteria:1) weight
forheight
and agegreater
than the 75thpercentile
of the HANES survey-U.S.Department
of Health, Education andWelfare.14
2)
triceps
andsubscapular
skin-fold thickness greater than the 80thpercentile
for ageby
HANEScriteria;
and3)
percent
fat greater than the 80thpercentile
for age. Consent was obtained from bothparent and child.
Sociodemographic
and otherobesity-relevant
characteristics of theparticipants
arepresented
in Table 1. Childrenranged
in age from 10 to 16 years(mean=13.1)
andwere without
physical
illness that wouldrequire drug therapy
or which wouldprohibit
dietary
restriction or exercise. Initialseverity
ofobesity ranged
from5%
to157%
overweight,
above the minimum admission criterion described for thisstudy.
Therewere 28
girls
and 12boys;
thesample
waspredominantly
Caucasian,
and six childrenlived with a
single
parent
(mother). Ninety-five
percent
of the children lived with atleast one
overweight
family
member.Twenty-five
(62.5%)
of the children hadprevi-ously
been on aweight-loss diet,
and 33(82.5%)
hadpreviously experienced parental
use of food as a reward.
Weight
Loss InterventionA behavior modification program was
implemented
to achieveweight
lossthrough
changes
ineating
and exercise behaviors.During weekly
one-hour groupsessions,
thechildren and adolescents learned about
good
nutrition,
moreappropriate
eating
andTable 1. Characteristics of Obese Children.
Accumulation of
points
coupled
withweight
loss was then converted to monetary reinforcersgiven
on aregular
schedule,
(e.g.,
200points
and fourpounds
lost wasworth
$1.50).
Separate meetings
were held with theparents
periodically
toprovide
nutrition education and
specific
instructions aboutreinforcement,
altering
the foodenvironment, and
maintaining
proper attitudes.The
dietary
component of this intervention program wasdesigned
toprovide
anacceptable dietary
pattern which contained the necessary nutrients topromote
growth
Design
and MeasuresBefore
participating
in theweight
loss intervention program, eachsubject
andhis/
herparent
were administered aquestionnaire
assessing
characteristics andbeliefs/per-ceptions
related to health,weight,
and diet. Thequestionnaire
was based on aninstru-ment
previously
utilizedby
Becker etal.6
Modifications in thewording
ofquestions
were necessary for
subject
interviews sinceonly
parents
had beensurveyed
in the earlierstudy.
Thequestionnaires
werepilot-tested
on a group of 18 obese adolescents and theirparents
who hadpreviously participated
in theweight
loss program. Furtheradjustments
were made wherequestions
were unclear orconfusing,
or where desiredinformation was not elicited
by
thequestion.
Mostquestions assessing
aparticular
belief or attitude were scored on a
six-point Likert-type
scale.Psychosocial
variables assessed included:perceived
threat ofobesity,
perceived
barriers ordifficulty
oflosing
weight, feelings
of control overweight, obesity
attribu-tions, and
family
support
network factors. Itemsrelating
to theperceived
threatposed
by obesity
were combined into an index. Ten itemsregarding
theperceived
severity
ofobesity
as well asperceived susceptibility
to, andseverity of,
the consequences ofobesity
were included. The index wascomprised
of &dquo;threat variables&dquo; which wereidentified as
predictive
ofweight
lossand/or
appointment-keeping
in thestudy by
Becker et
al .6
Withregard
to the internalconsistency
of theindex,
analysis
ofinter-item
reliability
yielded alpha
coefficients of 0.74 forparents
(N 40)
and 0.69 forchildren
(N 40).
&dquo;Perceived barriers&dquo; tocompliance
orweight
control was measuredby
the amount ofdifficulty
thesubject/parent
felt there was in order &dquo;to dosome-thing
tohelp
thisoverweight problem.&dquo;
Perception
ofpersonal
control overweight
was measuredby
amount ofagreement/disagreement
with the statesments&dquo;some-times no matter what you do, you can’t lose
weight&dquo;
and &dquo;there isn’t much anyonecan do about how much he
weighs&dquo; (r=0.418
forparents
and r=0.083 forchildren).
Each of elevenperceived
causes of, or reasons for.obesity
was also ratedby
thesubject/parent
toidentify
anyspecific
obesity
attribution ofsignificance.
Threeseparate dimensions of
family
support
were assessed: &dquo;instrumentalsupport,&dquo;
asmeas-ured
by
number of obesefamily
members(modeling)
andwillingness
offamily
mem-bers to diet as
perceived
by
thechild;
&dquo;emotionalsupport,&dquo;
as measuredby
thepro-portion
offamily
members the adolescentperceived
would encourageweight
lossefforts;
and &dquo;normative orappraisal
support.&dquo;
as measuredby
theparent’s
attitude orexpectation regarding
the child’sweight
control.Prior to the
intervention,
anthropometric
measurements were also obtained andin-cluded
weight, height,
skinfold measurements, andbody composition
determinations(by
hydrostatic
weighing). Weight
wassubsequently
measured at each behavior ther-apy sessionusing
a beam balance scale with thesubject
in street clothes and without shoes.Weights
were obtained and recordedby
a staff nurse in the clinic.Using
astabilometer,
height
wasagain
measured to the nearest 0.1 cmapproximately
20 weeksafter the intervention was initiated.
Subjects
whodropped
out of the intervention programprior
to 20 weeks wererequested
to return to the clinic for measurement atthat time. The last available
height
andweight
(at
16-19weeks)
was considered thepost intervention
(time 2)
measurement if a measure at 20 weeks could not beob-tained.
biological
variations in the response of individuals to diet andexercise,
it remains themost
important
outcome. The obesesubjects
were, of course,overweight
tovarying
extents, and were alsogrowing
inheight
at different rates. In anattempt
to achievesome standardization across
subjects,
thestudy’s
major
dependent
outcome variablewas the
change
inpercent
overweight (greater
than the 75thpercentile weight
forheight)
20 weeks after initiation of the intervention(time 2):
RESULTS
Health Beliefs
Associations between the health beliefs of the obese children and health beliefs of
their
parents
arepresented
in Table 2. Theonly
significant
positive
correlationbe-tween parents and children is with
respect
to beliefs about the threat ofobesity.
Bothparents
(X=4.44)
and obese children(X=4.04)
tended toreport
at least moderate levels of threat.However.
significant
negative
associations were found between the child’s beliefsregarding
the threat ofobesity
andparental perception
ofpersonal
control, andbe-tween the
parent’s perception
of barriers ordifficulty
and the child’sperception
ofpersonal
control overweight.
Children feel lesspersonal
control overweight
as theparents
perceive
more barriers related to management of the child’sweight problem.
’While there were nosignificant
correlations amongparental
health beliefs, it can be seen from Table 2 that for the child,perception
of the threat ofobesity
ispositively
associated with
perception
of barriers toweight
control andnegatively
associated withfeelings
ofpersonal
control overweight.
Children who viewobesity
as agreater
threat also tend toperceive
more barriers toweight
control and feelthey
have lesspersonal
control over theirweight problem.
There was no association, however, between be-liefs about barriers andperception
ofpersonal
control(or
previous
dietattempts).
Itis
interesting
that obese females tended toperceive
greater
barriers toweight
control than did malesubjects (t=1.75,
0.05<p < 0.1).
Associations between health beliefs and
compliance
orweight
loss outcome arepre-sented in Table 3. There was a
significant
association between the child’s beliefsregarding personal
control overweight
and theweight
loss outcome. Ashypothesized,
poor
weight
loss was related to decreasedfeelings
ofpersonal
control overweight.
There was also a
significant
pusitive
association between the child’s beliefsregarding
barriers or the
difficulty
oflosing weight
andweight
loss outcome. Obesesubjects
who felt it would be most difficult to control their
weight
were most successful. Since there was little variance in the threat measure in thissample,
this index did notdig-tinguish compliers
fromnoncompliers.
Noparental
health belief wassignificantly
associated with
weight
loss outcome.Clearly,
the child’s health beliefsregarding
Table 3. Correlations
(Pearson)
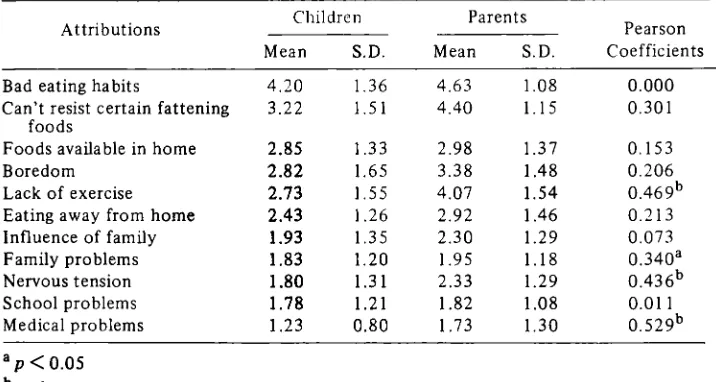
Between Health Beliefs and Outcome.Table 4. Mean Scores and Correlations Among
Obesity
Attributions of Children and Parents(Scale
values for attributions range from 1=not at all to6=completely.).
Attributions
Obese
subjects
and theirparents
rated 11possible
causes of the child’sobesity.
Mean scores and correlations between
obesity
attributions of the children andparents
arepresented
in Table 4. Bothparents
and childrenthought
thateating
behaviors,(i.e.,
badeating
habits andinability
to resist certainfattening foods),
were themajor
causes ofobesity.
Children were morelikely
thanparents
to rate thetypes
of foods available in the home as a cause of theirobesity
relative to otherpossible
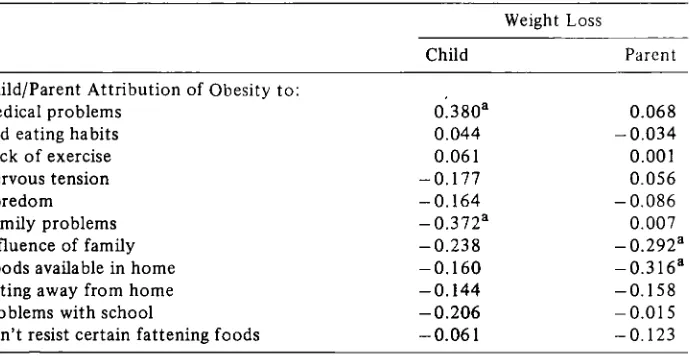
causes while [image:8.423.49.407.310.501.2]Table 5. Correlations
(Pearson)
BetweenObesity
Attributions and Outcome Measure.of obese
boys
andgirls,
parents
of femalesubjects
felt that lack of exercise(t=2.90,
p(0.01),
boredom(t=2.63, p=0.01)
andinability
to resist certainfattening
foods(t=2.13,
p <0.05)
were morelikely
causes of their child’sobesity.
There weresignifi-cant correlations between the
parent’s
and the child’s beliefs withrespect
to four ofthe eleven
obesity
attributions: lack ofexercise,
family
problems,
nervous tension, andmedical
problems. (Medical problems
were notgenerally regarded
by
eitherparents
orchildren, however,
as alikely
cause of theobesity.)
Other than the associationspre-sented in Table
4,
it is of interest that thehighest
correlation within beliefsregarding
attributions for bothparents
and children, was betweenfamily problems
and nervoustension,
with Pearson’s correlations of 0.637 for parents and 0.634 forchildren,
(p < 0.001).
Correlations between
obesity
attributions andweight
loss arepresented
in Table 5. While few children attributed theirobesity
to medicalproblems,
this attributionalbelief was
positively
associated withweight
loss outcome,contrary
to the directionhypothesized.
There was asignificant negative
association between the child’sattribu-tion of
obesity
tofamily problems
andweight
loss. It is of further interest that this attribution was found to bestrongly
correlated with thefrequency
offamily problems
(r=0.543,
p(O.001)
and,
aspreviously
mentioned,
with the attribution ofobesity
tonervous tension
(r=0.634, p(O.001)
which was alsohighly
correlated with thefre-quency of
family
problems
(r=0.596,
p(0.001).
Children who attributed theirobesity
to
family problems,
orperhaps family
stress, lost lessweight.
Parental attributions of their child’s
obesity
to the kinds of foods available in thehome,
and to the influence offamily
members,
werenegatively
associated withweight
loss outcome. These attributions also seem to be related to the
frequency
offamily
problems.
Additionalanalyses
reveal that attribution to the influence offamily
mem-bers is
positively
correlated with attribution tofamily problems (r=0.384, p=0.02),
with both attributions
positively
correlated with thefrequency
offamily problems
(r=0.364,
0.493,
p <0.03).
Poorweight
loss is related to theparent’s
perception
that bothfamily
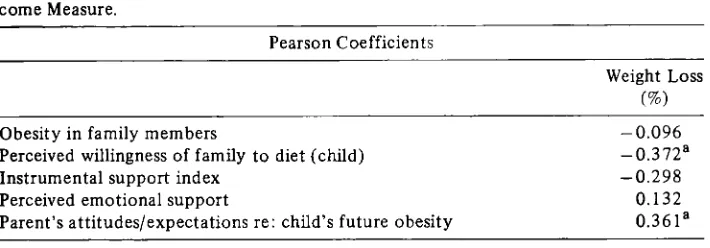
members and foods available in the home environment contribute to their [image:9.423.33.378.81.259.2]Table 6. Correlations Between
Family
Support Network Characteristics andOut-come Measure.
Family Support
NetworkRelationships
betweenfamily
support
network characteristics and thedependent
variable measures arepresented
in Table 6. Perceivedwillingness
offamily
to diet wasnegatively
associated withweight
losscompliance,
contrary
to the directionhypothe-sized.
Children
whoperceived
morewillingness
offamily
members to diet lost lessweight.
When this variable wasmultiplied
by
theproportion
of obesefamily
membersto create the instrumental
support
index,
the association withweight
loss was nolonger significant. (There
was nosignificant
correlation between thepreintervention
perceived
willingness
offamily
members to diet and theperceived willingness
offamily
members to dietfollowing
the intervention(N 25).)
There was also nosignificant
association between familial
obesity
andweight
losscompliance.
Emotional
support
fromfamily
members,
asperceived by
thechild,
was notsig-nificantly
correlatedwith
weight
loss.However,
weight
loss waspositively
associatedwith
theparental
belief
that their child was notlikely
to beoverweight
in the future(r=0.361),
p <0.05).
Children
ofparents
whoexpressed
apessimistic
orhopeless
attitude
regarding
their child’sobesity
lost lessweight,
and suchpessimism
was also associated withgreater familial
obesity
(r=-0.320,
p <0.05).
DISCUSSION
Bivariate
relationships
between theattitudes/beliefs
of obese childrenregarding
weight/diet
and somefamily
support
characteristics andsubsequent weight
lossout-come are summarized in Table 7. Based on this
study’s findings,
it can be concludedthat the health beliefs of obese adolescents are
important
factors in theexplanation
andprediction
ofweight
loss response to a behavioralchange weight
controlinterven-tion. In obese
children,
10 to 16 years of age,weight
loss wassignificantly
associatedwith their
perceptions
regarding:
(1) personal
control overweight,
(2)
barriers ordifficulty
oflosing weight,
(3)
medicalproblems
as a cause of theirobesity,
(4) family
problems
as a cause of theirobesity,
and(5)
willingness
offamily
members to diet. Ingeneral,
the child’sweight
loss response was notdirectly
correlated withparental
health
beliefs,
although
theparent’s
beliefs may have influenced the child’s [image:10.423.47.402.80.204.2]Table 7.
Summary
of BivariateRelationships
for Predictors ofWeight
LossAs
anticipated,
children enrolled in theweight
control intervention programre-garded obesity
as asignificant
threat tophysical
orpsychological well-being.
In thesechildren, perception
ofpersonal
control overweight
was asignificant
factor inweight
loss behavior. A
perception
ofpersonal
control overweight prior
toparticipation
in abehavioral
change
intervention mayfacilitate
weight
losscompliance.
The child’s control beliefs were not related to the child’s age or to the actualseverity
ofobesity.
Children whoseparents
perceived
greater
threat and more barriers toweight
control felt lesspersonal
control overweight. Perhaps
parents
who were more overwhelmedby
their child’sobesity
communicated these beliefs to their children andthereby
diminished the child’s
feelings
ofpersonal
control overhis/her weight.
Thissuggests
that
parental
beliefs may influence their children’sbeliefs.
Withrespect
to the child’sweight
lossbehavior, however,
the adolescent’spersonal
health belief wasclearly
amore
significant
factor inpredicting weight
loss outcome than theparent’s
health belief. Aspostulated
previously,
in older children who havegreater
control over their own behavior in anexpanded
socialenvironment,
there may be moreopportunity
forthe adolescent’s
personal
health beliefs to have animpact
on behavior.&dquo;Barriers,&dquo;
or theappraised difficulty
ofweight
control,
was anotherimportant
perception
of the obese adolescent related toweight
loss outcome. Their beliefsre-garding
barriershowever
did not appear to bedirectly
related to thebeliefs
of theirparents
or toprevious
dietattempts.
Obesechildren/adolescents
who felt it would bemore
difficult
to control theirweight
were most successful.Perhaps
this was relatedto their more accurate
expectations
regarding
their own role incompliance
with theweight
control
regimen.
Social forces direct manyoverweight
adolescents tofad
diets in the vainhope
ofachieving weight
loss without difficult diet restrictions or behaviorBandural
as the conviction that one cansuccessfully
execute the behaviorrequired
toproduce
the outcome. In a recent review of researchexploring
the role ofself-efficacy
in
achieving
health behaviorchange
among adults,self-efficacy
appeared
to be acon-sistent
predictor
of short-andlong-term
success for all health-related areas studied,including
weight
control.’
Furthermore, it wassuggested
thatself-efficacy
can beenhanced and that this enchancement is related to
subsequent
health behaviorchange.
Causalexplanations
ofobesity,
asperceived
by
the obese child, may also beimpor-tant factors
influencing weight
loss behavior. Consistent with thefindings
ofEdel-man.I7
obese childrenreported
badeating
habits as the mostlikely
cause of theirobesity.
Attributions ofobesity
to medicalproblems
and tofamily
problems
were,however, more
significant
predictors
ofweight
loss. Greaterweight
loss in childrenwho attributed their
obesity
to medicalproblems
may have been related to thesetting
in which the
weight
control intervention was offered. In ahospital-based
intervention program, theperceived
efficacy
of the intervention and thecredibility
of the source ofrecommendations may have been enhanced, thus
promoting
compliance.
This attribu-tional belief was alsostrongly supported
by
theirparents
who may have reinforcedconfidence in a
hospital-based
intervention.Poor
weight
loss outcome was associated with the obese child’s attribution ofhis/her obesity
tofamily problems.
In addition to thisimportant
longitudinal
relation-ship,
cross-sectionalanalyses
revealed that the child’s attribution of theirobesity
tofamily problems
was alsohiglly
correlated with the attribution ofobesity
to nervoustension, the
frequency
offamily
problems,
andparental
attribution ofobesity
tofamily
problems.
Thus, it appears thatfamily
stress may be animportant
factor in thetreatment of
obesity.
It has beensuggested
that childhoodobesity develops
even ininfancy
when food is used for relief of various states oftension, 18
and that laterobesity
may become a&dquo;padding&dquo; against
a hostile, homeenvironment.’
Overeating
has been included among emotion-focused
coping behaviors.2°
It is therefore under-standable that thespecific
attribution ofobesity
tofamily
problems
isnegatively
associated with
weight
loss,
especially
if alternativestrategies
formanaging
stress orcoping
withfamily
problems
are notprovided.
Additional
family-related
detrimental effects onweiglt
control may be seen inparental
attribution data. Poorweight
loss outcome was related to theparent’s
per-ception
that foods available in the home environmentand,
to a lesser extent,family
members, contributed to the child’sobesity.
Sinceparents
largely
control thequality
andquantity
of food in the home. this attributional belief suggests anunwillingness
to
provide
some environmental control for the obese child.Obesity
attributions ofparents also
suggest
thatparents
ofgirls
&dquo;blame,&dquo;
or attribute theobesity
to the adolescent’spersonal
behaviors-lack of exercise, boredom,inability
to resistfattening
foods-rather than onphysical
or environmental conditions. While these beliefs ofparents
were notdirectly
associated withweight
loss,they
may be related toparenting
’behaviors which diminished the adolescent’s
self-efficacy
beliefsregarding
weight
control.Among
thefamily
support dimensions assessed in thisstudy, only
normative orappraisal
support waspositively
correlated withweight
loss. Apositive parental
atti-tude or
expectation
that the child was lesslikely
to beoverweight
in the future wasassociated with
greater
weight
loss. Thisfamily
support variable did notrely
on the child’sperceptions
offamily
support or beliefs, and therefore isperhaps
a better,
and emotional support, responses of the obese children may have been biased
by
the desire to avoid embarrassment when socialsupport
fromfamily
waslacking.
Thesignificant
negative
association betweenwillingness
offamily
members to diet(as
perceived
by
thechild)
andweight
loss may reflect the child’shopes
or wishfulthink-ing prior
toparticipation
in the intervention program. Childrenliving
with other obesefamily
membersmight
expect
weight
control to be a desirablegoal
for their entirefamily.
Children who did notrely
onfamily
modeling
or environmentalsupport
seemto be more successful in
losing
weight, perhaps
again suggesting
theirgreater
feelings
ofself-efficacy.
Children who expect instrumental and normativesupport
fromparents
or
family
membersmight
benefit more from afamily-based
behavior modificationprogram as
suggested by
Epstein
andassociates.21
1CONCLUSIONS
In summary, our data
highlight
the roleplayed
by
the adolescent’s beliefsregarding
weight
andfamily
support
inpredicting weight
lossregimen
compliance.
For obeseadolescents,
weight
loss wassignificantly
associated with their beliefsregarding: (1)
personal
control overweight; (2)
&dquo;barriers&dquo; ordifficulty
oflosing weight;
(3)
medicalproblems
as a cause of theirobesity;
(4)
family problems
as a cause of theirobesity;
and
(5) perceived
willingness
offamily
members to diet. Inaddition,
&dquo;appraisal
sup-port&dquo;
(parental
expectation
that the child was lesslikely
to beoverweight
in thefuture)
was associated withgreater
weight
loss. Otherparental
healthbeliefs,
how-ever, did not
generally predict
the child’sweight
loss but may have influenced thechildren’s beliefs
regarding
weight
control.Based on these
findings,
several recommendations forenhancing
the effectiveness ofbehavioral
change weight
control interventions areproposed
for consideration:(1)
anassessment should be made of the attitudes and beliefs of the obese children and
parents,
especially
withregard
to theirobesity
attributions,
personal
controlpercep-tions,
and viewsconcerning
barriers toweight
control(this
information should be in-cluded in discussions with parents and children as a basis foridentifying
weight
controlneeds); (2)
anattempt
should be made to increasefeelings
of control overweight by
helping
adolescents to focus on behaviors that are alterable(it
may beespecially
important
to include education in thedevelopment
ofproblem-solving
skills and stressmanagement
techniques);
and(3)
in addition toinforming
parents
about nutrition and behavioralchange
strategies,
family
members may need education to enhancesup-portive
interactions in the adolescent’s social environment.References
1.
Kannel, WB, Gordon,
T:Physiological
and Medical concomitants ofobesity:
TheFramingham study.
In Bray G.(ed.), Obesity
in America. U.S.Department
of Health,Education,
andWelfare,
NIH Publication No.79-359,
1979.2. Charney, E,
Goodman,
HC, McBride, M, Lyon, B, Pratt R: Childhood antecedents of adult obesity. NewEngland
Journalof Medicine 295:6-9,
1976.4. LeBow, MD: Child Obesity-A New Frontier of Behavior
Therapy.
New York:Springer,
1984.5. Janz, NK and Becker MH: The health belief model: A decade later. Health Educa-tion
Quarterly
11:1-47, 1984.6. Becker, MH, Maiman, LA, Kirscht,
JP,
Haefner,DP,
Drachman RH: The healthbelief model and
prediction
of dietarycompliance:
A fieldexperiment.
Journalof
Health and Social Behavior18:348-366,
1977.7. Costanzo, PR Woody, EZ: Parental
perspectives
on obesity in children: Theim-portance of sex differences. Journal
of
Social and ClinicalPsychology 2:305-313,
1984.
8.
Natapoff,
JN: Adevelopmental analysis
of children’s ideas of health. Health Edu-cationQuarterly 9:34-45,
1982.9. Gochman D: Some correlates of children’s health beliefs and
potential
health be-havior. Journalof
Health and Social Behavior12:148-154,
1971.10. Lewis,
CE,
Lewis, MA, Lorimer, A, andPalmer,
BB: Child-initiated care: The useof school nursing services by children in an "adult free" system. Pediatrics 60:
499-507, 1977.
11.
Dielman, TE,
Leech, S, Becker,MH,
Rosenstock, I, Horvath, W, Radius, SM: Parental and child health beliefs and behavior. Health EducaionQuarterly
9:60-77,1982.
12.
Radius, SM, Dielman,
TE, Becker, MH,Rosenstock, IM,
Horvath, WJ: Adolescentperspectives
on health and illness. Adolescence15:375-384,
1980.13. Kegeles,
SS, Lund,
AK: Adolescents’ health beliefs and acceptance of a novelpre-ventive dental
activity: Replication
and extension. Health EducationQuarterly
9:96-112, 1982.
14. United States
Department
ofHealth,
Education and Welfare: NCHS Growth Curves for Children. (The HanesData)
Vital
and Health Statistics: Series11,
Publication No.
(PHS)
78-1650, 1977.15. Bandura, A:
Self-efficacy:
Toward aunifying
theory of behavioralchange.
Psy-chological Review 84:191-215, 1977.
16.
Strecher,
VJ,DeVellis,
BM, Becker, MH, Rosenstock, IM: The role ofself-efficacy
inachieving
health behaviorchange.
Health EducationQuarterly
13:73-92,1986.
17. Edelman B:
Developmental
differences in theconceptualization
ofobesity.
Jour-nal of American Dietetic Association
80:122-127,
1982.18. Bruch, H: Emotional aspects of
obesity
in children. Pediatric Annals4:91-99,
1975.19. Kornhaber, A, Kornhaber E:
Psychopathological
obesity types in children andtheir treatment. In
Collipp,
PJ(ed.),
ChildhoodObesity. Littleton,
PSGPublish-ing Company, Inc.,
1980.20.
Moos,
RH,Billings,
AG:Conceptualizing
andmeasuring coping
resources andprocesses. In
Goldberger,
L and Breznitz S(eds.),
Handbook of Stress: Theoreticaland Clinical Aspects. New York, Free Press, 1982.
21.
Epstein,
LH,Wing
RR, Koeske,R,
Andrasik, F, Ossip, DJ: Child and parentweight
loss infamily-based
behavior modification programs. Journalof
Consulting