0095-1137/11/$12.00 doi:10.1128/JCM.00012-11
Copyright © 2011, American Society for Microbiology. All Rights Reserved.
Comparison of Clinical and Analytical Performance of the Abbott
RealTime High Risk HPV Test to the Performance of Hybrid Capture
2 in Population-Based Cervical Cancer Screening
䌤
Mario Poljak,
1* Anja Osˇtrbenk,
1Katja Seme,
1Veronika Uc
ˇakar,
2Peter Hillemanns,
3Eda Vrtac
ˇnik Bokal,
4Nina Janc
ˇar,
4and Irena Klavs
2Institute of Microbiology and Immunology, Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia1; National Institute of
Public Health of Slovenia, Ljubljana, Slovenia2; Clinic of Obstetrics and Gynecology, Hannover Medical School, Hanover,
Germany3; and Department of Obstetrics and Gynecology, University Medical Centre Ljubljana, Ljubljana, Slovenia4
Received 4 January 2011/Returned for modification 23 February 2011/Accepted 14 March 2011
The clinical performance of the Abbott RealTime High Risk HPV (human papillomavirus) test (RealTime) and that of the Hybrid Capture 2 HPV DNA test (hc2) were prospectively compared in the population-based
cervical cancer screening setting. In women >30 years old (nⴝ3,129), the clinical sensitivity of RealTime for
detection of cervical intraepithelial neoplasia of grade 2 (CIN2) or worse (38 cases) and its clinical specificity for lesions of less than CIN2 (3,091 controls) were 100% and 93.3%, respectively, and those of hc2 were 97.4%
and 91.8%, respectively. A noninferiority score test showed that the clinical specificity (P< 0.0001) and clinical
sensitivity (Pⴝ0.011) of RealTime were noninferior to those of hc2 at the recommended thresholds of 98% and
90%. In the total study population (women 20 to 64 years old;nⴝ4,432; 57 cases, 4,375 controls), the clinical
sensitivity and specificity of RealTime were 98.2% and 89.5%, and those of hc2 were 94.7% and 87.7%, respectively. The analytical sensitivity and analytical specificity of RealTime in detecting targeted HPV types evaluated with the largest sample collection to date (4,479 samples) were 94.8% and 99.8%, and those of hc2 were 93.4% and 97.8%, respectively. Excellent analytical agreement between the two assays was obtained (kappa value, 0.84), while the analytical accuracy of RealTime was significantly higher than that of hc2. RealTime demonstrated high intralaboratory reproducibility and interlaboratory agreement with 500 samples retested 61 to 226 days after initial testing in two different laboratories. RealTime can be considered to be a
reliable and robust HPV assay clinically comparable to hc2 for the detection of CIN2ⴙlesions in a
population-based cervical cancer screening setting.
High-risk genotypes of human alpha papillomaviruses (hrHPV) are etiologically linked to virtually all cervical carci-nomas and their immediate precursors—high-grade cervical intraepithelial neoplasia (CIN) lesions (49). HPV DNA testing has therefore become an important part of cervical carcinoma screening and management algorithms in several countries (re-viewed in references 10 and 41). The four main clinical appli-cations of HPV DNA testing at present are (i) triage of women with equivocal screening cytology results in order to determine which patients should be referred for colposcopy, (ii) follow-up of women with abnormal screening cytology results who are negative at initial colposcopy/biopsy, (iii) prediction of the therapeutic outcome after treatment of high-grade CIN lesion, and (iv) primary screening of womenⱖ30 years old in combi-nation with the Pap smear to detect cervical cancer precursors (1, 3, 10–11, 13, 15).
Several in-house and more than 35 commercial assays for the detection of hrHPV are currently available (reviewed in references 11, 40, and 44). These assays have significantly dif-ferent clinical performance for high-grade CIN lesion detec-tion and are not necessarily useful for primary screening (21,
40). The Hybrid Capture 2 HPV DNA Test (hc2; Qiagen, Hilden, Germany) is the most frequently used diagnostic HPV assay worldwide and has been used in the majority of key trials that have proved the clinical value of hrHPV testing (summa-rized in references 10, 12–13, and 32). In order to assess suit-ability and facilitate the acceptance of novel hrHPV assays for primary cervical cancer screening, it has been recently recom-mended that candidate HPV assays should show clinical char-acteristics similar to those of hc2, i.e., clinical sensitivity, clin-ical specificity, and reproducibility, before they can be used for cervical cancer screening (32). Based on the reported clinical characteristics of hc2, the requirement has been set that the candidate assay should have a clinical sensitivity and clinical specificity for high-grade CIN or worse (CIN2⫹) of not less than 90% and 98% of those of hc2, respectively, in a popula-tion of women⬎30 years old (32). A candidate assay should be robust and display high intralaboratory reproducibility and in-terlaboratory agreement with a lower confidence boundary of not less than 87% (32). Stoler at al. recently proposed that any novel HPV assay intended for use in cervical screening should have a clinical sensitivity and clinical specificity for CIN3⫹of 92%⫾3% and at least 85%, respectively (46). The common idea behind all currently proposed recommendations is that a clinically useful HPV assay should achieve an optimal balance between clinical sensitivity and clinical specificity for detection of CIN2⫹in order to detect virtually all women with cervical cancer or immediate precursors and, at the same time, mini-* Corresponding author. Mailing address: Institute of Microbiology
and Immunology, Faculty of Medicine, University of Ljubljana Zalosˇka 4, 1000 Ljubljana, Slovenia. Phone: 386 1 543 7453. Fax: 386 1 543 7418. E-mail: [email protected].
䌤Published ahead of print on 23 March 2011.
1721
on May 16, 2020 by guest
http://jcm.asm.org/
mize redundant or excessive follow-up procedures for hrHPV-positive women with transient hrHPV infections and/or with-out cervical lesions (19, 27, 32, 46).
Several recent studies have clearly shown that a negative hrHPV result provides more reassurance against cervical precancerous lesions and cancer than a negative cervical cytology result and therefore safely permits longer intervals between screenings (4, 8, 12, 13, 16, 31, 33). However, among hrHPV-positive women, only a small proportion will have a concurrent clinically relevant disease, creating a di-lemma of how to identify the subset of women who require further immediate clinical attention, such as colposcopy (2, 8). One approach to improving the positive predictive value (PPV) for disease among hrHPV-positive women is the use of limited HPV genotyping for identification of the two most oncogenic HPV types, HPV16 and HPV18 (9, 26). A new generation of commercial assays that test for the most im-portant hrHPV types and, in addition, have the potential to separate cytologically negative/hrHPV-positive women at highest risk for CIN3⫹ (HPV16 or HPV18 positive) from those at lower risk (HPV16 and HPV18 negative) has been recently introduced (reviewed in reference 40).
One of the next-generation tests, the Abbott RealTime High Risk HPV test (RealTime; Abbott, Wiesbaden, Germany), detects a pool of 12 carcinogenic HPV genotypes in aggregate, with concurrent, separate detection of HPV16 and HPV18. The assay was launched in Europe in January 2009. In previous evaluations, RealTime demonstrated analytical specificity su-perior to that of hc2 and analytical sensitivity similar to that of hc2 (23, 39). The clinical sensitivity of RealTime for CIN2⫹ lesions in six published studies performed with different study populations was at least comparable to that of hc2 (14, 20, 22, 25, 39, 47). The clinical specificity and PPVs of RealTime and hc2 for either CIN2⫹ or CIN3⫹ in a triage of women with abnormal cervical cytology smears were comparable in one study (22), while RealTime performed slightly better in an-other study (14).
We present here the results of the first comparative evalu-ation of the clinical performance of RealTime and hc2 in the population-based cervical cancer screening setting. This study was primarily designed and statistically powered to determine the clinical specificity of RealTime for the detection of lesions of less than CIN2 in women⬎30 years old, although applicable data were also obtained related to the clinical sensitivity of RealTime for the detection of CIN2⫹lesions. In addition, the two HPV assays were compared for analytical performance with the largest sample collection to date (4,479 samples) and the first data on the intralaboratory reproducibility and inter-laboratory agreement of RealTime are provided.
MATERIALS AND METHODS
Study population and sample collection.During the period from December 2009 to August 2010, we prospectively enrolled all of the women attending the routine organized national cervical screening program within a network of 16 outpatient gynecology services with nationwide geographical coverage. In the Slovenian National Cervical Cancer Screening Program, which started in 2003, each woman between the ages 20 and 64 years is invited to have a preventive gynecological examination, together with a PAP smear once every 3 years (after two consecutive negative smears taken 1 year apart) (35). All smear and histology reports are gathered in a central database, which is linked to the Central Pop-ulation Registry. The present study (Slovenian HPV Prevalence Study) was
conducted in accordance with the Helsinki Declaration and was approved by the National Medical Ethics Committee at the Slovenian Ministry of Health. Women were eligible for inclusion if they were attending the routine organized Slovenian national cervical cancer screening program. The exclusion criteria were atten-dance for a gynecological examination after an atypical/abnormal cytology result, history of CIN of any grade or treatment for cervical disease in the preceding year, hysterectomy, and menstruation or pregnancy at presentation (36). A total of 34 gynecologists were responsible for patient recruitment and management. Written informed consent was obtained from all of the women by the pating gynecologists. Patient identities were kept secret from all study partici-pants except the participating gynecologists. During the gynecological examina-tion, the cervix was visually inspected and a sample was taken for routine cervical cytology by following the procedures normally used in each gynecological prac-tice. Samples were most often taken with a wooden or plastic spatula or with an endocervical brush, smeared onto a microscope slide, and spray fixed. In addition to this standard procedure at gynecological examination for cervical cancer screening, a second sample was obtained for HPV DNA testing with either a Cervex-Brush (Rovers Medical Devices, Oss, Netherlands) (in 87.6% of the cases) or a Pap Perfect Plastic Spatula and Cytobrash Plus GT Gentle Touch (Medscand sample collection kit; Medscand Medical, Berlin, Germany) (in 12.4% of the cases) and placed into ThinPrep PreservCyt solution (Hologic, Marlborough, MA). Coded ThinPrep vials and all accompanying data collection forms were transported to the laboratory on a weekly basis. Immediately on arrival at the laboratory, the specimens were split into several aliquots. The first two aliquots were used alternately for hc2 and RealTime testing, and the re-maining aliquots were stored at⫺70°C.
RealTime HPV testing.The RealTime assay was performed with the fully automated nucleic acid preparation instrumentm2000sp and the real-time PCR instrumentm2000rt (Abbott) by following the manufacturer’s instructions as previously described (20, 23). The assay uses four channels for the detection of fluorescent signals, one for the detection of an internal process control (136-bp region of human-globin) for sample adequacy and DNA extraction and am-plification, a second one for the detection of HPV16, a third for the detection of HPV18, and a fourth for the aggregate detection of the 12 HPV types, i.e., HPV31, HPV33, HPV35, HPV39, HPV45, HPV51, HPV52, HPV56, HPV58, HPV59, HPV66, and HPV68 (23). PCR amplification of HPV targets was achieved using a modified GP5⫹/6⫹primer mix consisting of three forward and two reverse primers (24). The assay cutoff is set at a fixed cycle threshold (CT)
value of 32. According to the manufacturer’s instructions, the assay was repeated with samples that showed initial invalid results for the internal control and additionally, at our discretion, with samples that showed some degree of HPV-specific positive amplification signal(s) but whoseCT values were above the
manufacturer’s fixed assay cutoff cycle and with samples that showed an initial HPV-negative result but had been defined as cases (CIN2⫹) during the evalu-ation of clinical performance.
hc2 HPV testing.hc2 is a hybridization assay designed for aggregate detection of 13 HPV types (HPV16, HPV18, HPV31, HPV33, HPV35, HPV39, HPV45, HPV51, HPV52, HPV56, HPV58, HPV59, and HPV68) using a mixture of unlabeled single-stranded full-genomic-length RNA probes (30, 37). Testing was performed by following the manufacturer’s instructions. Samples with a relative light unit per cutoff (RLU/CO) ratio higher than 2.50 were considered positive, and samples with an RLU/CO value of less than 1.00 were considered negative. According to the manufacturer’s instructions, all samples with RLU/CO ratios between 1.00 and 2.50 were retested and the results were interpreted according to the manufacturer’s instructions. Additionally, hc2 was repeated at our discre-tion with samples that showed borderline initial hc2 HPV-negative results (RLU/CO ratios of 0.80 to 0.99) and with samples that showed negative initial hc2 results but had been defined as cases (CIN2⫹) during the evaluation of clinical performance.
HPV genotyping and discordant analysis.To detect the HPV type(s) present in a sample, all samples with concordant positive RealTime/hc2 results and all samples with discordant results were additionally tested using the Linear Array HPV Genotyping Test (Linear Array; Roche Molecular Diagnostics, Branch-burg, NJ), which is capable of recognizing 36 different HPV types and 1 HPV subtype (including all 13 HPV types common to both assays, i.e., types targeted by both RealTime and hc2) by following the manufacturer’s instructions (45). Samples with a positive Linear Array HPV52 cross-reactive probe signal were additionally tested with an HPV52 type-specific real-time PCR assay as previ-ously described (29). All Linear Array HPV-negative samples and all samples in which no HPV types common to both assays were identified by Linear Array were additionally tested with the INNO-LiPA HPV Genotyping ExtraTest (Innogenetics, Ghent, Belgium), which is capable of recognizing 28 different alpha-HPV types (including all 13 types common to both assays) by following the
on May 16, 2020 by guest
http://jcm.asm.org/
manufacturer’s instructions. Finally, all INNO-LiPA HPV-negative samples and all samples in which no types common to both assays were identified by INNO-LiPA were tested using an in-house GP5⫹/GP6⫹PCR assay targeting a 150-bp fragment in the HPV L1 gene with additional HPV68-specific primers as previ-ously described (18, 34). Direct sequencing of the GP5⫹/GP6⫹PCR products with the same primers was used for genotyping as previously described (28). All HPV types identified by any of the genotyping tests were considered when interpreting the RealTime/hc2 discordant results. The analytical reliability of the applied three-step genotyping strategy was verified using the HPV DNA Profi-ciency 2010 Panel prepared by the World Health Organization HPV Laboratory Network (LabNet) (17). The panel consisted of 46 coded samples with a titration series of purified plasmids of 16 different HPV types (including all 13 types common to both assays), at levels ranging from 5 to 500 IU of HPV16 or HPV18 DNA and 5 to 500 genome equivalents of the other 14 HPV types. The geno-typing strategy used in this study showed 100% specificity and 100% sensitivity for a total of 72 HPV types present in 46 proficiency panel specimens.
Cytological examination.All cervical smears were examined under routine screening conditions by certified cytologists normally used by each participating gynecology practice who were blinded to HPV results.
Colposcopic referral. According to the criteria of the Slovenian National Cervical Cancer Screening Program, women were called for immediate colpos-copy using a cytology threshold of atypical squamous cells—cannot exclude high-grade lesion (ASC-H)/atypical glandular cells (AGC) or worse. In addition, irrespective of their cytology result, according to our study protocol, women were also invited for colposcopy if they were positive for HPV16 or HPV18. In women positive for hrHPV other than HPV16 and HPV18, immediate colposcopy was performed at the physician’s discretion; otherwise, the woman was invited to a control gynecological examination after 6 months to 1 year. Colposcopy was performed by certified colposcopists according to standard operating procedures, and the international nomenclature was used (48). During colposcopy, punch biopsy specimens were taken from any regions suspicious for CIN. No biopsy specimen was taken from women with normal colposcopy results, since this is considered unethical in Slovenia. The three-tier CIN nomenclature was used for biopsy classification, and the most severe abnormality was selected for final histopathological diagnosis. An expert histopathology system was used for his-topathological assessment: all biopsy specimens were first examined by a certified pathologist with more than 20 years of experience in gynecological pathology, followed by an independent, blinded histopathological review. In discrepant cases, the final diagnosis was the consensus reached by a panel of three pathol-ogists. Pathologists performing histopathological assessments were blinded to the HPV status but did have access to concurrent cytology results.
Intralaboratory reproducibility and interlaboratory agreement of RealTime. To assess RealTime intralaboratory reproducibility in time, a total of 500 sam-ples (167 randomly selected HPV-positive samsam-ples and 333 randomly selected HPV-negative samples) were retested after 61 to 226 days (median, 73 days) from initial testing, as recently recommended (32). In addition, two sets of coded 0.7-ml ThinPrep aliquots (2⫻500 samples) were prepared from the same 167 HPV-positive and 333 HPV-negative samples and shipped on dry ice to a col-laborative laboratory in Hannover, Germany, where two additional HPV testing rounds were performed. The results obtained were used to calculate intralabo-ratory reproducibility in time in the two participating laboratories, as well as interlaboratory agreement between the Ljubljana and Hannover laboratories. Reproducibility testing was performed using coded samples, and the technicians performing the assay in the two laboratories were completely blinded to the HPV status of the samples.
Statistical analysis.For assessment of the clinical performance of RealTime and hc2, we defined cases as women with high-grade cervical disease (CIN2⫹) and controls as women without high-grade cervical disease (less than CIN2). The clinical performance of the two assays was compared using a noninferiority score test, as recently recommended (32). The thresholds used for noninferiority were specificity for the detection of lesions less severe than CIN2 of at least 98% and sensitivity for the detection of CIN2⫹lesions of at least 90% relative to the results of hc2, as previously described (32). Since we enrolled more than 2,500 women⬎30 years old, for clinical specificity, the power of the study was more than 99% (32). The analytical performance of the two HPV assays was deter-mined against hrHPV status, which was defined by the concordance between RealTime and hc2 and, for discordant specimens, by genotyping results. Geno-typing results were designated hrHPV positive when at least 1 of the 13 HPV types common to both assays was detected, i.e., HPV16, HPV18, HPV31, HPV33, HPV35, HPV39, HPV45, HPV51, HPV52, HPV56, HPV58, HPV59, or HPV68. Sensitivity, specificity, negative predictive value (NPV), and PPV were calculated by using the conventional contingency tables, and 95% confidence intervals (95% CI) were computed using exact binomial methods. The level of
agreement between tests was assessed by the kappa statistics. The chi-square test was used for intercomparison of proportions. All statistical analyses were per-formed using R software version 2.12.0 (Free Software Foundation, Boston, MA). The level of statistical significance was set at a value of 0.05.
RESULTS
Between December 2009 and August 2010, 4,602 eligible women were invited to participate in this study, of which 88 (1.9%) declined to participate for various reasons. Seven women were excluded from the study due to ThinPrep sample spillage during transport (3 women) or missing ThinPrep sam-ples (4 women). HPV testing was thus finally performed using RealTime and hc2 for a total of 4,507 women.
RealTime was repeated with a total of 41 samples. The assay was repeated according to the manufacturer’s instructions for 10 samples due to initial invalid results for internal control; all 10 samples also had repeated invalid results and were excluded from the study. All excluded samples were repeatedly hc2 negative and were obtained from women who had normal cytology results. Of 30 samples that initially showed RealTime HPV-specific positive amplification butCT values that were
above the manufacturer’s fixed assay cutoff cycle and were repeated at our discretion, 8 turned out to be HPV positive after repeat testing and 22 again showed HPV-specific CT
values above the manufacturer’s cutoff. A single sample that showed an initial RealTime HPV-negative result but was de-fined as a case (CIN2⫹) during the evaluation of clinical per-formance (repeated at our discretion) was again RealTime HPV negative on repeat testing.
hc2 was repeated with a total of 137 samples. The test was repeated according to the manufacturer’s instructions with 101 samples due to an initial RLU/CO ratio between 1.00 and 2.50 (borderline HPV-positive results), among which 43 samples had to be retested twice. Of these 101 samples, after discordant analysis and HPV genotyping, 41 were finally considered to be analytically true positive by hc2 (the sample contained at least one targeted HPV type) and 60 were considered to be analyt-ically false positive by hc2 (no targeted HPV types were de-tected). All 101 women with initially borderline HPV-positive samples by hc2 were defined as controls (less than CIN2⫹) in the clinical performance assessment. Of 32 samples that showed borderline initial hc2 HPV-negative results (RLU/CO ratios between 0.80 and 0.99) and were repeat tested at our discretion, 7 turned out to be hc2 positive after repeat testing and 25 again had RLU/CO ratios below 1.00. Of the 4 samples that showed negative initial hc2 results but were defined as cases (CIN2⫹) during the evaluation of clinical performance and were retested at our discretion, 3 were again hc2 negative on repeat testing (initial RLU/CO ratios of 0.29, 0.42, and 0.55 and repeat RLU/CO ratios of 0.43, 0.74, and 0.73, respectively) and 1 turned out to be hc2 positive after repeat testing (initial RLU/CO ratio of 0.84, repeat RLU/CO ratio of 1.44).
Clinical performance of RealTime and hc2.Of 4,497 women
who had valid HPV results in both assays, 14 were excluded from the assessment of the clinical performance of RealTime and hc2 due to missing cytology results and 51 women eligible for colposcopy (according to the protocol criteria) were ex-cluded because they did not respond in time to repeated invi-tations for colposcopy or they refused colposcopy. The clinical
on May 16, 2020 by guest
http://jcm.asm.org/
performance of the HPV assays was finally assessed for a total of 4,432 women using two study groups, i.e., women⬎30 years old and all participating women (the numbers of womenⱕ29, 30 to 39, 40 to 49, 50 to 59, andⱖ60 years old were 1,304, 1,528, 976, 542, and 82, respectively).
Clinical performance of RealTime and hc2 for women >30
years old. Women ⬎30 years old represented our primary
study group for evaluation of the clinical performance of RealTime and hc2 (n⫽3,129 women; mean age, 41.5 years; median age, 40 years). The overall prevalences of HPV infec-tion in women⬎30 years old assessed by RealTime and hc2 were 7.8% (243/3,128; 95% confidence interval [CI], 6.9 to 8.8%) and 9.3% (290/3,128; 95% CI, 8.3 to 10.4%),
respec-tively, and the HPV prevalences in women with cytology results negative for intraepithelial lesion and malignancy (NILM) was 6.1% (180/2,974; 95% CI, 5.2 to 7.0%) and 7.4% (219/ 2,974; 95% CI, 6.5 to 8.4%), respectively. Table 1 shows the RealTime results for women⬎30 years old, stratified for cases and controls, in comparison to the hc2 findings. A total of 38 cases were identified among women⬎30 years old (18 CIN2 lesions, 16 CIN3 lesions, one carcinoma in situ, and three invasive carcinomas), and 3,091 women were classified as con-trols. The clinical sensitivity for the detection of CIN2⫹, clin-ical specificity for the detection of lesions less than CIN2, PPV, and NPV of RealTime and hc2 at RLU/CO cutoff values of 1.00 and 2.50 are shown in Table 2. The single CIN2⫹case missed by hc2 (at an RLU/CO cutoff value of 1.00) had RLU/CO values of 0.42 and 0.74 in initial and repeat hc2 testing, respectively. A noninferiority score test performed to determine whether the clinical specificity of RealTime for the detection of lesions less than CIN2 and the clinical sensitivity of RealTime for the detection of CIN2⫹lesions were noninferior to those of the hc2 (RLU/CO cutoff, 1.00) at recommended thresh-olds of 98% and 90% (32), respectively, showed that both the clinical specificity (P⬍0.0001) and clinical sensitivity (P⫽0.011) of RealTime were noninferior to those of hc2.
Clinical performance of RealTime and hc2 in the total study
population.The total study population represented our
[image:4.585.43.283.98.335.2]sec-ondary study group for evaluation of the clinical performance of RealTime and hc2 (n⫽4,432 women; mean age, 36.6 years; median age, 35 years). The overall prevalences of HPV infec-tion assessed by RealTime and hc2 were 11.6% (515/4,431; 95% CI, 10.7 to 12.6%) and 13.3% (589/4,431; 95% CI, 12.3 to 14.3%), respectively. The prevalences of HPV infection in women with NILM cytology assessed by RealTime and hc2 were 9.7% (411/4,217; 95% CI, 8.9 to 10.7%) and 11.2% (474/ 4,217; 95% CI, 10.3 to 12.2%), respectively. As shown in Table 1, a total of 57 cases were found in the total study population, i.e., 31 CIN2 lesions, 22 CIN3 lesions, one carcinomain situ, and three invasive carcinomas, and 4,375 women were classi-fied as controls. The clinical sensitivity, clinical specificity, PPV, and NPV of RealTime and hc2 at RLU/CO cutoff values of 1.00 and 2.50 are shown in Table 2. A noninferiority score test showed that both the clinical specificity (P⬍0.0001) and TABLE 1. Comparison of resolved RealTime and hc2 results
stratified for casesaand controlsbin 3,129 women⬎30 years old and the total study population of 4,432 women
Study group and RealTime result
No. (%) of samples tested by hc2
Negative Positive Total
Women⬎30 years old Controls
Negative 2,816 (91.1) 69 (2.2) 2,885 (93.3) Positive 21 (0.7) 185 (6.0) 206 (6.7) Total 2,837 (91.8) 254 (8.2) 3,091
Cases
Negative 0 (0.0) 0 (0.0) 0 (0)
Positive 1 (2.6) 37 (97.4) 38 (100.0)
Total 1 (2.6) 37 (97.4) 38
Total study population Controls
Negative 3,800 (86.9) 115 (2.6) 3,915 (89.5) Positive 39 (0.9) 421 (9.6) 460 (10.5) Total 3,839 (87.8) 536 (12.2) 4,375
Cases
Negative 1 (1.8) 0 (0.0) 1 (1.8)
Positive 2 (3.5) 54 (94.7) 56 (98.2)
Total 3 (5.3) 54 (94.7) 57
aDefined as having CIN2⫹lesions. bDefined as having lesions less than CIN2.
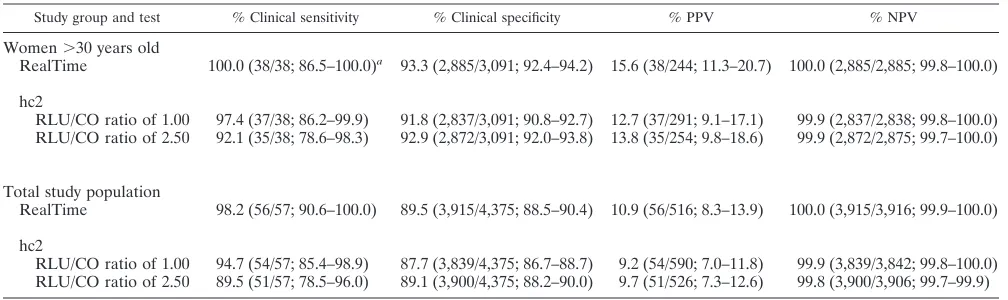
TABLE 2. Comparison of clinical sensitivity for the detection of CIN2⫹, clinical specificity for the detection of lesions less than CIN2, PPV, and NPV of RealTime and hc2 at RLU/CO cutoff values of 1.00 and 2.50 in women⬎30 years old and in the total study population
Study group and test % Clinical sensitivity % Clinical specificity % PPV % NPV
Women⬎30 years old
RealTime 100.0 (38/38; 86.5–100.0)a 93.3 (2,885/3,091; 92.4–94.2) 15.6 (38/244; 11.3–20.7) 100.0 (2,885/2,885; 99.8–100.0)
hc2
RLU/CO ratio of 1.00 97.4 (37/38; 86.2–99.9) 91.8 (2,837/3,091; 90.8–92.7) 12.7 (37/291; 9.1–17.1) 99.9 (2,837/2,838; 99.8–100.0) RLU/CO ratio of 2.50 92.1 (35/38; 78.6–98.3) 92.9 (2,872/3,091; 92.0–93.8) 13.8 (35/254; 9.8–18.6) 99.9 (2,872/2,875; 99.7–100.0)
Total study population
RealTime 98.2 (56/57; 90.6–100.0) 89.5 (3,915/4,375; 88.5–90.4) 10.9 (56/516; 8.3–13.9) 100.0 (3,915/3,916; 99.9–100.0)
hc2
RLU/CO ratio of 1.00 94.7 (54/57; 85.4–98.9) 87.7 (3,839/4,375; 86.7–88.7) 9.2 (54/590; 7.0–11.8) 99.9 (3,839/3,842; 99.8–100.0) RLU/CO ratio of 2.50 89.5 (51/57; 78.5–96.0) 89.1 (3,900/4,375; 88.2–90.0) 9.7 (51/526; 7.3–12.6) 99.8 (3,900/3,906; 99.7–99.9)
a
The values in parentheses are the number of samples/total; 95% CI.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.41.545.567.717.2]clinical sensitivity (P⫽0.015) of RealTime were also nonin-ferior to those of hc2 in the total study population.
Analytical performance of RealTime and hc2. Of 4,497
women who had valid HPV results in both assays, 18 were excluded from an assessment of analytical performance be-cause HPV genotyping showed the presence of HPV66 alone or in combination with other, nontargeted, HPV genotypes. All excluded HPV66-positive samples tested RealTime posi-tive, and 16 out of 18 samples tested hc2 positive (although HPV66 is not targeted by hc2). The analytical performance of the HPV assays was finally assessed with a total of 4,479 spec-imens. As shown in Table 3, after repeat hc2 testing of 101 samples according to the manufacturer’s instructions (initial results), excellent agreement between RealTime and hc2 was obtained with a kappa value of 0.83 (95% CI, 0.80 to 0.85) and a total agreement percentage of 96.0% (4,304/4,479; 95% CI, 95.5 to 96.6%). After repeat testing of 62 samples (30 samples by RealTime and 32 samples by hc2) at our discretion (re-solved results; see reasons for repeated testing in Materials and Methods), excellent agreement was obtained with a kappa value of 0.84 (95% CI, 0.82 to 0.87) and a total agreement percentage of 96.4% (4,319/4,479; 95% CI, 95.8 to 96.9%).
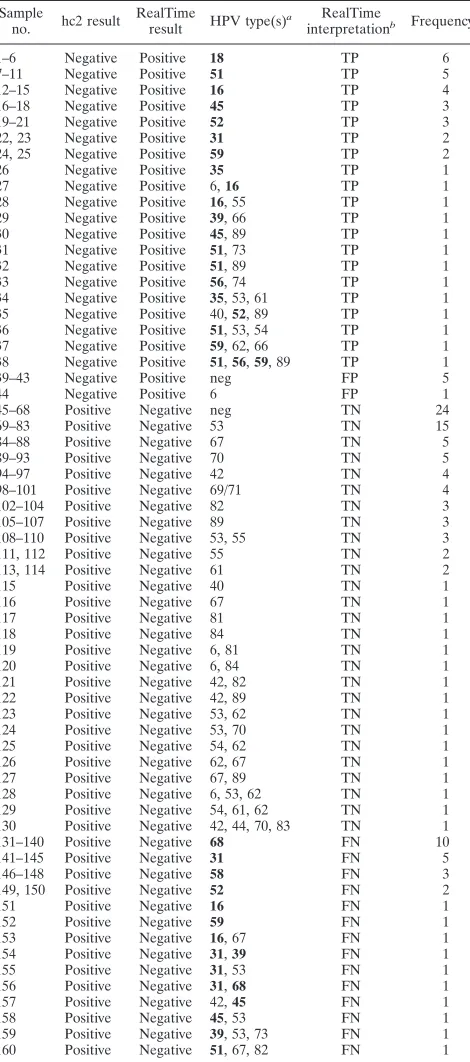
The HPV types determined in 160 samples with analytically discordant RealTime and hc2 results are presented in Table 4. Of the 44 samples detected by RealTime and not by hc2 (re-solved results), 38 were positive for at least one HPV type common to both assays and were considered to be analytically RealTime true positive/hc2 false negative. hc2 most frequently missed HPV51 (in nine samples), followed by HPV16 and HPV18 (in six samples each) (Table 4). Five RealTime-posi-tive/hc2-negative samples tested HPV DNA negative using all three broad-range PCR-based genotyping methods applied, and only low-risk HPV6 was found in one RealTime-positive/ hc2-negative sample. These six samples were considered to be analytically RealTime false-positive/hc2 true-negative samples. Of the 116 samples detected by hc2 and not by RealTime (resolved results), only nontargeted HPV types were identified in 62 samples and 24 samples tested HPV DNA negative by all three of the broad-range PCR-based genotyping methods ap-plied (Table 4). These 86 samples were considered to be ana-lytically hc2 false positive/RealTime true negative. The most frequently identified nontargeted HPV type causing an hc2
[image:5.585.303.538.91.622.2]false-positive result was HPV53 (in at least 15 samples), fol-lowed by HPV67 and HPV70 (in at least five samples each). In 30 RealTime-negative/hc2-positive samples, genotyping showed the presence of at least one HPV type common to both assays and these samples were considered to be analytically hc2 TABLE 3. Analytical results of testing for 13 assay-common HPV
types using RealTime and hc2 in 4,479 samplesa
Testing result
No. (%) of samples
Initial
results Resolved results
RealTime positive/hc2 positive 490 (10.9) 505 (11.2) RealTime negative/hc2 negative 3,814 (85.2) 3,814 (85.2) RealTime positive/hc2 negative 51 (1.1) 44 (1.0)b
RealTime negative/hc2 positive 124 (2.8) 116 (2.6)c
Total 4,479 4,479
aAfter repeat testing of 101 samples by hc2 according to the manufacturers’
instructions (initial results) and after repeat testing of 62 samples at our discre-tion (30 samples by RealTime and 32 samples by hc2) (resolved results).
b38 samples considered to be analytically RealTime true positive and 6
sam-ples considered to be RealTime false positive.
c86 samples considered to be analytically hc2 false positive and 30 samples
[image:5.585.42.282.91.182.2]considered to be hc2 true positive.
TABLE 4. HPV types determined in 160 analytically discordant samples based on resolved hc2/RealTime results
Sample
no. hc2 result
RealTime
result HPV type(s)
a RealTime
interpretationb Frequency
1–6 Negative Positive 18 TP 6
7–11 Negative Positive 51 TP 5
12–15 Negative Positive 16 TP 4
16–18 Negative Positive 45 TP 3
19–21 Negative Positive 52 TP 3
22, 23 Negative Positive 31 TP 2
24, 25 Negative Positive 59 TP 2
26 Negative Positive 35 TP 1
27 Negative Positive 6,16 TP 1
28 Negative Positive 16, 55 TP 1
29 Negative Positive 39, 66 TP 1
30 Negative Positive 45, 89 TP 1
31 Negative Positive 51, 73 TP 1
32 Negative Positive 51, 89 TP 1
33 Negative Positive 56, 74 TP 1
34 Negative Positive 35, 53, 61 TP 1
35 Negative Positive 40,52, 89 TP 1
36 Negative Positive 51, 53, 54 TP 1
37 Negative Positive 59, 62, 66 TP 1
38 Negative Positive 51,56,59, 89 TP 1
39–43 Negative Positive neg FP 5
44 Negative Positive 6 FP 1
45–68 Positive Negative neg TN 24
69–83 Positive Negative 53 TN 15
84–88 Positive Negative 67 TN 5
89–93 Positive Negative 70 TN 5
94–97 Positive Negative 42 TN 4
98–101 Positive Negative 69/71 TN 4
102–104 Positive Negative 82 TN 3
105–107 Positive Negative 89 TN 3
108–110 Positive Negative 53, 55 TN 3
111, 112 Positive Negative 55 TN 2
113, 114 Positive Negative 61 TN 2
115 Positive Negative 40 TN 1
116 Positive Negative 67 TN 1
117 Positive Negative 81 TN 1
118 Positive Negative 84 TN 1
119 Positive Negative 6, 81 TN 1
120 Positive Negative 6, 84 TN 1
121 Positive Negative 42, 82 TN 1
122 Positive Negative 42, 89 TN 1
123 Positive Negative 53, 62 TN 1
124 Positive Negative 53, 70 TN 1
125 Positive Negative 54, 62 TN 1
126 Positive Negative 62, 67 TN 1
127 Positive Negative 67, 89 TN 1
128 Positive Negative 6, 53, 62 TN 1
129 Positive Negative 54, 61, 62 TN 1
130 Positive Negative 42, 44, 70, 83 TN 1
131–140 Positive Negative 68 FN 10
141–145 Positive Negative 31 FN 5
146–148 Positive Negative 58 FN 3
149, 150 Positive Negative 52 FN 2
151 Positive Negative 16 FN 1
152 Positive Negative 59 FN 1
153 Positive Negative 16, 67 FN 1
154 Positive Negative 31,39 FN 1
155 Positive Negative 31, 53 FN 1
156 Positive Negative 31,68 FN 1
157 Positive Negative 42,45 FN 1
158 Positive Negative 45, 53 FN 1
159 Positive Negative 39, 53, 73 FN 1 160 Positive Negative 51, 67, 82 FN 1
a
HPV types common to both assays are in bold.
b
TP, true positive; FP, false positive; TN, true negative; FN, false negative.
on May 16, 2020 by guest
http://jcm.asm.org/
true positive/RealTime false negative. Of these 30 samples, 16 repeatedly showed some degree of RealTime HPV-specific amplification but theCTvalues were above the manufacturer’s fixed assay cutoff (32nd cycle) and 14 samples were RealTime HPV nonreactive. Among these RealTime-negative/hc2-posi-tive samples, RealTime most frequently missed HPV68 (in 10 samples).
Comparison of RealTime and hc2 results against resolved HPV status showed that the analytical sensitivity of RealTime was 94.8% (543/573; 95% CI, 92.6 to 96.4%) and its analytical specificity was 99.8% (3,900/3,906; 95% CI, 99.7 to 99.9%). By comparison, these analytical values for hc2 at an RLU/CO cutoff value of 1.00 were 93.4% (535/573; 95% CI, 91.0 to 95.3%) and 97.8% (3,820/3,906; 95% CI, 97.3 to 98.2%), re-spectively. The analytical accuracies of RealTime and hc2 in detecting 13 HPV types targeted by the two assays were 99.2% (4,443/4,479; 95% CI, 98.9 to 99.4%) and 97.2% (4,355/4,479; 95% CI, 96.7 to 97.7%), respectively; the values were signifi-cantly different (P ⬍ 0.0001). The analytical accuracies of RealTime in detecting HPV16 and HPV18 at the manufactur-er’s fixed assay cutoff (32nd cycle) were 99.8% (4,471/4,479; 95% CI, 99.6 to 99.9%) and 99.8% (4,473/4,479; 95% CI, 99.6 to 99.9%), respectively.
Intralaboratory reproducibility of RealTime. In Ljubljana,
there was excellent agreement between the overall RealTime HPV results of two rounds of testing, with a kappa value of 1.0 (95% CI, 0.98 to 1.0), a percentage of agreement of 100% (500/500; 95% CI, 99.0 to 100.0%), and a percentage of posi-tive agreement of 100% (167/167; 95% CI, 97.1 to 100.0%). After stratification of RealTime HPV-positive results into three categories (HPV16 positive, HPV18 positive, and posi-tive for the other 12 HPVs), the percentage of agreement was 99.0% (495/500; 95% CI, 97.5 to 99.6%), the percentage of positive agreement was 97.0% (162/167; 95% CI, 92.7 to 98.8%), and the kappa value was 0.98 (95% CI, 0.96 to 0.99). All HPV type-specific discordant results were obtained with samples containing several HPV types (mixed HPV infection); an additional HPV type(s) was detected in four samples in the second testing round (HPV18 3 times, other hrHPVs once) and in one sample in the first testing round (other hrHPVs).
In Hannover, there was also excellent agreement between overall RealTime HPV results of the two rounds of testing, with a kappa value of 0.99 (95% CI, 0.98 to 1.0), a percentage of agreement of 99.8% (499/500; 95% CI, 98.7 to 99.9%), and a percentage of positive agreement of 99.4% (166/167; 95% CI, 96.2 to 99.9%). One sample was positive for HPV16 in the first testing round (CT⫽30.21) and HPV negative in the second
but with HPV16-specific amplification near the cutoff (CT⫽
32.28). After stratification of RealTime HPV-positive results into three categories, the percentage of agreement was 99.0% (495/500; 95% CI, 97.5 to 99.6%), the percentage of positive agreement was 97.0% (162/167; 95% CI, 92.7 to 98.8%), and the kappa value was 0.98 (95% CI, 0.96 to 0.99). HPV type-specific discordant results were obtained with a total of five samples, in a previously described sample with a discordant HPV16 result and in four samples with mixed HPV infections; an additional HPV type(s) was detected in two samples in the first testing round (HPV18 once, other hrHPVs once) and in two samples in the second testing round (HPV18 twice).
Interlaboratory agreement of RealTime.There was excellent
agreement of overall HPV results between the Ljubljana and Hannover laboratories in the first and second testing rounds, with kappa values of 1.0 (95% CI, 0.98 to 1.0) and 0.99 (95% CI, 0.98 to 1.0), respectively, percentages of agreement of 100.0% (500/500; 95% CI, 99.0 to 100.0%) and 99.8% (499/ 500; 95% CI, 98.7 to 99.9%), respectively, and positive agree-ment percentages of 100.0% (167/167; 95% CI, 97.1 to 100.0%) and 99.4% (166/167; 95% CI, 96.2 to 99.9%), respec-tively. In the second testing round, one sample was positive for HPV16 in Ljubljana (CT⫽30.15) and HPV16 negative when tested in Hannover but with HPV16-specific amplification near the cutoff (CT⫽32.28). After stratification of RealTime HPV-positive results into three categories, in the first and second testing rounds, the percentages of agreement were 99.2% (496/ 500; 95% CI, 97.8 to 99.7%) and 98.2% (491/500; 95% CI, 96.4 to 99.1%), respectively, the percentages of positive agreement were 97.6% (163/167; 95% CI, 93.5 to 99.2%) and 94.6% (158/167; 95% CI, 89.7 to 97.3%), respectively, and the kappa values were 0.98 (95% CI, 0.96 to 0.99) and 0.96 (95% CI, 0.94 to 0.98), respectively. In the first testing round, all HPV type-specific discordant results were obtained with samples of mixed HPV infections; an additional HPV type(s) was detected in three samples in Ljubljana (HPV16 once, HPV18 twice) and in one sample in Hannover (other hrHPVs once). In the second testing round, HPV type-specific discordant results were ob-tained with a total of nine samples, i.e., in a previously de-scribed single sample with an HPV16 discordant result, in one sample in which different HPV types were detected (in Lju-bljana, HPV16; in Hannover, other hrHPVs), and in seven samples with mixed HPV infections; an additional HPV type(s) was detected in six samples in Ljubljana (HPV18 5 times, other hrHPVs once) and in one sample in Hannover (HPV18 once).
DISCUSSION
The most important consideration when evaluating an assay for routine detection of hrHPVs in cervical specimens is the clinical accuracy of the detection of high-grade cervical lesions (10, 27, 32, 46). A clinically useful hrHPV assay should have balanced clinical sensitivity and clinical specificity for CIN2⫹ lesions to ensure reliable detection of women with high-grade disease and to minimize HPV-positive results in those with minimal risk of disease (19, 32, 46). In recent years, it has become clear that many currently available commercial hrHPV assays are not very useful for primary cervical cancer screening, mainly as a result of misguided attempts to achieve perfect clinical sensitivity via increasing analytic sensitivity (27, 32, 40). Such analytically highly sensitive HPV assays, although capable of recognizing almost all women with underlying high-grade disease, usually yield a large number of clinically insignificant positive results, which cause unnecessary clinical follow-up, unnecessary diagnostic procedures, and unnecessary treatment of healthy women (27). In order to facilitate the evaluation and acceptance of novel hrHPV assays, guidelines describing re-quirements for the use of HPV assays for primary cervical cancer screening have recently been provided with European-North American collaboration (32). These guidelines recom-mend the use of a so-called clinical validation strategy, based
on May 16, 2020 by guest
http://jcm.asm.org/
on analysis of the equivalence of the result of the candidate hrHPV assay relative to that of an already clinically validated reference HPV assay such as hc2, with clinical samples that originate from a population-based cervical cancer screening, as assessed by the use of a noninferiority score test (21, 32). According to the guidelines, three characteristics of the can-didate hrHPV assay should be assessed during the clinical validation process by using predetermined thresholds of clini-cal sensitivity, cliniclini-cal specificity, and reproducibility (32).
RealTime is a recently launched next-generation HPV assay designed to detect a pool of 12 carcinogenic HPV genotypes in aggregate, with concurrent, separate detection of HPV16 and HPV18. In the past, the clinical performance of RealTime has been assessed with preselected archived cervical samples ob-tained from women with histologically confirmed high-grade cervical lesions (25, 39, 47) or in triage settings with cervical samples obtained from women with abnormal cytology re-ferred for colposcopy (14, 20, 22). The clinical sensitivity of RealTime for high-grade cervical lesions in these studies per-formed with a total of 1,481 histologically confirmed CIN2⫹ lesions was⬎96% in all six studies and noninferior to that of hc2 (14, 20, 22, 25, 39, 47). In the present study, we assessed, for the first time, the two remaining requirements for the use of RealTime for primary cervical cancer screening, i.e., clinical specificity for the detection of lesions less than CIN2 in women ⬎30 years old in the population-based primary cervical cancer screening setting and intralaboratory reproducibility/interlabo-ratory agreement. Although our study was designed and sta-tistically powered primarily to determine the clinical specificity of RealTime (with a power greater than 99%), applicable data relevant to the clinical sensitivity of RealTime were also ob-tained. In our primary study group for evaluation of the clinical performance of RealTime (3,128 women ⬎30 years old; 38 cases and 3,091 controls), both the clinical specificity of RealTime for the detection of lesions less than CIN2 and the clinical sensitivity of RealTime for the detection of CIN2⫹ lesions were noninferior to those of the clinically validated reference HPV assay (hc2) with the use of predetermined thresholds of 98% and 90% (specificity and sensitivity of RealTime relative to those of hc2), respectively. The favorable clinical performance of RealTime was also confirmed in our secondary study group (the total study population), which com-prised 4,432 women 20 to 64 years old (57 cases and 4,375 controls). Some previous studies have shown that hc2 might benefit from adjustment of the RLU/CO cutoff value to 2.0 to 2.5, which improved the clinical specificity and PPV of hc2 while the effect on clinical sensitivity was minimal (42–43). This was not confirmed in our study, since adjustment of the hc2 RLU/CO cutoff value from 1.00 to 2.5 resulted in a marginal improvement of the clinical specificity of hc2 but a substantial reduction of its clinical sensitivity. This was probably the result of a specific distribution of hc2 RLU/CO values among cases, i.e., three women with CIN2⫹had RLU/CO values between 1.00 and 2.00 (1.18, 1.44, and 1.67).
The clinical specificity of hc2 assessed in our study is in agreement with results obtained in similar previous studies. Recent meta-analysis of HPV primary screening trials thus showed a pooled clinical specificity of hc2 in North American and European trials of 91.3% (95% CI, 89.5 to 93.1%; range, 85 to 95%) (1, 32). In European HPV primary screening
stud-ies, the pooled clinical specificity of hc2 and GP5⫹/6⫹ PCR was 93.3% (95% CI, 92.9 to 93.6%) for women 35 to 49 years of age and 90.7% (95% CI, 90.4 to 91.1%) for all women (12). In recent trials, the clinical specificity of hc2 was 93.2% (95% CI, 92.8 to 93.6%) for women 35 to 60 years of age (41) and 94.1% (95% CI, 93.4 to 94.8%) for women 30 to 69 years of age (31). Due to the fact that the prevalence of hrHPV among Slovenian women is still relatively high in the 30- to 34-year-old age group (12.8% by Abbott; 14.4% by hc2), based on our results, HPV primary screening in our country would be fea-sible only if it started at the age of 35 years. Similar findings have also been recently described in other European countries (1, 12, 16, 41). The clinical specificity of the two HPV assays in our study improved substantially in women ⬎35 years old: RealTime had a clinical specificity of 94.4% (2,188/2,317; 95% CI, 93.4 to 95.3%), and hc2 had a clinical specificity at an RLU/CO cutoff value of 1.00 of 93.0% (2,154/2,317; 95% CI, 91.9 to 94.0%).
In addition to the assessment of clinical performance, six previously published RealTime evaluations have also assessed some analytical characteristics of the novel assay, mainly in comparison to hc2 (14, 20, 22, 25, 39, 47), and one study examined the analytical performance of RealTime in detail (23). In these seven studies, RealTime showed analytical sen-sitivity comparable to that of hc2 but superior analytical spec-ificity. These findings were also confirmed in the present study, in which the two HPV assays were compared for analytical performance with the largest sample collection to date (4,479 samples). Excellent analytical agreement between RealTime and hc2, with a kappa value of 0.84 and a total agreement of 96.4%, was obtained in our study, but the analytical accuracy of RealTime in detecting 13 HPV types common to both assays was significantly higher than that of hc2. A majority of 116 RealTime-negative/hc2-positive samples were considered to be analytically hc2 false positive, probably as a consequence of previously described hc2 probe cocktail cross-reactivity with untargeted HPV types (7, 38). Similarly to previous findings, the four most frequently identified nontargeted HPV types causing false-positive hc2 results in our study were HPV66, HPV53, HPV67, and HPV70. One-quarter of the RealTime-negative/hc2-positive samples were considered to be analyti-cally falsely RealTime negative; approximately half of these samples repeatedly showed some degree of RealTime HPV-specific amplification but with a cycle number beyond the assay cutoff, and approximately half of the samples were RealTime HPV nonreactive. RealTime most often missed HPV68, prob-ably due to the lower ability of the GP5⫹/6⫹ primer mix to detect the HPV68 prototype. This problem is not limited to GP5⫹/6⫹-based assays such as RealTime. PGMY primer-based assays such as Linear Array, designed to detect HPV68 subtype b, also cannot detect the HPV68 prototype because of several mismatches (34). HPV68 was the hrHPV type least commonly detected in the recent 2009 and 2010 HPV DNA proficiency panels prepared by LabNet; this HPV type was correctly identified by fewer than 38% of participating labora-tories (17). Of the 44 samples detected in our study by RealTime and not by hc2, 38 (86.3%) were considered to be analytically truly RealTime positive. hc2 most often missed HPV51, HPV16, and HPV18, probably due to the presence of low levels of the HPV target, which may not be reliably
on May 16, 2020 by guest
http://jcm.asm.org/
tected by hc2; i.e., approximately half of these samples had repeated hc2 RLU/CO values of 0.60 to 0.99. Five RealTime-positive/hc2-negative samples tested HPV DNA negative using all three broad-range PCR-based genotyping methods applied, and only low-risk HPV6 was found in one RealTime-positive/ hc2-negative sample. These six samples were considered to be analytically falsely RealTime positive; the most probable rea-son for false positivity was amplicon contamination (all sam-ples had lateCTs).
In the present study, the intralaboratory reproducibility and interlaboratory agreement of RealTime were assessed for the first time in two laboratories (Ljubljana and Hannover) by following the requirements set in guidelines for the evaluation of candidate HPV assays for cervical cancer screening (32). According to this document, intralaboratory reproducibility in time and interlaboratory agreement should be determined by the evaluation of at least 500 samples, 30% of which tested positive in a reference laboratory using a clinically validated assay. This should result in an agreement with a lower confi-dence boundary of not less than 87% (kappa value of at least 0.5 in this series of samples, including 30% positives), and the same intralaboratory reproducibility should be achieved after testing the same set of samples several weeks later. Our eval-uation showed that RealTime can be considered to be a reli-able and robust HPV assay, since intralaboratory and inter-laboratory kappa and agreement values exceeded those set in the recommendations and those obtained in similar previous evaluations of hc2 (5, 6). As expected, a majority of the oth-erwise infrequent HPV type-specific discordant RealTime re-sults were obtained in samples containing several HPV types (mixed HPV infection), probably due to amplification compe-tition. However, HPV type-specific discordant results did not influence the overall HPV positivity of RealTime, with the exception of a single sample in the Hannover laboratory, in which presumably the low quantity of HPV16 present in the sample produced discordant borderline positive and border-line negative results in the first and second testing rounds, respectively.
In summary, evaluation of RealTime in the population-based cervical cancer screening setting showed that the clinical performance of RealTime is not inferior to that of the clinically validated reference HPV assay hc2 for women⬎30 years old and women 20 to 64 years old. Excellent analytical agreement between RealTime and hc2 results was obtained while the analytical accuracy of RealTime was significantly higher than that of hc2. The typing information for HPV16 and HPV18 provided by RealTime could serve as a valuable additional tool in patient risk stratification and management. RealTime dis-played high intralaboratory reproducibility and interlaboratory agreement. According to our results and the results of previous studies, RealTime can be considered to be a reliable and ro-bust HPV assay clinically comparable to hc2 for the detection of CIN2⫹lesions in population-based cervical cancer screen-ing settscreen-ings.
ACKNOWLEDGMENTS
Abbott Molecular, the National Institute of Public Health of Slove-nia, and the Institute of Microbiology and Immunology, Faculty of Medicine, University of Ljubljana provided financial support for the assays and logistical conduct of this study.
Abbott Molecular was not involved in the study design, data collec-tion, data analysis and interpretacollec-tion, or writing the manuscript.
We thank clinical colleagues Petra Bavcˇar, Irena Begicˇ, Lara Besenicˇar Pregelj, Martina Bucˇar, Simona Cˇ opi, Petra Erzˇen Vrlicˇ, Andreja Gornjec, Mojca Grebenc, Mojca Jemec, Jozˇefa Kezˇar, Tat-jana Kodricˇ, Zdravka Koman, Jasna Kostanjsˇek, Jasna Kuhelj Recer, Zlatko Lazic´, Sonja Leposˇa, Mili Lomsˇek, Sladjana Malic´, Petra Meglicˇ, Maja Merkun, Aleksander Merlo, Anamarija Petek, Suzana Peternelj Marinsˇek, Igor Pirc, Ursˇula Resˇ Muravec, Filip Simoniti, Lucija Sorcˇ, Tina Steinbacher Kokalj, Mateja Darija Strah, Vesna S
ˇalamun, Ksenija Sˇelih Martinec, and Andrej Zore for patient recruit-ment and managerecruit-ment; Petra Markocˇicˇ for study management; Petra Cˇ uk, Robert Krosˇelj, Bosˇtjan J. Kocjan, and Mateja Jelen for excellent laboratory assistance; Jasna Sˇinkovec, Marja Lenart, and Bosˇtjan Lu-zar for cytology and histology review; Matthias Jentschke for repro-ducibility testing; Johannes Berkhof for help with noninferiority test calculations; and Miha Pirc for sample transportation.
REFERENCES
1.Arbyn, M., et al.2006. Chapter 9: clinical applications of HPV testing: a summary of meta-analyses. Vaccine24(Suppl. 3):S3/78–S3/89.
2.Arbyn, M., G. Ronco, J. Cuzick, N. Wentzensen, and P. E. Castle.2009. How to evaluate emerging technologies in cervical cancer screening? Int. J. Can-cer125:2489–2496.
3.Barzon, L., C. Giorgi, F. M. Buonaguro, G. Palu`, and Italian Society for Virology.2008. Guidelines of the Italian Society for Virology on HPV testing and vaccination for cervical cancer prevention. Infect. Agent Cancer3:14. 4.Bulkmans, N. W., et al.2007. Human papillomavirus DNA testing for the
detection of cervical intraepithelial neoplasia grade 3 and cancer: 5-year follow-up of a randomised controlled implementation trial. Lancet370: 1764–1772.
5.Carozzi, F. M., et al.2005. Reproducibility of HPV DNA testing by Hybrid Capture 2 in a screening setting. Am. J. Clin. Pathol.124:716–721. 6.Castle, P. E., et al.2004. Interlaboratory reliability of Hybrid Capture 2.
Am. J. Clin. Pathol.122:238–245.
7.Castle, P. E., et al.2008. Human papillomavirus genotype specificity of Hybrid Capture 2. J. Clin. Microbiol.46:2595–2604.
8.Castle, P. E., et al.2009. Short term persistence of human papillomavirus and risk of cervical precancer and cancer: population based cohort study. BMJ339:b2569.
9.Castle, P. E., et al.2009. Evaluation of a prototype real-time PCR assay for carcinogenic human papillomavirus (HPV) detection and simultaneous HPV genotype 16 (HPV16) and HPV18 genotyping. J. Clin. Microbiol.47:3344– 3347.
10.Cox, J. T.2009. History of the use of HPV testing in cervical screening and in the management of abnormal cervical screening results. J. Clin. Virol. 45(Suppl. 1):S3–S12.
11.Cuschieri, K. S., and H. A. Cubie.2005. The role of human papillomavirus testing in cervical screening. J. Clin. Virol.32(Suppl. 1):S34–S42. 12.Cuzick, J., et al.2006. Overview of the European and North American
studies on HPV testing in primary cervical cancer screening. Int. J. Cancer 119:1095–1101.
13.Cuzick, J., et al.2008. Overview of human papillomavirus-based and other novel options for cervical cancer screening in developed and developing countries. Vaccine26(Suppl. 10):K29–K41.
14.Cuzick, J., et al.2010. Performance of the Abbott RealTime high-risk HPV test in women with abnormal cervical cytology smears. J. Med. Virol.82: 1186–1191.
15.Desai, M. S., and H. A. Cubie.2005. The HPV test in cervical screening: a brave new world? Cytopathology16:3–6.
16.Dillner, J., et al.2008. Long term predictive values of cytology and human papillomavirus testing in cervical cancer screening: joint European cohort study. BMJ337:a1754.
17.Eklund, C., T. Zhou, J. Dillner, and WHO Human Papillomavirus Labora-tory Network.2010. Global proficiency study of human papillomavirus geno-typing. J. Clin. Microbiol.48:4147–4155.
18.Evans, M. F., C. S. Adamson, L. Simmons-Arnold, and K. Cooper.2005. Touchdown General Primer (GP5⫹/GP6⫹) PCR and optimized sample DNA concentration support the sensitive detection of human papillomavi-rus. BMC Clin. Pathol.5:10.
19.Gravitt, P. E., et al.2008. New technologies in cervical cancer screening. Vaccine26(Suppl. 10):K42–K52.
20.Halfon, P., et al.2010. Evaluation of the clinical performance of the Abbott RealTime High-Risk HPV for carcinogenic HPV detection. J. Clin. Virol. 48:246–250.
21.Hesselink, A. T., et al.2010. Comparison of the clinical performance of PapilloCheck human papillomavirus detection with that of the GP5⫹/6⫹-PCR-enzyme immunoassay in population-based cervical screening. J. Clin. Microbiol.48:797–801.
22.Huang, S., et al.2009. Clinical performance of Abbott RealTime High Risk
on May 16, 2020 by guest
http://jcm.asm.org/
HPV test for detection of high-grade cervical intraepithelial neoplasia in women with abnormal cytology. J. Clin. Virol.45(Suppl. 1):S19–S23. 23.Huang, S., et al.2009. Principles and analytical performance of Abbott
RealTime HR HPV test. J. Clin. Virol.45(Suppl. 1):S13–S17.
24.Jacobs, M. V., et al.1997. A general primer GP5⫹/GP6⫹-mediated PCR-enzyme immunoassay method for rapid detection of 14 high-risk and 6 low-risk human papillomavirus genotypes in cervical scrapings. J. Clin. Mi-crobiol.35:791–795.
25.Kaliterna, V., S. Z. Lepej, and A. Vince.2009. Comparison between the Abbott RealTime High Risk HPV assay and the Hybrid Capture 2 assay for detecting high-risk human papillomavirus DNA in cervical specimens. J. Med. Microbiol.58:1662–1663.
26.Khan, M. J., et al.2005. The elevated 10-year risk of cervical precancer and cancer in women with human papillomavirus (HPV) type 16 or 18 and the possible utility of type-specific HPV testing in clinical practice. J. Natl. Cancer Inst.97:1072–1079.
27.Kinney, W., M. H. Stoler, and P. E. Castle.2010. Special commentary: patient safety and the next generation of HPV DNA tests. Am. J. Clin. Pathol.134:193–199.
28.Kocjan, B. J., et al.2005. Distribution of human papillomavirus genotypes in plucked eyebrow hairs from Slovenian males with genital warts. Infect. Genet. Evol.5:255–259.
29.Kocjan, B. J., M. Poljak, and K. Seme.2010. Universal ProbeLibrary based real-time PCR assay for detection and confirmation of human papillomavi-rus genotype 52 infections. J. Virol. Methods163:492–494.
30.Lo¨rincz, A. T.1996. Hybrid Capture method for detection of human papil-lomavirus DNA in clinical specimens: a tool for clinical management of equivocal Pap smears and for population screening. J. Obstet. Gynaecol. Res.22:629–636.
31.Mayrand, M. H., et al.2007. Human papillomavirus DNA versus Papanico-laou screening tests for cervical cancer. N. Engl. J. Med.357:1579–1588. 32.Meijer, C. J., et al.2009. Guidelines for human papillomavirus DNA test
requirements for primary cervical cancer screening in women 30 years and older. Int. J. Cancer124:516–520.
33.Naucler, P., et al.2007. Human papillomavirus and Papanicolaou tests to screen for cervical cancer. N. Engl. J. Med.357:1589–1597.
34.Nazarenko, I., et al.2008. A novel method of HPV genotyping using Hybrid Capture sample preparation method combined with GP5⫹/6⫹PCR and multiplex detection on Luminex XMAP. J. Virol. Methods154:76–81. 35.Nicula, F. A., et al.2009. Challenges in starting organised screening
pro-grammes for cervical cancer in the new member states of the European Union. Eur. J. Cancer45:2679–2684.
36.Petry, K. U., et al.2003. Inclusion of HPV testing in routine cervical cancer screening for women above 29 years in Germany: results for 8466 patients. Br. J. Cancer88:1570–1577.
37.Poljak, M., A. Brencˇicˇ, K. Seme, A. Vince, and I. J. Marin.1999. Compar-ative evaluation of first- and second-generation Digene Hybrid Capture assays for detection of human papillomaviruses associated with high or intermediate risk for cervical cancer. J. Clin. Microbiol.37:796–797. 38.Poljak, M., I. J. Marin, K. Seme, and A. Vince.2002. Hybrid Capture II HPV
test detects at least 15 human papillomavirus genotypes not included in its current high risk cocktail. J. Clin. Virol.25(Suppl. 3):S89–S97.
39.Poljak, M., et al.2009. The Abbott RealTime High Risk HPV test: compar-ative evaluation of analytical specificity and clinical sensitivity for cervical carcinoma and CIN 3 lesions with the Hybrid Capture 2 HPV DNA test. Acta Dermatovenerol. Alp. Panonica Adriat.18:94–103.
40.Poljak, M., and B. J. Kocjan.2010. Commercially available assays for mul-tiplex detection of alpha human papillomaviruses. Expert Rev. Anti Infect. Ther.8:1139–1162.
41.Ronco, G., et al. 2009. Process performance of cervical screening pro-grammes in Europe. Eur. J. Cancer45:2659–2670.
42.Sargent, A., et al.2010. Optimal threshold for a positive hybrid capture 2 test for detection of human papillomavirus: data from the ARTISTIC trial. J. Clin. Microbiol.48:554–558.
43.Seme, K., K. Fujs, B. J. Kocjan, and M. Poljak.2006. Resolving repeatedly borderline results of Hybrid Capture 2 HPV DNA test using polymerase chain reaction and genotyping. J. Virol. Methods134:252–256.
44.Snijders, P. J., D. A. Heideman, and C. J. Meijer.2010. Methods for HPV detection in exfoliated cell and tissue specimens. APMIS118:520–528. 45.Stevens, M. P., S. M. Garland, and S. N. Tabrizi.2006. Human
papilloma-virus genotyping using a modified linear array detection protocol. J. Virol. Methods135:124–126.
46.Stoler, M. H., P. E. Castle, D. Solomon, and M. Schiffman.2007. The expanded use of HPV testing in gynecologic practice per ASCCP-guided management requires the use of well-validated assays. Am. J. Clin. Pathol. 127:335–337.
47.Tang, N., et al.2009. High-risk HPV detection and concurrent HPV 16 and 18 typing with Abbott RealTime High Risk HPV test. J. Clin. Virol. 45(Suppl. 1):S25–S29.
48.Walker, P., et al.2003. International terminology of colposcopy: an updated report from the International Federation for Cervical Pathology and Col-poscopy. Obstet. Gynecol.101:175–177.
49.zur Hausen, H.2009. Papillomaviruses in the causation of human cancers—a brief historical account. Virology384:260–265.