Copyright © 1999, American Society for Microbiology. All Rights Reserved.
Prospective Comparison of Whole-Blood- and Plasma-Based Hepatitis
C Virus RNA Detection Systems: Improved Detection Using
Whole Blood as the Source of Viral RNA
JACK T. STAPLETON,1,2* DONNA KLINZMAN,1WARREN N. SCHMIDT,1,2MICHAEL A. PFALLER,3
PING WU,1,2† DOUGLAS R. LABRECQUE,1,2JIAN-QIU HAN,1,2‡ MARY JEANNE PERINO PHILLIPS,2
ROBERT WOOLSON,4ANDBETH ALDEN3
Veterans Administration Medical Center, Iowa City, Iowa 52246,1and Departments of Internal Medicine,2Pathology,3 and Preventive Medicine,4University of Iowa College of Medicine, Iowa City, Iowa 52242
Received 22 September 1998/Returned for modification 9 November 1998/Accepted 30 November 1998
We previously demonstrated that whole blood contains significantly more hepatitis C virus (HCV) RNA than plasma. To validate the whole-blood-based HCV RNA detection method, a prospective comparison of HCV RNA detection in whole blood and plasma from 50 patients with chronic liver disease was undertaken. Whole-blood and plasma aliquots were independently tested for HCV RNA by reverse transcriptase (RT) PCR assay, and plasma was tested by the Roche Amplicor assay. HCV RNA was detected in 35 of 50 (70%)
whole-blood samples by RT-PCR but in only 26 of 50 (52%) plasma samples tested by the Amplicor assay (P<
0.01). HCV RNA was detected in 85% of HCV antibody-positive patients by the whole-blood method compared with 74% of plasma samples by the Amplicor method. The five HCV antibody-positive subjects who were negative by whole-blood-based RT-PCR assay were all receiving interferon therapy and had normal transami-nases at the time of testing. HCV RNA was detected in 38% of HCV antibody-negative subjects by the
whole-blood-based RT-PCR assay compared with 6.25% of these patients by the Amplicor assay (P< 0.05).
There were nine samples in which HCV RNA was detected in whole blood but the Amplicor test was negative. Eight of the nine RNAs prepared from these whole-blood samples tested positive in the Amplicor assay, thus confirming the specificity of our results. This study demonstrates that whole-blood-based HCV RNA detection is more sensitive than currently available commercial tests and that whole-blood RNA is suitable for use in commercial assays.
Hepatitis C virus (HCV) is a hepatotropic RNA virus re-sponsible for the majority of cases of posttransfusion and com-munity-acquired chronic non-A, non-B hepatitis in the United States (4, 5). It causes persistent infection in more than 90% of infected people, and up to 70% of these individuals develop progressive liver disease over a 20- to 30-year period (18, 34). An estimated 3.9 million people in the United States are cur-rently infected with HCV, and it is the leading etiology of end stage liver disease resulting in liver transplantation in the United States (3, 9).
HCV was originally identified by cloning RNA from the liver of a chimpanzee with chronic non-A, non-B hepatitis, express-ing the cDNA, and identifyexpress-ing cross-reactive antibodies in the original animal serum and in sera from well-characterized hu-man patients with non-A, non-B hepatitis (5, 8, 27). Commer-cial immunoassays were subsequently developed to detect an-tibodies against structural and nonstructural viral proteins (10, 25, 38), and later improvements have increased the sensitivity and positive predictive value of HCV antibody testing (1, 7, 16, 22, 24, 26, 41).
Although current immunoassays are successful in detecting most cases of chronic HCV infection, a significant percentage
of antibody-negative individuals (up to 5% of blood donors with elevated alanine aminotransferase levels) test positive for HCV RNA by serum or plasma nucleic acid amplification methods (4, 36, 39, 44). Our laboratory developed a method to detect HCV RNA in whole blood by using a cationic surfactant (Catrimox-14) to precipitate RNA from whole blood (30). We found that the amount of HCV RNA in whole blood was significantly higher than that present in plasma, and that plas-ma-based assays significantly underestimate the circulating HCV viral load (31, 33). Using this whole-blood-based HCV RNA detection system in patients from our liver clinic popu-lation, we found that the majority of people with unexplained chronic liver disease and negative HCV antibody tests were actually infected with HCV (32). Dries et al. recently con-firmed our findings in another population of chronic liver dis-ease patients (12). These investigators evaluated liver biopsy specimens from 44 patients with chronic, HCV antibody-negative liver disease and found that 61% of the specimens contained HCV RNA (12). These serosilent HCV infections probably contribute to the small-but-persistent risk of post-transfusion and community-acquired HCV infection.
We evaluated the distribution of HCV RNA among plasma and various cellular compartments in peripheral blood and determined that blood contains significantly more viral RNA than adjusted equivalent volumes of plasma or blood cells (33). Thus, measurement of whole-blood HCV RNA appeared to be more sensitive than measuring plasma HCV RNA (12, 33, 40). There are several potential reasons why whole-blood RNA contains a higher concentration of HCV than plasma. Al-though there are conflicting data regarding the replication of HCV in any of these cell types (6, 14, 19–21, 23), HCV RNA * Corresponding author. Mailing address: University of Iowa
Hos-pitals and Clinics, Department of Internal Medicine, SW 54 GH, 200 Hawkins Dr., UIHC, Iowa City, IA 52242. Phone: (319) 356-3168. Fax: (319) 356-4600. E-mail: [email protected].
† Present address: Shanghai RAAS Blood Product Co., Ltd., Shang-hai, People’s Republic of China.
‡ Present address: Shanghai Institute of Biological Products, Shang-hai 200052, People’s Republic of China.
484
on May 15, 2020 by guest
http://jcm.asm.org/
is present among circulating lymphocytes, neutrophils, and monocytes and in the erythrocyte-platelet pellet (33). We pre-dicted that the increased HCV RNA concentration was due to the addition of cell-associated HCV to plasma in the whole-blood preparation; however, we found that the intracellular HCV RNA accounted for only approximately half of the ad-ditional HCV RNA in the cell pellet (33). The remaining HCV RNA was removed by extensive washing of the cell pellet. Thus, we speculated that this cell-associated HCV RNA results from HCV-lipoproteins or HCV-immunoglobulin complexes that precipitate during plasma preparation (17, 33, 37).
The purpose of this study was to further validate our findings that whole-blood-based HCV RNA detection is more sensitive than plasma-based HCV RNA detection, to directly compare whole-blood-based HCV RNA detection with a widely used and validated commercial assay, and to determine if commer-cial assays can confirm the finding of HCV RNA in the whole blood of patients who are HCV antibody negative. To accom-plish this, we prospectively studied HCV antibody-positive and HCV antibody-negative patients with chronic liver disease. We then directly compared the use of whole-blood- and plasma-based HCV RNA detection systems with a commercial HCV reverse transcriptase (RT) PCR method. Our results confirm the increased sensitivity of whole-blood-based HCV RNA de-tection relative to plasma-based and commercial methods and demonstrate the feasibility of utilizing whole-blood RNA in currently available commercial assays.
MATERIALS AND METHODS
Patients and sample collection.Subjects with chronic liver disease followed by the University of Iowa Liver Clinic were invited to participate in this study. All patients had previously been tested for antibody to HCV, and subjects were selected for recruitment by using a ratio of two antibody-positive patients for each HCV antibody-negative subject. Chart review revealed that none of the patients were organ transplant recipients or clinically immunosuppressed due to known congenital or acquired immune deficiencies or medications. Five patients were receiving interferon therapy for chronic HCV infection at the time of blood sampling. These subjects had received 3 million units thrice weekly for more than 2 months at the time of sampling, and their serum transaminases were normal. In subjects who had previously undergone percutaneous liver biopsy, the original interpretation of the histopathologic findings was used for analysis in this study. Whole blood (anticoagulated with acid citrate dextrose) was collected as previously described and processed within 2 hours of collection (30, 33, 43). The samples were assigned code numbers, and HCV RNA testing was completed with laboratory personnel blinded to subject identity and HCV antibody status. Five 200-ml aliquots of whole blood were each mixed with 1.0 ml of Catrimox reagent prior to plasma separation (6003g; 10 min at 4°C) (30). Aliquots of plasma, plasma added to Catrimox (200ml to 1.0 ml), and whole blood plus Catrimox were frozen at280°C (30, 32). Plasma instead of serum was chosen for comparison with whole blood because it could be prepared from the sample of citrated whole blood, thus allowing direct comparison of whole blood and plasma from the same sample tube. In addition, plasma is specified by the Amplicor assay, and like others (28, 32, 33), we found that plasma-based HCV RNA testing was as sensitive or slightly better than serum-based HCV RNA testing (data not shown). The study was approved by the University of Iowa Institutional Review Board (Committee A), and informed consent was obtained from each patient.
RNA extraction and HCV RT-PCR assays.RNA was prepared from the Catrimox precipitate as previously described (30, 33). Briefly, the Catrimox-RNA precipitate was washed twice with diethyl pyrocarbonate-treated H2O and
ex-tracted with acid-buffered phenol and 4 M guanidinium isothiocyanate reagent. Following ethanol precipitation, whole-blood and plasma RNAs were amplified by our in-house method, which employs nested oligonucleotide primers derived from the highly conserved 59 nontranslated region (NTR) of the virus (30). Unless noted otherwise, 25% of the initial whole-blood or plasma sample was used in the RT-PCR. Thus, the RNA template represented the amount of RNA present in 50ml of the original whole-blood or plasma sample. Amplification conditions were not changed from those previously described (30, 32, 33). DNA products (250 bp) were detected by ethidium bromide following electrophoresis on a 1.5% agarose gel (30). The lower limit of detection of HCV RNA in our whole-blood assay was approximately 240 genome equivalents/ml of plasma, as previously described (33).
Rigorous standardization of reagents, sample preparation, and thermocycling parameters were employed to control for known variations in PCR efficiency (11, 29, 30, 32, 33). All RNA samples were assayed with the same RT-PCR reagent
mix, and plasma and whole-blood specimens from the same blood sample were always evaluated together. A positive control sample was evaluated in each assay, and two negative control preparations consisting of no template (water) and known HCV RNA-negative plasma samples were also evaluated to assess con-tamination.
Commercial HCV RNA assays.The Amplicor HCV test was used in these studies as recommended by the manufacturer (Roche Diagnostic Systems, Branchburg, N.Y.). RNA was prepared from the frozen plasma aliquots as recommended. The assay uses 50ml of a 1:10 dilution of RNA extracted from 100
ml of plasma, thus representing 5ml of the initial plasma sample. The Roche Amplicor test utilizes primers from the HCV 59 NTR to amplify the HCV genome in RT-PCRs. The negative sense primer is biotinylated, and amplicons are captured on HCV-specific oligonucleotide primers bound to the wells of microtiter plates. Detection of HCV amplicons is done with a primer-specific avidin-horseradish peroxidase conjugate, with subsequent determination of ab-sorbance following incubation with substrate provided by the manufacturer. Positive and negative control samples provided by the manufacturer were in-cluded as recommended. A single technician qualified by Roche in the perfor-mance of the Amplicor HCV RNA test system carried out the tests in this study. The average limit of detection of the Amplicor test is;200 genome equiva-lents/ml of plasma.
Cloning and sequence analysis of PCR products.Where indicated, PCR prod-ucts were separated by agarose gel electrophoresis, visualized by ethidium bro-mide staining, excised, and purified with the Promega (Madison, Wis.) DNA purification system kit. The fragments were ligated into [email protected] (Original TA cloning kit; Invitrogen, Carlsbad, Calif.), and plasmid DNA was sequenced with primers complementary to the T7 polymerase or the M13 universal primer sequences present in the vector. Automated fluorescent dye terminator cycle sequencing was performed by the University of Iowa DNA Core Facility (DNA automatic sequencer model 373A; Applied Biosystems, Foster City, Calif.). Us-ing the sequences obtained and additional published sequences, we constructed phylogenetic trees to clarify the relationships between the HCV isolates and our laboratory positive control specimen. Nucleotide sequences were aligned, and the computed distances were used to construct phylogenetic trees by using the neighbor-joining method (DNAMan Software; Lynnon BioSoft, Quebec, Canada).
RESULTS
Fifty subjects (34 HCV antibody positive and 16 antibody negative) were prospectively enrolled in the study. HCV anti-body-negative subjects were significantly older than HCV an-tibody-positive subjects (57 versus 46 years old; P5 0.003 [t test] [SigmaStat for Windows version 2.0; Jandel Scientific Software]). Males were represented significantly more fre-quently than females in the HCV antibody-positive group (65%) compared to the HCV antibody-negative group (25%; P50.005 [chi-square test with Yates correction] [SigmaStat]). In addition, alanine aminotransferase values were significantly higher in the HCV antibody-positive group (154 IU/ml versus 81 IU/ml; P5 0.025 [Mann-Whitney rank sum test] [Sigma-Stat]). Twenty-four (71%) of the 34 HCV antibody-positive and 8 of 16 (50%) HCV antibody-negative patients had previ-ously undergone liver biopsy at our institution in order to evaluate the etiology and activity of their hepatitis. In subjects who had more than one liver biopsy, the most recent biopsy was used in the analysis. In this group of patients referred for chronic liver disease, there were no differences between the amounts of inflammation or fibrosis noted in the HCV anti-body-positive and -negative groups.
To insure that the whole-blood tests and both methods of testing plasma were performed on the same blood sample from each patient, a single tube of blood was obtained and labeled with a code to blind the laboratory investigators to the subject’s identity and plasma and whole-blood aliquots were prepared and stored under identical conditions. Samples of whole blood mixed with Catrimox and plasma mixed with Catrimox were tested by our in-house RT-PCR test. A plasma aliquot was also tested by the Roche Amplicor test by the University of Iowa Clinical Virology Laboratory. Neither laboratory knew the other laboratory’s results until all 50 patients were studied. Among HCV antibody-positive individuals, 85% of whole-blood samples, 77% of plasma-Catrimox samples, and 74% of Roche plasma assays were positive (Table 1). When we
on May 15, 2020 by guest
http://jcm.asm.org/
viewed the clinical records of these 34 subjects, all 5 of those who were negative by the whole-blood-based test were receiv-ing and respondreceiv-ing to interferon therapy at the time of testreceiv-ing and had tested positive by both whole-blood and plasma meth-ods prior to therapy. All five of these subjects were also neg-ative by plasma testing.
HCV RNA was detected in the whole blood of 6 of 16 HCV antibody-negative individuals (Table 1). Only 2 of 16 subjects had HCV RNA detected by the plasma-Catrimox method, and only 1 of these was also positive by the Roche assay (Table 1). Cryoglobulins are detected in approximately 40% of individu-als with chronic HCV infection (2). These large virus-antibody complexes are likely to precipitate with the cellular pellet dur-ing plasma preparation and may lead to false-negative HCV antibody tests and plasma HCV RNA determinations (17, 33). We therefore reviewed the medical records of the antibody-negative subjects for evidence of cryoglobulinemia. Both of the subjects with HCV RNA in their plasma were found to have cryoglobulinemia. One additional subject with cryoglobuline-mia was identified, and this subject tested positive by whole-blood-based HCV RNA testing, although the plasma samples tested negative by both methods. Thus, three of the six HCV antibody-negative subjects in whom HCV RNA was detected had cryoglobulins present in their plasma. Liver biopsy results were available for four of these antibody-negative, RNA-pos-itive subjects. One biopsy was interpreted to include “autoim-mune” features (in a subject with cryoglobulinemia). Another biopsy was read as primary biliary cirrhosis, and the remaining two were interpreted as hepatitis of unknown etiology.
When the HCV RNA test results of both HCV antibody-positive and -negative subjects were combined, 70% of whole-blood samples, 56% of plasma-Catrimox samples, and 52% of plasma samples tested by Amplicor were positive for HCV RNA. Using Cochran’s test for related samples to determine if there were any differences among of the groups (42), an exact Pvalue of 0.0005 was found, suggesting that the HCV RNA detection rates of the three tests (whole blood, plasma-Catri-mox, and plasma-based Amplicor) were different. Using Mc-Nemar’s test for related (or correlated or matched) samples, whole blood differed from plasma-Catrimox (exact two-tailed P value, 0.0156) and whole blood differed from the Roche Amplicor test (P50.0039) (42). No difference was identified between plasma-Catrimox and Roche Amplicor (P50.6875). The Roche and the whole-blood-versus-plasma comparisons were also statistically significant at the 0.05 level when the Bonferroni method was applied (to eval-uate for multiple pairwise comparisons) (42). In all instances where plasma samples were positive (by either the Roche test or our plasma test), whole blood was also positive. Thus, there was never discordance between our whole-blood test and a positive plasma test.
To determine if whole-blood-based RNA results could be
confirmed in the Amplicor assay, and to verify that the whole-blood results represented true HCV infection and not false-positive results, we utilized RNA extracted from whole blood as the template RNA in the Roche assay. As noted above, in the Roche system RNA is prepared from 100ml of plasma and then 5% of the RNA preparation is used in the assay (28). Using equivalent concentrations of RNA prepared from whole blood, we performed additional studies of the nine whole-blood RNA-positive, Amplicor-negative subjects. RNA was prepared from the whole blood of these individuals, and the RNA was used as the template in the commercial Amplicor system. Six of these samples were from HCV antibody-negative subjects, and three were from HCV antibody-positive people. In addition, we tested RNA prepared from six subjects whose initial whole-blood RNA tested positive in our in-house assay and for whom the plasma Amplicor test was positive. These samples served as the positive controls. Table 2 demonstrates that whole-blood RNAs from all of the subjects who were positive by the plasma-based Amplicor test were positive; thus, whole-blood RNA can serve as a suitable template for ampli-fication in the Amplicor system. However, all nine of the whole-blood RNA samples for which plasma was initially neg-ative by the Amplicor test were also negneg-ative in the whole-blood-based Amplicor test. Thus, upon initial analysis, the whole-blood-based Amplicor results were no different from the plasma-based Amplicor results and they did not support the hypothesis that the positive whole-blood-based HCV RNA results obtained from our house assay represented true in-fection.
Review of the protocols indicated that our in-house RT-PCR method uses a 10-fold-greater concentration of RNA than the Amplicor system. We therefore repeated the whole-blood-based RNA testing of the nine samples that were negative by the Amplicor test and positive by the whole-blood-based test and the six samples that were negative by the whole-blood- and plasma-based tests from the HCV antibody-negative group of subjects, using the increased RNA concentration. Under these conditions, eight of the nine subjects (89%) who were positive in the initial whole-blood-based testing were also positive by the Roche Amplicor system (Table 2). It is unclear why we were unable to amplify the ninth sample using the Amplicor system, although differences in PCR primers, PCR inhibition, RNA degradation, or false-positive results may account for this finding.
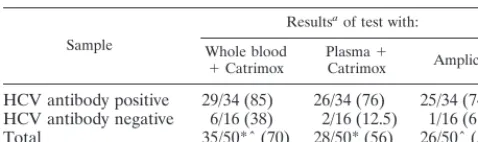
[image:3.612.54.293.93.164.2]Importantly, all of the whole-blood RNA’s that tested neg-ative in the in-house assay also tested negneg-ative by the Roche assay, even when RNA samples derived from high volumes of whole blood were tested (n 5 15). RNA was also prepared from 50ml of plasma from six of the antibody-negative subjects who were positive by the whole-blood-based tests. All six of these samples were negative by the Amplicor assay, although TABLE 1. Comparison between HCV RNA detection by Roche
Amplicor and by whole blood or plasma in Catrimox tests
Sample
Resultsaof test with:
Whole blood
1Catrimox PlasmaCatrimox1 Amplicor
HCV antibody positive 29/34 (85) 26/34 (76) 25/34 (74) HCV antibody negative 6/16 (38) 2/16 (12.5) 1/16 (6.25) Total 35/50*ˆ (70) 28/50* (56) 26/50ˆ (52)
aResults are given as number positive/total number studied (%). * and ˆ
[image:3.612.309.552.93.171.2]indicate comparisons that were statistically significant (see the text).
TABLE 2. Use of whole-blood RNA as a template in the Roche Amplicor system
Results (whole blood/Roche)
Roche Amplicor results (no. positive/total)a
Standard
volume volumeHigh
Negative/negative 0/6 0/6
Positive/positive 6/6 NT
Positive/negative 0/9 8/9
aStandard volume utilized RNA from 5 ml of plasma or whole blood (see
text). High volume utilized RNA from 50 ml of whole blood. NT, not tested.
on May 15, 2020 by guest
http://jcm.asm.org/
the whole-blood-based Amplicor test was positive (data not shown). These results confirm the increased sensitivity of whole blood relative to plasma.
To further confirm that these amplified products repre-sented unique viral isolates and were unlikely to be due to laboratory contamination, we determined the nucleotide se-quences of the PCR products obtained from four antibody-negative subjects. These were compared with our laboratory positive control HCV sequence and sequences from three HCV antibody-positive subjects. The HCV 59NTR is the ge-nome region most highly conserved between isolates (35); hence, the sequence alignment of these eight isolates shown in Fig. 1 demonstrates that the isolates are distinct and do not represent our laboratory control strain of HCV. There were an average of seven mutations between isolates, or 3% of this highly conserved region. This degree of sequence heterogene-ity also argues strongly against PCR artifact, as the expected rate of misincorporations with Taq polymerase is approxi-mately 1 per 1,000 bases copied, or 0.01% (13).
Four of the six HCV antibody-negative subjects in whom HCV RNA was detected had previously undergone liver bi-opsy. Using the Mann-Whitney rank sum test and the equal variance test to compare the groups (antibody-positive RNA-positive, antibody-positive RNA-negative, antibody-negative RNA-positive, and antibody-negative RNA-negative groups), no differences in inflammation were found; however, the sta-tistical power was poor due to the small number of biopsies present in three of the four groups, and the possibility of differences cannot be excluded (Table 3). However,
signifi-cantly more fibrosis was observed in the HCV RNA-positive group compared with the HCV RNA-negative group (P 5 0.036 [Mann-Whitney rank sum test] [SigmaStat]). This raises the possibility that antibody-negative subjects with HCV infec-tion have more aggressive liver disease. Prospective studies are under way to address this issue.
DISCUSSION
We previously demonstrated that the Catrimox-14 whole-blood RNA extraction method provided high-quality RNA useful for detecting HCV RNA and that there is an increased concentration of HCV RNA in whole blood relative to plasma and individual blood cell compartments (30, 32, 33). Once mixed with Catrimox-14, HCV RNA in whole blood is stable for several days at room temperature (30). Since HCV RNA in plasma or serum is labile unless it is quickly processed and frozen at270°C, Catrimox-14 whole-blood RNA preparation offers a practical advantage in the clinical setting over plasma assays (30).
[image:4.612.340.524.73.369.2]Whole-blood-based HCV RNA detection was previously shown to be more sensitive than plasma-based detection in HCV antibody-positive patients during interferon therapy (31, 40). Patients in whom HCV RNA was detected at the end of therapy were significantly more likely to relapse than those with negative whole-blood-based HCV RNA tests (31, 40); thus, this approach may have important clinical implications.
FIG. 1. Homology tree of HCV 59NTR constructed by the neighbor-joining method. The data represent four HCV antibody-negative subjects (1 to 4), the laboratory positive control isolate (5), and three HCV antibody-positive subjects (6 to 8).
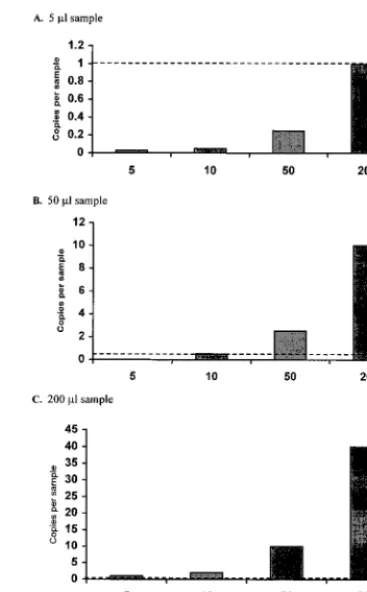
FIG. 2. Demonstration of the number of HCV RNA copies present in a given sample volume at various RNA concentrations. The dashed line represents the approximate lower limit of detection for our in-house RT-PCR assay and the Roche Amplicor test (200 copies per ml51 copy per 5ml or 10 copies per 50
[image:4.612.83.258.79.212.2]ml). Note that at low concentrations of HCV RNA and low sample volumes, the amount of RNA present in a given sample frequently falls below the limit of detection.
TABLE 3. Histopathologic findings among HCV antibody-negative subjects stratified by HCV RNA and antibody statusa
Group and biopsy finding
Biopsy resultsa
HCV antibody
negative HCV antibodypositive Total
HCV RNA negative
Inflammation 1.0 (n54) 1.5 (n54) 1.25 (n58)
Fibrosis 0.5 0.25 0.375*
HCV RNA positive
Inflammation 1.75 (n54) 1.45 (n520) 1.5 (n524)
Fibrosis 2.75 1.75 1.92*
aBiopsy results were scored as follows: 0, absent; 1, mild; 2, mild to moderate;
3, moderate; 4, moderate to severe; and 5, severe. *,P50.036 (Mann-Whitney rank sum test).
on May 15, 2020 by guest
http://jcm.asm.org/
[image:4.612.52.293.605.704.2]In this study, we confirmed the enhanced sensitivity of whole blood relative to plasma for HCV RNA detection in a mixed population of patients with liver disease, and we expanded previous findings by directly comparing the whole-blood-based assay with our in-house plasma-based assay and the well-vali-dated Amplicor RT-PCR assay (28).
Confirmation of the specificity of our assay was accom-plished by demonstrating that whole-blood RNA was suitable for amplification in the commercial assay. In all but one of the subjects with a positive whole-blood-based test but a negative plasma-based test, the Roche assay was positive when the con-centration of whole-blood RNA was increased. The approach of using higher volumes of sample to prepare RNA has been proven useful in other systems, specifically in HCV (15, 16) and human immunodeficiency virus (HIV) diagnostics. For example, the only difference between the “ultrasensitive” HIV RNA detection assay and the standard HIV Amplicor test is that there is a 10-fold increase in the volume of the input serum used to prepare RNA in the former (manufacturer’s instructions; Roche Diagnostic Systems). The specificity of our whole-blood-based HCV RNA assay was demonstrated when HCV RNA-negative samples were negative in the Roche as-say, even when higher concentrations of whole-blood RNA were used in the RT-PCRs. We also confirmed the specificity of our results by cloning and amplifying the sequences of the PCR products from several of the subjects, demonstrating that these are independent isolates and unlikely to be the result of contamination.
We previously reported that a significant proportion of HCV RNA in whole blood segregates with the cellular pellet during the preparation of plasma or serum (33). As noted above, approximately half of the HCV in the cell pellet is adherent to the cells and not intracellular (33). This is presumably due to the binding of immune complexes or HCV-lipid complexes to cell surfaces (17, 37). Although technical issues, such as differ-ences in PCR primers, could account for differdiffer-ences in sensi-tivity, we believe that the improved sensitivity found with whole blood is due to the increased concentration of virus in the cellular pellet. Since our lower limit of detection is approx-imately the same as, or slightly higher than, that of the Am-plicor assay, the increased sensitivity does not appear to be inherent in the RT-PCR procedure. If the limit of detection is 200 copies per ml, as reported for Amplicor, the HCV viral load would have to be 200 copies per ml before each 5-ml sample would be predicted to contain detectable virus (Fig. 2). Consequently, in patients with low-level viremia (,200 copies per ml), increasing the volume of the initial sample or enhanc-ing the concentration of virus within the sample is necessary to allow detection.
This study also expands our previous observations of HCV antibody-negative, RNA-positive disease (serosilent HCV in-fection). Six of 16 (38%) of our HCV antibody-negative pa-tients were found to be infected with HCV, slightly lower than in our prior study of patients with HCV antibody-negative cryptogenic hepatitis (32). These results are also similar to those of Dries et al., who detected HCV RNA in liver biopsy specimens in 61% of patients with cryptogenic hepatitis (12). Although three of the six HCV RNA-positive, antibody-nega-tive patients we identified had cryoglobulins in their sera, there were no other reasons identified to explain the failure to detect anti-HCV antibody. Thus, at least in this population, it appears that our previous findings are reproducible and HCV infection is common among individuals with chronic liver disease of undetermined etiology.
The mechanism by which the HCV isolates in these individ-uals avoid detection by commercial antibody tests is unclear.
Antibodies may be present in the subjects, but due to extensive sequence differences between the individual isolates and the commercial antigen, the antibodies may be different enough to prevent detection in the commercial assay. Alternatively, vari-ation in host immune responses may lead to diminished or absent antibody production in some HCV-infected individuals. Studies are under way to evaluate why antibodies are not detected in these individuals.
In summary, this study confirms and expands our previous observations of increased HCV RNA levels in whole blood relative to plasma and demonstrates that this RNA is suitable for use in commercial diagnostic assays. The studies suggest that whole-blood-based RNA detection has increased sensitiv-ity for detecting HCV in antibody-negative people and may therefore be important in the screening of blood donors. In addition, it has been shown to be more sensitive than plasma-based HCV RNA detection in patients receiving interferon; thus, it may prove important for the management of HCV therapy (31). Studies to determine the rates of antibody-neg-ative, RNA-positive HCV infection in different populations of patients and to characterize the viral isolates and immune responses of these patients are under way.
ACKNOWLEDGMENTS
We thank Fred LaBrecque and Molly Stapleton for establishing the database on liver histopathology, Donald McFarlane and Iowa Bio-technology for providing Catrimox-14, and the nursing staff of the University of Iowa Digestive Disease Center and Clinical Research Center for assistance in collecting specimens.
This work was supported by a Merit Review Grant from the Veter-ans Administration (J.T.S.) and mentored scientist award 1KO8 AI01460 (W.N.S.) from the National Institutes of Health, and patient care was provided in part by the GCRC Program in NCRR, NIH no. RR0059.
REFERENCES
1.Aach, R. D., C. E. Stevens, F. B. Hollinger, J. W. Mosley, D. A. Peterson, P. E. Taylor, R. G. Johnson, L. H. Barbosa, and G. J. Nemo.1991. Hepatitis C virus infection in post-transfusion hepatitis. An analysis with first- and sec-ond-generation assays. N. Engl. J. Med.325:1325–1329.
2.Agnello, V., R. T. Chung, and L. M. Kaplan.1992. A role for hepatitis C virus infection in type II cryoglobulinemia. N. Engl. J. Med.327:1490–1495. 3.Alter, M. J.1997. Epidemiology of hepatitis C. Hepatology26:62S–65S. 4.Alter, M. J., H. S. Margolis, K. Krawczynski, F. N. Judson, A. Mares, W. J.
Alexander, P. Y. Hu, J. K. Miller, M. A. Gerber, and R. E. Sampliner.1992. The natural history of community-acquired hepatitis C in the United States. The sentinel counties chronic non-A, non-B hepatitis study team. N. Engl. J. Med.327:1899–1905.
5.Alter, M. J., and R. E. Sampliner.1989. Hepatitis C: and miles to go before we sleep. N. Engl. J. Med.321:1538–1540.
6.Bouffard, P., P. Hayashi, R. Acevedo, N. Levy, and J. Zeldis.1992. Hepatitis C virus is detected in a monocyte/macrophage subpopulation of peripheral blood mononuclear cells of infected patients. J. Infect. Dis.166:1276–1280. 7.Bresters, D., H. T. M. Cuypers, H. W. Reesink, W. P. Schaasberg, C. L. Van der Poel, E. P. Mauser-Bunschoten, M. Houghton, Q. L. Choo, G. Kuo, and R. Lesniewski.1992. Enhanced sensitivity of a second generation ELISA for antibody to hepatitis C virus. Vox Sang.62:213–217.
8.Choo, Q. L., G. Kuo, A. Weiner, L. Overby, D. W. Bradley, and M. Houghton. 1989. Isolation of a cDNA derived from a blood-borne non-A, non-B viral hepatitis genome. Science244:359–362.
9.Conry-Cantilena, C., M. VanRaden, J. Gibble, J. Melpolder, A. O. Shakil, L. Viladomiu, and L. Cheung.1996. Routes of infection, viremia and liver disease in blood donors found to have hepatitis C virus. N. Engl. J. Med. 334:1691–1695.
10. Cotton, P.1991. Tests help nail down HCV; but not entirely. JAMA265:312. 11. Crotty, P. L., R. A. Staggs, P. T. Porter, A. A. Killeen, and R. C. McGlennen. 1994. Quantitative analysis in molecular diagnostics. Hum. Pathol.25:572– 579.
12. Dries, V., I. von Both, M. Muller, G. Gerken, P. Schirmacher, M. Odenthal, K. H. Meyer zum Buschenfelde, and H. P. Dienes.1997. Detection of hep-atitis c virus (HCV) in liver tissue of HCV-RNA seronegative patients by means of anti-HCV-antibodies and RT-PCR. Hepatology26:140A. 13. Eckert, K. A., and T. A. Kunkel.1991. DNA polymerase fidelity and the
polymerase chain reaction. PCR Methods Appl.1:17–24.
on May 15, 2020 by guest
http://jcm.asm.org/
14.Gil, B., C. Qian, J. Riezu-Boj, M. P. Civeira, and J. Prieto.1993. Hepatic and extrahepatic HCV RNA strands in chronic hepatitis C: different patterns of response to interferon treatment. Hepatology18:1050–1054.
15. Gretch, D., L. Corey, J. Wilson, C. dela Rosa, R. Willson, R. Carithers, M. Busch, J. Hart, M. Sayers, and J. Han.1994. Assessment of hepatitis C virus RNA levels by quantitative competitive polymerase chain reaction: high-titer viremia correlates with advanced stage of disease. J. Infect. Dis.169:1219– 1225.
16. Gretch, D. R.1997. Diagnostic tests for hepatitis C. Hepatology26:43S–47S. 17. Han, J.-Q., W. N. Schmidt, P. Wu, P. Loh, G. Neil, D. R. LaBrecque, and J. T. Stapleton.1997. Specific binding of hepatitis C virus to the Fc fragment of immunoglobulin molecules, p. 228–231.InM. Rizzeto et al. (ed.), Viral hepatitis and liver disease. Edizioni Minerva Medica, Turin, Italy. 18. Hoofnagle, J. H.1997. Hepatitis C: the clinical spectrum of disease.
Hepa-tology26:15S–20S.
19. Lanford, R. E., D. Chavez, F. V. Chisari, and C. Sureau.1995. Lack of detection of negative-strand hepatitis C virus RNA in peripheral blood mononuclear cells and other extrahepatic tissues by the highly strand-specific rTth reverse transcriptase PCR. Virology69:8079–8083.
20. Laskus, T., M. Radkowski, L. F. Wang, J. Cianciara, H. Vargas, and J. Rakela.1997. Hepatitis C virus negative strand RNA is not detected in peripheral blood mononuclear cells and viral sequences are identical to those in serum: a case against extrahepatic replication. J. Gen. Virol.78: 2747–2750.
21. Laskus, T., M. Radkowski, L. F. Wang, H. Vargas, and J. Rakela.1998. Detection of hepatitis G virus replication sites by using highly strand-specific Tth-based reverse transcriptase PCR. J. Virol.72:3072–3075.
22. Lee, S., J. McHutchison, B. Francis, R. DiNello, A. Polito, S. Auan, and M. Nelles.1992. Improved detection of antibodies to hepatitis C virus using a second generation ELISA. Adv. Exp. Med. Biol.312:183–189.
23. Lerat, H., F. Berby, M. A. Trabaud, O. Vidalin, M. Major, C. Trepo, and G. Inchauspe.1996. Specific detection of hepatitis C virus minus strand RNA in hematopoietic cells. J. Clin. Investig.97:845–851.
24. Lok, A. S. F., and N. T. Gunaratnam.1997. Diagnosis of hepatitis C. Hepa-tology26:48S–56S.
25. Major, M. E., and S. M. Feinstone.1997. The molecular virology of hepatitis C. Hepatology25:1527–1538.
26. Nakatsuji, Y., A. Matsumoto, E. Tanaka, H. Ogata, and K. Kiyosawa.1992. Detection of chronic hepatitis C virus infection by four diagnostic systems: first-generation and second-generation enzyme-linked immunosorbent as-say, second-generation recombinant immunoblot assay and nested polymer-ase chain reaction analysis. Hepatology16:300–305.
27. NIH Consensus Development Panel on Infectious Disease Testing for Blood Transfusions.1995. Infectious disease testing for blood transfusions. JAMA 274:1374–1379.
28. Prati, D., C. Capelli, P. Bosoni, F. Mozzi, A. Zanella, and G. Sirchia.1994. Determination of hepatitis C virus RNA in the serum by the Amplicor HCV PCR kit. Vox Sang.67:112–114.
29. Reischl, U., and B. Kochanowski.1995. Quantitative PCR. Mol. Biotechnol. 3:55–71.
30. Schmidt, W. N., D. Klinzman, D. LaBrecque, D. E. Macfarlane, and J. T. Stapleton.1995. Direct detection of hepatitis C virus (HCV) RNA from whole blood, and comparison with HCV RNA in plasma and peripheral blood mononuclear cells. J. Med. Virol.47:153–160.
31. Schmidt, W. N., P. Wu, D. Brashear, D. Klinzman, M. J. Perino-Phillips, D. R. LaBrecque, and J. T. Stapleton.1998. Effect of interferon therapy on hepatitis C virus RNA in whole blood, plasma and peripheral blood mono-nuclear cells. Hepatology28:1110–1116.
32. Schmidt, W. N., P. Wu, J. Cederna, F. A. Mitros, D. R. LaBrecque, and J. T. Stapleton.1997. Surreptitious hepatitis C virus (HCV) infection detected in the majority of patients with cryptogenic chronic hepatitis and negative HCV antibody tests. J. Infect. Dis.176:27–33.
33. Schmidt, W. N., P. Wu, J.-Q. Han, M. J. Perino, D. R. LaBrecque, and J. T. Stapleton.1997. Distribution of hepatitis C virus (HCV) RNA in whole blood and blood cell fractions: plasma HCV RNA analysis underestimates circulating virus load. J. Infect. Dis.176:20–26.
34. Seeff, L. B.1997. Natural history of hepatitis C. Hepatology26:21S–28S. 35. Simmonds, P.1995. Variability of hepatitis C virus. Hepatology21:570–583. 36. Sugitani, M., G. Inchauspe, M. Shindo, and A. M. Prince.1992. Sensitivity of serological assays to identify blood donors with hepatitis C viremia. Lancet 339:1018–1019.
37. Thomssen, R., S. Bonk, and A. Thiele.1993. Density heterogeneities of hepatitis C virus in human sera due to binding of beta-lipoproteins and immunoglobulins. Med. Microbiol. Immunol.182:329–334.
38. Van der Poel, C. L., H. T. Cuypers, H. W. Reesink, A. J. Weiner, S. Quan, R. DiNello, J. J. VanBoven, I. Winkel, D. Mulder-Folkerts, and P. J. Exel-Oehlers.1991. Confirmation of hepatitis C virus infection by new four-antigen recombinant immunoblot assay. Lancet337:317–319.
39. Villa, E., L. Ferretti, M. DePalma, M. Melegari, P. P. Scaglioni, P. Trande, C. Vecchi, N. Fratti, and F. Manenti.1991. HCV RNA in serum of asymp-tomatic blood donors involved in post-transfusion hepatitis (PTH). J. Hepa-tol.13:256–259.
40. Watkins-Riedel, T., H. Hofmann, P. Steindl, C. Muller, and P. Ferenci.1997. Comparison of whole blood and serum for the detection of hepatitis c virus (HCV) RNA in interferon (IFN) treated patients. Hepatology26:140A. 41. Wilber, J. C.1993. Development and use of laboratory tests for hepatitis C
infection. J. Clin. Immunoassay16:204–207.
42. Woolson, R. F.1987. Statistical methods for the analysis of biomedical data, p. 513. John Wiley & Sons, New York, N.Y.
43. Xiang, J. H., D. Klinzman, J. McLinden, W. N. Schmidt, D. R. LaBrecque, R. Gish, and J. T. Stapleton.1998. Characterization of hepatitis G virus (GB-C virus) particles: evidence for a nucleocapsid and expression of se-quences upstream of the E1 protein. J. Virol.72:2738–2744.
44. Zanetti, A. R., E. Tanzi, and G. Zehender.1990. Hepatitis C virus in symp-tomless donors implicated in post-transfusion non-A, non-B hepatitis. Lan-cet336:448.