_____________________________________________________________________________________________________
(Past name: British Journal of Medicine and Medical Research, Past ISSN: 2231-0614, NLM ID: 101570965)
Morphometric Evaluation of Styloid Process Using
Cone Beam Computed Tomography- A
Retrospective Study of Chennai Population
S. Kailasam
1, F. Massillamani
1, Venkata Lakshmi Aparna Potluri
1,
Akila Prabakaran
1, Naga Leela Guntuku
1*and C. K. Vishnu Priya
11Department of Oral Medicine and Radiology, Ragas Dental College and Hospital, Uthandi, Chennai,
India.
Authors’ contributions
This work was carried out in collaboration between all authors. Author SK designed the study and concept. Author FM wrote the protocol, and manuscript review. Authors FM and AP did clinical studies. Author AP wrote the first draft of the manuscript and analysis of study. Authors VLAP and CKVP performed the statistical analysis. Author NLG managed the literature search, analyses of the study and involved in manuscript preparation. All authors read and approved the final manuscript.
Article Information DOI: 10.9734/JAMMR/2018/39071
Editor(s):
(1)Fatima Mubarak, Department of Radiology, Aga Khan University, Karachi, Pakistan. (2)Costas Fourtounas, Faculty of Medicine, School of Health Sciences, University of Thessaly, Greece.
Reviewers:
(1) Luciana de Barros Correia Fontes, Universidade Federal de Pernambuco, Brazil. (2)Oguzhan Gorler, Cumhuriyet University, Turkey. Complete Peer review History:http://www.sciencedomain.org/review-history/23599
Received 28th December 2017 Accepted 25th February 2018 Published 12th March 2018
ABSTRACT
Introduction: The styloid process arises from petrous part of temporal bone as an osseous projection and shows considerable anatomic variability. The elongated styloid process presents with various signs and symptoms. The manifestations may vary widely such as cervicofacial pain, cerebral ischaemia and even death. Diagnosis can be made by clinical evaluation and different imaging modalities of which Cone Beam Computed Tomography(CBCT) gives a more accurate measurement. The morphological knowledge of styloid process and its variation is essential as it has various clinical implications in the field of dentistry, cardiology and forensic sciences.
Aim: The objective of the present study is to evaluate 3 dimensionally the structural variation of styloid process, to evaluate the length and to analyse the prevalence of elongated styloid process
Kailasam et al.; JAMMR, 25(8): 1-12, 2018; Article no.JAMMR.39071
according to age and gender using CBCT.
Study Design: Cross sectional retrospective study.
Materials and Methods: A series of CBCT images from 100 patients comprising of 74 males and 26 females were collected retrospectively at Ragas Dental College, Chennai during the period from September 2016 to October 2016. CBCT of study subjects were obtained using Galileos Comfort Plus. Statistics used was Chi Square test and analysis was done by using the statistical package SPSS version 20.0
Results: The prevalence of elongated styloid process was 56.6% with more prevalence in males 46.5% with 47% being Type I elongation(with uninterrupted integrity of styloid process) and 41% had type A pattern of calcification(calcified outline of styloid process)
Conclusion: This study provides 3 dimensional knowledge of anatomical variation in styloid process according to age and gender. Assessment should be done during routine assessment to rule out any abnormalities.
Keywords: Elongated styloid process syndrome; Eagle’s syndrome; styloid-stylocarotid syndrome; cone beam computed tomography.
Key Message:An elongated styloid process or styloid chain ossification can present with wide range of symptoms even leading to death. Hence a thorough knowledge of its presence, anticipation of cause when patient is symptomatic and prompt diagnosis is required which can save a life.
1. INTRODUCTION
The styloid process is a part of the stylohyoid chain which also includes the stylohyoid ligament (SHL) and lesser cornu of hyoid bone. The styloid process is located on the inferior aspect of temporal bone [1]. It normally measures 25mm in length although the length and structure may vary [2,3)]. The styloid process is considered to be elongated when it measures more than 30mm [2,4-7]. Elongated styloid process can present with 2 manfiestations-the classical stylohyoid syndrome and the stylocarotid which was described in 1937 by Walt Eagle. Patients may remain asymptomatic or may present with a
plethora of symptoms to the dental,
otorhinolaryngology, ophthalmology or neurology clinics. It is also of importance to forensic sciences as sudden death has also been reported [8].
1.1 Aims and Objectives
The aim and objectives of this study is to analyse the variation in length, size, shape and calcification pattern according to age and gender using CBCT which provides a detailed and accurate 3 dimensional evaluation with its clinical and medicolegal significance.
2. MATERIALS AND METHODS
CBCT scans of 100 patients (74 male and 26 female) from Ragas Dental College, Oral and Maxillofacial Radiology Clinic electronic archive
were used in this study. The study group included healthy individuals who were not suffering from any systemic disease during CBCT acquisition. The study followed the college’s IRB guidelines. CBCT images were acquired with Galileos Comfort Plus scanner 16cm*13cm FOV at 90kV, 4mA and 11.26 seconds for 0.125mm voxel size. Acquired scans were viewed on 24” Dell monitor. Exclusion criteria were images with minimum FOV. The
images were stored in Sirona viewer.
Measurements of styloid process were
performed from the tympanic plate to the tip of the styloid process. The type of elongation was noted which was described by Langlais et al.
Langlais et al has classified various types of styloid process and described using numerical method in 1986 which was then modified by Mac Donald-Jankowski as:
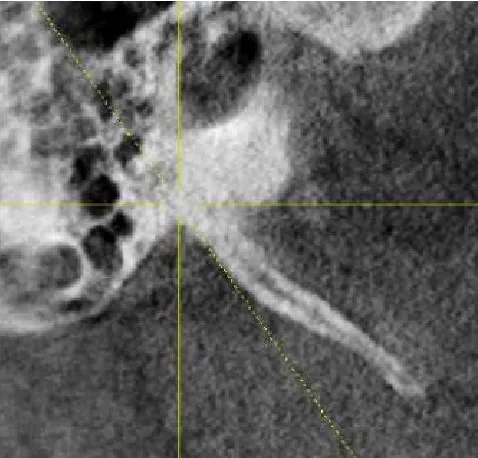
Type I: Uninterrupted integrity of styloid process (>30mm)(Fig.1)
Type II: Styloid process joined to the mineralised submandibular or stylohyoid ligament by a single pseudoarticulation(Fig. 2)
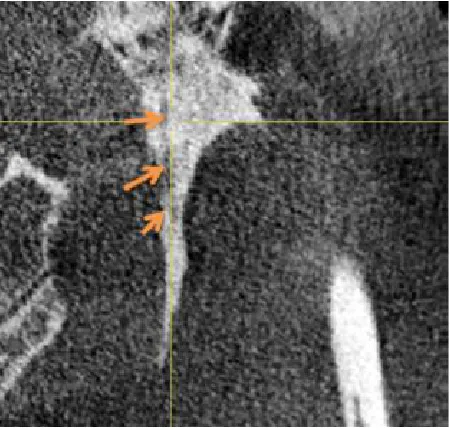
Type III: Segmented styloid process containing multiple segmented pseudoarticulations(Fig. 3)
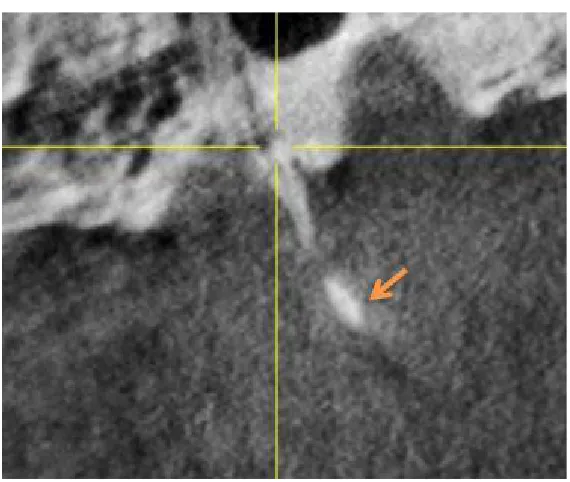
Type IV: Elongation of styloid process due to distant ossification(Fig. 4).
Fig. 1. Type I Pattern (Un interrupted type)
Fig. 2. Type II Pattern (Single Pseudo Articulation)
Type A: Calcified outline of styloid process(Fig.5)
Type B: Partially calcified styloid process with discontinuous radiolucent core(Fig. 6)
Type C: Nodular appearance of styloid process with varying degrees of central radiolucency(Fig. 7)
Type D: Completely calcified styloid process with
no evidence of a radiolucent interior
structure.(Fig. 8).
3. RESULTS
Out of 100 CBCT images, 200 styloid
processes were evaluated. 133 styloid
Kailasam et al.; JAMMR, 25(8): 1-12, 2018; Article no.JAMMR.39071
Fig. 3. Type III pattern (Multiple segmented pseudo articulation)
Fig. 4. Type IV Pattern (Distant ossification)
3.1 Effect of Gender on Elongated Styloid Process
The mean length of the styloid process was 31.09mm. On comparing the elongated
3.2 Effect of Sides and Gender on Elongated Styloid Process
Among 100 styloid processes, in the right side 74 showed elongation on which 48 were male and 26 were female and one female showed absence of styloid process which showed a positive correlation with a significant value of 0.023*. In the left side 74 styloid processes showed elongation of which 45 were male and 29 were female which showed a positive correlation with a significant value of 0.041*.(Graph 1 and 2).
3.3 Effect of Age on Styloid Process Elongation
The mean age of the patients with elongated styloid process was 40.92 years. The mean age of the patients with ESP in males was 41.54 years and in females was 39.19 years. There was no statistically significant difference in mean age of the males and the females.
3.4 Effect of Gender and Sides on Elongation Pattern
Type I elongation was the most frequent type of styloid process in both male 36% and female 10.5%. Type I elongation is the most common in both right and left sides followed by Type IV. No significant association was observed between gender and elongation patterns. (Graph 3,4)
3.5 Effect of Gender and Sides on the Calcification Type
The most frequent pattern of calcification was Type A in male 32.5% and in female showed equal prevalence of Type A(8.5%) and Type
D(8.5%). The most common pattern of
calcification on both right and left sides is Type A followed by Type D. No significant association was observed between gender and calcification pattern. (Graph 5,6)
4. DISCUSSION
The embryological origin of the styloid process is the second brachial arch, Reicher’s cartilage [9]. There are 4 cartilage structures that give rise to styloid process [1,10]. The muscles that are attached to styloid process are styloglossus, stylohyoid, stylopharyngeus and are required for normal oropharyngeal functions [4,11]. The
lesser cornu of hyoid bone provides
attachment to the stylohyoid ligament which is a continuation of the apex of the styloid process. It is present within the lateral pharyngeal wall lateral to the tonsillar fossa and is located between the external and internal carotid arteries [5]. Important vessels such as the carotid arteries, the internal jugular vein and the facial, glosopharyngeal, vagus and hypoglossal nerves are all located in the region and hence is clinically important [2].
Kailasam et al.; JAMMR, 25(8): 1-12, 2018; Article no.JAMMR.39071
Fig. 6. Type B Calcification (Partially calcified with discontinuous radiolucent core)
Fig. 7. Type C Calcification (Nodular appearance with varying degrees of central radiolucency)
The styloid process normally measures 25mm in length [3]. Watt Eagle, an otolaryngologist considered any styloid process to be elongated styloid process when it measures longer than 30mm [2,4-7]. He found 4% of the population with elongated styloid process [2]. In the present study, 100 CBCT samples were collected randomly of which 74 were male and 26 were female and the age range was from 13 to 80
The mean age of prevalence was 40.92 yrs in our study, which was in accordance with Al-Kaki et al. [16] who reported increased prevalence among 20-40 yrs. Some authors have reported an increased prevalence among older age groups. Guimaraes et al. [13] reported an increased prevalence between 41 and 50 yrs and Corell et al. [17] after 50 yrs. There is still no
agreement among authors regarding the
common age group.
In this study, the rate of elongated
stylloid process was greater in male 46.5% than the female 10% in accordance with Ghafari et al. [18] in 2012, who stated that the rate of elongated styloid process was greater in males(52.9%) than in the females which was also in accordance with Gupta et al. 72.5% [5]. However, this finding differed from a study by Ferrario et al. [19] who found equal prevalence among both sexes.
Fig. 8. Type D Calcification (Completely calcified with no evidence of a radiolucent interior structure)
Kailasam et al.; JAMMR, 25(8): 1-12, 2018; Article no.JAMMR.39071
Graph 2. Distribution of elongation-Left side by sex
Legend for Graph 1 and 2: 1- Elongation present, 2- Elongation absent, x- Complete absence of styloid process
Graph 3. Distribution of Pattern of elongation -Right side by sex
Graph 4. Distribution of Pattern of elongation -Left side by sex
Graph 5. Distribution of Pattern of Calcification -Right side by sex
Graph 6. Distribution of Pattern of Calcification -Left side by sex
Legend for Graph 5,6- 1-Type A calcification pattern, 2- Type B calcification pattern, 3- Type C calcification pattern, 4-Type D calcification pattern, x- Absence of styloid process
Several theories have been proposed to explain the etiopathology of Eagle’s syndrome. Lengele and Dhem [20] reported congenital elongation of styloid process as the cause of Eagle’ syndrome, Fini et al. [9] concluded that past tonsillectomy to be the cause. Other theories are persistence of mesenchymal elements, local chronic irritation, previous history of trauma and endocrine disorders in female at menopause as the cause of calcification and ossification of the stylohyoid ligament [21].
Elongated styloid process shows 2 clinical expressions, the classic styloid syndrome that commonly occurs after tonsillectomy as dull and persistent pharyngodynia localized in the tonsillar fossa, sometimes presents with dysphagia, facial and cervical pain, odynophagia, hypersalivation, foreign body sensation and the stylocarotid syndrome causing impingement in the internal or
external carotid artery results in migraines, cluster headaches due to irritation of the peri arterial sympathetic plexus in the area of the pain [22], transient ischemic attack (TIA), or stroke. The symptoms vary according to the structures affected. When there is pain in the neck on turning head, or pain radiating to different orofacial structures such as the eye, ear, angle of the mandible, soft palate and nose, the external carotid artery maybe affected and when the internal carotid artery is involved, the patient may experience pain over the entire head and larynx [2,9,23,24].
In our study, bilateral elongated styloid
process(56.6%) was more common than
Kailasam et al.; JAMMR, 25(8): 1-12, 2018; Article no.JAMMR.39071
Similar findings have been reported by Rizzatti et al (55%) [3] and Gupta et al. [5] (72.5%). Gulmara Scaf et al. [25] has contradictory result with unilateral involvement of right side (76.2%) being common.
Diagnosis can be made on physical examination of the tonsillar region [24] and imaging studies such as plain radiography including panoramic radiograph, Towne’s radiograph, lateral oblique-mandible, AP-skull [26], barium swallow study in which the indentation of the elongated styloid
process appears as filling defect [27].
Conventional radiographs are cheaper but have the main disadvantage of superimposition, distortion and magnification that may hinder proper diagnosis. Hence, three dimensional evaluation using computed tomography, cone beam computed tomography can be used for accurate measurement [14] and analyse its spatial geometry. CBCT has the added advantage of less radiation exposure when compared to CT.
The most common type of elongated styloid
process according to Langlais’s [28,29]
classification was Type I ESP (91.5%) than other types which was in accordance with this study in which Type I was common with 47%. Many studies have reported similar results as Langlais with Gupta et al. [5] (91.5%), Krusolgu et al. [12] (81%), Asrani et al. [30] (90%), Chabikuli et al. [4] (59%), Shah et al. [31] (65%) stating that type I was more common, Oztunc et al. [32] in 2014, in his study, stated that pseudo articulated Type(Type II) (50%), was the most common type among the male and female which was not in accordance with this study where continuous type (Type I) was more common in male and female.
An ossified stylohyoid ligament can cause difficulty during tracheal intubation. Stylohyoid ligament ossification can lead to immobile larynx and the elevation of epiglottis due to forward traction of hyoid bone would cause difficulty during direct laryngoscopy procedures. This can lead to serious consequences and risk of regurgitation during emergency situation [33].
In this study, the highest incidence of calcification pattern was Type A(calcified outline) 41% followed by Type D. This was in accordance with Chabikuli et al. [4] (Type A 48.9%), Shaik et al. [34] (Type A 28.6-94%), Bagga et al. [35] (Type A>55%) being the most frequent type. Sudhakar Reddy et al. [14] has given contradictory results with Type D(58%) being the most common.
Sudden death has also been reported due to elongated styloid process [8]. It occurs when an enlarged styloid process compresses the internal carotid artery causing transient ischemic attack. The compression can cause dilatation and widening of the internal carotid artery resulting in carotid sinus syndrome. This is more prevalent in the elderly affecting those above 50 years. The carotid sinus artery becomes more sensitive to any form of stimulation known as carotid sinus hypersensitivity leading to exaggerated response with bradycardia or vasodilatation and invariably leading to hypotension, presyncope and syncope [36]. Carotid sinus reflex death occurs when vagus nerve impulse causes the heart to stop beating, leading to cardiac arrest [37]. Elongated styloid process has also been a cause of death in neck injuries [8].
Presence of cervical spondylosis and anomalies of vertebral arteries have been reported with ESP in the literature, where care must be taken by therapists during manipulation of spine in the cervical region. Potential of fracturing ESP have been reported with traumatic injuries. Thus a manipulative contact in the styloid process area could induce iatrogenic fracture resulting in pain and symptoms of Eagle’s syndrome which can
be confirmed radiologically after clinical
examination [38].
Differential diagnoses include conditions with similar signs and symptoms. Temporomandibular joint diseases are the most common condition with patients presenting with unilateral pain. Other conditions that can be considered are neuralgias like trigeminal, sphenopalatine or glossopharyngeal neuralgias, headache like cluster type headache, migraine, temporal arteritis, hyoid bursitis, chronic infections like pharyngotonsillitis, otitis media. Even dental pain, improperly fitting dental prostheses can cause vague pain symptoms. Sailvary gland disorders like sialadenitis or sialolithiasis, foreign bodies,
and tumors, etc [23], laryngopharyngeal
dysesthesia, Sluder's syndrome, esophageal diverticula should also be considered [39].
Management includes both conservative and surgical approach. Conservative management
includes injection of non-steroidal anti
inflammatory drugs, long acting local
anaesthetics at site of palpation, oral
Though, a majority of patients may remain asymptomatic, elongated styloid process can cause further complications during intubations, neck injury and can also be a risk factor for fracture of styloid process, cause of sudden death and incidental finding during autopsy, all of which are important in medicolegal point of view.
.
5. SUMMARY AND CONCLUSION
The present study was conducted to evaluate the various morphological changes in the styloid process using CBCT. 100 samples comprised of 200 styloid processes, with a higher frequency of ESP in males (46.5%) than females (10%), out of which 58% had an elongation in the right side and 55% in the left side with 47% Type I elongation and 41% Type A calcification pattern.
Patients presenting with complaint of the intermittent pain of cervicofacial region, transient
neurological symptoms, suspicion of an
elongated styloid process has to be made and for early diagnosis of asymptomatic patients, routine
dental examination should also include
evaluation of the styloid process.
CONSENT AND ETHICAL APPROVAL
It is not applicable.
COMPETING INTERESTS
Authors have declared that no competing interests exist.
REFERENCES
1. Başekim CÇ, Mutlu H, Güngör A, et al.
Eur Radiol. 2005;15(1):134-139.
2. Eagle WW. Symptomatic elongated styloid
process: report of two cases of styloid
process-carotid artery syndrome with
operation. Arch Otolaryngol
1949;49(5):490-503.
3. Rizzati-Barbosa C, Ribeiro M,
Silva-Concilio L, Di Hipolito O, Ambrosano G. Is an elongated styloid process prevalent in the elderly? A radiographic study in a
Brazilian population. Gerodontology
2005;22(2):112-5.
4. Chabikuli NJ, Noffke CEE. Styloid process
elongation according to age and gender: A
radiological study. S. Afr. Dent.
J. 2016;71(10):470-473.
5. Gupta N, Khan M, Doddamani LG,
Kampasi N, Ohri N. A study on assessment
of the length of styloid process in digital panoramic radiographs. J Indian Oral Med Radiol. 2015;27:516-9.
6. Haroun HSW. Morphometric and
radiological evaluation of the stylohyoid complex in man. Ann. of Int. Med. & Den. Res. 2015;1(2):49-52.
7. Tassoker M, Ozcan S. Prevalence of
styloid process elongation in An Elderly Turkish population. IOSR Journal of Dental and Medical Sciences. 2016;15(9):158-160.
8. Kumar P, Raymane AP, Subbaramaiah M.
Sudden death due to eagle syndrome. Am J For Pathol. 2013;34:231-233.
9. Fini G, Gasparini G, Filippini F, Becelli R,
Marcotullio D. The long styloid process syndrome or Eagle's syndrome. J Cranio-Maxillofac Surg. 2000;28:123–127.
10. Magotra R, Razdan S. Elongated styloid
process: Anatomical variations. J K
Science. 2008;10(4):203-205.
11. Das S, Suhaimi FH, Othman F, Latiff
AA. Anomalous styloid process and its
clinical implication. Bratisl Lek. Listy. 2008;109(1):31-3.
12. Lee S, Hillel A. Three-dimensional
computed tomography imaging of Eagle's syndrome. Am J Otolaryngol. 2004;25:109.
13. Guimarães Simone Maria Ragone, et al.
Prevalência de alteração morfológica do processo estilóide em pacientes com
desordem temporomandibular. Radiol
Bras Dec. 2006;39(6):407-411.
14. Reddy R, Sai Kiran Ch, Sai Madhavi N,
Raghavendra MN, Satish A. Prevalence of elongation and calcification patterns of elongated styloid process in South India. J Clin Exp Dent. 2013;5(1):30-35.
15. Jung T, Tschernitschek H, Hippen H,
Schneider B, Borchers L. Elongated styloid process: when is it really elongated? Dentomaxillofac Radiol. 2004;33:119–124.
16. Al-Kaki Raood T, El-Khateeb Sara M,
Arnout Eman A. Radiographic prevalanace
and clinial significance/ etiology of
elongated styloid process in females. British Journal of Medicine and Medical Research. 2016;15(6):1-8.
17. Correll RW, Jensen JL, Taylor JB, Rhyne
RR. Mineralization of the
stylohyoid-stylomandibularligament complex. A
radiographic incidence study. Oral Surg Oral Med Oral Pathol. 1979;48(4):286–91.
18. Ghafari R, Hosseini B, Shirani AM,
Kailasam et al.; JAMMR, 25(8): 1-12, 2018; Article no.JAMMR.39071
panoramic radiographs and some of the general health conditions in patients over 40 years of age in the Iranian population. Dental Research Journal. 2012;9(Suppl 1): S52-S56.
19. Ferrario VF, Sigurta D, Daddona A, Dalloca
L, Miani A, Tafuro F, Sforza C. Calcification of the stylohyoid ligament: Incidence and morphoquantitative evaluations. Oral Surg Oral Med Oral Pathol. 1990;69:524-9.
20. Lengele B, Dhem A. Microradiographic and
histological study of the styloid process of the temporal bone. Acta Anat (Basel) 1989;135:193-9.
21. Lentini A. Gli aspetti clinici e radiologici
delle anomalie dell’ apparato stilo-joideo. Radiol Med. 1975;61:337-364.
22. Andrei F, Motoc AGM, Didilescu AC, Rusu
MC. A 3D cone beam computed
tomography study of styloid process of
the temporal bone. Folia Morphol.
2013;72(1):29–35.
23. Jain S, Bansal A, Paul S, Prashar DV.
Styloid-stylohyoid syndrome. Ann
Maxillofac Surg. 2012;2(1):66-9.
24. Prabhu LV, et al. An unusually lengthy
styloid process. Singapore Med
J. 2007;48(2):e34-6.
25. Scaf G, Freitas DQ, Loffredo Lde C.
Diagnostic reproducibility of the elongated styloid process. J Appl Oral Sci. 2003;11: 120-4.
26. Prasad KC, Panduranga Kamath M, Jagan
Mohan Reddy K, Raju K, Agarwal S. Elongated styloid process (Eagle's
syndrome): A clinical study. J Oral
Maxillofac Surg. 2002;60(2):171–175.
27. Renu Tanwar , Chandrashekhar L, Asha
R, Iyengar Nagesh KS, Subhash BV. Stylohyoid ligament syndrome –solving the riddle with 3D computed tomography. Journal of Dental Sciences and Research. 2011;2(2):46-49.
28. Langlais R, Miles D, Van Dis M. Elongated
and mineralized stylohyoid ligament
complex: A proposed classification and report of a case of eagles syndrome. Oral
Surg Oral Med Oral Pathol. 1986;61(6): 527-32.
29. Candice Colby C, John Del Gaudio M.
Stylohyoid complex syndrome. A new diagnostic classification. Arch Otolaryngol Head Neck Surg. 2011;137(3):248–252.
30. More CB, Asrani MK. Evaluation of the
styloid process on digital panoramic radiographs. Indian J Radiol Imaging 2010;20:261-5.
31. Shah S, Praveen N, Subhashini A.
Elongated styloid process: A retrospective panoramic radiograph study. World J Dent 2012;3(4):316-9.
32. Oztunc H, Evlice B, Tatli U, Evlice A.
Cone-beam computed tomographic evaluation of styloid process: A retrospective study of 208 patients with orofacial pain. Head Face Med. 2014;10:5.
33. Ames WA, McNiellis N. Stylohyoid
ligament calcification as a cause of difficult intubation? Anaesthesia. 1998;53:415–6.
34. Shaik M, Naheeda, Kaleem S, Wahab A,
Hameed S. Prevalence of elongated styloid process in Saudi population of the Aseer region. Eur J Dent. 2013;7:449-54.
35. Bagga MB, Kumar C, Yeluri G.
Clinicoradiologic evaluation of styloid
process calcification. Imaging Sci Dent. 2012;42(3):155-61.
36. Miller VM, Kenny RA, Slade JY, et al.
Medullary autonomic pathology in carotid sinus hypersensitivity. Neuropathol Appl Neurobiol. 2008;34(4):403-411.
37. Jagadish Rao PP, et al. Legal Medicine.
2010;12(4):184-18.
38. Vougiouklakis T. Overview of the ossified
styloid ligament based in more than 1200 forensic autopsies. J Clin Forens Med. 2006;13:268–270.
39. Savranlar A, Uzun L, Ugur MB, Ozer T.
Three dimensional CT of Eagle's
syndrome. Diagn Interv Radiol.
2005;11(4):206–9.
40. Sadaksharam J, Singh K. Stylocarotid
syndrome: An unusual case
report. Contemporary Clinical Dentistry. 2012;3(4):503-506.
_________________________________________________________________________________ © 2018 Kailasam et al.; This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Peer-review history: