Fast Forward Rounds: An Effective Method for Teaching Medical
Students to Transition Patients Safely Across Care Settings
Karin Ouchida, MD,
Veronica M. LoFaso, MD,
wCarol F. Capello, PhD,
wSharda Ramsaroop, MD,
wand M. Carrington Reid, MD, PhD
wAdverse events commonly occur during hospital-to-home transitions and cause substantial morbidity. This study evaluated the effectiveness of Fast Forward Rounds (FFR), a novel educational intervention that aims to foster aware-ness of the essential elements of transitional care in 3rd-year medical students. FFR consists of two 90-minute sessions using lectures, an interactive video, small-group discussion, and a team-based learning exercise. It emphasizes func-tional assessment to identify patients at risk for poor dis-charge outcomes, promotes interdisciplinary collaboration to link vulnerable patients with appropriate services, re-views Medicare and Medicaid reimbursement, and teaches development of comprehensive care plans. Using a pre/ posttest design, participants’ knowledge, attitudes and be-haviors within the domains of transitional care, functional assessment, interdisciplinary team, community resources, and reimbursement were assessed. Of 103 students, 99.0% attended Session 1 and 97.1% attended Session 2 (pretest completion rate 99.0%, posttest 94.1%). Significant im-provements were found in all domains, with the largest gains seen in transitional care. After the intervention, 56.0% iden-tified medication errors as the most common source of ad-verse events after discharge (vs 14.9% before the intervention, Po.001). Significantly more participants re-ported feeling competent or expert in safely discharging chronically ill patients (66.3% vs 9.8%, Po.001) and in educating patients about discharge medications (75.8% vs 28.4%,Po.001). Participants also reported changes in tran-sitional care behaviors (e.g., 71.6% now review the dis-charge medication list with patients and caregivers 50% of the time (vs 42.3%, P5.002)). A multimodal educational intervention for medical students increased their transitional care knowledge, reported frequency of transitional care behaviors, and perceived competence in managing the discharge process.J Am Geriatr Soc 57:910–917, 2009.
Key words: transitional care; discharge planning; curric-ulum; medical student education
E
ach year, older adults with chronic illness see as many as seven different community physicians and, when hos-pitalized, receive care in up to four subsequent clinical set-tings.1,2During a transition to a different location or level of care, timely communication of a comprehensive care plan between sending and receiving providers, medication reconciliation, and appropriate patient education are so es-sential to patient safety that the Joint Commission on Ac-creditation of Healthcare Organizations incorporated them into the 2009 National Patient Safety Goals.2,3In the com-monly studied hospital-to-home transition, approximately one in five patients experiences an adverse event. Two-thirds of adverse events are medication related and more than half result in greater healthcare utilization, including hospital readmission.4,5Clinical interventions designed to improve the hospital-to-home transition demonstrate positive patient outcomes and reductions in healthcare utilization, but they rely on nonphysician providers6–13 or the patients themselves to bridge gaps in continuity of care.14,15 Educational inter-ventions to ensure safe transitions are scarce. Chronic ill-ness and home visiting curricula improve students’ attitudes toward the chronically ill and provide vital exposure to nontraditional clinical sites,16–19 but they do not situate fundamental geriatrics competencies such as functional as-sessment within the framework of safe transitions. Further-more, they do not focus on the skills necessary to promote cross-site collaboration (e.g., medication reconciliation and provider–provider communication). The few educational interventions targeting care transitions incorporate post-hospitalization home visits20,21 or emphasize proper dis-charge summary preparation.22 Although these programs expose potential pitfalls during care transitions, they do not actively engage participants in the creation of discharge plans. Therefore, it is imperative to implement educational
Address correspondence to Karin Ouchida, Montefiore Medical Center, Albert Einstein College of Medicine, 111 East 210th Street, Bronx, NY 10467. E-mail: [email protected]
DOI: 10.1111/j.1532-5415.2009.02203.x
Division of Geriatrics, Montefiore Medical Center, Albert Einstein College
of Medicine, Bronx, New York; andwDivision of Geriatrics and Gerontology, Weill Medical College, Cornell University, New York, New York.
JAGS 57:910–917, 2009 r2009, Copyright the Authors
interventions that teach physicians to recognize their role within an interdisciplinary team and their responsibility to ensure safe transitions.23
To address this gap in medical education geriatrics fac-ulty at Weill Cornell Medical College developed Fast For-ward Rounds (FFR), an innovative curriculum emphasizing five domains: transitional care, functional assessment, in-terdisciplinary team, community resources, and reimburse-ment. This study sought to assess the effect of FFR on participants’ knowledge, attitudes, and self-reported be-haviors in these domains. It was hypothesized that a cur-riculum combining an interdisciplinary team approach and diverse teaching modalities would improve participants’ transitional care knowledge, perceived competence in man-aging the discharge process, and frequency of transitional care behaviors such as patient education and medication reconciliation. It was also hypothesized that participants would respond positively to an interactive, multimodal learning climate.
METHODS
Participants and Setting
The FFR curriculum became a mandatory component of the 12-week internal medicine clerkship in July 2006. Partic-ipants (N5103) consisted of third-year medical students completing their required internal medicine rotations be-tween July 2006 and June 2007. Approximately 25 students participated in each of the four rotations. Slightly more than half of participants (52%) were female, and the mean age was 27 (range 23–37). Of those reporting ethnicity, 60% were Caucasian, 17% Asian, 10% black, and 7% Hispanic. Third-year internal medicine residents (n55) completed a 4-hour training session led by core geriatrics faculty and then served as adjunct faculty by delivering a lecture, eval-uating the discharge summary assignment, and facilitating small-group discussions. The institutional review board of Weill Cornell Medical College approved the study.
Intervention (Curriculum Description)
FFR consists of two 90-minute sessions that incorporate interdisciplinary lectures, an educational digital video disc (DVD), small-group discussion, and a team-based learning exercise. Sessions were scheduled during Weeks 4 and 8 of the 12-week inpatient medicine clerkship to ensure famil-iarity with the inpatient wards, sufficient time for comple-tion of the written assignment, and opportunities to practice transitional care behaviors (Figure 1).
Session 1 begins with a brief overview of the transi-tional care literature, followed by a DVD featuring a hypo-thetical clinical vignette of a resident physician hurriedly discharging a patient admitted for acute myocardial infarc-tion. The DVD is paused for a guided discussion of the resident’s inattention to transitional care (e.g., her failure to assess the patient’s understanding of key medication changes) and prediction of the patient’s posthospital course. When the DVD resumes, the resident is shown readmitting the patient with congestive heart failure due to medication nonadherence, lack of home care services, and inappropri-ate clinical follow-up.
Session 1 concludes with focused lectures illustrating how a team approach to the hypothetical patient would ensure a safer hospital-to-home transition and prevent re-hospitalization. A geriatric nurse practitioner demonstrates how functional assessment can identify patients at high risk for poor discharge outcomes, and a social worker reviews home and community-based services and Medicare and Medicaid reimbursement. The course addresses insurance coverage of critical services such as home health care and durable medical equipment, because appropriate discharge planning requires an understanding of who qualifies for these services and how they are reimbursed. Although the curriculum promotes interdisciplinary collaboration with social work, it also equips students with the basic reim-bursement knowledge necessary to prevent them from communicating incorrect or inappropriate discharge Figure 1. Components of Fast Forward Rounds transitional care curriculum.
information to patients. Between sessions, students submit a discharge summary for a patient they cared for in the hospital.
Session 2 begins with a physical therapist and geriat-rician presenting potential discharge venues for hospitalized older adults, including rehabilitation facilities and housing options. Next, participants divide into small groups to re-ceive written and verbal feedback from course facilitators about their discharge summaries. Each group then chooses their most exemplary discharge summary to play the FFR board game, an interactive team-based exercise that rein-forces the major content domains and incorporates role-playing exercises as a means to practice communication skills.
A Web-based participant manual is available to stu-dents for optional review. Course materials are also avail-able on-line at http://www.POGOe.com.
Survey Instrument
Participants complete a pretest at the start of Session 1 and a posttest at the conclusion of Session 2. The 28-item assess-ment tool contains content questions and self-assessassess-ment questions on attitudes and behaviors in the domains of transitional care, functional assessment, interdisciplinary team, community resources, and reimbursement. The post-test also includes three open-ended questions soliciting feedback about the course and its overall effect on patient care. Geriatrics faculty (n54) with extensive experience in medical education developed the assessment tool, which was then revised for content and clarity with assistance from leaders in the primary care residency and internal medicine clerkship.
Statistical Analysis
Univariate statistics were calculated on all study variables. Differences in pre- and posttest scores were evaluated using chi-square or Fisher exact tests as appropriate. To examine how percentage correct changed over time and differences according to domain and wave, this dependent variable was analyzed in a mixed model including fixed factors for do-main, wave, and time; the interactions between these vari-ables; and questions as levels of a random factor.
Two investigators (KO, VL) independently reviewed all written responses to the open-ended questions and gener-ated a list of themes used to code all comments using stan-dard methods.24Discrepancies in coding were resolved by discussion until consensus was reached.
RESULTS
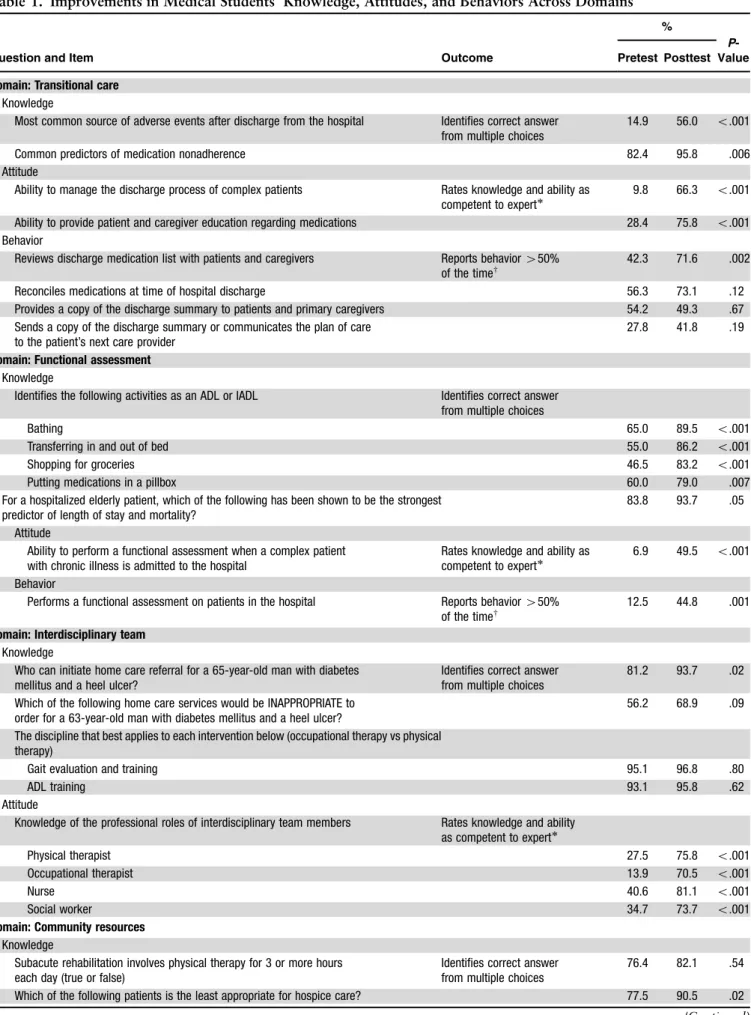
Attendance was 99.0% for Session 1 and 97.1% for Session 2, with pre- and posttest completion rates of 99.0% and 94.1%, respectively. The largest gains were in the domains of functional assessment, interdisciplinary team, and tran-sitional care, but significant improvements were found in all five domains (Table 1). Performance did not vary as a function of group (i.e., results were generally the same ir-respective of when students participated in the course over the 1-year study period).
Within the functional assessment domain, participants scored significantly better on the posttest items requiring them to distinguish activities of daily living (ADLs) from
instrumental activities of daily living (IADLs). After the course, 83.1% labeled shopping as an IADL, compared with 46.5% before the course (Po.001), and 86.2% iden-tified transferring as an ADL, compared with 55.0% before the course (Po.001). The proportion of students feeling competent, proficient, or expert in performing functional assessment increased from 6.9% to nearly 49.5% (Po.001), and the percentage of students reporting perfor-mance of functional assessment more than tripled (from 12.5% to 45.0%,Po.001).
Interdisciplinary team items reflected knowledge of home health care and familiarity with the roles of various team members. On the pretest, 81.2% of students correctly identified which individuals can initiate home care referrals, but a significant improvement was observed in the posttest score (93.7%,P5.02). The proportion of students rating their understanding of the professional roles of various terdisciplinary team members as competent to expert in-creased considerably. Before the course, 13.9% of students felt knowledgeable about the role of occupational therapy, 27.5% understood the role of physical therapy, and 34.7% were familiar with social work and 40.6% with nursing. After the course, these numbers rose to 70.5% for occupa-tional therapy, 75.8% for physical therapy, 73.7% for so-cial work, and 81.1% for nursing (Po.001).
Substantial gains emerged in the transitional care do-main on knowledge, attitudes, and behavior items. After completing the course, 56.0% of students correctly identi-fied medication errors as the most common source of ad-verse events after hospital discharge (vs 14.9% at the time of the pretest,Po.001). Participants demonstrated higher confidence levels in managing the discharge process of pa-tients with chronic illness, with 66.3% of students rating themselves as competent to expert after the course (vs 9.8%,Po.001). Significantly greater numbers of students also reported feeling skilled in educating patients and their caregivers about discharge medications (75.8% vs 28.4%, Po.001). Finally, participants indicated greater frequency of key transitional care behaviors. Postintervention, 71.6% of students reported reviewing discharge medications with patients or caregivers at least 50% of the time (vs 42.3%, P5.002). Although the growth in the proportion of stu-dents performing medication reconciliation was not signifi-cant (from 56.3% to 73.1%), nearly three-fourths of the students reported engaging in this critical component of the care transition at the conclusion of the course.
Within the reimbursement domain, the percentage of students self-rating their knowledge of Medicare and Med-icaid as competent to expert was five times greater (4.9% before the FFR vs 26.3% after;Po.001). After FFR, 40.0% of students felt competent to expert in their knowledge of community resources, compared with 2.0% before the course (Po.001).
Open-Ended Responses
Eighty-six students (83.5%) generated 230 responses to the open-ended question asking what they liked most about the course. Most (79.6%) comments centered on course con-tent (37.4%), learning climate (18.7%), faculty (12.6%), and the game (10.9%). Participants described the content as ‘‘focused, high-yield information’’ that ‘‘targeted a clear set
Table 1. Improvements in Medical Students’ Knowledge, Attitudes, and Behaviors Across Domains
Question and Item Outcome
%
P-Value Pretest Posttest
Domain: Transitional care
Knowledge
Most common source of adverse events after discharge from the hospital Identifies correct answer from multiple choices
14.9 56.0 o.001 Common predictors of medication nonadherence 82.4 95.8 .006 Attitude
Ability to manage the discharge process of complex patients Rates knowledge and ability as competent to expert
9.8 66.3 o.001 Ability to provide patient and caregiver education regarding medications 28.4 75.8 o.001 Behavior
Reviews discharge medication list with patients and caregivers Reports behavior450% of the timew
42.3 71.6 .002 Reconciles medications at time of hospital discharge 56.3 73.1 .12 Provides a copy of the discharge summary to patients and primary caregivers 54.2 49.3 .67 Sends a copy of the discharge summary or communicates the plan of care
to the patient’s next care provider
27.8 41.8 .19
Domain: Functional assessment
Knowledge
Identifies the following activities as an ADL or IADL Identifies correct answer from multiple choices
Bathing 65.0 89.5 o.001
Transferring in and out of bed 55.0 86.2 o.001 Shopping for groceries 46.5 83.2 o.001 Putting medications in a pillbox 60.0 79.0 .007 For a hospitalized elderly patient, which of the following has been shown to be the strongest
predictor of length of stay and mortality?
83.8 93.7 .05 Attitude
Ability to perform a functional assessment when a complex patient with chronic illness is admitted to the hospital
Rates knowledge and ability as competent to expert
6.9 49.5 o.001 Behavior
Performs a functional assessment on patients in the hospital Reports behavior450% of the timew
12.5 44.8 .001
Domain: Interdisciplinary team
Knowledge
Who can initiate home care referral for a 65-year-old man with diabetes mellitus and a heel ulcer?
Identifies correct answer from multiple choices
81.2 93.7 .02 Which of the following home care services would be INAPPROPRIATE to
order for a 63-year-old man with diabetes mellitus and a heel ulcer?
56.2 68.9 .09 The discipline that best applies to each intervention below (occupational therapy vs physical
therapy)
Gait evaluation and training 95.1 96.8 .80
ADL training 93.1 95.8 .62
Attitude
Knowledge of the professional roles of interdisciplinary team members Rates knowledge and ability as competent to expert
Physical therapist 27.5 75.8 o.001 Occupational therapist 13.9 70.5 o.001
Nurse 40.6 81.1 o.001
Social worker 34.7 73.7 o.001
Domain: Community resources
Knowledge
Subacute rehabilitation involves physical therapy for 3 or more hours each day (true or false)
Identifies correct answer from multiple choices
76.4 82.1 .54 Which of the following patients is the least appropriate for hospice care? 77.5 90.5 .02 (Continued)
of principles’’ and had ‘‘practical applications.’’ Many stu-dents emphasized the novelty of the content (e.g., ‘‘vital info not taught elsewhere’’ and ‘‘the lectures were all on valuable topics, i.e., Medicare/Medicaid that we have no other ex-posure to in medical school’’). The course heightened par-ticipants’ awareness of the larger healthcare system (e.g., ‘‘The course explained some of the ‘mystery’ of the health care system’’ and ‘‘covered large points in how the system works’’). In praising the learning climate, students often mentioned the ‘‘interactive format’’ with a ‘‘variety of ac-tivities, games and videos to teach points.’’ One participant wrote ‘‘The interactive learning process helped to make the information stick and made things fun.’’
Sixty-seven students (65.0%) generated 122 responses to the open-ended question asking how the course could be improved. Most suggestions (45.9%) focused on the dura-tion of the sessions and timing of the course during the workday. Others commented ‘‘[Schedule] earlier in the course so we can use the skills during clerkship right away’’ and ‘‘Get started earlier within the rotation because [the information is] so applicable and important.’’ Negative re-marks about course content (18.0%) often reflected stu-dents’ desire for more information on a particular topic such as reimbursement or requests for less lecture time.
Sixty-eight students (66.0%) responded to the final open-ended question soliciting feedback about how the course affected the way they care for hospitalized patients. These comments convey the effect of FFR on participants’ transitional care knowledge, attitudes, and behaviors (Ta-ble 2). Students reported improved knowledge about the deficiencies in the current discharge process (e.g., ‘‘[The
course] explains explicitly where the gaps are in the dis-charge management of patientsFthings I thought would be taken care of somewhere along the course of a patient’s health care really are not’’). Many participants reported greater awareness of the discharge summary as one way to bridge this gap.
Responses also revealed a shift in transitional care at-titudes as students described a willingness to ‘‘think about what the patient’s life is like when they leave,’’ being ‘‘more thoughtful about post-hospital planning,’’ and wanting ‘‘to be more personal with the patient and really emphasize patient education to improve compliance.’’ Many responses described a planned or adopted behavioral change reflecting the transitional care skills promoted by the course (pro-vider–provider communication and patient education). For example, one student wrote, ‘‘[I] definitely appreciate more how important the discharge summary is [and] will start including more specific instructions for patients and offer them/family members a copy. I will also start forwarding to next care provider.’’
Participants praised FFR for providing a ‘‘specific for-mat’’ to address transitional care issues and ‘‘have certain aspects of follow-up care clarified.’’ One student wrote, ‘‘[I] feel more aware of discharge issuesFsomething I was NOT learning on the floors.’’ Several responses suggest that stu-dents perceive their interns and resistu-dents to be dismissive of the importance of the discharge summary. One student re-ported, ‘‘I paid more attention to writing discharge sum-maries and going through the discharge plan with my patients. It was ironic because my intern thought it was ‘scut work’ but it’s one of my favorite parts of patient care, Table 1. (Contd.)
Question and Item Outcome
%
P-Value Pretest Posttest
All of the following are aims of palliative care EXCEPT 86.1 86.3 .97 Attitude
Knowledge of community resources available for patients with chronic illness Rates knowledge and ability as competent to expert
2.0 40.0 o.001 Ability to access hospice and palliative care services for patients 4.9 53.7 o.001
Domain: Reimbursement
Knowledge
In NY state, the following health services are covered by (Medicare, Medicaid, both, or neither)?
Identifies correct answer from multiple choices
Long-term care in a skilled nursing facility 17.4 47.4 o.001 Rolling walker for a patient after hip fracture repair 70.7 85.3 .02 Nurse to assess a patient at home postdischarge from hospital 51.0 83.2 o.001 Home hospice care 46.4 45.3 .99 Grab bar for bathroom 47.5 71.6 .001 Adult day care 12.2 53.7 o.001 Attitude
Understanding of Medicare and Medicaid reimbursement Rates knowledge and ability as competent to expert
4.9 26.3 o.001
5-point scale: novice, beginner, competent, proficient, expert. w
5-point scale: never,o50% of the time, 50%,450%, always. ADL5activity of daily living; IADL=instrumental activity of daily living.
and I really did feel like I made a difference with my pa-tients.’’ Another stated, ‘‘I understand that discharge sum-maries do matter, despite what the residents might say. I will make sure to contact the patient’s PMD upon discharge and give them all pertinent info.’’
DISCUSSION
In the current healthcare system, threats to care coordina-tion abound. Incompatible informacoordina-tion systems and drug formularies isolate acute care hospitals, rehabilitation fa-cilities, and ambulatory sites. Patients may fail to
partici-pate in their own care transitions because of increased functional impairment and insufficient health literacy. When ‘‘fumbled handoffs’’ occur, one major system deficit is the problem of ‘‘diffused responsibility,’’ where providers on either end of a transition assume the other will follow up on a test result or ensure the accuracy of the medication list.25 The increased use of hospitalists and adoption of resident work hours regulations have resulted in a greater number of providers sharing the care of a given patient,26,27 yet the increased burden of care coordination for physicians has not coincided with additional training and incentives to collaborate across care settings.27 Existing clinical inter-ventions focus on circumventing physician-level barriers by using additional nonphysician providers to address gaps in continuity of care, but introducing another clinician or ‘‘transitionalist’’ may have the unintended consequence of further obfuscating the lines of responsibility and account-ability.
FFR is unique in its emphasis, at an early stage of clin-ical training, onthe physician’sduty to ensure safe transi-tions. Furthermore, the course is designed to equip medical students with the critical transitional care knowledge, at-titudes, and behaviors necessary to embrace this responsi-bility. A 2001 survey of 70 course directors at 16 representative U.S. medical schools revealed that critical transitional care concepts are often absent from medical school curricula.28Only 36% of surveyed course directors reported including functional assessment of chronically ill patients in required activities; 36% reported evaluating students’ awareness of community services for patients with chronic illness, and 16% taught students to recognize in-dications for home health services. Finally, only 19% of those surveyed said their institutions required teaching ac-tivities focused on ‘‘principles of coordinating care among multiple consultants, including timely communication of relevant clinical data, setting common goals of care, and avoiding redundancy or gaps in care.’’
The FFR course is innovative, effective, and feasibly implemented at other academic institutions using the cur-ricular materials available on-line at www.POGOe.com. It integrates fundamental geriatrics concepts such as func-tional assessment and interdisciplinary team with practical healthcare systems issues like reimbursement and accessing community resources, all under the umbrella of transitional care. The curriculum fulfills several of the educational ob-jectives of the Liaison Committee on Medical Education by emphasizing multidisciplinary care of older patients with chronic illness and the importance of communication with patients, their family members, and other health profes-sionals.29
Qualitative feedback demonstrates that the interactive, multimodal nature of FFR was well received by medical students and can positively influence their attitudes and behaviors toward managing the discharge process even in the face of a ‘‘hidden curriculum’’ that discourages atten-tiveness to the discharge summary, the most common means of provider–provider communication. The not-so-hidden curriculum promulgated on the inpatient wards directly counteracts the transitional care attitudes and behaviors promoted by FFR, but the students’ comments suggest that the course helped them disregard the examples set by cer-tain residents. The potential power of the FFR curriculum Table 2. ‘‘How Did This Course Affect the Way You
Care for Patients in the Hospital?’’
Responses reflecting changes in transitional care knowledge
‘‘[I am] more aware of functional status on presentation. Learned importance of good discharge summary.’’
‘‘[The course] reminded me [of] the importance of discharge summaries when so often they are considered formalities. Started educating me about the importance of insurance status of a patient and how it can influence care and services.’’
‘‘I think the course armed me with valuable resources I can use to better care for my patients by making their transitions smoother and easier.’’
‘‘[I have a] more detailed understanding of integration of everyone involved in patient care [SW, nurses, PT/OT].’’
‘‘I am more aware of the services that exist for patients once they leave the hospital.’’
‘‘[I am] better prepared to discharge patients with proper knowledge of meds and side effects as well as pertinent follow-up information.’’
‘‘I will be better able to think about my patients’ post-discharge care and know what to do to help them at home.’’
Responses reflecting changes in transitional care attitudes
‘‘[The course] made its point. Discharges are important, and ensuring a good transition home and proper care equals better health, and that’s what we’re all here for.’’
‘‘[The course] made me think about what the patient’s life is like when they leave so as to make it easier and prevent re-admission.’’
‘‘I feel more confident in planning for discharge and am more aware of issues that can arise.’’
‘‘[I have a] desire to be more personal with the patient and really emphasize patient education to improve compliance.’’
‘‘[I am] more thoughtful about post-hospital planning. More communication with patients about meds/plans.’’
‘‘I think more about how to give [patients] a smooth transition and I know more about the terms used in discharge planning.’’
‘‘[The course] made me more attentive to discharge issues.’’
Responses reflecting changes in transitional care behaviors
‘‘Will write more effective, comprehensive discharge plans’’ ‘‘I will spend more time explaining the discharge plan to patients.’’ ‘‘[The course] helped me with understanding the patient’s perspective from discharge and realize how little they know. I take more time now in explaining to patients what is going on, tell them test results, etc.’’
‘‘It encouraged me to spend more time on discharge summaries and to communicate with PMDs before discharge.’’
‘‘[I] definitely appreciate more how important the discharge summary is. Although there is no designated space for it, I will start including more specific instructions for patients and offer them/family members a copy. I will also start forwarding to next care provider.’’
SW5social work; PT5physical therapy; OT5occupational therapy; PMD5primary medical doctor.
to promote transitional care attitudes and behaviors even in the face of negative pressure from one’s superiors is truly exciting. Finally, the course involves dual learner levels by incorporating primary care residents as adjunct faculty.
This study has several limitations. The course was im-plemented at one academic institution, and the results re-flect a single cohort of medical students. The pre/postcourse assessment tool has not been validated and relies on par-ticipants’ reported behavioral changes as opposed to their actual clinical practice. Because the pre- and posttest sur-veys were administered 4 weeks apart during the internal medicine clerkship, improvements in knowledge and changes in attitudes and behaviors could also be attributed to other aspects of the rotation, but students’ comments about lack of exposure to transitional care concepts in other venues make it more likely that the positive trends are re-lated to participation in the course. Finally, because of the small sample size of the primary care residents involved, changes in their transitional care knowledge, attitudes and behaviors cannot be analyzed.
The FFR transitional care curriculum is a novel and effective educational intervention. Geriatrics-trained pro-viders may be the ideal group to teach about transitions because of their experience in interdisciplinary and cross-site collaboration.30 Next steps include targeting other learner levels such as medical residents, expanding the cur-riculum to other academic institutions, and incorporating direct-observation tools to evaluate behavioral change. Hospitals seeking to improve handoffs and demonstrate compliance with the Joint Commission’s patient safety standards may also wish to adopt the curriculum for hos-pitalists and other key ‘‘sending’’ providers who bridge the divide between inpatient and outpatient care.3,27 Future research should also assess the effect of educational inter-ventions like FFR on patient-specific outcomes such as sat-isfaction with the discharge process, self-efficacy, healthcare utilization, morbidity, and mortality.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the support of the Donald J. Reynolds Foundation, the John A. Hartford Foundation, and the Bureau of Health Professions. The au-thors are indebted to Melissa Dehner, MSE, Sandy Ganz, PT, DSc, Melissa Kramps, GNP, Deirdre Mole, GNP, and Amy Stern, LCSW, for their expertise, creativity, and pas-sion for teaching about transitions; Charles Bardes, MD, Judy Tung, MD, and Suzanne Wenderoth, MD, for their commitment to the course; and Chuck Henderson, PhD, for his statistical support.
Conflict of Interest:None reported.
Author Contributions:K. Ouchida: study concept and design, acquisition of data, analysis and interpretation of data, and preparation of manuscript. V.M. LoFaso: study concept and design, acquisition of data, analysis and inter-pretation of data, and preparation of manuscript. C.F. Ca-pello: study concept and design and preparation of manuscript. S. Ramsaroop: study concept and design, ac-quisition of data, and preparation of manuscript. M.C. Reid: study concept and design, acquisition of data, analysis and interpretation of data, and preparation of manuscript.
REFERENCES
1. Pham HH, Schrag D, O’Malley AS et al. Care patterns in Medicare and their implications for pay for performance. N Engl J Med 2007;356: 1130–1139.
2. Coleman EA. Falling through the cracks: Challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc 2003;51:549–555.
3. The Joint Commission on Accreditation of Healthcare Organizations. The Joint Commission Accreditation Program: Ambulatory Health Care National Patient Safety Goals [on-line] 2008. Available at http://www.jointcommission.org/NR/ rdonlyres/979098FA-74FD-4F25-AF41-EDD48FBD300E/0/AHC_NPSG.pdf Accessed December 15, 2008.
4. Forster AJ, Murff HJ, Peterson JF et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med 2003;138:161–167.
5. Forster AJ, Clark HD, Menard A et al. Adverse events among medical patients after discharge from the hospital. Can Med Assoc J 2004;170:345– 349.
6. Schnipper JL, Kirwin JL, Cotugno MC et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med 2006;166:565–571.
7. Boockvar KS, LaCorte JC, Giambanco V et al. Medication reconciliation for reducing drug-discrepancy adverse events. Am J Geriatr Pharmacother 2006;4:236–243.
8. Crotty M, Rowett D, Spurling L et al. Does the addition of a pharmacist transition coordinator improve evidence-based medication management and health outcomes in older adults moving from the hospital to a long-term care facility? Results of a randomized, controlled trial. Am J Geriatr Pharmacother 2004;4:257–264.
9. Naylor MD, Brooten D, Campbell R et al. Comprehensive discharge planning and home follow-up of hospitalized elders: A randomized clinical trial. JAMA 1999;281:613–620.
10. Naylor MD, Brooten D, Campbell RL et al. Transitional care of older adults hospitalized with heart failure: A randomized, controlled trial. J Am Geriatr Soc 2004;52:675–684.
11. Rich MW, Beckham V, Wittenberg C et al. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N Engl J Med 1995;333:1190–1195.
12. Stewart S, Horowitz JD. Home-based intervention in congestive heart failure. Circulation 2002;105:2861–2866.
13. Inglis SC, Pearson S, Treen S et al. Extending the horizon in chronic heart failure. Circulation 2006;114:2466–2473.
14. Coleman EA, Smith JD, Grank JC et al. Preparing patients and caregivers to participate in care delivered across settings: The care transitions intervention. J Am Geriatr Soc 2004;52:1817–1825.
15. Coleman EA, Parry C, Chalmers S et al. The care transitions intervention. Arch Intern Med 2006;166:1822–1828.
16. Yuen JK, Breckman R, Adelman RD et al. Reflections of medical students on visiting chronically ill older patients in the home. J Am Geriatr Soc 2006;54:1178–1183.
17. Jerant AF, Levich B, Balsbaugh T et al. Walk a mile in my shoes: A chronic illness care workshop for first-year students. Fam Med 2005; 37:21–26.
18. Burke M, Smith LG. Nurse-practitioner-led home care curriculum for third-year medical students. Mt Sinai J Med 2005;72:312–316.
19. Medina-Walpole A, Heppard B, Clark NS et al. Mi casa o su casa? Assessing function and values in the home. J Am Geriatr Soc 2005;53:336– 342.
20. Matter CA, Speice JA, McCann JR et al. Hospital to home: Improving internal medicine residents’ understanding of the needs of older persons after a hospital stay. Acad Med 2003;78:793–797.
21. Lai CJ, Nye HE, Bookwalter T et al. Post-discharge follow-up visits for medical and pharmacy students on the inpatient medicine clerkship. J Hosp Med 2008;3:20–27.
22. Myers JS, Jaipaul CK, Kogan JR et al. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med 2006;81:S5–S8.
23. Coleman EA, Boult C. Improving the quality of transitional care for persons with complex care needs. J Am Geriatr Soc 2003;51:556– 557.
24. Strauss A, Corbin J. Basics of Qualitative Research. Techniques and Proce-dures for Developing Grounded Theory. Thousand Oaks, CA: Sage Publica-tions, 1998.
25. Gandhi TK. Fumbled handoffs: One dropped ball after another. Ann Intern Med 2005;142:352–358.
26. Volpp KG, Landrigan CP. Building physician work hour regulations from first principles and best evidence. JAMA 2008;300:1197–1199.
27. Pham HH, Grossman JM, Cohen G et al. Hospitalists and care transitions: The divorce of inpatient and outpatient care. Health Aff 2008;27:1315–1327. 28. Pham HH, Simonson L, Elnicki M et al. Training U.S. medical students to care
for the chronically ill. Acad Med 2004;79:32–41.
29. Liaison Committee on Medical Education. LCME Accreditation Standards [on-line] Updated June 2008. Available at www.lcme.org/func tionslist.htm#educational%20program Accessed September 3, 2008. 30. Boockvar KS, Burack OR. Organizational relationships between nursing
homes and hospitals and quality of care during hospital-nursing home patient transfers. J Am Geriatr Soc 55:1078–1084.