Development and Implementation of a
Standardized Sliding Scale Insulin Protocol
Margaret H. Bahlinger, MS, RPh, and Kathryn A. Adkins, RN, BSN, CPHQM
edication errors are one of the most common caus-es of avoidable harm to patients in health care organizations. Among the “high-alert” medica-tions that have the highest risk of causing injury when mis-used is insulin [1–3]. In 2000, Baptist St. Anthony’s Health System (BSA), a nonprofit regional referral center located in Amarillo, Texas, participated in a VHA Medication Error Reduction initiative to reduce the likelihood of medication errors at the hospital. In light of the fact that 12% of inpa-tients in 2000 had a diagnosis of diabetes and that insulin was the second most common medication reported in med-ication error reports, BSA decided to focus on reducing insulin-related medication errors and preventable adverse events. In this paper, we describe a quality improvement project to reduce errors of insulin prescribing and adminis-tration using a standardized protocol and preprinted order form.Background
BSA is licensed for approximately 400 beds, employs 2900, and has 326 physicians on staff. The center serves southern Colorado and Kansas, northeastern New Mexico, and the panhandles of Oklahoma and Texas. Medicare covers 55% of BSA’s patient population. The area has an increasing obese, sedentary, and aging population and a growing number of diabetics. BSA is a member of VHA, Inc., a national alliance of 2200 community-owned health care organizations.
The quality improvement project was implemented by BSA’s interdisciplinary Medication Error Committee, which meets weekly to review medication errors and adverse events. The committee identifies trends and problems and delegates these to subcommittees or teams for action plans. The team appointed to attend VHA’s Medication Error Re-duction program included 4 nurses, a pharmacist, a quality improvement (QI) reviewer, and the hospital’s risk manager. A physician member of the hospital’s pharmacy and thera-peutics committee volunteered to serve as team advisor.
Evaluation of Clinical Processes
Variations in blood glucose levels in diabetic patients at BSA were often addressed with an insulin sliding scale. Although
there is debate about the applicability of the traditional ing scale in inpatient blood glucose management [4–6], slid-ing scale insulin is relatively common in the hospital as an adjunct diabetes management tool. To identify types and numbers of sliding scales in current use, team members retrieved and examined copies of all sliding scale insulin orders from pharmacy files between 1 and 14 November 2000. Results of this preliminary audit showed the following:
• 94 different sliding scale orders
• 44% of the orders used the abbreviation “u” for “units,” a potential cause of tenfold dosing error [1,2]
• Lack of consistent measures to address hypo-glycemia
• Difficulties in order interpretation due to hand-writing
To obtain a more detailed clinical picture, systematic sam-pling was used to obtain a 5% sample of patients who had received sliding scale insulin at BSA between December 2000 and February 2001; the charts of 32 patients were reviewed. Data from this assessment are shown in the baseline column in Table 1.
The team was concerned about these findings. Good man-agement of blood glucose levels in hospitalized diabetics is important; it improves the healing process and decreases the risk of complications [7,8]. The American Diabetes Associ-ation generally suggests target blood glucose levels of 80 to 120 mg/dL before meals and 100 to 140 mg/dL at bedtime in otherwise well diabetics [9]. Although hospitalized diabetics could be expected to have blood glucose readings somewhat higher than this, the mean of 214.9 mg/dL was inappropri-ately high. Patients averaged 27 finger sticks each, suggesting that the high readings required additional follow-up testing and care. Better blood glucose control presumably could prevent or reduce the need for this. The usual standard of nursing care at BSA is to telephone the physician when a
glucose level is below 60 or above 400 mg/dL. With better blood glucose control, the need for such calls would diminish.
Intervention
To address the problems identified in the audit, the team decided to develop and implement a standardized sliding scale insulin protocol for inpatients with type 2 diabetes, by far the most common form of diabetes [10]. Standardizing the protocol would reduce the opportunities for errors such as omissions, wrong timing, and dosing mistakes due to misunderstood handwriting and abbreviations. Safety would be enhanced through the use of a preprinted order form that clearly designates the specific increments of insulin coverage [11].
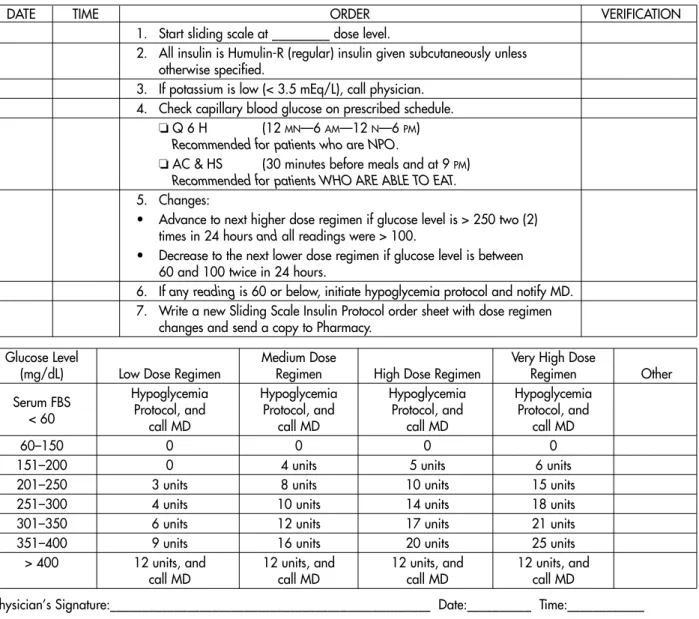
Sample insulin sliding scale orders that had been suc-cessfully used in other VHA member hospitals were down-loaded from VHA’s electronic database. Components of var-ious sample orders were selected and incorporated into a new form; the form was reviewed by BSA’s pharmacy and therapeutics committee, staff endocrinologists, and a family practice physician and revised based on their input. The pilot form is shown in Figure 1. The preprinted, standard-ized order form eliminates abbreviations and the need for handwriting that could lead to error. Four dosing regimens are identified. The form includes instructions for adjusting the dosing scale upward or downward based on specific parameters and nursing assessment data and indicates when the nurse is to contact a physician.
A pilot nursing unit serving family practice and a variety of medical and surgical patients was selected, and nurses
were instructed on the protocol during regularly scheduled staff meetings in late May 2001. The pharmacy manager educated pharmacists about the new order and protocol in staff meetings during the same period, and standard phar-macy computer input methods were developed to facilitate and standardize pharmacist order processing. The imple-mentation team mailed a sample order form and letter to all staff physicians, offering but not mandating the pilot proto-col. Soon after the physicians received the letter, many asked for the protocol to be made available throughout the institu-tion, not just on 1 nursing unit, and the pilot unit concept was abandoned. Nursing directors, with the help of BSA’s diabetes educator, quickly educated nurses about the proto-col on other patient care units.
The sliding scale insulin order sheet instructs the user to employ another protocol, the hypoglycemia protocol, when fasting blood sugar is below 60 mg/dL (Figure 1). Although the hypoglycemia protocol was a current part of nursing pol-icy, physicians, nurses, and pharmacists asked for informa-tion and clarificainforma-tion on this protocol. Medicainforma-tion floor stock levels were found to be inadequate to support protocol-based hypoglycemia care in some nursing units. Pharmacy and nursing personnel examined each floor’s automated dispensing cabinets, and each was stocked with 40% dex-trose oral gel, 50% dexdex-trose injection syringes, and glucagon injection sufficient to manage estimated need.
Measurement
The implementation team’s nurse QI reviewer collected data from pilot protocol orders on file in the pharmacy written between 7 June (pilot start date) and 17 July. Physicians from 9 specialties had used the protocol for 24 patients, or 13% of all patients who had received sliding scale insulin during this time. Mean blood glucose level decreased from 214.9 to 182.7 mg/dL. Glucose problems were reduced by more than half. Other comparative measures are shown in Table 1.
In August 2001, the team completed another round of data collection, reviewing the charts of the 27 patients for whom pilot protocol orders were written between 18 July and August 14. Of greatest interest was the control of the patients’ blood glucose. Data showed sustained improvement (Table 1). Phys-icians from 12 specialties had used the protocol.
Improvement Needs
Further education for physicians, nurses, and pharmacists is needed regarding patient selection for application of the standardized sliding scale insulin protocol. Chart review revealed that two type 1 diabetics were placed on the proto-col. For 1 patient, the protocol was discontinued and new orders written before the patient received any protocol-based treatment. The second patient received sliding scale insulin on the protocol and had inadequate blood glucose Table 1.Clinical and Performance Measures in Insulin Sliding
Scale Project
Protocol Protocol Baseline Group 1 Group 2
Measure n= 32 n= 24 n= 27
Glucose problem (< 60 or 47% 21% 15%
> 400 mg/dL)
Glucose ≥251 mg/dL 27% 5% 18%
Mean blood glucose, mg/dL 214.9 182.7 182
Median blood glucose, mg/dL 192 169 163
Interventions to treat 13 1 3
low blood glucose
Extra blood glucose 80 3 5
checks
Extra insulin doses 20 2 0
Calls made to physicians 55 5 7
for either high or low blood glucose readings
BSA
PHYSICIAN’S ORDERSStanding Sliding Scale Insulin
PILOT
INSULIN PROTOCOL FOR TYPE II DIABETICS
Not recommended for more than two (2) days as the only method of control.
REGIMENS:
• Low Dose Regimen: Suggested as starting point for the thin and elderly. • Moderate Dose Regimen: Suggested as the starting point for average weight. • High Dose Regimen: Suggested as the starting point for overweight patients.
• Very High Dose Regimen:Suggested as the starting point for patients with infections or those receiving steroids.
DATE TIME ORDER VERIFICATION
1. Start sliding scale at _________ dose level.
2. All insulin is Humulin-R (regular) insulin given subcutaneously unless otherwise specified.
3. If potassium is low (< 3.5 mEq/L), call physician. 4. Check capillary blood glucose on prescribed schedule.
❏ Q 6 H (12 MN—6 AM—12 N—6 PM)
Recommended for patients who are NPO.
❏ AC & HS (30 minutes before meals and at 9 PM)
Recommended for patients WHO ARE ABLE TO EAT.
5. Changes:
• Advance to next higher dose regimen if glucose level is > 250 two (2) times in 24 hours and all readings were > 100.
• Decrease to the next lower dose regimen if glucose level is between 60 and 100 twice in 24 hours.
6. If any readingis 60 or below, initiate hypoglycemia protocol and notify MD. 7. Write a new Sliding Scale Insulin Protocol order sheet with dose regimen
changes and send a copy to Pharmacy.
Glucose Level Medium Dose Very High Dose
(mg/dL) Low Dose Regimen Regimen High Dose Regimen Regimen Other Serum FBS Hypoglycemia Hypoglycemia Hypoglycemia Hypoglycemia
< 60 Protocol, and call MD Protocol, and call MD Protocol, and call MD Protocol, and call MD
60–150 0 0 0 0
151–200 0 4 units 5 units 6 units 201–250 3 units 8 units 10 units 15 units 251–300 4 units 10 units 14 units 18 units 301–350 6 units 12 units 17 units 21 units 351–400 9 units 16 units 20 units 25 units
> 400 12 units, and 12 units, and 12 units, and 12 units, and call MD call MD call MD call MD
Physician’s Signature:__________________________________________________ Date:__________ Time:____________
Suggested conversion to daily Humulin-N requirement:Use 3/4of total daily Humulin-R requirement as the total daily
Humulin-N requirement.
AFFIX PATIENT LABEL HERE
control. In addition, improved consistency is needed in doc-umenting blood glucose data in the patient chart diabetic record. At BSA, blood glucose values and sliding scale in-sulin doses must be documented both on the medication administration record (MAR) and in the patient diabetic chart record. Documentation on the MAR was very good. Documentation in the chart record, however, was sometimes not completed simultaneously, making patient assessment more time consuming. This has been addressed with nurs-ing education and procedural changes.
Changes to the order form also are needed. The next draft will state specificially the events that the nurse is to report to the physician, such as reporting that a patient’s food intake has changed. Boxes and lines on the form were distracting and interfered with clarity and will be revised or deleted as appropriate in the next version. The name of the form will be changed to make it clear that it is only for patients with type 2 diabetes and that the protocol is for sliding scale insulin cov-erage, (eg, “Type 2 diabetic sliding scale insulin protocol”).
The protocol is not recommended for more than 2 days as the only method of control. However, there is no reference on the form to long-acting insulins or oral antidiabetic agents that may be appropriate for the patient to continue while hospitalized. This also will be addressed in the next draft of the form. Further, a cautionary statement will be added that the protocol must not be used to manage diabetic ketoacido-sis. The revised form and protocol will become official in the hospital pending the pharmacy and therapeutics commit-tee’s approval.
Cost-Savings Analysis
BSA’s project implementation team performed an analysis to estimate cost avoidance associated with the standardized sliding scale insulin protocol. The team based their cost-saving analysis on the following assumptions:
• The number of BSA inpatients using sliding scale insulin in a year could be estimated from the pro-portion of sliding scale insulin patients in the base-line group, compared to total patients during the same time frame. Of 4995 inpatients in 3 months, 12%, or about 600, of these patients used sliding scale insulin. In 1 year, this totals 2400 patients. • Team members who were nurses estimated
nurs-ing time needed to treat high or low blood glu-cose (minimum of 30 minutes per episode), extra blood glucose checks and monitoring (minimum of 10 minutes per check), and telephone calls to physicians (at least 1 hour for telephone call, instructions, and documentation). This averaged 10.4 hours of extra nursing time per patient in the pre-protocol group with out-of-control blood
glu-cose. “Out of control” blood glucose was defined as less than 60 or greater than 400 mg/dL. A tele-phone call was required for each blood glucose reading outside this range, and often more than 1 intervention was needed.
• At the time of baseline data collection, the average salary and benefit cost per hour for a registered nurse was estimated conservatively at $21.75. This equated to $226.20 (10.4 hours x $21.75/hour) in salary and benefit time for a nurse to manage blood glucose that was too high or too low. Before pilot protocol introduction, however, BSA adjust-ed nursing salaries such that the average salary and benefit cost was $23.00 per hour. Therefore, the team estimated comparable excess nursing time cost in the protocol group to be $239.20 (10.4 hours x $23.00/hour).
• Out-of-control blood glucose has the potential to lead to an adverse drug event (ADE), with its attendant costs and hazards.
• The incidence of out-of-control blood glucose ings was calculated as the percentage of all read-ings under 60 and over 400 mg/dL in both the baseline and protocol groups. For estimation pur-poses, the same percentage estimate was used to calculate the number of patients in a year who could be at risk for experiencing a sliding scale insulin-related ADE.
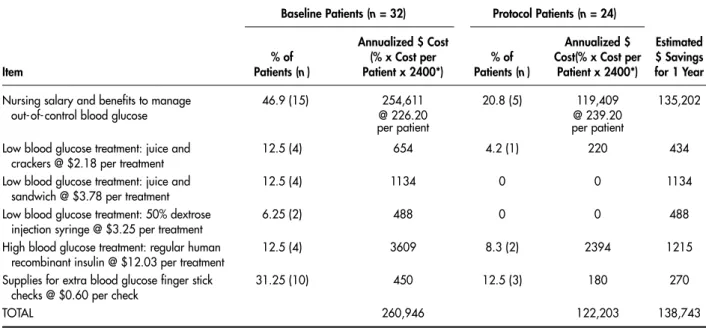
• Risk avoidance was calculated based on the dol-lars the hospital paid for claims associated with adverse drug events from October 1999 through March 2001, averaged over the number of report-ed preventable adverse drug events (mreport-edication errors) that reached patients during the same peri-od at BSA. The average amount per event was $2097. This figure excluded cost of insurance, legal fees, personnel costs, and supply expense. Using these assumptions, the team calculated dollar esti-mates for supplies, nursing time, and risk avoidance for both the baseline and protocol groups of patients. They extrapo-lated these estimates to the total number of patients using sliding scale insulin at BSA in 1 year. Comparisons of annu-alized cost estimates and savings are shown in Table 2. Pro-jected savings for risk avoidance are shown in Table 3. An-nualized potential savings projections totaled $340,055.
Applicability
Potential savings figures do not necessarily translate into identifiable dollars in the hospital’s bottom line. They are
“soft” dollars. These figures are useful primarily in con-structing estimates to cost-justify a project and appraise anticipated benefits. It is reasonable to expect an improve-ment of this nature to save the hospital money by increasing staff efficiency and by reducing unnecessary use of materi-als. The analysis we conducted is a method of attaching a value to increased efficiency and reduced wastage.
The savings estimate does not include costs associated with increased length of stay (LOS) due to lack of blood glu-cose control. To date, the team has not examined the LOS variable in this project. All of the patients in both the baseline or protocol groups were admitted to the hospital primarily for treatment of another condition, with diabetes as comor-bidity. A patient’s LOS was associated more closely with the
admitting diagnosis than with blood glucose control or lack thereof. The same was true of costs associated with level of care. In the patient charts examined, the team did not find any transfers to higher levels of care due to blood glucose control problems. Like LOS, the level of care was more close-ly related to the patient’s admitting diagnosis than to blood glucose control. Level of care cost variations were not includ-ed in cost estimates for this project. Both LOS and level of care may become important considerations as the project continues.
The results of this project may not be applicable to the needs of other institutions and patient populations. It is best described as a quality improvement effort, and adjustments and continued monitoring are necessary. The observed Table 2. Cost Analysis for Sliding Scale Insulin: Projected 1-Year Cost Savings
Baseline Patients (n = 32) Protocol Patients (n= 24)
Annualized $ Cost Annualized $ Estimated % of (% x Cost per % of Cost(% x Cost per $ Savings Item Patients (n) Patient x 2400*) Patients (n) Patient x 2400*) for 1 Year
Nursing salary and benefits to manage 046.9 (15) 254,611 20.8 (5) 119,409 135,202
out-of-control blood glucose @ 226.20 @ 239.20
per patient per patient
Low blood glucose treatment: juice and 12.5 (4) 654 4.2 (1) 220 434
crackers @ $2.18 per treatment
Low blood glucose treatment: juice and 12.5 (4) 1134 0 0 1134
sandwich @ $3.78 per treatment
Low blood glucose treatment: 50% dextrose 6.25 (2) 488 0 0 488
injection syringe @ $3.25 per treatment
High blood glucose treatment: regular human 12.5 (4) 3609 8.3 (2) 2394 1215
recombinant insulin @ $12.03 per treatment
Supplies for extra blood glucose finger stick 31.25 (10) 450 12.5 (3) 180 270
checks @ $0.60 per check
TOTAL 260,946 122,203 138,743
*Average nursing salary cost per hour changed between baseline and protocol data collection periods. Estimated number of sliding scale insulin patients at BSA in 1 year = 2400. See assumptions in text.
Table 3.Risk Avoidance: Projected Savings
Baseline Group Protocol Group
Number of Readings (n= 868) Number of Readings (n= 327) Annualized $ Cost Annualized $ Cost
Potential ADEs Potential ADEs Estimated % Potential (% x Cost per % Potential (% x Cost per $ Savings
Item ADEs ADE*x 2400) ADEs ADE*x 2400) for 1 Year
Blood glucose > 400 mg/dL 5.9 296,935 2.1 105,689 191,246
Blood glucose < 60 mg/dL 0.5 025,164 0.3 015,098 010,066
TOTAL 322,099 120,787 201,312
ADE = adverse drug event.
improvements may not be due solely to the new protocol, and the baseline and protocol groups may vary with respect to traits yet to be identified. The additional staff education and the attention focused on diabetes care in general are probably responsible for some positive changes.
Summary
An easy-to-use preprinted order form and standardized sliding scale insulin protocol for type 2 diabetics simplified the complex process of administering and monitoring a high-alert medication. Improved blood glucose control and more efficient use of resources were observed. Further ad-justment and improvement of the order form and protocol are planned, and continued quality improvement monitor-ing is needed.
BSA team members included the authors, Terry Ammerman, RN, MSN; Marty Farris, RN, CDE; Carla Jones; Susan Jones, RN, BSN; Marilyn Mays, RN; and Lou Rogers, RN, BS. The team gratefully acknowledges the support and advice of Dr. Charles V. Wright Jr, MD, MMM, Texas Tech University Health Sciences Center Medical School at Amarillo, physician advisor for the project. Thanks also to Dr. Ken Brantley, MD, PhD, for constructive comments and suggestions for improvements, and to Dr. Robert S. Urban, MD, Chair, BSA Pharm-acy and Therapeutics Committee.
Corresponding author: Margaret H. Bahlinger, MS, RPh, Pharmacy Manager, Baptist St. Anthony’s Health System, 1600 Wallace Blvd., Amarillo, TX 79106.
References
1. Cohen MR, Kilo CM. High-alert medications: safeguarding against errors. In: Cohen MR, editor. Medication errors. Wash-ington (DC): American Pharmaceutical Association; 1999. 2. Joint Commission on Accreditation of Healthcare
Organi-zations. High-alert medications and patient safety. Sentinel Event Alert 1999 Nov 19; Issue 11.
3. Argo AL, Cox KK, Kelly WN. The ten most common lethal medication errors in hospital patients. Hosp Pharm 2000; 35:470–4.
4. Hirsch IB, Farkas-Hirsch R. Sliding scale or sliding scare: it’s all sliding nonsense. Diabetes Spectrum 2001;14:79–81. 5. Bergenstal RM, Fish LH, List S. The insulin sliding scale is
not dead. Arch Intern Med 1998;158:298.
6. Nath C, Ponte CD. Lessons learned about insulin therapy. Nursing 2000;30:40–5.
7. American Diabetes Association. Insulin administration [position statement]. Diabetes Care 2001;24(Suppl 1):S94–7. 8. Kendall DM, Bergenstal RM. Comprehensive management
of patients with type 2 diabetes: establishing priorities of care. Am J Manag Care 2001;7(10 Suppl):S327–43.
9. Standards of medical care for patients with diabetes mellitus. American Diabetes Association. Diabetes Care 1994;17:616–23 10. Centers for Disease Control and Prevention. National dia-betes fact sheet: national estimates and general information on diabetes in the United States. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 1998.
11. Smetzer J, Cohen MR. Safety briefs. ISMP medication safety alert! 2001;6:2.