Office-Based Intervention to Reduce Bottle Use Among
Toddlers: TARGet Kids! Pragmatic, Randomized Trial
WHAT’S KNOWN ON THIS SUBJECT: Observational studies suggest associations between prolonged bottle-feeding, excessive milk intake, and iron deficiency. The AAP recommends complete bottle-weaning by 15 months, but many parents bottle-feed much longer. No evidence-based interventions exist to promote timely bottle-weaning.
WHAT THIS STUDY ADDS: This pragmatic trial of an educational intervention did not result in a decrease in iron deficiency but did result in a 60% reduction in prolonged bottle use. This is the first study to demonstrate a reduction in bottle use.
abstract
OBJECTIVE:The goal was to determine whether an office-based, edu-cational intervention for parents of 9-month-old children could reduce bottle use and iron depletion at 2 years of age.
METHODS:Between January 2006 and 2007, 251 healthy, 9-month-old infants attending a routine health maintenance visit were assigned randomly to intervention or control groups. Parents in the intervention group were introduced to a 1-week protocol to wean their children from the bottle. Iron depletion (ferritin levels of⬍10g/L) and bottle use at 2 years were assessed.
RESULTS:A total of 201 children were monitored to 2 years of age (follow-up rate: 81%). Rates of iron depletion (10 [10%] of 102 children vs 13 [13%] of 99 children;P⫽.42) and milk consumption of⬎16 oz (16 [16%] of 102 children vs 17 [17%] of 99 children; P⫽.7) were not significantly different between the 2 groups at 2 years of age. However, children in the intervention group started using a cup 3 months earlier (9 vs 12 months;P⫽.001), were weaned from the bottle 4 months earlier (12 vs 16 months;P⫽.004), and were more than one-half as likely to be using a bottle at 2 years of age (15 [15%] of 102 children vs 39 [40%] of 99 children;P⫽.0004).
CONCLUSIONS:This simple intervention administered during a health maintenance visit did not result in a decrease in iron depletion at 2 years of age but did result in a 60% reduction in prolonged bottle use.
Pediatrics2010;126:e343–e350 AUTHORS:Jonathon L. Maguire, MD, MSc, FRCPC,a,b,c,d,e
Catherine S. Birken, MD, MSc, FRCPC,b,c,d,eSheila Jacobson, MD,b,c,dMichael Peer, MD,b,c,dCarolyn Taylor, MD,b,c,dAmina Khambalia, PhD,c,dMagda Mekky, MSc,c,d Kevin E. Thorpe, MMath,a,fand Patricia Parkin, MD, FRCPCb,c,d,e
aApplied Health Research Centre, Li Ka Shing Knowledge Institute, St Michael’s Hospital,bDepartment of Pediatrics, Faculty of Medicine, andfDivision of Biostatistics, Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario, Canada;cDivision of Pediatric Medicine anddPediatric Outcomes Research Team, Hospital for Sick Children, Toronto, Ontario, Canada; andeChild Health Evaluative Sciences, Hospital for Sick Children Research Institute, Toronto, Ontario, Canada
KEY WORDS
randomized, controlled trial, bottle-feeding, iron deficiency anemia, infant, child, preschool, ambulatory care, health promotion
ABBREVIATIONS
AAP—American Academy of Pediatrics CI— confidence interval
This trial has been registered at www.clinicaltrials.gov (identifier NCT00907088).
www.pediatrics.org/cgi/doi/10.1542/peds.2009-3583
doi:10.1542/peds.2009-3583
Accepted for publication Apr 23, 2010
Address correspondence to Jonathon L. Maguire, MD, MSc, FRCPC, Applied Health Research Centre, Li Ka Shing Knowledge Institute, Department of Pediatrics, St Michael’s Hospital, 61 Queen St East, 2nd Floor, Toronto, Ontario, Canada M5C 2T2. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
15 to 18 months of age, excessive milk intake, and iron deficiency.1–4On the
basis of data from 120 healthy children 12 to 38 months of age, we found that 37% of bottle-fed infants had low iron stores, compared with 18% of cup-fed infants.5Similarly, Bonuck and Kahn,6
in a cross-sectional analysis of data for 95 children 18 months to 5 years of age, found that 25% of children with iron deficiency anemia were still using a bottle, whereas only 15% of children without iron deficiency anemia were bottle-users. Brotanek et al,7 using
data for 2121 children in National Health and Nutrition Examination Sur-vey III (1988 –1994), found a nearly threefold increase in the odds of iron deficiency for children who were weaned from the bottle late (between 24 and 48 months), compared with children who were weaned before 12 months of age.
The American Academy of Pediatrics (AAP) recommends complete bottle-weaning for healthy children by 15 months of age.8 However, many
par-ents choose to feed their children by bottle much beyond this age. Hammer et al,9in a cross-sectional analysis of
data for 191 healthy, middle class tod-dlers, found that 40% were bottle-fed at 24 months, 16% at 36 months, and 8% at 48 months. Similarly, Safer et al4
found that 18% of 165 middle class children were still using a bottle at 42 months of age. Brotanek et al,7using
data from National Health and Nutri-tion ExaminaNutri-tion Survey III, found that 37% of 603 Mexican American children were bottle-fed beyond 2 years of age.
A survey of 180 parents of children 12 to 36 months of age found that late-weaning parents tended to be less knowledgeable about weaning recom-mendations and negative health con-sequences associated with late wean-ing, compared with parents of children
weaning time reported by
late-weaning parents was 5 months later than that reported by parents who weaned their children in a timely man-ner (19.9 months vs 13.6 months). Bro-tanek et al,11through semi-structured
interviews with 37 parents of Mexican American toddlers, determined that convenience and lack of knowledge re-garding iron deficiency and bottle-weaning recommendations were ma-jor barriers to bottle-weaning. Parents also reported not receiving enough ed-ucation from physicians.
Physicians’ uncertainty regarding bottle-weaning recommendations may con-tribute to parents’ uncertainty. In a survey of 118 urban, Canadian pedia-tricians regarding anticipatory guid-ance on bottle-weaning, we showed that 17% of pediatricians reported not routinely providing recommendations. Of the respondents who provided rec-ommendations routinely, 78% did not know the AAP recommendations re-garding bottle-weaning.12 Similarly,
data from a survey of 687 AAP mem-bers found that 88% of general pedia-tricians did not know AAP bottle-weaning recommendations and only 44% routinely told parents that pro-longed bottle-feeding can lead to iron deficiency.13 The objective of this
study was to evaluate the effective-ness of a brief, pediatric office-based, bottle-weaning educational intervention for parents of 9-month-old children for the prevention of prolonged bottle-feeding and iron depletion at 2 years of age.
METHODS
Study Design
This study was conducted as a prag-matic, randomized, controlled trial. Pragmatic, randomized, controlled tri-als aim to maximize the applicability of trial results by assessing the
effective-participants.14–16
Participants
The parents of healthy infants ⬃9 months of age who were attending a routine, 9-month, health maintenance visit with their primary care pediatri-cians were approached for participa-tion. Children were excluded if they had birth weights of ⬍2 kg, had a chronic illness other than asthma, had previously diagnosed anemia, or were currently receiving iron supplements. Study participants were recruited be-tween January 2006 and January 2007 from a 3-physician (Drs Jacobson, Peer, and Taylor), community-based, pediatric group practice located in To-ronto, Canada. This practice is partici-pating in TARGet Kids! (Toronto Area Re-search Group), a university-affiliated, practice-based, primary care research network. Characteristics assessed at baseline, including age, gender, birth weight, parents’ ethnicity and maximal education, breastfeeding history, bot-tle use, plans to wean from the breast or bottle, cow’s milk and juice intake, and day care attendance, were col-lected by using a parent-completed, standardized, data collection form.
Interventions
Parents of children in both the interven-tion and control groups received stan-dardized counseling on healthy nutrition, which was based on Canadian Paediatric Society guidelines,17from trained study
book endorsed by the Hospital for Sick Children.19
During the same 9-month visit, parents of infants assigned to the intervention group also were given a sippy cup (Avent Magic Cup [Koninklijke Philips Electronics NV, Eindhoven, The Nether-lands]) and were shown how to use it. A trained research assistant told par-ents in the intervention group about the risks of continued bottle use, includ-ing tooth decay, iron deficiency anemia, and iron deficiency-associated behavior problems and poorer school achieve-ment. Parents were instructed to limit daily milk consumption to 16 oz and were counseled to discontinue bottle use in the following week by using a stepwise protocol, which was de-scribed on a handout to be placed on the refrigerator (Appendix 1). This counseling was repeated at the child’s 15-month visit if the child had not yet transitioned to use of a cup. Parents of
infants assigned to the control group did not receive this information. All counseling was delivered by the same nutrition-trained research assistant, who was instructed to maintain blind-ing for the attendblind-ing physicians.
Outcomes
All outcomes were measured at 2 years of age, during the child’s routine, 2-year, health maintenance appoint-ment. Follow-up assessment at 2 years was chosen empirically to allow suffi-cient time for prolonged bottle-feeding to affect iron stores.
The primary outcome was iron depletion at 2 years of age, defined as serum fer-ritin levels ofⱕ10g/L.20,21Blood
sam-ples were obtained during the children’s
physician appointments and were
transported on ice to the biochemis-try laboratory at the Hospital for Sick Children each day. Ferritin levels were analyzed by using a Siemens Immulite 2500 analyzer (Siemans
Healthcare Diagnostics Inc, Deer-field, IL).
Secondary outcomes were prolonged bottle use (defined as daytime or nighttime bottle use at 2 years of age) and nighttime bottle use (defined as bottle use while the child was in bed). Covariates included daily milk con-sumption, daily juice concon-sumption, age at cup introduction, age at bottle-weaning, breastfeeding, age at wean-ing from the breast, barriers to bottle-weaning, and BMI. BMI was calculated as weight (in kilograms) divided by height (in square meters).22,23 Weight
was measured (⫾0.025%) by using a precision digital scale (SECA, Ham-burg, Germany), and standing height was measured by using a stadiometer (SECA). Nutritional survey data were collected by using a standardized, parent-completed, data collection form adapted from the Canadian Community Health Survey.24
Sample Size
The prevalence of iron depletion among bottle-fed children in our previ-ous, cross-sectional study of children recruited from the same practice was 37%, and the prevalence of iron deple-tion among cup-fed children was 18%.5
With the assumption of a prevalence of iron depletion in the control group of 37% and a prevalence of iron depletion in the intervention group of 20%, a sample size of 100 children per group would maintain a type 1 error of .05 and a power of 80% with a 2-sided test. Therefore, random assignment of 120 children per group at 9 months was chosen to accommodate a 20% loss to follow-up monitoring at 2 years of age.
Randomization
Patients were assigned randomly by us-ing a computerized, random-number generator, and assignment concealment was maintained through the use of se-quentially numbered, opaque, sealed
en-velopes. The assignment sequence was generated by the research coordinator (Ms Mekky), and the research assistant enrolled participants and assigned par-ticipants to their groups.
Blinding
Attending pediatricians, laboratory personnel, and study personnel who conducted the 2-year outcome assess-ments were blinded to the group as-signments. Although blinding of par-ents to the educational intervention was not possible, parents were not in-formed of the group assignment or the exact nature of the study, except that it was a study on toddler nutrition. Par-ents in the 2 groups received identical bags weighted with the provided nutri-tion book, to mask the sippy cup, and were asked not to discuss the study with parents of other children.
Statistical Analyses
An intention-to-treat (intervention group versus control group) analysis was performed. Differences between con-tinuous variables were analyzed by us-ing Student’s t test, and differences between categorical variables were analyzed by using exact methods. Ad-justments for obvious baseline differ-ences were accomplished through lo-gistic regression modeling, with iron depletion or bottle use at 2 years as binary outcome variables and group assignment as the exposure variable. All data were analyzed by using SAS 9.0 (SAS Institute, Cary, NC).
Ethics Approval
All parents of participating children consented to participate. This study was approved by the research ethics board of the Hospital for Sick Children.
RESULTS
Participant Flow and Recruitment Participant flow through the trial is summarized in Fig 1. A total of 301
tients were assessed for eligibility and 251 children were assigned randomly to intervention or control groups be-tween January 2006 and January 2007; 102 children in the intervention group and 99 children in the control group underwent follow-up assessments at 2 years of age (81% follow-up rate for both groups), between April 2007 and May 2008.
Baseline Data
Baseline characteristics of children in the intervention and control groups at 9 months of age are presented in Table 1. Children in the 2 groups had similar ages, gender distributions, race/eth-nicity distributions, birth weights, and BMI values (BMI is not calculated in routine practice for children⬍2 years of age but is presented here for de-scriptive purposes). The groups had
postsecondary education. The popula-tion was mainly white, with highly edu-cated mothers and a high rate (50%) of breastfeeding at 9 months of age. Chil-dren in the intervention group had par-ents who less frequently reported planning to wean from the children from the bottle by 2 years of age (84% vs 91%) and more frequently reported providing cow’s milk for the children (12% vs 4%).
Intention-to-Treat Analysis
In the intention-to-treat analysis, there was no difference in iron depletion at 2 years of age for children in the inter-vention and control groups (12% vs 17%;P⫽.42) (Table 2). However, chil-dren in the intervention group were less likely to be using a bottle during the day at 2 years (15% vs 40%;P⫽
.0004) and were less likely to be using a bottle in bed (3% vs 10%;P⫽.05) (Tables 2 and 3). Children in the
inter-Excluded (n=50)
Not meeting inclusion (n=10) Refused to participate (n=40)
Randomized (n=251)
Intervention group (n=129)
Control group (n=122)
Follow-up at 2 years (n=102, 81%)
Follow-up at 2 years (n=99, 81%) Withdrew (n=2)
Lost to f/u (n=22)
Withdrew (n=1) Lost to f/u (n=22) 15 Month top-up intervention
(n=126)
Withdrew (n=2) Lost to f/u (n=1)
FIGURE 1
Participant flow through trial. f/u indicates follow-up monitoring.
TABLE 1 Baseline Characteristics at 9 Months of Age
N Intervention (N⫽129) Control (N⫽122)
Child age, mo 250
Median (IQR) 9.16 (9.03–9.42) 9.10 (9.03–9.32)
Mean⫾SD 9.25⫾0.38 9.24⫾0.41
Male, % (n) 251 49 (63) 57 (69)
Birth weight, kg 240
Median (IQR) 3.27 (3.00–3.61) 3.36 (3.12–3.61)
Mean⫾SD 3.31⫾0.46 3.33⫾0.42
Child BMI, kg/m2 240
Median (IQR) 16.5 (15.2–17.5) 16.9 (15.9–18.0)
Mean⫾SD 16.5⫾1.7 16.9⫾1.5
Feeding, % (n) 246
Breast only 30 (38) 38 (46)
Bottle only 49 (61) 50 (60)
Breast and bottle 21 (26) 12 (15)
Plan to bottle-wean by 2 y, % (n) 149 84 (63) 91 (67) Drinking cow’s milk, % (n) 250 12 (16) 4 (5) Attending day care, % (n) 251 14 (18) 10 (12) Mother’s education, % (n) 251
Elementary school 0 (0) 0 (0)
High school 14 (18) 11 (13)
University/college 86 (111) 89 (109)
Race/ethnicity, % (n) 251
White 71 (92) 70 (85)
Asian 9 (12) 15 (18)
Hispanic 14 (18) 11 (13)
Black 5 (7) 5 (6)
vention group, compared with children in the control group, started using a cup 3 months earlier (median: 9 vs 12 months; P⫽.001) and were weaned from the bottle 4 months earlier
(me-dian: 12 vs 16 months;P⫽.004). Daily cow’s milk intake (median: 14 vs 12 oz;
P⫽.7) and juice intake (median: 5 vs 4 oz;P⫽.6) were similar in the 2 groups.
With adjustment for baseline group dif-ferences in gender, parents’ plans for bottle-weaning before 2 years, and cow’s milk use at 9 months, the risk of iron depletion in the intervention group, compared with the control group, remained nonsignificant (abso-lute risk difference: 0.05 [95% confi-dence interval [CI]:⫺0.07 to 1.6]) (Ta-ble 4). However, differences in bottle use in the intervention group, com-pared with the control group, during
the day (absolute risk difference: 0.25 [95% CI: 0.13– 0.37]) and in bed (abso-lute risk difference: 0.07 [95% CI: 0.003– 0.14]) at 2 years remained significant.
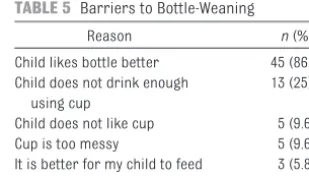
Barriers to Bottle-Weaning
When asked to choose among 5 rea-sons for continued bottle use at 2 years, 86% of parents of children using the bottle reported that the child “likes the bottle better than the cup” (Table 5). The second most common re-sponse (25%) was that the child “does not drink enough using a cup.”
DISCUSSION
This pragmatic, randomized, con-trolled trial of a brief educational in-tervention administered to parents of 9-month-old children during a health maintenance visit was not able to dem-onstrate a reduction in iron depletion
TABLE 2 Results of Intention-to-Treat Analysis (2-Year Follow-up Evaluation)
N Intervention (N⫽102) Control (N⫽99)
Iron depletion, % (n) 158
No 88 (71) 83 (64)
Yes 12 (10) 17 (13)
Ferritin level,g/L 158
Median (IQR) 22 (15–28) 21 (13–35)
Mean⫾SD 24⫾15 26⫾18
Bottle use during day, % (n) 194
No 85 (82) 60 (58)
Yes 15 (15) 40 (39)
Bottle use in bed, % (n) 195
No 97 (95) 90 (87)
Yes 3 (3) 10 (10)
BMI, kg/m2 194
Median (IQR) 16.0 (15–16.9) 15.8 (14.8–16.7)
Mean⫾SD 16.1⫾1.5 15.8⫾1.6
Age at cup start, mo 192
Median (IQR) 9.0 (8.0–12.0) 12.0 (8.0–12.0)
Mean⫾SD 9.4⫾2.5 11.0⫾3.9
Age at bottle-weaning, mo 90
Median (IQR) 12.0 (10.6–16.0) 16.0 (12.0–19.0)
Mean⫾SD 13.4⫾4.3 16.0⫾4.1
Daily cow’s milk intake, oz 180
Median (IQR) 14.0 (9.0–16.0) 12.0 (8.0–16.0)
Mean⫾SD 13.1⫾5.6 12.8⫾5.4
⬎16 oz of milk per d, % (n) 180
No 83 (77) 80 (70)
Yes 17 (16) 20 (17)
Daily juice intake, oz 167
Median (IQR) 5.0 (3.0–7.8) 4.0 (2.0–7.0)
Mean⫾SD 5.6⫾4.2 5.4⫾4.0
⬎8 oz of juice per d, % (n) 167
No 90 (77) 85 (69)
Yes 10 (9) 15 (12)
Breastfeeding at 2 y, % (n) 195
Yes 8 (8) 5 (5)
No 92 (90) 95 (92)
Age at breast-weaning, mo 106
Median (IQR) 9.0 (4.2–12.0) 12.0 (6.0–16.0)
Mean⫾SD 9.9⫾6.5 11.2⫾6.0
Nvalues are numbers of nonmissing values. IQR indicates interquartile range.
TABLE 3 SelectedPValues in Intention-to-Treat Analysis
Outcome P
Iron depletion .419
Ferritin level .387
Bottle use 1⫻e⫺4
Age at cup start .001
Age at bottle-weaning .004
For iron depletion and bottle use,2tests (without conti-nuity correction) were used. The rest of the outcomes were tested with Welchttests (which allowed for non-equal variances).
TABLE 4 Adjusted Treatment Effect Estimates
Outcome Treatment Effect (95% CI)
Iron depletion 0.045 (⫺0.065 to 0.156) Ferritin level 2.268 (⫺2.897 to 7.433) Bottle use during day 0.247 (0.126–0.369) Bottle use in bed 0.072 (0.003–0.142) BMI ⫺0.275 (⫺0.714 to 0.163) Age at cup start 1.562 (0.635–2.49) Age at bottle-weaning 2.662 (0.864–4.46) Daily cow’s milk intake ⫺0.275 (⫺1.9 to 1.349) ⬎16 oz of milk per d 0.023 (⫺0.09 to 0.137) Daily juice intake ⫺0.26 (⫺1.51 to 0.99) ⬎8 oz of juice per d 0.043 (⫺0.057 to 0.144) Breastfeeding at 2 y ⫺0.03 (⫺0.1 to 0.04) Age at breast-weaning 1.301 (⫺1.105 to 3.707)
The treatment effect is expressed as an absolute risk dif-ference for dichotomous outcomes and as the difdif-ference in means for continuous outcomes (control⫺ interven-tion for all outcomes).
TABLE 5 Barriers to Bottle-Weaning
Reason n(%)
Child likes bottle better 45 (86.5) Child does not drink enough
using cup
13 (25)
Child does not like cup 5 (9.6) Cup is too messy 5 (9.6) It is better for my child to feed
by bottle
3 (5.8)
Although 54 subjects reported bottle use at 2 years, data on the reasons were completely missing for 2 subjects. Therefore, this table uses a denominator of 52 throughout.
dren with prolonged bottle use (at 2 years) reported intense child motiva-tion for continued bottle use.
One of the major strengths of our study was the pragmatic nature of the inter-vention. Because the intervention re-quired⬍5 minutes for administration, primary care physicians could provide it routinely. We chose to test the inter-vention at the 9-month visit, when no routine vaccinations are scheduled, to allow time for this additional anticipa-tory guidance. Nine months also is an ideal age at which to emphasize the importance of nutrition in the second and third years of life.
Two other randomized, controlled tri-als of educational interventions re-garding bottle-weaning were reported, neither of which demonstrated a re-duction in bottle use. Kahn et al25
ran-domly assigned 48 Hispanic children, 18 to 30 months of age, from 3 Supple-mental Nutrition Program for Women, Infants, and Children sites in New York City to a parental bottle-weaning edu-cational intervention, with follow-up evaluations after 2 months. This inter-vention included a scripted 4-step pro-tocol for bottle-weaning. Although there was no significant difference in bottle use in the intervention and con-trol groups after 2 months (50% vs 67%;P⫽.3), children in the interven-tion group consumed ⬃1 bottle per day less than did children in the con-trol group. Findings from that study might have been limited because of the broad, late age range at the time of the intervention and the relatively short follow-up period.
Franco et al26randomly assigned 185
black children, 4 months of age, from an inner-city, pediatric clinic in Louis-ville, Kentucky, to a parental bottle-weaning educational intervention, with follow-up evaluations between 12 and 24 months of age. The intervention
scripted counseling protocol for im-mediate nighttime bottle cessation, with complete bottle-weaning recom-mended by 12 months of age. At the follow-up evaluations, there was no difference in bottle use in the inter-vention and control groups (73% vs 83%; P ⫽ .2) and no difference in dental caries.
We speculate that our bottle-weaning intervention reduced bottle use for a number of reasons. First, the interven-tion was brief, with a clear message regarding the dangers of prolonged bottle use. Second, the intervention ex-pressed urgency regarding the need to wean children from the bottle, cause we suspected that weaning be-comes much more difficult as the child enters the second year of life. Indeed, our data support this hypothesis. Chil-dren in the intervention group were in-troduced to the cup 1.6 months earlier and were weaned from the bottle 2.6 months earlier than were children in the control group. Furthermore, chil-dren with bottle use at 2 years of age were introduced to the cup 1.6 months later than were children who had been weaned successfully (11.4 vs 9.8 months).
Third, the intervention was provided at a sufficiently young age (9 months) that the child’s behavior could be mod-ified with minimal resistance. Our data also support this; 83% of parents of children with bottle use at 2 years of age reported that the main reason for not weaning the child from the bottle was that the child “likes the bottle bet-ter than the cup.”
Fourth, our population included a large proportion of children with well-educated mothers. Such parents may be more successful at effecting behav-ior change in their children than are parents of lower socioeconomic status. Finally, the intervention was endorsed by
ing guidance.
This study was not able to demon-strate a reduction in iron depletion as a result of timely bottle-weaning. Insuf-ficient study power might have ac-counted for this. The prevalence of iron depletion in the control group was 14%, which was substantially lower than the 37% found in our previous work from the same physician prac-tice (which guided our sample size cal-culation).5
We chose to have research assistants
perform the placebo counseling ses-sion, to maintain the blinding of par-ents and attending physicians and to minimize the risk of contamination. However, the detailed nutritional infor-mation provided (which included ap-propriate timing of initiation of solid foods, iron-containing food choices, and limitation of juice intake, accord-ing to Canadian Paediatric Society recommendations) might have been more intensive than that provided by primary care providers in routine practice.17We suggest that the
unex-pectedly low prevalence of iron de-pletion in the control group might have resulted in part from the posi-tive effects of the placebo counseling on iron stores.
In addition, better adherence to the AAP guideline on milk intake might have been a factor, because the pri-mary care physicians caring for these children reported discussing this guideline routinely with patients since participation in our earlier observa-tional study.5 Indeed, the observation
demonstrate an effect of bottle cessa-tion on iron stores.
Contamination also might have con-tributed to a lack of effect. Although much effort was made to minimize the risk of contamination, including having research assistants and not the pri-mary care physicians administer the intervention, to maintain physician blinding, parents in the intervention group still might have discussed the intervention with their parent friends in the control group. Finally, because the probability of iron depletion in-creases as the duration of bottle use
increases, it is possible that differ-ences in iron depletion may be realized when these children are older (eg, 3 or 4 years of age).5
This pragmatic, randomized, con-trolled trial of a bottle-weaning educa-tional intervention at the 9-month health maintenance visit was not able to demonstrate a reduction in iron de-pletion but was very effective in reduc-ing prolonged bottle use. Additional studies are needed to determine whether decreasing prolonged bottle use could lead to a reduction in iron depletion in higher-risk populations,
as well as other proposed conse-quences of prolonged bottle-feeding, including bottle-related caries, otitis
media, and behavior problems.
ACKNOWLEDGMENTS
This study was supported by a grant-in-aid from the Danone Institute of Canada. The Pediatric Outcomes Re-search Team is supported by a grant
from the Hospital for Sick Children Foun-dation. Dr Maguire was supported by a Canadian Institutes of Health Research fellowship.
REFERENCES
1. Kaste LM, Gift HC. Inappropriate infant bot-tle feeding: status of the Healthy People 2000 objective.Arch Pediatr Adolesc Med. 1995;149(7):786 –791
2. Lampe JB, Velez N. The effect of prolonged bottle feeding on cow’s milk intake and iron stores at 18 months of age.Clin Pediatr (Phila).1997;36(10):569 –572
3. Northstone K, Rogers I, Emmett P. Drinks consumed by 18-month-old children: are current recommendations being followed? Eur J Clin Nutr.2002;56(3):236 –244
4. Safer DL, Bryson S, Agras WS, Hammer LD. Prolonged bottle feeding in a cohort of children: does it affect caloric intake and dietary composition?Clin Pediatr (Phila). 2001;40(9):481– 487
5. Sutcliffe TL, Khambalia A, Westergard S, Ja-cobson S, Peer M, Parkin PC. Iron depletion is associated with daytime bottle-feeding in the second and third years of life.Arch Pe-diatr Adolesc Med.2006;160(11):1114 –1120
6. Bonuck KA, Kahn R. Prolonged bottle use and its association with iron deficiency ane-mia and overweight: a preliminary study. Clin Pediatr (Phila).2002;41(8):603– 607
7. Brotanek JM, Halterman JS, Auinger P, Flores G, Weitzman M. Iron deficiency, pro-longed bottle-feeding, and racial/ethnic dis-parities in young children. Arch Pediatr Adolesc Med.2005;159(11):1038 –1042
8. Korsch M, Nelson K, Reinhart J. Feeding be-haviors in infancy and early childhood. In: Guidelines for Health Supervision III. Elk Grove Village, IL: American Academy of Pediatrics; 1997:57– 65
9. Hammer LD, Bryson S, Agras WS. Develop-ment of feeding practices during the first 5 years of life.Arch Pediatr Adolesc Med. 1999;153(2):189 –194
10. Frazier JP, Countie D, Elerian L. Parental bar-riers to weaning infants from the bottle.Arch Pediatr Adolesc Med.1998;152(9):889 – 892
11. Brotanek JM, Schroer D, Valentyn L, Tomany-Korman S, Flores G. Reasons for prolonged bottle-feeding and iron deficiency among Mexican-American toddlers: an ethnographic study.Acad Pediatr.2009;9(1):17–25
12. Sutcliffe TL, Parkin PC. Anticipatory guidelines for bottle weaning: a survey of pediatricians. Paediatr Child Health.2002;7(suppl A):43A
13. Brotanek JM, Deisz M, Lin H, Santoyo J, Lopez D, Flores G. Knowledge, beliefs, and anticipatory guidance practices regarding prevention of iron deficiency in toddlers: a national survey of US pediatricians. E-PAS2009:2819.205. Available at: www.pas-meeting.org/2009Baltimore/Abstracts/ default.asp. Accessed March 15, 2010
14. Zwarenstein M, Treweek S, Gagnier JJ, et al. Improving the reporting of pragmatic trials: an extension of the CONSORT statement. BMJ.2008;41(8):a2390
15. Thorpe KE, Zwarenstein M, Oxman AD, et al. A pragmatic-explanatory continuum indica-tor summary (PRECIS): a tool to help trial designers.CMAJ.2009;180(10):E47–E57
16. Thorpe KE, Zwarenstein M, Oxman AD, et al. A pragmatic-explanatory continuum indicator summary (PRECIS): a tool to help trial design-ers.J Clin Epidemiol.2009;62(5):464 – 475
17. Canadian Paediatric Society; Dieticians of Canada; Health Canada. Nutrition for Healthy Term Infants. Ottawa, Canada: Min-ister of Public Works and Government Services; 2005. Available at: www.hc-sc.gc.ca/fn-an/pubs/infant-nourrisson/ nut_infant_nourrisson_term-eng.php. Ac-cessed April 1, 2010
18. Health Canada. Canada’s Food Guide.
Ottawa, Canada: Health Canada; 2008. Avail-able at: www.hc-sc.gc.ca/fn-an/food-guide-aliment/index-eng.php. Accessed April 1, 2010
19. Kalnins D, Saab J.Better Baby Food: Your Essential Guide to Nutrition, Feeding & Cooking for All Babies & Toddlers. Toronto, Canada: Robert Rose; 2001
20. Centers for Disease Control and Prevention, Expert Scientific Working Group. Summary of a report on assessment of the iron nutri-tional status of the United States popula-tion.Am J Clin Nutr.1985;42(6):1318 –1330 21. Guyatt GH, Oxman AD, Ali M, Willan A, McIlroy
W, Patterson C. Laboratory diagnosis of iron-deficiency anemia: an overview.J Gen Intern Med.1992;7(2):145–153
22. Mei Z, Grummer-Strawn LM, Pietrobelli A, Goulding A, Goran MI, Dietz WH. Validity of body mass index compared with other body-composition screening indexes for the assessment of body fatness in children and adolescents. Am J Clin Nutr.2002;75(6): 978 –985
23. Pietrobelli A, Faith MS, Allison DB, Gallagher D, Chiumello G, Heymsfield SB. Body mass index as a measure of adiposity among chil-dren and adolescents: a validation study. J Pediatr.1998;132(2):204 –210
24. Statistics Canada. Canadian Community Health Survey. Available at: www.statcan.gc. ca/concepts/health-sante/content-contenu-eng.htm. Accessed April 1, 2010
25. Kahn R, Bonuck K, Trombley M. Randomized controlled trial of bottle weaning intervention: a pilot study.Clin Pediatr (Phila).2007;46(2): 163–174
26. Franco S, Theriot J, Greenwell A. The influence of early counselling on weaning from a bottle. Community Dent Health.2008;25(2):115–118
DOI: 10.1542/peds.2009-3583 originally published online July 12, 2010;
2010;126;e343
Pediatrics
Taylor, Amina Khambalia, Magda Mekky, Kevin E. Thorpe and Patricia Parkin
Jonathon L. Maguire, Catherine S. Birken, Sheila Jacobson, Michael Peer, Carolyn
Pragmatic, Randomized Trial
Office-Based Intervention to Reduce Bottle Use Among Toddlers: TARGet Kids!
Services
Updated Information &
http://pediatrics.aappublications.org/content/126/2/e343 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/126/2/e343#BIBL This article cites 20 articles, 3 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/breastfeeding_sub Breastfeeding
http://www.aappublications.org/cgi/collection/nutrition_sub Nutrition
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2009-3583 originally published online July 12, 2010;
2010;126;e343
Pediatrics
Taylor, Amina Khambalia, Magda Mekky, Kevin E. Thorpe and Patricia Parkin
Jonathon L. Maguire, Catherine S. Birken, Sheila Jacobson, Michael Peer, Carolyn
http://pediatrics.aappublications.org/content/126/2/e343
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.