ARTICLE
Expert Survey for the Management of Adolescent
Depression in Primary Care
Amy H. Cheung, MDa, Rachel A. Zuckerbrot, MDb, Peter S. Jensen, MDb, Ruth E. K. Stein, MDc, Danielle Laraque, MDd,
the GLAD PC Steering Committee
aDepartment of Psychiatry, University of Toronto, Toronto, Ontario, Canada;bDivision of Child Psychiatry, Columbia University/New York State Psychiatric Institute, New York, New York;cREACH Institute, Resources for Advancing Children’s Health, New York, New York;dDepartment of Pediatrics, Mount Sinai School of Medicine, New York, New York
Financial Disclosure: Dr Cheung is on the Speakers’ Bureau of Eli Lilly; Dr Jensen has received several unrestricted educational grants from Eli Lilly, McNeil, and Janssen-Ortho and is a consultant for Shire-Richwood, UCB Pharma, McNeil, and Janssen-Ortho and is also on the Speakers’ Bureau for UCB Pharma, McNeil, and Janssen-Ortho. The other authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.Primary care clinics have become the “de facto” mental health clinics for teens with mental health problems such as depression; however, there is little guidance for primary care professionals who are faced with treating this population. This study surveyed experts on key management issues regarding adolescent depres-sion in primary care where empirical literature was scant or absent.
METHODS.Participants included experts from family medicine, pediatrics, nursing, psy-chology, and child psychiatry, identified through nonprobability sampling. The ex-pert survey was developed on the basis of information from focus groups with patients, families, and professionals and from the research literature and included sections on early identification, assessment and diagnosis, initial management, treat-ment, and ongoing management. Means, standard deviations, and confidence inter-vals were calculated for each survey item.
RESULTS.Seventy-eight of 81 experts agreed to participate (return rate of 96%).
Fifty-three percent of the experts (n ⫽ 40) were primary care professionals. Experts
endorsed routine surveillance for youth at high risk for depression, as well as the use of standardized measures as diagnostic aids. For treatment, “active monitoring” was deemed appropriate in mild depression with recent onset. Medication and psycho-therapy were considered acceptable options for treatment of moderate depression without complicating factors such as comorbid illness. Fluoxetine was rated as the most appropriate antidepressant for use in this population. Finally, experts agreed that patients who are started on antidepressants should be followed within 2 weeks after initiation.
CONCLUSIONS.Survey results support the identification and management of adolescent depression in the primary care setting and, in specific situations, referral and co-management with specialty mental health professionals. Even with the recent controversies around treatment, experts across primary care and specialty mental health alike agreed that active monitoring, pharmacotherapy with selective serotonin reuptake inhibitors, and psychotherapy can be appro-priate under certain clinical circumstances when initiated within primary care settings.
A
DOLESCENT DEPRESSION IS a typically recurring disorder with serious morbidity and mortality.1,2 It occurscommonly, affecting between 3% and 7% of adolescents.2,3Although the majority of primary care professionals
(PCPs) believe that it is their responsibility to diagnose depression in their adolescent patients, many of these teens
go unrecognized and untreated.4,5 In fact, research shows that only 50% of adolescents with depression receive a
diagnosis before reaching adulthood.4
In the past few decades, much new information has come forth from the research literature regarding the management of depression in adolescents; however, few studies have examined several aspects of depression identification and management, including strategies for assessment and initial management after diagnosis, such as
www.pediatrics.org/cgi/doi/10.1542/ peds.2006-3560
doi:10.1542/peds.2006-3560 Key Words
adolescents, depression, expert survey, primary care
Abbreviations
PCP—primary care professional PC—primary care
GLAD-PC—Guidelines for Adolescent Depression–Primary Care
DSM-IV—Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition
FDA—Food and Drug Administration Accepted for publication May 29, 2007 Address correspondence to Amy H. Cheung, MD, Department of Psychiatry, University of Toronto, 33 Russell St, Third Floor Tower, Toronto, Ontario, M5S 2S1, Canada. E-mail: [email protected]
the use of mnemonics, standardized assessment tools, and frequency of initial follow-up. Furthermore, the translation of what has been learned through research efforts into clinical practice has been limited by the shortage of mental health professionals throughout the United States and Canada. This shortage increased the need for information and strategies on the management of depression in primary care (PC) settings, although few PCPs have adequate training in the identification and management of depression in adolescents.
PCPs’ ability to manage adolescent depression is also limited by the lack of research conducted specifically in PC settings. Many issues pertaining to optimal manage-ment of adolescent depression in PC have not been addressed by research to date; neither are some critical questions likely to be answered by future research, in part because of feasibility challenges and lack of funding,
to name just a few obstacles.6–8Such issues include
rec-ommended strategies for early identification and fre-quency of follow-up.
To fill in these knowledge gaps, a steering committee of US and Canadian experts in depression and in PC developed a survey for administration to a larger group of PC and specialty mental health professionals to gather and develop consensus expert opinions regarding critical issues in the management of adolescent depression in the PC setting. This steering committee developed the survey on behalf of a larger guidelines development effort, known as the Guidelines for Adolescent
Depres-sion–Primary Care (GLAD-PC).9,10
METHODS
Survey Development
The expert survey was developed on the basis of infor-mation from 2 sources: (1) focus groups with patients, families, and professionals and (2) the research litera-ture. We conducted 16 focus groups (both for this
project and for other associated projects) in Canada (n⫽
6) and the United States (n⫽10) with PCPs (n⫽90) and
youth patients (n⫽ 12) and their families (n⫽38) to
review issues that are pertinent to the management of depression in PC. The focus groups were conducted in PC clinics, including pediatric clinics and family medi-cine clinics, in Canada (Montreal, and Toronto) and the United States (New Jersey, Utah, and Florida). Findings from the focus groups were used to identify clinicians’ views about critical issues and clinical concerns arising from the management of adolescent depression in PC and to guide the development of the survey. In-depth results from the focus groups will be available in a sep-arate publication. Briefly, focus group results indicated that clinicians’ questions, concerns, and need for guid-ance about adolescent depression management in PC fell into 5 areas: early identification, assessment/diagnosis, initial management, treatment, and ongoing manage-ment.
We then searched the literature to find what evidence was available to address these 5 problem areas where research data might provide clinical guidance. The areas reviewed included (1) major depressive disorder
identi-fication/assessment in PC settings; (2) efficacy of psycho-pharmacologic and psychotherapeutic treatments (with almost all data available only via clinical trials conducted in specialty mental health settings, rather than PC set-tings); (3) efficacy of brief counseling and psychosocial supportive interventions when offered in PC; and (4) efficacy and impact of ongoing clinical management and follow-up to include mental health referral, establishing other community linkages when needed, and organiza-tion of care.
In areas where the literature was silent but clinical guidance was nonetheless needed, we developed ques-tions to ascertain expert opinion to fill in these evidence gaps. Where common sense dictated, no questions were developed. One such example is the merit of providing education about depression to patients and families.
The initial draft of the survey was reviewed by mem-bers of the GLAD-PC steering group, including experts in PC and mental health (see Acknowledgments), and modifications were made on the basis of their feedback. The final draft was edited and finalized by 2 expert PCPs (Drs Stein and Laraque) to ensure relevance and appli-cability for PCPs and that items encompassed the full range of sensible options for the PC setting. Additional review was done with a small group of PCPs to ensure clarity and to estimate the time required for completion. The final questionnaire was organized into several sec-tions, early identification, assessment and diagnosis, ini-tial management, treatment, and ongoing management, and consisted of 34 general question categories and 220 response options.
The survey, using a 9-point scale (1⫽most
inappro-priate treatment and 9 ⫽extremely appropriate
treat-ment), is a modified survey format developed by the
Rand Corporation for examining expert consensus.11The
large number of response options allowed us to gather expert opinion regarding depression management under a variety of clinical circumstances. For example, experts were asked to rate the appropriateness of specific strat-egies for identifying depression during different types of visits, such as well-child and urgent care. We were also able to seek expert opinion on the appropriateness of specific management strategies for different clinical pre-sentations, varying by the presence or absence of a spe-cific symptom, such as psychosis, in patients with de-pression. In addition, the 9-point scale provided detailed responses regarding the appropriateness of individual strategies and treatment choices in specific clinical sce-narios. Finally, a small proportion of items in the survey asked for experts to estimate timelines (eg, how many weeks would you wait before starting treatment?). A copy of the survey is available on request.
Participant Selection
citations; or (4) key PC clinical and research leaders with expertise in the area of guideline development and/or emotional and behavioral disorders that present in PC settings. As is typical of activities in which expert opin-ion is sought, selectopin-ion of experts was nonrandom and likely does not represent the diversity of community-based PCPs for children. We deliberately sought experts in PC because their practices, although not representa-tive, might serve as a standard for more “representative” PCPs. In addition, we attempted to include a broad range of experts from several disciplines, including family medicine, pediatrics, nursing, psychology, and child psy-chiatry. This method of nonprobability sampling is
fre-quently used in social science research.12The survey and
procedures were approved by the institutional review board of New York State Psychiatric Institute.
Survey Analyses
The mean, SDs, and 95% confidence intervals were calculated for each item. For making responses more clinically applicable, a categorical tag such as “treatment of choice,” “first-line,” “second-line,” and “third-line” treatment were designated on the basis of the lowest category in which the confidence interval fell, with boundaries ofⱖ8 as treatment of choice,ⱖ7 as first-line,
and ⱖ4 as second-line. Items with responses ⬍4 were
considered generally inappropriate in the PC setting.
RESULTS
Seventy-eight of 81 invited experts agreed to participate (return rate of 96%). On average, the experts had been in practice for 20 years (SD: 8.6 years). Fifty-three
per-cent of the experts (n⫽40) were PCPs; the remainder
were specialty mental health experts in child and ado-lescent psychiatry and in psychology. Only 76 of the 78
completed surveys were available for data analysis, with one completed survey lost in the mail and another com-pleted survey misplaced prior to data entry.
Identification
Overall, findings indicate that experts thought that the strategies used for early identification of emotional prob-lems should vary on the basis of the circumstances of the presentation by an adolescent (Fig 1). In well-child vis-its, the intervention that was rated as most appropriate was “asking general questions” (average: 8.41; SD: 1.25), described as “surveillance” by the American Academy of Pediatrics. Of the several options that were rated highly, answers were not exclusive; that is, one could indicate that multiple particular approaches were acceptable, but one cannot determine from these responses in isolation which of the acceptable responses was optimal. In the case of an urgent care visit for some medical chief com-plaint where the physician has another, potentially ur-gent, problem to attend to, only asking general questions was rated as a first-line practice.
In contrast, when experts were asked about how to gather information regarding depression during an out-patient visit for adolescents who present with an emo-tional problem as the chief complaint, all choices were rated as strategies of choice or first-line with the excep-tion of depending solely on youth and/or parental com-plaints. These endorsed strategies included the use of youth- or parent-reported psychosocial or depression checklists, use of the screener interview HEADSS-home, and education/employment, activities, drugs, sexuality, suicide/depression, use of the screener Guidelines for Adolescent Preventive Services questionnaire, and ask-ing the youth both general and depression specific ques-tions (Fig 1). In such instances, both face-to-face inter-L o g i ca l M e m or y I I mm e i d a te
Extremely inappropriate
Extremely appropriate
3.49 4.36 3.74
7.74 4.06
5.29
8.51 4.70
7.25
8.28 7.32
8.41
8 6.04
8
8.86 5.7
7.36
8.24 4.25
6.16
1 2 3 4 5 6 7 8 9
Emotional problems Urgent care Well-child visit
Youth completed depression checklist
Youth interview asking depression-specific questions
Use of a screener like HEADSS
Youth interview asking general questions
Youth-completed psychosocial checklist
Parent-completed depression checklist
Reliance solely upon youth and/or parent complaints/concerns
(1.97)
(2.00) (1.95) (1.91) (2.31)
(1.79)
(2.22)
(2.30) (2.34)
(1.74) (1.69)
(2.38)
(2.52) (2.17)
(1.16)
(1.53) (2.61)
(1.33) (0.86)
(0.39) (1.25)
FIGURE 1
view questions and structured checklists were thought to be of use.
Assessment/Diagnosis
Given the scenario that the PCP already suspects depres-sion during the assessment, experts agreed that inter-views should be conducted with the adolescent alone (average: 8.9; SD: 0.4), with the parent/caregiver alone (average: 7.74; SD: 2.05), and jointly with both (average: 8.04; SD: 1.28). Experts also agreed that the use of a youth-report depression questionnaire, such as the Beck Depression Inventory, was appropriate (average: 7.88; SD: 1.53).13
As part of an evaluation to confirm the diagnosis of depression, experts agreed that each of the following was a critical component of the assessment: obtaining history of presenting illness (average: 8.96; SD: 0.2), previous history and treatment for depression and/or emotional problems (average: 8.96; SD: 0.2), medical history (average: 8.66; SD: 0.81), substance use history (average: 8.93; SD: 0.34), psychosocial history (ie, cur-rent stressors) (average: 8.92; SD: 0.32), curcur-rent func-tioning at school or with friends (average: 8.95; SD: 0.22), and family history (average: 8.78; SD: 0.51). To confirm the diagnosis of depression, the experts agreed
that the Diagnostic and Statistical Manual of Mental
Disor-ders, Fourth Edition (DSM-IV) diagnostic criteria should
be used (average: 8.34; SD: 0.96). Investigations and examinations that were rated as essential to rule out other causes of depressive symptoms included specific (ie. focused) physical examination as indicated by his-tory (average: 8.19; SD: 1.36), a complete physical ex-amination (average: 8.09; SD: 1.70), and tests for thyroid function (average: 7.35; SD: 2.04).
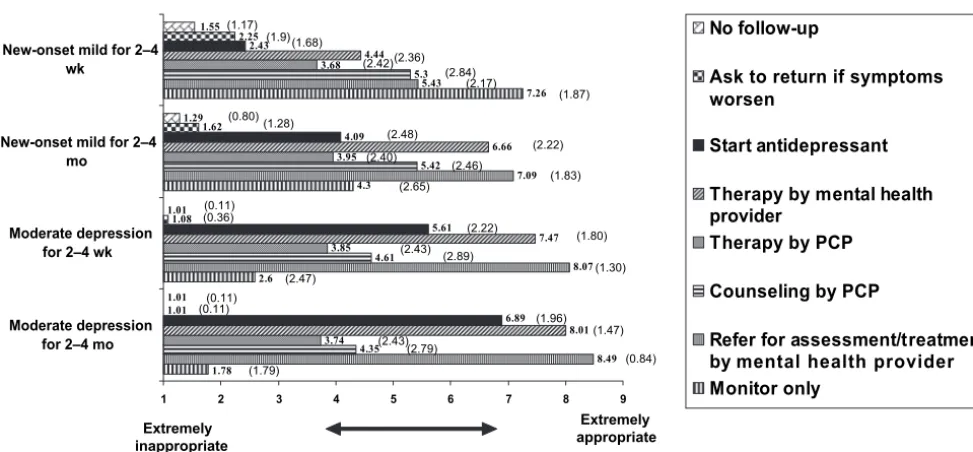
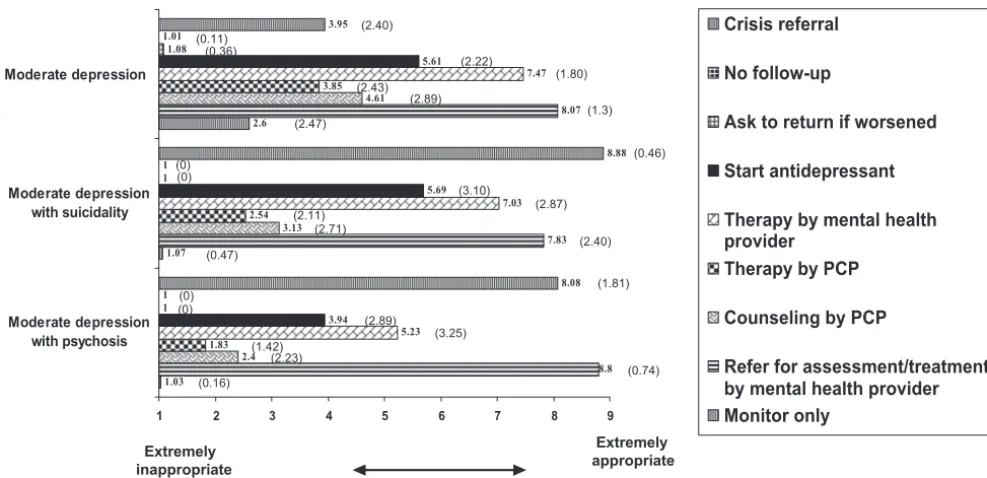
Treatment
Experts’ responses regarding recommended treatment options for mild and moderate/severe depression are
shown in Figs 2 and 3. As seen in these figures, experts’ recommendations differed on the basis of se-verity of depressive symptoms, duration of illness, and the occurrence of comorbidity and/or suicidality or psychosis.
For all cases of confirmed depression, experts agreed that it would not be appropriate to have no follow-up or to ask the patient to return only if their symptoms worsen (Figs 2 and 3). Active monitoring was deemed acceptable but only appropriate in “mild” depression (for
discussion, see “Limitations”) lasting⬍4 weeks. In
con-trast, experts generally agreed that if a patient has mod-erate depression regardless of duration, then he or she should be referred to mental health for assessment and/or treatment and the initiation of antidepressants should be considered. When questioned about whether the PCP should consider starting an antidepressant for moderate depression lasting 2 to 4 months, the overall rating was 6.89, just shy of the average of 7 (first line). For patients who present with either psychosis or sui-cidality, referral to crisis settings or to mental health for assessment and treatment was rated highly, essentially as the treatment of choice. As seen in these figures, the use of antidepressant treatment is viewed as more ap-propriate the longer a patient has been experiencing symptoms of depression with suicidality. Finally, in pa-tients with comorbid illnesses (eg, substance abuse, con-duct disorder, attention deficit hyperactivity disorder, anxiety disorders), experts were less likely to recom-mend the initiation of an antidepressant by the PCP. In these patients, referral to mental health for assessment and treatment were considered more appropriate.
Treatment of choice among the antidepressants were selective serotonin reuptake inhibitors (average: 8.46; SD: 1.1), specifically fluoxetine (average: 8.54; SD: 0.76). Sertraline (average: 7.83; SD: 1.68), citalopram (average: 7.55; SD: 1.72), and escitalopram (average:
Extremely inappropriate Extremely appropriate 1.78 2.6 4.3 7.26 8.49 8.07 7.09 5.43 4.35 4.61 5.42 5.3 3.74 3.85 3.95 3.68 8.01 7.47 6.66 4.44 6.89 5.61 4.09 2.43 1.01 1.08 1.62 2.25 1.01 1.01 1.29 1.55
1 2 3 4 5 6 7 8 9
Moderate depression for 2–4 mo Moderate depression
for 2–4 wk New-onset mild for 2–4
mo
New-onset mild for 2–4 wk
No follow-up
Ask to return if symptoms worsen
Start antidepressant
Therapy by mental health provider
Therapy by PCP
Counseling by PCP
Refer for assessment/treatment by mental health provider Monitor only (1.17) (1.68) (1.9) (2.36) (2.42) (2.84) (2.17) (1.87) (0.80) (2.46) (2.40) (1.28) (2.22) (2.48) (1.83) (2.89) (2.65) (0.36)(0.11) (2.22) (1.80) (2.43) (1.30) (2.47) (0.11) (0.11) (1.47) (1.96) (2.43) (1.79) (0.84) (2.79) FIGURE 2
7.26; SD: 2.23) were rated as first-line treatments. Both tricyclic antidepressants (average: 2.88; SD: 2.24) and monoamine oxidase inhibitors (average: 1.86; SD: 1.35) were considered inappropriate in this age group. When the PCP is prescribing antidepressant treatment, experts generally concluded that patients should be followed up within 2 weeks after the initiation of antidepressant treatment (mean: 1.98 weeks: SD: 1.04) and within 7 weeks for those who have stabilized on medication (mean: 7.2 weeks; SD: 4.53). Finally, in terms of man-agement of adverse events, the experts consider all of the following procedures as highly appropriate: assessing for adverse effects after every new medication is started (average: 8.89; SD: 0.39), asking about common adverse effects on every visit (average: 8.61; SD: 0.95), talking to family/caregivers (average: 7.85; SD: 1.53), and exam-ining the patient (average: 7.08; SD: 1.92).
Ongoing Management
For those with partial improvement with antidepressant treatment, the experts thought that the maximum ther-apeutic dosage should be used (average: 8.14; SD: 1.17) but not exceeded (average: 2.91; SD: 2.17). If partial improvement is achieved with maximum dosages of an antidepressant, then referral to mental health for addi-tional assessment and treatment recommendations (av-erage: 8.18; SD: 1.2) and/or for implementation of treat-ment (average: 7.88; SD: 1.37) were deemed as the most appropriate. Similarly, for those who do not improve on antidepressant treatment, again, the maximum thera-peutic dosage should be used (average: 7.72; SD: 1.94); however, it should not be exceeded (average: 2.73; SD: 2.06). If there is no response with the maximum dosage of antidepressant treatment, then experts endorsed re-ferral to mental health for additional assessment and
treatment recommendations (average: 8.22; SD: 1.22), referral to mental health for actual treatment delivery (average: 7.88; SD: 1.37), or switching to another anti-depressant (average: 7.43; SD: 2.22). Finally, in cases in which a mental health referral has been made, experts recommended that PCPs continue to provide support to the patient and see the patient again within 4 weeks (mean: 3.51 weeks; SD: 2.34) even though the patient has been referred.
DISCUSSION
General Observations
The results of this survey suggest remarkable consistency among experts in the field on the need for particular assessment, treatment, and management strategies. The findings from the expert survey support the use of strat-egies for early identification of patients who are at high risk for developing depression. Several strategies were rated as extremely appropriate during well-child visits and appointments at which the chief complaint is an emotional problem. The somewhat lower rating for “de-pression-specific checklists” in these clinical encounters may be because such a checklist might miss a youth with some other type of behavioral or emotional problem. In urgent care visits, only asking general questions was rated as extremely appropriate (strategy of choice). In contrast to the expert opinion, there is emerging evi-dence from the literature supporting the use of standard-ized tools to identify adolescents with emotional prob-lems such as depression even during urgent care
visits.14,15This highlights a common problem with
rely-ing solely on expert opinion: expert opinion may not have incorporated the most up-to-date research evi-dence, or experts may be limited in their willingness to
Extremely inappropriate
Extremely appropriate
1.03 1.07
2.6
8.8 7.83
8.07
2.4 3.13
4.61
1.83 2.54
3.85
5.23
7.03 7.47
3.94
5.69 5.61
1 1
1.08
1 1 1.01
8.08 8.88 3.95
1 2 3 4 5 6 7 8 9
Moderate depression with psychosis Moderate depression
with suicidality Moderate depression
Crisis referral
No follow-up
Ask to return if worsened
Start antidepressant
Therapy by mental health provider
Therapy by PCP
Counseling by PCP
Refer for assessment/treatment by mental health provider Monitor only
(0.11) (2.40)
(2.22) (0.36)
(1.80) (2.89)
(2.43)
(2.71)
(1.3) (2.47)
(0.46) (0)
(3.10)
(2.87) (2.11)
(1.42)
(1.81)
(0.47) (2.40)
(2.89) (0)
(0)
(0.74) (3.25)
(0)
(2.23) (0.16)
FIGURE 3
do so because of the constraints of practice settings, which are not usually present when auxiliary research staff conduct studies. However, these contradictory re-sults may also represent the strength of the research evidence (ie, the sum of the current research evidence may not be strong enough to change current expert opinion). A recent example of this is the use of antide-pressants in children and adolescents. Although the Food and Drug Administration (FDA) reanalyses of safety data showed an increased risk for adverse effects in patients who were treated with antidepressants com-pared with those who were given placebo, expert panels from both the American Academy of Child and Adoles-cent Psychiatry and the American Psychiatric Associa-tion remain supportive of the use of antidepressants in children and adolescents, citing that benefits from the
medications outweigh the risks.16
With regard to diagnosis, the results of the expert survey support the use of the DSM-IV criteria by PCPs to diagnose depression in adolescents. The experts also agreed that interviews should include meeting with the adolescent alone and with the parents/caregivers. Al-though this was rated as extremely appropriate, it is not always possible to include family members in the assess-ment of an adolescent. Factors that may limit the in-volvement of the family include geographic distance in cases of separated families or the adolescent’s reluctance to have his or her family contacted.
The experts agreed that active monitoring, pharma-cotherapy with selective serotonin reuptake inhibitors, and psychotherapy can be appropriate under certain clinical circumstances. The choice of treatment strategy varied on the basis of the severity and the duration of depressive symptoms and the occurrence of comorbidity. Thus, findings generally supported the premise that it may be acceptable (and essential) for the PCP to provide treatment for adolescent depression, in instances of moderate to severe depression lasting months, and in the face of difficulties obtaining access to child and ad-olescent psychiatry. In terms of the question pertaining to whether the PCP should consider starting an antide-pressant for moderate depression lasting 2 to 4 months, although the overall rating (6.89) fell short of the aver-age of 7 (first line), there were interesting differences among respondents, with 65% of child and adolescent psychiatrists rating this as a first-line strategy but only 43% of PCPs rating this as an acceptable first-line strat-egy. These findings might suggest the concerns that PCPs have about taking on this responsibility without addi-tional support and training.
The survey also provided guidance regarding ongoing treatment of adolescents with antidepressants. Strategies for addressing partial or no improvement on antidepres-sants were recommended including using the maximum therapeutic dosage and referral to mental health if there is only partial improvement with the maximum dosage. Although the experts agreed that PCPs are able to treat adolescents with depression in their practices, they also agreed that in many clinical scenarios, referral to mental health was the strategy of choice, such as with a suicidal or psychotic adolescent; however, many factors
influ-ence a successful mental health referral, including pa-tient and parent/caregiver acceptance and availability of mental health professionals. Because it is not always feasible for adolescents to be referred to mental health, guidance for the management of more complicated cases in the PC setting may also be needed.
One aspect of treatment, the appropriate frequency of follow-up when initiating antidepressant treatment, was addressed by the FDA. The monitoring guide provided by the FDA gives clear direction regarding the frequency of face-to-face follow-up for the first weeks of antide-pressant treatment. The FDA expert panel recom-mended that follow-up occur within 1 week of initiation of antidepressant treatment. Similarly, our expert survey
recommended ⬍2 weeks as the maximum time before
the first follow-up. The lack of research studies that have addressed this issue makes expert guidance particularly important regarding this aspect of treatment.
Finally, in this survey, the definitions of mild, mod-erate, and severe depression were left up to the clinical judgment of the survey completers; however, for the results of this report to be clinically useful, theses defi-nitions must be clarified. According to the DSM-IV, se-verity of depressive disorders can be based on symptom
count.17This commonly used method to define
depres-sion severity has been used in large population-based
studies18and may be particularly relevant in PC settings,
where less severe clinical presentations of depression may be more common. Thus, mild depression may be characterized on the basis of lower scores in standardized depression scales, shorter duration of symptoms, or meeting minimal criteria for depression. Following the DSM-IV, mild depression might be defined as 5 to 6 symptoms that are mild in severity. Furthermore, the patient might experience only mild impairment in func-tioning. In contrast, depression might be deemed to be severe when a patient experiences all of the depressive symptoms listed in the DSM-IV. Depression might also be considered severe if the patient experiences severe impairment in functioning. Moderate depression falls between these 2 categories. In general, however, even if not all 9 DSM-IV– defined symptoms of depression are present, an adolescent with at least 5 criteria of depres-sion should be considered to be in the severe category if presenting with a specific suicide plan, clear intent, or recent attempt; psychotic symptoms; or severe impair-ment in functioning (eg, unable to leave home).
Limitations
clear from the survey results whether these strategies or treatments should be used in combination or would also be appropriate if used alone. To provide appropriate clinical guidance, the survey results cannot serve as free-standing recommendations but need to be developed into coherent guidelines for PCPs. Nonetheless, our find-ings do provide support for the benefits of expert con-sensus approaches in addressing questions that would otherwise remain unaddressed in other types of empir-ical studies.
CONCLUSION
The high degree of consistency on several recommenda-tions suggests that PCPs can be given clear guidance on the management of depression, especially in settings where mental health services are accessible. Other find-ings that could provide additional guidance, such as a comparison of responses from those who are and are not PC providers and from providers who work in different health care systems (eg, Canadian versus American ex-perts), are beyond the scope of this article and will be presented in subsequent publications.
ACKNOWLEDGMENTS
We acknowledge the financial support of the Center for the Advancement of Children’s Mental Health and Sun-nybrook Health Sciences Centre.
The GLAD-PC Steering Committee consists of the following (listed alphabetically): Boris Birmaher, MD, Western Psychiatric Institute and Clinic, University of Pittsburgh; John Campo, MD, Ohio State University; Greg Clarke, PhD, Center for Health Research, Kaiser Permanente; Dave Davis, MD, University of Toronto; Angela Diaz, MD, Mount Sinai School of Medicine; Allen Dietrich, MD, Dartmouth Hitchcock Medical Cen-ter; Graham Emslie, MD, University of Texas Southwest-ern Medical School; BSouthwest-ernard Ewigman, MD, Depart-ment of Family Medicine, University of Chicago; Eric Fombonne, MD, McGill University; Sherry Glied, PhD, Columbia University; Kimberly Eaton Hoagwood, PhD, Office of Mental Health, New York State, and Columbia University; Charles Homer, MD, National Initiative for Children’s Healthcare Quality; Miriam Kaufman, MD, Hospital for Sick Children, University of Toronto; Kelly J. Kelleher, MD, Ohio State University; Stanley Kutcher, MD, Dalhousie Medical School; Danielle Laraque, MD, American Academy of Pediatrics New York Chapter 3, District II, and Mount Sinai School of Medicine; Michael Malus, MD, Department of Family Medicine, McGill University; James Perrin, MD, Massachusetts Medical School, Harvard Medical School; Harold Pincus, MD, Columbia University; Brenda Reiss-Brennan, APRN, In-termountain Health, UT; Diane Sacks, MD, Canadian Pediatric Society; Ruth E. K. Stein, MD, Forum for Child Health, New York Academy of Medicine, Albert Einstein College of Medicine; Bruce Waslick, MD, Baystate Health Systems, MA.
REFERENCES
1. AACAP. Practice parameters for the assessment and treatment of children and adolescents with depressive disorders. J Am Acad Child Adolesc Psychiatry.1998;37(suppl):63S– 83S 2. Fleming JE, Offord DR, Boyle MH. Prevalence of childhood and
adolescent depression in the community: Ontario Child Health Study.Br J Psychiatry.1989;155:647– 654
3. Cheung A, Dewa C. Canadian Community Health Survey: depression and suicidality among adolescents aged 15–18.
Healthcare Policy.2006;2(2):76 – 89
4. Kessler RC, Avenevoli S, Ries Merikangas K. Mood disorders in children and adolescents: an epidemiologic perspective. Biol Psychiatry.2001;15:1002–1014
5. Olson AL, Kelleher KJ, Kemper KJ, Zuckerman BS, Hammond CS, Dietrich AJ. Primary care pediatricians’ roles and perceived responsibilities in the identification and management of de-pression in children and adolescents. Ambul Pediatr. 2001;1: 91–98
6. Clarke G, Debar L, Lynch F, et al. A randomized effectiveness trial of brief cognitive-behavioral therapy for depressed adoles-cents receiving antidepressant medication. J Am Acad Child Adolesc Psychiatry.2005;44:888 – 898
7. Asarnow JR, Jaycox LH, Duan N, et al. Effectiveness of a quality improvement intervention for adolescent depression in primary care clinics: a randomized controlled trial. JAMA.
2005;293:311–319
8. Horwitz SM, Kelleher K, Boyce T, et al. Barriers to health care research for children and youth with psychosocial problems.
JAMA.2002;288:1508 –1512
9. Zuckerbrot RA, Cheung AH, Jensen PS, Stein REK, Laraque D; GLAD PC Steering Group. Guidelines for Adolescent Depres-sion in Primary Care (GLAD-PC): part I—identification, assess-ment, and initial management.Pediatrics.2007;120(5). Avail-able at: www.pediatrics.org/cgi/content/full/120/5/e1299 10. Cheung A, Zuckerbrot RA, Jensen PS, et al. Guidelines for
Adolescent Depression in Primary Care (GLAD-PC): part II— treatment and ongoing management.Pediatrics.2007;120(5). Available at: www.pediatrics.org/cgi/content/full/120/5/e1313 11. Kahn DA, Frances A, Docherty JP. Expert consensus guidelines series: treatment of bipolar disorder. J Clin Psychiatry. 1996; 57(suppl 12A):3– 89
12. Mutchnick RJ, Berg BL.Research Methods for the Social Sciences. Needham Heights, MA: Allyn and Bacon; 1996
13. Beck AT, Steer RA.Manual for the Beck Depression Inventory. San Antonio, TX: Psychological Corporation; 1987
14. Borowsky IW, Mozayeny S, Ireland M. Brief psychosocial screening at health supervision and acute care visits.Pediatrics.
2003;112(pt 1):129 –133
15. Zuckerbrot RA, Maxon L, Pagar D, Davies M, Fisher PW, Shaffer D. Adolescent depression screening in primary care: feasibility and acceptability.Pediatrics.2007;119:101–108 16. American Academy of Child and Adolescent Psychiatry.
Psy-chiatric medication: March 2004 FDA Advisory. Available at: www. aacap.org/page.ww?section⫽Psychiatric⫹Medication&name⫽ March⫹2004⫹FDA⫹Advisory. Accessed December 4, 2007 17. American Psychiatric Association.Diagnostic and Statistical Manual
of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994
DOI: 10.1542/peds.2006-3560
2008;121;e101
Pediatrics
Laraque
Amy H. Cheung, Rachel A. Zuckerbrot, Peter S. Jensen, Ruth E.K. Stein and Danielle
Expert Survey for the Management of Adolescent Depression in Primary Care
Services
Updated Information &
http://pediatrics.aappublications.org/content/121/1/e101
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/121/1/e101#BIBL
This article cites 12 articles, 2 of which you can access for free at:
Subspecialty Collections
y_sub
http://www.aappublications.org/cgi/collection/psychiatry_psycholog Psychiatry/Psychology
ub
http://www.aappublications.org/cgi/collection/psychosocial_issues_s Psychosocial Issues
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2006-3560
2008;121;e101
Pediatrics
Laraque
Amy H. Cheung, Rachel A. Zuckerbrot, Peter S. Jensen, Ruth E.K. Stein and Danielle
Expert Survey for the Management of Adolescent Depression in Primary Care
http://pediatrics.aappublications.org/content/121/1/e101
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.