EXPERIENCE & REASON
Pulmonary Function Assessment in an Infant With
Barnes Syndrome: Proactive Evaluation for Surgical
Intervention
Thomas L. Miller, PhDa, Timothy Cox, RRTb, Thomas Blackson, RRTc, David Paul, MDc, Kerry Weiss, MD, MPHd, Thomas H. Shaffer, PhDa,e
aNemours Research Lung Center andbNemours Children’s Clinic, Alfred I. duPont Hospital for Children, Wilmington, Delaware;cChristiana Care Health System, Newark,
Delaware;dSt Peter’s University Hospital, New Brunswick, New Jersey;eDepartments of Physiology and Pediatrics, Temple University School of Medicine, Philadelphia,
Pennsylvania
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
Our aim for this study was to report pulmonary mechanics in a neonate with a severe case of Barnes syndrome, a rare form of thoracolaryngopelvic dysplasia, and to use these data to guide ventilatory support and serve as a presurgical screening tool. A comprehensive pulmonary function evaluation was performed on a 36-day-old patient with Barnes syndrome who was being mechanically ventilated because of severe pulmonary distress secondary to thoracic dystrophy. The measurements consisted of respiratory volumes including functional residual capacity, ventilatory mechanics including compliance and resistance, and thoracoabdominal synchrony. Chest wall compli-ance was 64% below normal, and the thoracoabdominal motion was indicative of predominantly abdominal displacement during inspiratory breaths. The lungs were functioning at a low functional residual capacity, resulting in low lung compliance and increased pulmonary resistance. As a result of the evaluation, the patient was recommended for lateral thoracic expansion surgery and the ventilatory management was adjusted to focus on end-distending pressure support.
B
ARNES SYNDROME IS a rare, autosomal dominant form of thoracolaryngopelvic dysplasia, whereby chondrodystrophy of the thoracic cage can result in death by asphyxiation. First described in case reports by Barnes et al1in 1969, Barnes syndrome is distinct fromthe better-known form of asphyxiating thoracic dystro-phy (Jeune syndrome) in that rib shortening is less severe and the thoracic dystrophy is complemented by laryngeal stenosis and reduced pelvic dimensions.2Key
features of the infants described with Barnes syndrome are a small, rigid, bell-shaped thorax with horizontal ribs; however, their lungs are typically not hypoplastic. In addition, these infants have abnormal laryngeal car-tilage configurations and expanded costochondral junc-tions.3 Beyond the reduced thoracic and pelvic cavity
sizes, the heads, limbs, hands, and feet of these infants were of normal proportions.1
Although Barnes syndrome can result in severe respi-ratory distress and death, it has been identified in a less-severe, non–life-threatening form in family mem-bers of infants who did not survive.1,4 In that lungs of
infants with reduced thoracic size are not hypoplastic, surgical intervention to expand the thoracic volume has
been shown to be successful.3In this report, we present
a case study of the pulmonary mechanics for a neonate with severe respiratory limitations subsequent to clini-cally prominent Barnes syndrome. The results of the pulmonary evaluation were used to assist in establishing acceptable ventilator settings and serve as a presurgical screening tool before consideration of lateral thoracic expansion.
MATERIALS AND METHODS
Case History
This protocol was approved by the institutional review board of Nemours Biomedical Research, and the study
Key Words:thoracolaryngopelvic dysplasia, chondrodystrophy, asphyxiating thoracic dystrophy, thoracic expansion, thoracoabdominal motion, functional residual capacity
Abbreviation:FRC, functional residual capacity
www.pediatrics.org/cgi/doi/10.1542/peds.2006-0135
doi:10.1542/peds.2006-0135
Accepted for publication May 23, 2006
Address correspondence to Thomas L. Miller, PhD, Nemours Biomedical Research, AR-282, Alfred I. duPont Hospital for Children, 1600 Rockland Rd, Wilmington, DE 19803. E-mail: thmiller@nemours. org
was performed at the Alfred I. duPont Hospital for Chil-dren. The infant was a term, 36-day-old girl weighing 3.2 kg. She was born with obvious thoracic dystrophy and, at the time of the evaluation, was breathing through a 3.5-mm internal diameter tracheostomy tube (Mallinckrodt, St Louis, MO) with mechanical ventila-tory assistance (Bird VIP, Viasys, Palm Springs, CA). The ventilator was set for intermittent mechanical breaths (40 breaths per minute) with pressure-limited setting as follows: peak inspiratory pressure⫽26 cm H2O, positive end-expiratory pressure⫽7 cm H2O, inspiratory time⫽ 0.4 seconds, and fraction of inspired oxygen⫽0.4. There were no other reported cases of Barnes syndrome in the family history.
Measurement of Ventilatory Mechanics
Ventilatory mechanics were assessed by simultaneous measurement of transpulmonary pressure and respira-tory airflow with esophageal and airway manometry and pneumotachography, as previously described.5,6The
patient was instrumented with a 6F esophageal pres-sure-monitoring catheter,7,8 and transpulmonary
pres-sure was derived from proximal airway prespres-sures and esophageal pressure by a differential pressure transducer (Validyne DP15-28; Validyne, North Ridge, CA). Opti-mum placement of the esophageal water-filled catheter was confirmed by real-time monitoring of pressure trac-ings using criteria of maximum negative deflection dur-ing inspiration with minimum cardiac artifact. Airflow was measured with a low dead-space volume pneumo-tachometer (No. 00, Fleish, Eplinges, Switzerland) and differential pressure transducer (Validyne MP45). Respi-ratory volumes were determined by integration of time and flow signals, and respiratory compliance and resis-tance were calculated by least-mean-square algorithms incorporated into a well-calibrated computerized pulmo-nary-function system (PeDs; MAS, Inc, Hatfield, PA).6
Lung compliance (CL) was differentiated from total re-spiratory compliance (Ctotal) by using esophageal pres-sures or ambient pressure, respectively, to derive trans-mural pressures with respect to proximal airway pressure. Compliance of the chest wall (CCW) is repre-sented as the inverse of the difference betweenCtotal⫺1 and
CL⫺1. As an objective measure for pulmonary
overinfla-tion, the compliance value from the last 20% of the inspired volume relative to theCtotal(C20/Ctotal) was cal-culated.9 Respiratory resistance is represented as total
resistance (Rtotal) and subdivided into resistance for the inspiratory (Rinsp) and expiratory (Rexp) phases. Re-ported mechanics measurements were based on the av-erage of at least 10 breaths.
Measurement of Functional Residual Capacity
Functional residual capacity (FRC) was measured using a helium dilution system (Panda; MAS, Inc) based on a previously described protocol.5,10–12 Briefly, a valve
de-vice was placed inline between the endotracheal tube and the ventilator. At end expiration, the valve device was activated to connect and ventilate the patient inline with a closed-circuit gas reservoir of known volume and helium concentration. On the basis of the new equilib-rium helium concentration reached from 30 to 45 sec-onds and encompassing numerous breaths, FRC was calculated. Helium loss through inherent gas leaks was accounted for by distinguishing between the equilibra-tion and leak phases of the helium concentraequilibra-tion curve and adjusting the FRC calculation accordingly.11,12FRC
determinations were performed in triplicate and aver-aged.
Measurement of Thoracoabdominal Motion
The relationship between thoracic and abdominal con-tributions to the respiratory effort was assessed by using respiratory inductive plethysmography (Respitrace; Nims, Inc, North Bay Village, FL).13,14Bands containing
inductive coils were placed around the ribcage at the level of the axillae and around the abdomen midway between the xiphisternal junction and the umbilicus. The Respitrace device was used in the uncalibrated mode in which voltage changes in response to changes in band inductance were used to construct Lissajous loops and for calculation of phase angle between the ribcage and abdominal movement associated with respiration.5,15,16
Reported phase-angle measurements were based on the average of at least 10 breaths.
RESULTS
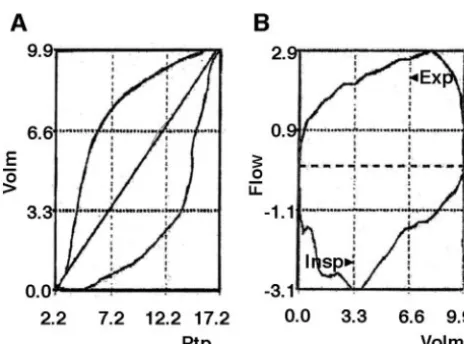
The infant tolerated the pulmonary function evaluation with no remarkable changes in vital signs, oxygen satu-ration, or blood chemistries around the time of the test procedures. Oxygen saturation remained⬎95%, with a fraction of inspired oxygen of 0.6. Averaged pulmonary-function measures for the patient along with predicted normal values are given in Table 1, and typical pressure-volume and flow-pressure-volume loops are presented in Fig 1.
Ctotal, CL, and CCW values were notably reduced from
predicted values17,18; however, theC
20/Ctotalwas appre-ciably greater than predicted.Rtotal,Rinsp, andRexpwere all⬎300% of the predicted values. FRC was only 37% of predicted values, and the phase angle for thoracoab-dominal motion was much greater (200%) than normal values for an infant of this age.
DISCUSSION
The major aim of this report was to use pulmonary-mechanics measurements with esophageal manometry to determine the relative contribution of the chest wall and lungs to the decrease in total thoracic compliance experienced by a newborn with Barnes syndrome. All indications from this evaluation are that the patient was ventilating at the low end of the lung pressure-volume
PEDIATRICS Volume 118, Number 4, October 2006 e1265
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
relationship curve subsequent to a noncompliant chest wall.
The prognosis of ribcage chondrodystrophy was con-firmed here by a chest wall compliance value that was only 64% of the predicted norm. As a result, this infant had a thoracoabdominal phase angle much greater than the predicted normal,19 indicating that the respiratory
work was being accomplished predominantly by dis-placement of the abdomen and not the ribcage.
Subsequent to the limitation on thoracic expansion, the lungs were functioning at a greatly reduced and inefficient FRC. The measurement of FRC as only 37% of the predicted value was confirmed in that the C20/
Ctotal is relatively high and the inflation limb of the
pressure volume curve (Fig 1A) demonstrates that one third of the tidal volume falls below the lower inflection
point. Thus, theCLwas also reduced from the expected normal level because of a low FRC and contributed to an overall lowCtotal. In addition, the highC20/Ctotalratio can be taken to indicate that the lungs are not hypoplastic, which supports the conclusion that the reduced compli-ance is secondary to thoracic volume complications.
The elevation in pulmonary resistance is likely sec-ondary to the low FRC. Collapse of the lung below the lower inflection point on the pressure-volume curve can also result in collapse of the intrapulmonary airways. This reduction in airway diameter results in a resistive load contributing to the greater-than-normal thoracoab-dominal phase angle.20,21In addition, this resistive load
can contribute to complications on expiration, as indi-cated on the expiratory limb of the flow-volume curve (Fig 1B) by an early spike and subsequent degeneration in flow.
This case demonstrates the use of proactive pulmo-nary function assessment in the early stabilization and management of a patient destined to require long-term respiratory care. Whereas there is not a widespread availability of the current instruments used to perform this thorough evaluation, we are using new commercial instruments to operate an infant pulmonary diagnostics laboratory to make this clinical service more readily available. On the basis of these data, the ventilatory management plan was directed toward reducing peak inspiratory pressure support, increasing positive end-expiratory pressure for FRC management, and empha-sizing chest wall stabilization to allow growth and mat-uration. This patient was recommended for lateral thoracic expansion surgery and serial pulmonary func-tion studies, which are warranted after surgery.
ACKNOWLEDGMENTS
We gratefully acknowledge the support of National In-stitutes of Health Centers of Biomedical Research Excel-lence grant 1 P20 RR020173-01 (the Center for Pediatric Research).
TABLE 1 Pulmonary Mechanics Measurements
Parameter Predicted Normal Test Results (Mean⫾SEM)
Percent Predicted
Tidal volume, mL/kg 6–8 2.9⫾0.2 48
Total compliance, mL/cm H2O per kg 0.8–1.3 0.22⫾0.02 23
Lung compliance, mL/cm H2O per kg 1.0–1.5 0.24⫾0.01 19
Chest wall compliance, mL/cm H2O per kg 4.2 2.7⫾0.0 64
C20/Ctotal ⬎1.0 2.5⫾0.0 250
Total resistance, cm H2O/L per sec 29–40 136.6⫾12.7 397
Inspiratory resistance, cm H2O/L per sec 29–40 105.4⫾14.5 303
Expiratory resistance, cm H2O/L per sec 29–40 129.9⫾26.8 371
FRC, mL/kg 24–30 10.1⫾0.6 37
Thoracoabdominal phase angle, ° 0–30 60⫾1 200
C20/Ctotalrepresents respiratory compliance from the last 20% of the tidal volume relative to the total respiratory compliance. The normal value for thoracoabdominal phase angle is from Allen JL, Greenspan JS, Deoras KS, Keklikian E, Wolfson MR, Shaffer TH.Pediatr Pulmonol. 1991;11:37– 43; the normal value for chest wall compliance is from Gerhardt T, Hehre D, Feller R, Reifenberg L, Bancalari E.Pediatr Pulmonol. 1987;3:309 –316; all other normal values are from Bhutani VK, Sivieri EM, Abbasi S. Evaluation of pulmonary function in the neonate. In: Polin RA, Fox WW, eds.Fetal and Neonatal Physiology. WB Saunders; 1998:1143–1164.
FIGURE 1
Graphs of the transpulmonary pressure (Ptp; cm H2O)⫺volume (volm; mL) (A) and flow
(L/minute)⫺volume (volm; mL) (B) relationships from the patient. The right limb of the transpulmonary pressure-volume curve represents inspiration and the left limb of the transpulmonary pressure-volume curve represents deflation. TheC20/Ctotterm repre-sents the ratio of the slope of the last 20% of the inflation curve divided byCtotas
We thank Barbara E. Gray, BA, CPM (Administrative Manager, Nemours Research Lung Center), for editing of this manuscript.
REFERENCES
1. Barnes ND, Hull D, Symons JS. Thoracic dystrophy.Arch Dis Child.1969;44:11–17
2. Burn J, Hall C, Marsden D, Matthew DJ. Autosomal dominant thoracolaryngopelvic dysplasia: Barnes syndrome.J Med Genet.
1986;23:345–349
3. Barnes ND, Hull D, Milner AD, Waterston DJ. Chest recon-struction in thoracic dystrophy. Arch Dis Child. 1971;46: 833– 837
4. Bankier A, Danks DM. Thoracic-pelvic dysostosis: a “new” autosomal dominant form.J Med Genet.1983;20:276 –279 5. Miller TL, Palmer C, Shaffer TH, Wolfson MR. Neonatal chest
wall suspension splint: a novel and noninvasive method for support of lung volume.Pediatr Pulmonol.2005;39:512–520 6. Bhutani VK, Sivieri EM, Abbasi S, Shaffer TH. Evaluation of
neonatal pulmonary mechanics and energetics: a two factor least mean square analysis.Pediatr Pulmonol.1988;4:150 –158 7. Baydur A, Behrakis PK, Zin WA, Jaeger M, Milic-Emili J. A
simple method for assessing the validity of the esophageal balloon technique.Am Rev Respir Dis.1982;126:788 –791 8. Beardsmore CS, Helms P, Stocks J, Hatch DJ, Silverman M.
Improved esophageal balloon technique for use in infants.
J Appl Physiol.1980;49:735–742
9. Fisher JB, Mammel MC, Coleman JM, Bing DR, Boros SJ. Identifying lung overdistention during mechanical ventilation by using volume-pressure loops. Pediatr Pulmonol. 1988;5: 10 –14
10. Koen PA, Moskowitz GD, Shaffer TH. Instrumentation for measuring functional residual capacity in small animals.J Appl Physiol.1977;43:755–758
11. Schwartz JG, Fox WW, Shaffer TH. A method for measuring
functional residual capacity in neonates with endotracheal tubes.IEEE Trans Biomed Eng.1978;25:304 –307
12. Fox WW, Schwartz JG, Shaffer TH. Effects of endotracheal tube leaks on functional residual capacity determination in intu-bated neonates.Pediatr Res.1979;13:60 – 64
13. Duffty P, Spriet L, Bryan MH, Bryan AC. Respiratory induction plethysmography (Respitrace): an evaluation of its use in the infant.Am Rev Respir Dis.1981;123:542–546
14. Stick SM, Ellis E, LeSouef PN, Sly PD. Validation of respiratory inductance plethysmography (“Respitrace”) for the measure-ment of tidal breathing parameters in newborns.Pediatr Pul-monol.1992;14:187–191
15. Miller TL, Blackson TJ, Shaffer TH, Touch SM. Tracheal gas insufflation-augmented continuous positive airway pressure in a spontaneously breathing model of neonatal respiratory dis-tress.Pediatr Pulmonol.2004;38:386 –395
16. Wolfson MR, Greenspan JS, Deoras KS, Allen JL, Shaffer TH. Effect of position on the mechanical interaction between the rib cage and abdomen in preterm infants.J Appl Physiol.1992; 72:1032–1038
17. Bhutani VK, Sivieri EM, Abbasi S. Evaluation of pulmonary function in the neonate. In: Polin RA, Fox WW, eds.Fetal and Neonatal Physiology. WB Saunders; 1998:1143–1164
18. Gerhardt T, Hehre D, Feller R, Reifenberg L, Bancalari E. Pulmonary mechanics in normal infants and young children during first 5 years of life.Pediatr Pulmonol.1987;3:309 –316 19. Allen JL, Greenspan JS, Deoras KS, Keklikian E, Wolfson MR,
Shaffer TH. Interaction between chest wall motion and lung mechanics in normal infants and infants with bronchopulmo-nary dysplasia.Pediatr Pulmonol.1991;11:37– 43
20. Deoras KS, Greenspan JS, Wolfson MR, Keklikian EN, Shaffer TH, Allen JL. Effects of inspiratory resistive loading on chest wall motion and ventilation: differences between preterm and full-term infants.Pediatr Res.1992;32:589 –594
21. Allen JL, Wolfson MR, McDowell K, Shaffer TH. Thoracoab-dominal asynchrony in infants with airflow obstruction.Am Rev Respir Dis.1990;141:337–342
PEDIATRICS Volume 118, Number 4, October 2006 e1267
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2006-0135 originally published online September 1, 2006;
2006;118;e1264
Pediatrics
Thomas H. Shaffer
Thomas L. Miller, Timothy Cox, Thomas Blackson, David Paul, Kerry Weiss and
Evaluation for Surgical Intervention
Pulmonary Function Assessment in an Infant With Barnes Syndrome: Proactive
Services
Updated Information &
http://pediatrics.aappublications.org/content/118/4/e1264 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/118/4/e1264#BIBL This article cites 20 articles, 4 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/pulmonology_sub Pulmonology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2006-0135 originally published online September 1, 2006;
2006;118;e1264
Pediatrics
Thomas H. Shaffer
Thomas L. Miller, Timothy Cox, Thomas Blackson, David Paul, Kerry Weiss and
Evaluation for Surgical Intervention
Pulmonary Function Assessment in an Infant With Barnes Syndrome: Proactive
http://pediatrics.aappublications.org/content/118/4/e1264
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2006 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news