167
Available at www.jpbms.info
Original article
From diem Payment to Case-based
Per-episode Payment for Acute Mental Disorders in
Guangzhou, China: A Propensity Score
Matching and Difference-in-Differences
Analysis using Real World Data
Peiyao Lu
1,+, Tiantian Zhang
1,+, Jingmei Xie
1, Sen Wang
1, Junming Lin
1,
Jeff Jianfei Guo
2,*, Jie Jiang
1,3,*Author affiliations 1
College of Pharmacy, Jinan University, Guangzhou, PR China 2
College of Pharmacy, University of Cincinnati, Cincinnati, OH, USA 3 Dongguan Institute of Jinan University, Dongguan, PR China
+
These authors contributed equally to this work
Address reprint requests to
Jie Jiang
College of Pharmacy, Jinan University, Guangzhou, PR China Email: [email protected]
Jeff Jianfei Guo
College of Pharmacy, University of Cincinnati, Cincinnati, OH, USA Email: [email protected]
Abstract:
Purpose Mental disorders affect millions of people with a great economic burden. Guangzhou, a major city in China, initiated the case-based per-episode payment policy for patients with acute mental disorders since 2015.This study aimed to explore whether aggregated payment with per-diem for chronic patients and case-based per-episode for acute patients is more cost-saving than traditional payment with per-diem for both chronic and acute patients.
Methods A total of 6,778 episodes of medical records from Feb 1, 2014 to Feb 1, 2016, including 2,091 patients in one intervention hospital and 4,687 patients in ten control hospitals were extracted from Guangzhou Urban Employee Basic Medical Insurance. Length of stay, number of hospitalization and medical expenditures per year were compared between groups. The total medical expenditures were calculated as sum of medical insurance reimbursement and patient out-of-pocket payments. Economic impact was assessed using propensity score matching (PSM) plus difference-in-differences (DID) method.
Results From governmental health insurance prospective, significant reductions in intervention group were observed in relevant economic outcomes per year per capita, including length of stay reduced 14.11 days (P=0.037), number of hospitalization reduced 0.02 times (P=0.04), medical insurance reimbursement reduced US$439.4 (P=0.017), patient out-of-pocket payments reduced US$242.4 (P<0.01), total medical expenditures reduced US$681.8 (P=0.002).
Conclusions The new payment policy was proved cost-saving and may facilitate acute mental disorder patients’ prognosis.
Key words
mental disorders, policy reform, per-diem payment, case-based per-episode payment, costanalysis.
https://doi.org/10.20936/jpbms/18/11/01
168
INTRODUCTION
ental disorders are characterized as distinctive distortions in perception and thinking as well as inappropriate or blunted affect. It includes major depression, selected anxiety disorders, bipolar disorder, schizophrenia, epilepsy, dementia, parkinson’s disease, alcohol, drug use disorder and so on[1].
According to the latest report of World Health Organization (WHO)[2], mental disorders became
one of the leading causes of years living with disability for it accounted for around 6.2% of the total global disease burden as measured in Disability Adjusted of Life Years (DALYs). As the data showed, nearly 350 million people affected by depression in the world, 60 million suffered from bipolar effective disorder and 21 million attacked by schizophrenia and other psychoses globally[3].
As the greatest component of China’s total burden of disease, mental illness surpassed tumors and cardiovascular diseases, accounted for 20% of healthcare budget[4]. In 2013, people
from developing countries experienced three-quarters of the global mental, neurological and substance use disorder burden while China shared around 17%. The disease burden especially in China, accounted for 36 million DALYs (10% of total disease burden), and other developing countries accounted for 31 million DALYs (6% of total disease burden). The heavy disease burden of acute mental disorders in China has already drawn the global attention [5]. Meanwhile,
mental disorders bring heavy financial burden[6]. One study estimated that the total annual costs
of mental disorders increased more than 3 times from 2005 (US$21.0 billion) to 2013 (US$88.8 billion) in China and the annual cost per capita has raised to US$3,665 [7], let alone the income of
those patients accounted for only around 36% of the average normal individual income[8].
As the professional therapeutic pathway suggested, mental disorders can be categorized as acute and chronic types. Patients with acute mental disorders were defined as those whose clinical global impression score (CGI score) an evaluation scale of severity of illness (CGI-SI) was more than 4 points. Unfortunately, the routine payment for these acute patients was the same as for chronic patients. Take Guangzhou as an example. Before Feb 1, 2015, either acute or chronic patients were reimbursed by per-diem payment according to which US$27-33 (¥180-215, in 2016 a US dollar was equivalent to ¥6.6) (varied by different hospital level) was paid per capita per day. It is a cost-control payment using hospital bed as the payment unit, whose essence is paid by the unit[9,10].
To enhance mental disorders management, Guangzhou city government took the first step to carry out a new policy to implement case-based per-episode payment on urban-employees patients with acute mental disorders (the Policy). The Policy covered following patients with acute mental disorders who must be eligible for Guangzhou Urban Employee Basic Medical Insurance (GUEBMI) coverage, at least one of psychiatric diagnose ICD-10 codes F00-F99 and the severe psychiatric symptoms significantly affect the social function with CGI-SI more than 4. According to official clinical pathway and standard payment for mental disorders, the total expense per capita is around US$1,515-$3,333(¥10,000-22,000)[11], basing on which each
eligible patients could be reimbursed up to (no more than) US$1,970(¥13,000) per hospital stay according to the Policy.
So far, the Policy has been carried out for more than two years. This study was aimed to assess the impact of Policy whether aggregated payment with per-diem for chronic patients as well as case-based per-episode for acute patients is more cost-saving than traditional payment with per-diem for both chronic and acute patients.
METHOD
STUDY DESIGN AND DATA SOURCE
The data in this study was sourced from GUEBMI which covered approximately six million people (71% of Guangzhou’s total population) authorized by the Guangzhou Medical Insurance Service Administration Bureau[12]. Guangzhou with 13 million people has the top three high
Gross Domestic Product among all provinces and municipalities in China. The Gross Domestic
169
Product per capita of Guangzhou has reached approximately $21,868 in 2016 and ranked sixth nationwide.
The study didn’t involve patient privacy and all data were obtained after the deletion of each patient's private information. The study period was from one year before (Feb 1, 2014-Feb 1, 2015) and one year after (Feb 1, 2015-Feb 1, 2016) the Policy. An episode was defined as the duration from admission to formal discharge. Episode claims of which admission date ranged from Feb 1, 2014 to Feb 1, 2016 with diagnose ICD-10 codes F00-F99 were included into our study including major depression, selected anxiety disorders, bipolar disorder, schizophrenia and so on. All patients episode claims from 11 mental hospitals under GUEBMI were included and divided into two groups: (a) those admitted into 10 mental hospitals without the Policy intervention were served as the control group; (b) those admitted into one pilot mental hospital were served as the intervention group.
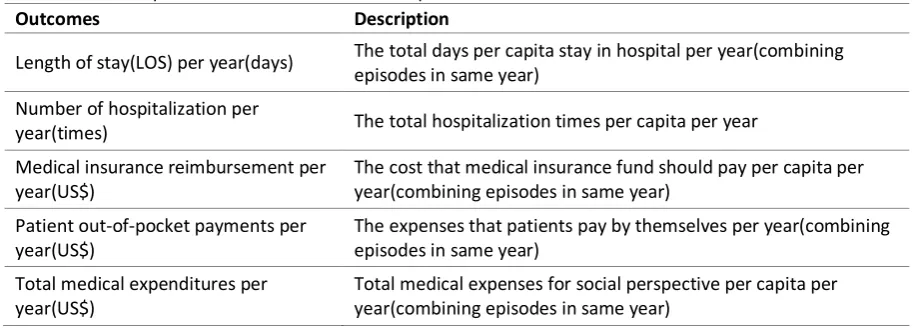
Length of stay, number of hospitalization and medical expenditures per yearwere measured and compared between intervention and control groups in the present study. The total medical expenditures were calculated as sum of medical insurance reimbursement and patient out-of-pocket payments. The description of outcomes was defined in Table 1.
Table 1 The description of economic outcomes for patients with mental disorders.
Outcomes Description
Length of stay(LOS) per year(days) The total days per capita stay in hospital per year(combining episodes in same year)
Number of hospitalization per
year(times) The total hospitalization times per capita per year Medical insurance reimbursement per
year(US$) The cost that medical insurance fund should pay per capita per year(combining episodes in same year) Patient out-of-pocket payments per
year(US$) The expenses that patients pay by themselves per year(combining episodes in same year) Total medical expenditures per
year(US$) Total medical expenses for social perspective per capita per year(combining episodes in same year)
ANALYSIS
Five economic outcome variables included: length of stay, number of hospitalization, medical insurance reimbursement, patient out-of-pocket payments and total medical expenditures.
We tested for statistically significant differences in outcomes between intervention and control group using an interaction term for intervention with a binary indicator for the intervention period. The interaction term gives the relative difference in the Policy for the intervention practices (the change in use over time beyond the change observed in the control group—the “DID”).The time schedule of the Policy was showed in Fig 1.
Fig. 1 Time schedule of the per-episode Policy between intervention and control groups.
170
control group once a particular policy is initiated while assuming that unobserved covariates are the same for both the intervention group and the control group[13,14] .Our study applied this
method to make an objective assessment for the Policy during the period from the year before (Feb 1, 2014-Feb 1, 2015) and after (Feb 1, 2015-Feb 1, 2016) the Policy. The double difference regression model was as follows:
Yit = β1 + β2 treatmenti + β3 timet +ε(treatment*time) +β4 X+ eit
Define Yit to be the observed outcomes (eg: length of stay, number of hospitalization, medical
insurance reimbursement, patient out-of-pocket payments and total medical expenditures) for individual i in period t. Treatment is the group variable (intervention vs. control). Individuals in the sample at treatment i = 0 (control group) or i = 1 (intervention group).Time is the time variable (pre- vs. post- intervention).Individuals in the sample at time t = 0 (Feb 1, 2014-Feb 1, 2015) or t = 1 (Feb 1, 2015 -Feb 1, 2016).The treatment*time is the interaction between group and time (i.e. DID estimator) and the ε represents the effect of the Policy. In the equation, X is the observed background covariates including sex (male or female), age, employment level (employed or unemployed), period (pre-Policy or post-Policy) and disease sub-type (schizophrenia, depression, bipolar disorder and else). The eit refers to the unobservable [15, 16].
The basic demographic characteristics of observations differed significantly before matching. To overcome selection bias, we matched intervention practices to control practices via the propensity score matching (PSM) method, which mitigates treatment selection bias by adjusting as many observed background covariates(including sex, age, employment level, period and disease sub-type) as possible across treatments and estimates realistically the treatment effects[17,18]. We constructed our matched control and intervention groups under three
candidate matching methods including nearest neighbour with replacement (basing on propensity score closest proximity, each intervention practice is matched to 3 control practices), radius matching(basing on propensity score falls within a given radius(r=0.2), each intervention practice is matched to all control practices) and kernel weighting(basing on weighted relative to the distance in propensity score, all control practices are matched to the intervention practices within a bandwidth)[19]. As Rosenbaum and Rubin recommended, the
standardized bias was systematically under 5% and most empirical studies consider as sufficient a standardized bias below 3% or 5% after matching[20]. We tested mean standardized
bias before and after PSM for each three methods.
Stata 14.0 were used for all analysis[21]. The significance level of all statistical tests was 0.05.
All expenditures were converted to US$ using the exchange rate of 2016 (¥6.6 = US$1).
RESULTS
Between Feb 1, 2014 and Feb 1, 2015, we identified 962 patients in the intervention group and 2,235 patients in the control group. Between Feb 1, 2015 and Feb 1, 2016, we identified 1,129 patients in the intervention hospital and 2,452 patients in control hospitals.
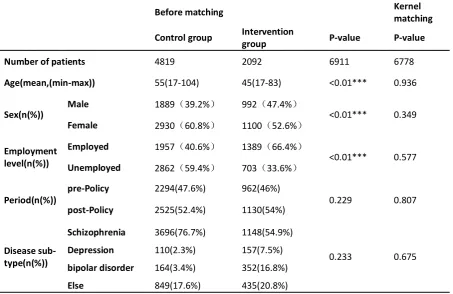
The baseline data included sex (male or female), age, employment level (employed or unemployed), period (pre-Policy or post-Policy) and disease sub-type (schizophrenia, depression, bipolar disorder and else). There was a significant difference at baseline characteristics. PSM method was used to adjust the unbalanced baseline. Comparing with the other matching methods, we chose the kernel matching method whose mean standardized bias before and after PSM is below the standard threshold of 5% (Table 2). After the matching comparisons including age, sex, employment level and disease sub-type between the intervention and control groups, no significant differences at baseline were observed as shown in Table 3.
171
per year (P=0.037).The reduction rate of number of hospitalization of intervention group was significantly decreased by 1.58% equaling 0.02times (P=0.04) per year (Table 4).
Meanwhile, Table 4 also showed that the medical insurance reimbursement decreased US$439.4(P=0.017), the patient out-of-pocket payments decreased US$242.4 (P<0.01), the total medical expenditures decreased US$681.8 (P=0.002).
Table 2 The mean standardized bias (%) before and after propensity score match (PSM) of three candidates.
Unmatched(U) %bias
Matched(M) Nearest neighbours matching(n=3) Radius matching(r=0.2) Kernel matching
Age U M -68.3 4.4 -68.3 1.9 -68.3 0.2
Sex U M -16.7 -3.6 -16.7 4.2 -16.7 -2.9 Employment
level U M -53.5 -4 -53.5 -4.2 -53.5 -1.7
Period U M 3.1 7.7 3.1 1.2 3.1 0.8
Disease sub-type U M 3.2 13 3.2 -12.1 3.2 1.3
NOTES:baseline data included sex (male or female), age, employment level (employed or unemployed), period (pre-Policy or post-Policy) and disease sub-type (schizophrenia, depression, bipolar disorder and else); nearest neighbour with replacement (each intervention practice is matched to 3 control practices), radius matching (basing on propensity score falls within a given radius (r=0.2), each intervention practice is matched to all control practices).
Table 3 Basic demographic characteristics of patient before and after matching.
Before matching Kernel matching
Control group Intervention group P-value P-value
Number of patients 4819 2092 6911 6778
Age(mean,(min-max)) 55(17-104) 45(17-83) <0.01*** 0.936
Sex(n(%)) Male 1889(39.2%) 992(47.4%) <0.01*** 0.349
Female 2930(60.8%) 1100(52.6%)
Employment level(n(%))
Employed 1957(40.6%) 1389(66.4%)
<0.01*** 0.577
Unemployed 2862(59.4%) 703(33.6%)
Period(n(%)) pre-Policy 2294(47.6%) 962(46%) 0.229 0.807
post-Policy 2525(52.4%) 1130(54%)
Disease sub-type(n(%))
Schizophrenia 3696(76.7%) 1148(54.9%)
0.233 0.675
Depression 110(2.3%) 157(7.5%)
bipolar disorder 164(3.4%) 352(16.8%)
Else 849(17.6%) 435(20.8%)
172
Average Difference-in-differences estimate
Control
group Intervention group S. Err Estimate P-value
Length of stay(days) Pre Post 262.39 260.29 133.63 115.62 7.76 -14.11 0.04**
Number of
hospitalization(times)
Pre 1.02 1.06
0.01 -0.02 0.04**
Post 1.04 1.06
Medical insurance reimbursement(US$)
Pre 6299.30 3830.87
185.48 -439.4 0.017**
Post 6760.63 3769.60
Patient out-of-pocket payments(US$)
Pre 853.42 1414.40
218.7 -242.4 <0.01***
Post 1051.72 1372.36
Total medical expenditures(US$)
Pre 7152.72 5245.27
49.19 -681.8 0.002**
Post 7809.22 5141.96
NOTES: S. Err means standard error; *** indicates significance at the 1% level, ** at the 5% level.
DISCUSSION
As our study showed, there were both a significant reduction found in terms of the length of stay and hospitalization times per capita per year. Meanwhile, the relative cost (medical insurance reimbursement, patient out-of-pocket payments and total medical expenditures) reduced significantly for mental disorders patients after the Policy. To explore the reason behind the remarkable reduction of cost, we speculated that under the greater support of health insurance reimbursement (up to no more than US$1,970), acute patients could get access to timely treatment with expensive but efficient medicines and may recover more easily. Therefore, due to the shortening of the length of stay and better prognosis, total cost dropped prominently.
For years, to contain the roaring up medical expenditures and release the patient economic burden without compromise of treatment quality and cost-saving, China has initiated numerous pilot programs on provider payment reform. During 2001-2009, the payment reforms from FFS to case-based payment were implemented in Chongqing for acute appendicitis[22], Jining for 128
included disease[23] as well as Hainan for catastrophic diseases[24], Zhenan for the diseases
included in the new rural cooperative medical care scheme[25]. Without exception, all these
pilots found an obvious reduction in relative healthcare expenditures. ZHOU studied the feasibility and operating environment of Diagnosis-Related Groups (DRGs) by comparing effects of DRGs and FFS in Hepu county of Guangxi province[26]. JIAN evaluated the impact of the
initiatives carried out in Beijing’s six hospitals (initiatives moving from FFS to prospective and aggregated payment methods including the use of DRGs) on cost-containment and found a positive controlling effect in the hospitalization expenses without significant negative effects on the medical quality[27]. In Jan 2017, Chinese central government announced 320 selected
173
However, as international experience showed, no provider payment is perfect, neither is the Policy. First of all, there was an absence of standardized assessment system for the effectiveness of the Policy.In light of expert opinions, the score improvement of professional Psychiatric Rating Scales (such as Hamilton Depression Scale(HAMD) for depression, Hamilton Anxiety Scale(HAMA) for anxiety, positive and negative syndrome scale(PANSS) for schizophrenia clinical global impression (CGI) for general mental disorders) should be taken as a critical discharge criteria for treatments effectiveness evaluation. Nonetheless, the scale measurement service wasn’t regulated as a compulsory procedure by many hospitals because it was out of the reimbursement list of Guangzhou Medical insurance. Therefore, only if the professional scales measurement were reimbursed, can the scales be accepted by healthcare providers and patients and consequently, can the effectiveness of case-based payment per-episode be well monitored and guaranteed.
Secondly, it was an unanswered issue that whether the reimbursement ceiling US$1,970 (¥13,000) was appropriate. A more accurate level may be reset after taking into account other cost such as comorbidity and side effect. Furthermore, to virtually stimulate hospital and clinical practitioners’ incentive on cost containment, payment ceiling should be replaced by fix amount and retrospective payment should be replaced by perspective payment on the premise that medical quality can be fully guaranteed.
As a retrospective study using the real world data, there were some additional limitations of the study. First, without the Psychiatric Rating Scale score changing from admission to formal discharge, we couldn’t have an accurate outcome to evaluate the effectiveness between two payments. Under this circumstance, number of hospitalization per year per capita was chosen as a substitute for clinical effectiveness assessment, which was deemed as a compromising choice and may overestimate the Policy effect on effectiveness. Therefore, further prospective study was suggested to capture comprehensive outcome such as rate of relapse, rate of readmission and other clinical effectiveness indicators.
Second, although the intervention and control group existed in similar local environment and appeared well balanced on variables after matching, more baseline characteristics information such as comorbidity and severity of patients was missing and not taken into analysis, which may bring potential bias.
Third, as the Policy has only been implemented in some particular hospitals for about two years, long term follow-up and observation should be conducted to draw a more robust and strong evidence-based conclusion, even the preliminary effect is encouraging and meaningful. Besides, satisfaction survey for clinical practitioners, patients as well as insurance administrative officers and other policymakers is necessary in further research.
CONCLUSION
Regardless of these weaknesses, the Policy of moving from per-diem payment to aggregated payment with per-episode payment for acute patients and per-diem payment for chronic patients was proved cost-saving. This study played as a demonstration for future similar evaluations as China now are announcing a series of ambitious provider payment reforms. Undoubtedly, concerning the uniqueness and specificity (demographic structure, population feature, economic development, medical service quality level, etc.) of other different settings, the scale up of the Policy should be conducted gradually and cautiously.
REFERENCES
1. Whiteford HA, Ferrari AJ, Degenhardt L, Feigin V, Vos T. The Global Burden of Mental, Neurological and Substance Use Disorders: An Analysis from the Global Burden of Disease Study 2010. Plos One. 2015;10(2). 2. Organization WH. Health in 2015: From MDGs
to SDGs Switzerland: Gov; 2015 [cited 2016
Oct 19th]. Available from:
http://www.who.int/gho/publications/mdgs-sdgs/en/
174 http://www.who.int/mediacentre/factsheets/fs
396/en/.
4. Feng Y, Xiong XJ, Xue QJ, Yao L, Luo F, Xiang L. The Impact of Medical Insurance Policies on the Hospitalization Services Utilization of People with Schizophrenia: A Case Study in Changsha, China. Pak J Med Sci. 2013;29(3):793-8.
5. Charlson FJ, Baxter AJ, Cheng HG, Shidhaye R, Whiteford HA. The burden of mental, Neurological, and Substance use Disorders in China and India: A Systematic Analysis of Community Representative Epidemiological Studies. Lancet. 2016;388(10042):376-89. 6. Baxter AJ, Charlson FJ, Somerville AJ,
Whiteford HA. Mental disorders as risk factors: assessing the evidence for the Global Burden of Disease Study. Bmc Med. 2011;9. 7. Xu JF, Wang J, Wimo A, Qiu CX. The Economic
Burden of Mental Disorders in China, 2005-2013: Implications for Health Policy. Bmc Psychiatry. 2016;16.
8. Zhang G. A Survey on the Healthcare Affordability of Mental Disorders Hopitalizated Insured Patient. Shanghai Arch Psychiatry. 2001;13(1):56-8.
9. Wang Kun WH, Du Yukai,et al. Analysis on the Modes of Medical Insurance Payment of Mental Health Insititutions Chin J Soc Med,. 2013;30:57-9.
10. Zheng Hong CQ, Zhao Lijun. Psychiatric Hospitals Under the New Health Care Health Insurance Payment and Cost Control. J Trad Chin Medi Man. 2013;11:1195-7.
11. China NHaFPCotPsRo. Implementaion for the clinical pathway of five severe mental disorders including bipolar disorder Beijing: Gov; 2013 [Available from: http://www.moh.gov.cn/zwgkzt/lclj/201306/f3 3f5a32f2594edd935a758f12752b5d.shtml. 12. Bureau GS. Statistical Communique of
Guangzhou on the 2016 Economic and Social development Guangzhou: Gov; 2017
[Available from: http://data.gzstats.gov.cn/gzStat1/chaxun/njsj
.jsp.
13. Antonakis J, Bendahan S, Jacquart P, Lalive R. On making Causal Claims: A Review and Recommendations. Leadership Quart. 2010;21(6):1086-120.
14. Angrist JD PJ-S. Mostly Harmless Econometrics: An Empiricist's Companion. Princeton: Princeton University Press; 2009. 15. Shen M, Hu M, Sun Z. Assessment of
School-Based Quasi-Experimental Nutrition and Food Safety Health Education for Primary School Students in Two Poverty-Stricken Counties of West China. PLoS One. 2015;10(12):e0145090.
16. Hutchinson PL, Meekers D. Estimating Causal Effects from Family Planning Health Communication Campaigns Using Panel Data: The "Your Health, Your Wealth'' Campaign in Egypt. Plos One. 2012;7(9).
17. Di Staso M, Gravina GL, Zugaro L, Bonfili P, Gregori L, Franzese P, et al. Treatment of Solitary Painful Osseous Metastases with Radiotherapy, Cryoablation or Combined Therapy: Propensity Matching Analysis in 175 Patients. PLoS One. 2015;10(6):e0129021. 18. Hammond GC, Croudace TJ, Radhakrishnan
M, Lafortune L, Watson A, McMillan-Shields F, et al. Comparative Effectiveness of Cognitive Therapies Delivered Face-to-Face or over the Telephone: An Observational Study Using Propensity Methods. Plos One. 2012;7(9). 19. Whittaker W, Anselmi L, Kristensen SR, Lau YS,
Bailey S, Bower P, et al. Associations between Extending Access to Primary Care and Emergency Department Visits: A Difference-In-Differences Analysis. Plos Med. 2016;13(9):e1002113.
20. Caliendo M, Kopeinig S. Some practical guidance for the implementation of propensity score matching. J Econ Surv. 2008;22(1):31-72.
21. Leuven E SB. PSMATCH: Stata module to perform full Mahalanobis and propensity score matching, common support graphing, and covariate imbalance testing 2003
[Available from: https://ideas.repec.org/c/boc/bocode/s43200
1.html.
22. Luo K NC, Dai W, et al. The Impact of Mixed Payment Systems in NCMS in Qianjiang of Chongqing. Chin J Hosp Manage. 2007;8:33-4.
23. Wu G ZY, Liu G, et al. Social Benefits from Adoption of Case-based Payment System. Chin J Hosp Manage. 2007;9:26-8.
24. Yip W, Eggleston K. Provider Payment Reform in China: The Case of Hospital reimbursement in Hainan province. Health Econ. 2001;10(4):325-39.
25. Chen Yao LH, Yu Y,Chen ML,Yao L. The Research on The Hospitalization Expenses Controlling Effects of the Quota for Single Disease Payment in Zhenan County Shaanxi province. Chinese Journal of Health Policy. 2009;2(9):18-23.
26. Zhou XY WL, Mao ZZ,et al. The Analysis of The Effect of DRGS in Hepu County of Guangxi Province. Mod Prev Med. 2006;33(11):2132-3.
175
Article citation: Peiyao Lu, Tiantian Zhang, Jingmei Xie,Sen Wang,Junming Lin, Jeff Jianfei Guo, Jie Jiang. From Per-diem Payment to Case-based per-Episode Payment for Acute Mental disorders in Guangzhou, China: A Propensity Score Matching and Difference-in-Differences Analysis Using Real World Data. J Pharm Biomed Sci. 2018;08(11):167-175. Available at htp://www.jpbms.info
Author Contributions: All authors were responsible for the structure of this paper. Jie Jiang and Tiantian Zhang contributed to the conception and design. Peiyao Lu and Jingmei Xie conducted literature search.Sen Wang and Junming Lin analyzed the data. Tiantian Zhang and Peiyao Lu drafted the paper. Jeff Jianfei Guo conducted critical revisions of the paper. And all authors approved the final versions for submission.
Conflicts of Interest: Tiantian Zhang, Jingmei Xie, Sen Wang, Jeff Jianfei Guo and Jie Jiang declare that they have no conflict of interest.
Statement of originality of work: The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and that each author believes that the manuscript represents honest and original work.
Source of support:This study was supported by the National Natural Science Foundation of China [Grant no. 71704064], the Natural Science Foundation of Guangdong Province, China [Grantno. 2017A030310174], and the Fundamental Research Funds for the Central Universities [Grant no. 21616324]. Publication of the study results was not contingent upon sponsor’s approval.
Conference presentation: Part of this paper was presented at the ISPOR Asia Pacific 2018 Meeting.