Pediatric Pneumococcal Bone and Joint Infections
John S. Bradley, MD*; Sheldon L. Kaplan, MD‡; Tina Q. Tan, MD§; William J. Barson, MDi; Moshe Arditi, MD¶; Gordon E. Schutze, MD#; Ellen R. Wald, MD**;
Laurence B. Givner, MD‡‡; Edward O. Mason, PhD‡; and
The Pediatric Multicenter Pneumococcal Surveillance Study Group (PMPSSG)
ABSTRACT. Objective. To describe the clinical and microbiological characteristics of infants and children with bone and joint infections caused by penicillin-sus-ceptible and penicillin-nonsuspenicillin-sus-ceptible strains of Strepto-coccus pneumoniae.
Design. Multicenter, prospective patient accrual; ret-rospective chart review of identified patients.
Setting. Eight children’s hospitals in the United States.
Participants. Forty-two children with bone and/or joint infections prospectively enrolled in the United States Pediatric Multicenter Pneumococcal Surveillance Study from September 1, 1993 to August 31, 1996.
Outcome Measures. Data were collected on multiple variables, including age, gender, race, days of symptoms before and during hospitalization, antibiotic and surgical therapy, laboratory and imaging studies.
Results. Of the 42 children enrolled (21 bone, 21 joint infections), 14 had isolates that were not susceptible to penicillin. Eight of 16 (50%) strains isolated from chil-dren who received antibiotics within 4 weeks before hospitalization were not susceptible to penicillin, com-pared with 4 of 15 (27%) strains isolated from children without previous antibiotic exposure. Clinical response to therapy was similar between children infected by pen-icillin-susceptible strains compared with those infected by penicillin-nonsusceptible strains, including duration of hospitalization (9.1 days vs 11.2 days), days of intra-venous antibiotic therapy (25.3 days vs 24.6 days), days of fever (3.6 days vs 3.1 days), and sequelae (14% vs 7%). The most commonly prescribed single agents for paren-teral therapy in definitive treatment were ceftriaxone (36%), penicillin (15%), and clindamycin (15%). Oral ther-apy followed parenteral therther-apy in 56% of children. The mean (6standard deviation) duration of total antibiotic therapy in children with osteomyelitis was 57.5 6 48.6 days (range, 23–196 days) and 29.2 6 11.8 days (range, 12– 67 days) for arthritis. Late sequelae (long-term de-structive changes of the bone or joint) were documented in 5 (12%) children, 4 with osteomyelitis, and 1 with arthritis. Sequelae occurred in 30% of children with long
bone osteomyelitis associated with infection in the adja-cent joint. The age of children with sequelae was younger than those without sequelae (6.4 months vs 18.6 months).
Conclusions. The demographic characteristics and an-atomic sites of infection in our patients were similar to previously published series collected from single insti-tutions before the emergence of significant antibiotic resistance in S pneumoniae. Our analysis suggests that children infected by penicillin-nonsusceptible strains have a similar clinical response to therapy when com-pared with children infected by penicillin-susceptible strains.Pediatrics1998;102:1376 –1382;septic arthritis, os-teomyelitis, antibiotic therapy, penicillin resistance, Streptococcus pneumoniae.
ABBREVIATIONS. PMPSSG, Pediatric Multicenter Pneumococcal Surveillance Study Group; MIC, minimum inhibitory concentra-tion; SD, standard deviaconcentra-tion; WBC, white blood cell count; PEN-S, penicillin-susceptible; PEN-NS, penicillin-nonsusceptible.
S
treptococcus pneumoniae is responsible for a small but consistent proportion (0%-4%) of all bone and joint infections in infants and chil-dren, following the more prevalent pathogens, Staph-ylococcus aureus, Streptococcus pyogenes, and in the pre-Haemophilus vaccine era, Haemophilus influenzae type b.1–13Bone and joint infections are a raremani-festation of invasive disease caused by pneumococ-cus in children, in contrast to the organism’s domi-nant role as a cause of bacteremia, meningitis, and respiratory tract infections.14 Previous reviews of
bone and joint infections caused by this organism in children have focused retrospectively on the clinical characteristics of infection in a single institution or region throughout time. These reports appeared be-fore the development of widespread antibiotic resis-tance inS pneumoniaein the United States. The Pedi-atric Multicenter Pneumococcal Surveillance Study Group (PMPSSG) was organized to collect current information in a prospective manner on all children with invasive pneumococcal disease seen in eight pediatric centers across the United States. During the first 3 years of surveillance by the PMPSSG, data were collected on the clinical manifestations of the infections caused by S pneumoniae, as well as the microbiological characteristics of these organ-isms.15–17 For this report, we examined the clinical
and laboratory characteristics of 42 children with pneumococcal bone and joint infections at the PMPSSG sites during the first 3 years of prospective From the *Children’s Hospital and University of California, San Diego,
California; the ‡Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas; the §Children’s Memorial Hospital, Chicago, Illinois; the
iColumbus Children’s Hospital, Columbus, Ohio; the ¶Children’s Hospital, Los Angeles, California; the #University of Arkansas for Medical Sciences and Arkansas Children’s Hospital, Little Rock, Arkansas; the **Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania; and the ‡‡Brenner Chil-dren’s Hospital, Winston-Salem, North Carolina.
Received for publication Mar 3, 1998; accepted May 7, 1998.
Reprint requests to (J.S.B.) Children’s Hospital, San Diego, 3020 Children’s Way, MC 5041, San Diego, CA 92123.
surveillance. This report represents the largest series of pneumococcal bone and joint infections in chil-dren.
METHODS Data Collection
Children with invasive pneumococcal infections were identi-fied prospectively between September 1, 1993 and August 31, 1996 from the eight children’s hospitals that comprise the PMPSSG: Texas Children’s Hospital, Houston, TX; Children’s Memorial Hospital, Chicago, IL; Columbus Children’s Hospital, Columbus, OH; Children’s Hospital of San Diego, San Diego, CA; Children’s Hospital of Los Angeles, Los Angeles, CA; Arkansas Children’s Hospital, Little Rock, AR; Brenner Children’s Hospital, Winston-Salem, NC; and Children’s Hospital of Pittsburgh, Pittsburgh, PA. Cases were identified based on positive cultures forS pneumoniae
from either blood or from other sterile body sites.
This report for osteomyelitis and septic arthritis analyzed data from children with a positive culture forS pneumoniaefrom a bone or joint, or those who had a positive blood culture forS pneumoniae
in the context of a clinical case of osteomyelitis or septic arthritis (based on results of examination, laboratory tests, and imaging studies). Charts were reviewed retrospectively using a standard-ized case report form. Data collected included information on the characteristics and duration of the presenting signs and symptoms of the infection, the clinical course during hospitalization, medical and surgical therapy, laboratory and imaging studies performed, characteristics of theS pneumoniaeisolate, and long-term outcome. Antibiotic susceptibilities and serotyping were performed by the C. T. Parker Infectious Diseases Laboratory, Texas Children’s Hospital. Susceptibilities were determined by microbroth dilution using Mueller-Hinton broth supplemented with 3% lysed horse blood.18Susceptibility breakpoints were based on the National Committee for Clinical Laboratory Standards guidelines.19 Organ-isms were considered: 1) susceptible to penicillin if they demon-strated a minimum inhibitory concentration (MIC)#0.06mg/mL; 2) intermediate to penicillin for a MIC of 0.1 to 1.0mg/mL; and 3) resistant to penicillin for a MIC $2.0 mg/mL. For ceftriaxone, organisms were considered: 1) susceptible if they demonstrated a MIC#0.5mg/mL; 2) intermediate for a MIC of 1.0mg/mL; and 3) resistant for a MIC $2.0 mg/mL. Organisms were considered nonsusceptible if they were either intermediate or resistant.
Strains were serotyped by the quellung reaction using commer-cially available antisera (Staten Seruminstitut, Daco, Inc, Carpin-teria, CA).
Statistical Analysis
Differences in clinical and laboratory parameters between the populations infected by penicillin-susceptible (PEN-S) strains and those infected with penicillin-nonsusceptible (PEN-NS) strains were calculated using the two-samplettest (Data Desk 4.0, Data Description, Ithaca, NY). Dichotomous variables were analyzed byx2.
RESULTS Demographics and Concurrent Illness
A total of 1255 children with invasive infections
caused by S pneumoniae were identified by the
PMPSSG during the 3-year data-collection period. Bone or joint infections were documented in 42 (3%) of these children. The mean (6 standard deviation [SD]) age of the 42 infected children was 17.1620.6 months, with a range of 11 days to 9 years; 30 chil-dren were male. There were 15 black chilchil-dren, 22 white children, and 5 Hispanic children. The mean (6SD) ages of the 21 children with bone infections and the 21 children with joint infections were 12.06 22.4 months and 21.5618.0 months, respectively (ns, P 5 .1). One child with arthritis had concurrent meningitis. Otitis media was concurrently diagnosed
in 5 of the 21 (23%) children with bone infections and in 6 of the 21 (29%) children with joint infections.
With respect to underlying immune-compromis-ing conditions, one 5-year-old boy with septic arthri-tis of the knee had previously undergone bone mar-row transplantation for leukemia. One 13-month-old girl, also with septic arthritis of the knee, was noted to have sickle cell trait. No other children were doc-umented to have an underlying condition that could potentially predispose to invasive pneumococcal in-fection.
Osteomyelitis
Sites of bone infection identified were: proximal femur (n 5 2), distal femur (n 5 5), proximal hu-merus (n53), distal humerus (n52), proximal tibia (n52), distal tibia (n52), calcaneus (n53), ileum (n 5 1), and 6th anterolateral rib (n 5 1). No child had two concurrent sites of osteomyelitis. Ten of 16 children with long bone osteomyelitis had clinically evident septic arthritis of the adjacent joint. The mean age of those with associated arthritis, 7.6 months, was statistically similar to those without arthritis, 6.8 months (P5.7). The knee was the most commonly associated joint, related to osteomyelitis in the adjacent femur (3 cases) and tibia (1 case), followed by the shoulder (2 cases), the elbow (2 cases of infection in the humerus), the hip (1 case), and the ankle (1 case of infection of the tibia). One child had septic arthritis of the right hip in association with osteomyelitis of the right proximal tibia. Four of the 21 children (19%) with osteomyelitis had a history of nonpenetrating trauma to the area infected, includ-ing an 11-day-old male with osteomyelitis of the proximal humerus after birth trauma to the arm. Children with osteomyelitis had a history of de-creased range of motion of the affected extremity before hospitalization for a mean of 5.1 days, and fever before hospitalization for a mean of 5.6 days (Table 1).
Arthritis
The site of infection for the 21 children with arthri-tis without concurrent osteomyeliarthri-tis was: hip (n 5 10), knee (n 5 8), and ankle (n5 4). One child had arthritis at two sites simultaneously (right knee and left hip). Only 2 of the 21 children with septic arthri-tis had a recognized history of trauma to the affected joint. Before hospitalization these children had a his-tory of 2 to 3 days of decreased range of motion of the affected joint or failure to bear weight, and a history of fever for a mean of 3.0 days (Table 1).
History of Illness
femur visited a clinic eight times for the same com-plaint throughout a period of 45 days before hospi-talization. Two children were initially hospitalized for fever without signs or symptoms of bone or joint infection. These children were subsequently docu-mented to be bacteremic; 1 developed signs of a knee infection 2 days after admission to the hospital and 1 was diagnosed with osteomyelitis of the femur by radiograph after 5 days of hospitalization.
History of Previous Antibiotic Use
Antibiotic use within 4 weeks of hospitalization was reported in 16 of 32 children from whom these data were available. In 10 patients the history of previous antibiotic use was unknown. The most fre-quent antibiotics used before hospitalization were: amoxicillin (6 children), intramuscular ceftriaxone (4 children), cefaclor (3 children), amoxicillin-clavu-lanate (2 children), azithromycin (2 children), and trimethoprim-sulfamethoxazole (2 children). Suscep-tibility data were available for 31 strains isolated from the 32 children from whom information was available on previous antibiotic use. Of strains cul-tured from those with antibiotic use, 8 of 16 (50%) had decreased susceptibility to penicillin, and 3 of 16 (19%) had decreased susceptibility to ceftriaxone. For those children without previous antibiotic therapy only 4 of 15 strains (27%) had decreased susceptibil-ity to penicillin and 3 of 15 strains (20%) had de-creased susceptibility to ceftriaxone (x251.78,P..1
with respect to penicillin susceptibility).
Laboratory
Microbiology
In 15 of 21 children with osteomyelitis the adjacent joint was tapped, yielding a positive Gram’s stain for Gram-positive diplococci in 7 and positive cultures in 10, suggesting an associated joint infection in at least 10 of the 21 (48%). Ten children with osteomy-elitis were documented to have concurrent bactere-mia. Blood was the only site of pathogen isolation in 6, bone was the only site in 5, and the adjacent joint was the only site in 5 children. Of the 21 children with septic arthritis, cultures of synovial fluid were positive in 19 and blood cultures were positive in 9. The joint was the only site of isolation of S
pneu-moniae in 12 children; blood was the only site of isolation in 2. One child with an infected shoulder had group A streptococcus isolated in addition toS pneumoniae from cultures of the synovial fluid.
Susceptibility data were available for 41 of the 42 strains originally isolated. Nine strains isolated from children with osteomyelitis, and 5 strains isolated from children with arthritis demonstrated decreased susceptibility to penicillin. Nonsusceptibility to ceftriaxone was demonstrated in 5 strains isolated from children with osteomyelitis and in 3 strains isolated from children with arthritis (Table 2).
Isolates from 21 children with osteomyelitis and 20 children with arthritis were serotyped. From chil-dren with osteomyelitis, the most commonly identi-fied serotypes were: type 19 (n 56), type 6 (n 54), type 9 (n5 4), type 23 (n5 3), and type 18 (n52). Serotypes most commonly identified in children with arthritis were: type 6 (n5 8), type 19 (n 5 4), type 23 (n53), and type 14 (n52). The distribution of serotypes in children with osteomyelitis and adja-cent arthritis reflected the overall distribution of se-rotypes in children with osteomyelitis, with a pre-dominance of type 19. Serotypes of isolates with decreased susceptibility to penicillin and ceftriaxone are also noted on Table 2.
TABLE 1. Clinical and Laboratory Data Observed in Children With Pneumococcal Bone and Joint Infections
Data Bone (n521) Joint (n521)
Before hospitalization
Tmax °F6SD* (range) 102.361.7 (99–105.4) 10361.1 (101–105)
Duration of fever.100.4°F, days6SD (range) 5.665.6 (1–24) 3.062.0 (1–10)
Decreased range of motion, days 5.166.1 (0–18) 2.161.1 (0–4)
Failure to bear weight (days) 2.161.4 (1–4) 2.262.3 (1–10)
Tenderness (days) 3.864.5 (1–18) 1.761.2 (1–5)
During hospitalization
Duration of fever.100.4°F, days SD, (range) 4.265.5 (1–24) 3.662.7 (1–6)
Hospital stay (days) 12.069.5 (4–27) 7.563.9 (4–17)
Laboratory studies at hospital admission
Peripheral white blood cell count (3103/mm3) mean6SD 19.968.3 21.3614.9
ESR† mm/h, mean6SD 64.8625.4 62.9624.9
CRP‡ mg/dL (mean6SD) 15.4613.6 19.3610.5
* Standard deviation.
† Erythrocyte sedimentation rate. ‡ C-reactive protein.
TABLE 2. Minimum Inhibitory Concentrations (mg/mL) of Penicillin and Ceftriaxone for All Penicillin-Nonsusceptible Strains ofStreptococcus pneumoniae
PEN (mg/mL) CRO (mg/mL) Serotype
Bone infections
4.0 1.0 23
4.0 1.0 6
2.0 1.0 23
2.0 1.0 9
2.0 1.0 9
2.0 0.5 35
1.0 0.5 6
0.5 0.5 6
0.125 0.015 19
Joint infections
2.0 1.0 6
2.0 1.0 9
2.0 0.5 19
0.5 4.0 23
0.125 0.125 14
Hematology
The peripheral white blood cell (WBC) count, erythrocyte sedimentation rate, and C-reactive pro-tein concentration at the time of diagnosis in children with bone infections and joint infections are given in Table 1. Because of the retrospective nature of the data collection, serial determinations of erythrocyte sedimentation rate and C-reactive protein were not available for analysis on most patients.
Of children with arthritis, without associated os-teomyelitis, the mean WBC count in synovial fluid was 187 500/mm3(range, 2000 – 412 000) with a mean
of 84% of WBCs identified as polymorphonuclear leukocytes. Similarly, in children with osteomyelitis associated with septic arthritis from whom data were available, the mean WBC count in synovial fluid was 124 000/mm3with 83% of WBCs described as
poly-morphonuclear leukocytes.
Imaging
Twenty of the 21 children with osteomyelitis had radiographs taken of the affected bone. In 14 of the 20, abnormalities of the bone or periosteum were demonstrated. Of these 14, 5 had radionuclide bone scans, 4 of which were interpreted as positive. Four of the remaining 6 patients with normal radiographs had positive radionuclide bone scans. In the other 2 children with normal radiographs and negative scans, the diagnosis was made by performance of a surgical procedure on the affected extremity (aspira-tion of the proximal femur) in 1 child and by fol-low-up radiographs 5 days into hospitalization, demonstrating radiolucencies of the proximal femur in the other. The single child who did not have a radiograph obtained at the time of admission had a positive radionuclide bone scan. Data were not sys-tematically collected on the types of imaging proce-dures in arthritis.
Treatment Course
Surgical Therapy
Data on surgical procedures were recorded for 19 children with osteomyelitis: 12 had incision and drainage, 5 had aspiration only, and 2 had no surgi-cal procedure performed. Data on the specific types of surgical procedures were not collected.
Incision and drainage was performed on all but 2 children with septic arthritis (1 with a hip infection and 1 with a knee infection, both treated with aspi-ration only). One child (left shoulder infection) re-quired two drainage procedures. Surgical drains were placed in all children except for the two infec-tions treated with aspiration only. The average (6SD) duration that the surgical drain was left in place was 2.16 0.7 days (range, 1–3 days).
Medical Therapy
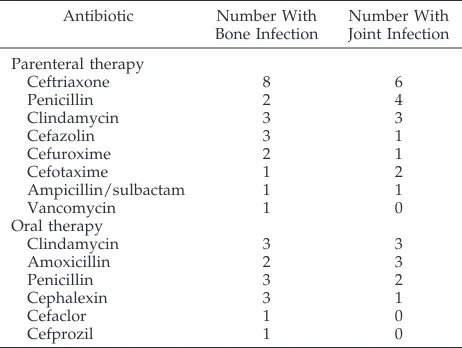
Antibiotics used most often for definitive paren-teral therapy and for oral therapy are listed in Table 3. For children with bone infections, the mean num-ber of days (6SD) of intravenous therapy was 31.66 28.8 (range, 6 –126 days); 13 received follow-up oral therapy for a mean of 43.1644.6 days (range, 12–147
days). The total antibiotic course for children with bone infections was 57.5 648.6 days (range, 23–196 days), with a median of 38 days.
For joint infections, the duration of intravenous therapy was shorter than for osteomyelitis, with a mean of 18.9 6 13.4 days (range, 3– 67 days); 9 re-ceived oral therapy for a mean of 22.1 6 8.9 days (range, 7–35 days). Total antibiotic therapy for joint infections (parenteral plus oral) was 29.2611.8 days (range, 12– 67 days).
Clinical Course of Children Infected With PEN-S Versus PEN-NS Isolates
Of the 9 children with osteomyelitis caused by PEN-NS strains, the mean duration of intravenous therapy was 30.6 days, compared with a mean dura-tion in the group with infecdura-tion caused by PEN-S strains of 32.3 days. For the 5 children with joint infections caused by PEN-NS strains, the mean du-ration of intravenous therapy was only 13.8 days, compared with 20.5 days in the 16 infected by PEN-S strains. The duration of hospitalization in the 14 children with bone or joint infections caused by PEN-NS strains was 11.2610.9 days, compared with 9.165.2 days in children with infections caused by PEN-S strains (P5 .4). The mean duration of fever during hospitalization for those children infected by nonsusceptible strains was 3.162.2 days; similar to that for children infected by susceptible strains, 3.66 4.6 days (P5.66). The ages of children infected with PEN-NS strains were statistically similar to those infected with PEN-S strains (11.7 months vs 19.8 months,P5 .24).
Definitive parenteral antibiotic therapy for chil-dren with osteomyelitis infected by PEN-NS strains consisted of ceftriaxone or cefotaxime (n 5 4), clin-damycin (n 5 3), vancomycin (n 5 1), or cefazolin (n 5 1). Five of the 9 children with bone infections caused by PEN-NS strains received oral follow-up therapy with clindamycin (n 5 2), amoxicillin (n 5 1), cefaclor (n 5 1), or cefprozil (n 5 1). Definitive parenteral therapy in children with arthritis infected by PEN-NS strains consisted of clindamycin (n5 3) or ceftriaxone/cefotaxime (n 5 2). Three of the 5
TABLE 3. Antibiotics Used Primarily for Definitive Paren-teral and Oral Therapy for Bone and Joint Infections
Antibiotic Number With
Bone Infection
Number With Joint Infection
Parenteral therapy
Ceftriaxone 8 6
Penicillin 2 4
Clindamycin 3 3
Cefazolin 3 1
Cefuroxime 2 1
Cefotaxime 1 2
Ampicillin/sulbactam 1 1
Vancomycin 1 0
Oral therapy
Clindamycin 3 3
Amoxicillin 2 3
Penicillin 3 2
Cephalexin 3 1
Cefaclor 1 0
children with joint infections caused by PEN-NS strains received oral follow-up therapy, all with clin-damycin.
Outcome
Sequelae were documented in 4 of the 21 (19%) children with osteomyelitis and in 1 of the 21 (5%) with arthritis. In all children with long bone osteo-myelitis demonstrating sequelae, organisms were cultured from the joint adjacent to the infected bone. Sequelae included a flexion contracture of the knee (distal femur), malalignment of the elbow joint (sec-ondary to changes in the proximal radius and distal humerus), destructive changes of the distal femoral epiphysis, rib resection in 1 child with rib osteomy-elitis, and avascular necrosis of the femoral head in 1 child with arthritis of the hip. Only 1 of 5 children noted to have sequelae was infected by a PEN-NS strain of pneumococcus (penicillin MIC 5 2.0 mg/ mL, ceftriaxone MIC 5 1.0mg/mL). The mean du-ration of symptoms before diagnosis, 7.7 days, was not significantly greater than for those without se-quelae. Antibiotic therapy was also similar between the two groups. The mean age of those with sequelae was 6.4 months, significantly less than the age of those without sequelae, 18.5 months,P5 .0078.
DISCUSSION
Bone and joint infections caused by S pneumoniae have been well-described.1–13,20 –26 This organism is
the responsible pathogen in up to 4% of all bacterial bone infections, and up to 20% of bacterial joint infections in children. Bone and joint infections rep-resented only 3% of all cases of invasive pneumococ-cal disease collected by the PMPSSG.15This is similar
to the data reported by Gray and Dillon14 and
Ja-cobs.21The average age of children in this report (17.6
months) is comparable to that for other pneumococ-cal infections reported from the PMPSSG.15 This
mean age is also comparable to previously published series of osteoarticular infections that include pneu-mococcal bone and joint infections1,2,22–24and slightly
older than the 11 months in the series reported by Jacobs.21 The specific bones and joints involved in
our patient population were distributed similarly to those previously reported in the literature; the femur and humerus the most often affected bones and the knee and hip the most commonly involved joints. The frequent association of septic arthritis with os-teomyelitis (50%) was also noted by Jacobs.21 The
high rate of bacteremia in our patients with osteo-myelitis (48%) and arthritis (43%) may represent the natural course of invasive infection with pneumococ-cus. However, the fact the most common site of pathogen isolation for children with osteomyelitis was the blood rather than bone, suggests the possi-bility of bias in case identification based on positive cultures, with overrepresentation of those children with osteomyelitis associated with bacteremia. The history of previous nonpenetrating trauma to an ex-tremity in 20% of children with osteomyelitis is con-sistent with the widely held concept of inoculation of injured tissues during bacteremia in the pathogene-sis of bone infections. Of interest was the fact that
10% of children in our report were hospitalized with-out localizing signs or symptoms of bone or joint infection, indicating that these infections should be considered in febrile children admitted to the hospi-tal with no apparent focus.
The serotypes of pneumococcus causing infection in our patients with osteomyelitis and septic arthritis were somewhat different from those causing infec-tion at other body sites in the PMPSSG group over-all.15 Types 6 and 19, which were the second and
third most prevalent strains isolated from all PSPSSG study patients, caused 57% of the cases of osteomy-elitis and 64% of cases of arthritis. The most preva-lent serotype of all isolates, regardless of site of iso-lation, in the PMPSSG group was type 14; however, none of the children with bone infection and only 2 of the 21 children with arthritis were infected by type 14 pneumococcus. The reasons for the apparent dif-ferences in serogroups of clinical isolates from bone and joint infections remain speculative.
Children and adults with underlying conditions represent up to 26% of those with invasive pneumo-coccal infections from other studies14,27and 27% of all
pneumococcal infections in PMPSSG patients.15 In
contrast only a single child in our series with a doc-umented bone or joint infection had a known under-lying immune-compromising condition other than age-dependent susceptibility. A poor response to polysaccharide antigens is well recognized in chil-dren,24 months of age. This immaturity leads to an increased incidence of pneumococcal infection in this age group compared with older children and adults.28 Immune deficiencies that have been
specif-ically reported to be associated with pneumococcal bone and joint infections include: splenic dysfunc-tion and/or humoral immune deficiencies caused by hemoglobinopathy29 and IgG subclass deficiency;30
neutrophil chemotactic deficiency;31and cellular
im-mune deficiency associated with bone marrow trans-plantation,32as was documented in 1 of our patients.
Associations have also been made between hemo-philia33,34 and prosthetic joints35 and pneumococcal
septic arthritis. Radiographic changes in the bone were apparent at the time of diagnosis in 70% of children with osteomyelitis, a somewhat higher fig-ure than the 36% reported by Jacobs.21 In all but 2
children with negative radiographs, however, a ra-dionuclide bone scan was diagnostic.
The mean duration of treatment of osteomyelitis and arthritis were 56.0 and 29.4 days, respectively. Only 63% of children with osteomyelitis and 41% of children with septic arthritis received sequential therapy with parenteral followed by oral therapy. The remaining children were treated with parenteral therapy exclusively. These differences may reflect the retrospective nature of the data collection and varying standards of practice at the different partic-ipating centers, taking into account issues other than the medical requirements of treatment. Surgical drainage of involved joints was performed in essen-tially all children, with drains left in place an average of 2 days before removal.
greater proportion of infections caused by PEN-NS organisms; however, this association did not reach statistical significance as it did for all isolates ana-lyzed in the PMPSSG study.15It is, however, of great
concern that 27% ofS pneumoniaeisolated from chil-dren without previous antibiotic therapy demon-strated decreased susceptibility to penicillin and 20% demonstrated decreased susceptibility to ceftriaxone. This clearly documents the high rates of antibiotic resistance in S pneumoniae in communities repre-sented by the PMPSSG.
Given the relatively small number of children in-fected by strains ofS pneumoniaethat were PEN-NS, we are not able to draw conclusions regarding the efficacy of antibiotic or surgical therapy in these children, although no microbiological failures were documented in the 14 children with osteomyelitis or septic arthritis caused by these strains. It is possible that the microbiological success in the treatment of children in this report is a function of both the sig-nificant antibiotic activity of penicillin and ceftriax-one against strains noted to have relative resistance to these antibiotics, as well as the excellent penetra-tion of the b-lactam antibiotics into bone and joint tissue with parenteral therapy. In combination, these two factors may result in bactericidal activity at the site of infection for at least 60% of the dosing interval, allowing for a microbiological cure.36 If b lactam
resistance continues to increase in S pneumoniae, or less active antibiotics are used in treatment, microbi-ological and clinical cures may not be achieved.
Sequelae of osteomyelitis occurred in 1 of 9 chil-dren infected by PEN-NS strains, compared with 3 of 12 infected by PEN-S strains. Furthermore, our anal-ysis of days of fever after the start of therapy, days of hospitalization, and sequelae in the children infected by PEN-NS strains compared with those infected by susceptible strains did not note any differences be-tween the two groups of children. Our findings are in contrast to those reported by Abbasi et al37 in 3
children with bone and joint infections caused by PEN-NS pneumococci. It is possible that the slow clinical response of 2 of their patients was related to the very high MICs to cefotaxime (6 mg/mL and 8
mg/mL) compared with the lower MICs of infecting organisms in our patients.
Nineteen percent of children with long bone osteo-myelitis demonstrated long-term sequelae. For chil-dren with involvement of the adjacent joint, the rate of sequelae was 30%. These rates are comparable to those previously summarized by Fink and Nelson6
for bone and joint infections primarily caused by Staphylococcus aureus, and to those cited by Jackson et al38 for children with arthritis adjacent to
osteomy-elitis. Given the retrospective nature of data collec-tion on these children, our stated rate of sequelae may actually underestimate the true rate. These data suggest that a more aggressive approach to diagnosis is needed, as the mean number of days of osteoar-ticular symptoms before hospitalization was 5.1 for children with bone infections and 2.2 for those with joint infections. Of particular interest was the obser-vation that the mean age of children with sequelae was significantly lower than the age of those without
sequelae (6.4 months vs 18.6 months). This observa-tion suggests that immunologic, anatomic, or clinical factors associated with young infancy may predis-pose to more destructive disease in this age group.
Pneumococcal bone and joint infections are an un-common complication of pneumococcal bacteremia. Assuming that;1% to 5% of children with bactere-mia caused by S pneumoniae develop meningitis,39
and that bone and joint infections were documented to occur with a frequency;20% of that of meningitis in the PMPSSG data set,15 bone and joint infections
seem to occur in;1 in 100 to 1 in 500 children with pneumococcal bacteremia. Because the serotypes causing these infections are represented in many of the new conjugate pneumococcal vaccines, the inci-dence of pneumococcal bone and joint infection should decrease dramatically after widespread rou-tine immunization of children.
ACKNOWLEDGMENTS
We wish to acknowledge financial support for the PMPSSG through Roche Laboratories, and for assistance with data collec-tion by Beverly Petrites and Joan Young (San Diego); Tracey Paris, Linda Lamberth, and Rebekah Lichenstein (Houston); Timothy Postula (Chicago); Susana Aragon (Los Angeles); Nancy C. Tucker (Little Rock); and Michele Ortenzo (Pittsburgh).
REFERENCES
1. Nelson JD, Koontz WC. Septic arthritis in infants and children: a review of 117 cases.Pediatrics. 1966;38:966 –971
2. Nelson JD. The bacterial etiology and antibiotic management of septic arthritis in infants and children.Pediatrics. 1972;50:437– 440
3. Gillespie R. Septic arthritis of childhood.Clin Orthop. 1973;96:152–159 4. Nade S. Choice of antibiotics in management of acute osteomyelitis and
acute septic arthritis in children.Arch Dis Child. 1977;52:679 – 682 5. Anderson JR, Orr JD, Maclean DA, Scobie WG. Acute haematogenous
osteitis.Arch Dis Child. 1980;55:953–957
6. Fink CJ, Nelson JD. Septic arthritis and osteomyelitis in children.Clin Rheum Dis. 1986;12:423– 435
7. Welkon CJ, Long SS, Fisher MC, Alburger PD. Pyogeic arthritis in infants and children: a review of 95 cases.Pediatr Infect Dis. 1986;5: 669 – 676
8. Herndon WA, Knauer S, Sullivan JA, Gross RH. Management of septic arthritis in children.J Pediatr Orthop. 1986;6:576 –578
9. Barton LL, Dunkle LM, Habib FH. Septic arthritis in childhood.Am J Dis Child.1987;141:898 –900
10. LaMont RL, Anderson PA, Dajani AS, Thirumoorthi MC. Acute hema-togenous osteomyelitis in children.J Pediatr Orthop. 1987;7:579 –583 11. Dich VQ, Nelson JD, Haltalin KC. Osteomyelitis in infants and children.
Am J Dis Child. 1975;129:1273–1278
12. Craigen MAC, Watters J, Hackett JS. The changing epidemiology of osteomyelitis in children.J Bone Joint Surg. 1992;74B:541–545 13. Unkila-Kallio L, Kallio MJT, Peltola H, and the Finnish Study Group.
Acute haematogenous osteomyelitis in children in Finland.Ann Med. 1993;25:545–549
14. Gray BM, Dillon HC. Clinical and epidemiologic studies of pneumo-coccal infection in children.Pediatr Infect Dis. 1986;5:201–207 15. Kaplan SL, Mason EO Jr, Barson WJ, et al. Three-year multicenter
surveillance of systemic pneumococcal infections in children.Pediatrics. 1998;102:538 –545
16. Tan T, The US Pediatric Multicenter Pneumococcal Surveillance Study Group. Clinical characteristics of children with pneumococcal pneumo-nia. Abstract No. 1102. Presented at the Annual Academic Societies Meeting (SPR/APS/APA); May 6 –10, 1996; Washington, DC 17. Arditi M, Mason EO Jr, Bradley JS, et al. Three-year multicenter
sur-veillance of pneumococcal meningitis in children: clinical characteris-tics, and outcomes related to penicillin susceptibility and dexametha-sone use.Pediatrics. 1998;102:1087–1097
18. National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Susceptibility Testing. Sixth informational sup-plement M1150 –56. Wayne, PA: National Committee for Clinical Lab-oratory Standards; 1995
mL) forStreptococcus spp. Table 2C. M100-S7. NCCLS Vol 17. No 2. 1997 20. Kauffman CA, Watanakunakorn C, Phair JP. Pneumococcal arthritis.
J Rheumatol. 1976;3:409 – 419
21. Jacobs NM. Pneumococcal osteomyelitis and arthritis in children.Am J Dis Child.1991;145:70 –74
22. Lakhani U. Pneumococcal osteomyelitis and arthritis in an infant.Conn Med. 1977;41:479 – 483
23. Chusid MJ, Sty JR. Pneumococcal arthritis and osteomyelitis in children. Clin Pediatr. 1981;20:105–107
24. Hadari I, Dagan R, Gedalia A, Jeaine J, Moses S. Pneumococcal osteomyelitis; an unusual cluster of cases.Clin Pediatr. 1985;24:143–145 25. Hellerstein A, Wiedermann BL. Pneumococcal sacroiliitis in an infant.
Pediatr Infect Dis J. 1987;6:759 –761
26. Pocheville I, Gutierrez C, Villas P, Noguerales F, Hernandez JL. Pneu-mococcal vertebral osteomyelitis: a clinical case.Pediatr Infect Dis J. 1995;14:160 –161
27. Burman LA, Norrby R, Trollfors B. Invasive pneumococcal infections: incidence, predisposing factors, and prognosis.Rev Infect Dis. 1985;7: 133–142
28. Bruyn GAW, Zegers BJM, van Furth R. Mechanisms of host defense against infection withStreptococcus pneumoniae.Clin Infect Dis. 1992;14: 251–262
29. Syrogiannopoulos GA, McCracken GH, Nelson JD. Osteoarticular in-fections in children with sickle cell disease.Pediatrics. 1986;78:1090 –1096 30. Gottsegen DN. Pneumococcal osteomyelitis associated with IgG2
sub-class deficiency.Pediatr Infect Dis J. 1987;6:281–284
31. Andersen BR, Mayer ME, Geiseler PJ, Niebel JP. Multi-joint pneumo-coccal pyarthrosis in a patient with a chemotactic defect.Arthritis Rheum. 1983;26:1160 –1162
32. Schwella N, Schwerdtfeger R, Schmidt-Wolf I, Schmid H, Siegert W. Pneumococcal arthritis after allogeneic bone marrow transplantation. Bone Marrow Transplant. 1993;12:165–166
33. Pappo AS, Buchanan GR, Johnson A. Septic arthritis in children with hemophilia.Am J Dis Child.1989;143:1226 –1228
34. Fajardo JE, Mickunas VH, deTriquet JM. Suppurative arthritis and hemophilia.Pediatr Infect Dis. 1986;5:593–594
35. Ryczak M, Sands M, Brown RB, Sklar JH. Pneumococcal arthritis in a prosthetic knee.Clin Orthop. 1987;224:224 –227
36. Craig WA. Interrelationship between pharmacokinetics and pharmaco-dynamics in determining dosage regimens for broad-spectrum cepha-losporins.Diagn Microbiol Infect Dis. 1995;22:89 –96
37. Abbasi S, Orlicek SL, Almohsen I, Luedtke G, English BK. Septic arthri-tis and osteomyeliarthri-tis caused by penicillin and cephalosporin-resistant Streptococcus pneumoniaein a children’s hospital.Pediatr Infect Dis J. 1996;15:78 – 83
38. Jackson MA, Burry VF, Olson LC. Pyogenic arthritis associated with adjacent osteomyelitis: identification of the sequela-prone child.Pediatr Infect Dis J. 1992;11:9 –13
39. Baraff LJ, Bass JW, Fleisher GR, et al. Practice guideline for the man-agement of infants and children 0 to 36 months of age with fever without source.Pediatrics. 1993;92:1–12
ELECTRONIC POSTING OF DISSERTATIONS PRODUCES PUBLISHING DILEMMAS
Virginia Tech’s mandate for online access raises questions about peer review, plagiarism, and journal editors’ policies.
Since January 1997, graduate students at Virginia Tech have faced an experience unlike any encountered by their peers in other universities. They must submit their master’s degree theses or doctoral dissertations in formats capable of being posted on the World Wide Web.
“What we’re doing is putting theses and dissertations in our library in an electronic format so that they can be found in a search,” explains John Eaton, Associate Vice Provost for Graduate Studies at Virginia Tech. “We’re trying to give our students access to tools that will show other scholars what they’ve found, and to find a way for scholars to access that information.”
Critics counter that the requirement to make theses and dissertations available online has several more or less severe perils. Mandated online publication of theses, they say, could prejudice graduate students’ chances of having work based on those theses published in scholarly journals. It could facilitate plagiarism. And it will preserve for electronic posterity dissertations that should better be left in obscurity as hardcopy dust-gatherers on library stacks.
Gwynne P.Scientist.1977;11(21)
DOI: 10.1542/peds.102.6.1376
1998;102;1376
Pediatrics
Pediatric Multicenter Pneumococcal Surveillance Study Group (PMPSSG)
Gordon E. Schutze, Ellen R. Wald, Laurence B. Givner, Edward O. Mason and The
John S. Bradley, Sheldon L. Kaplan, Tina Q. Tan, William J. Barson, Moshe Arditi,
Pediatric Pneumococcal Bone and Joint Infections
Services
Updated Information &
http://pediatrics.aappublications.org/content/102/6/1376
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/102/6/1376#BIBL
This article cites 36 articles, 8 of which you can access for free at:
Subspecialty Collections
skeletal_disorders_sub
http://www.aappublications.org/cgi/collection/rheumatology:musculo
Rheumatology/Musculoskeletal Disorders
http://www.aappublications.org/cgi/collection/pulmonology_sub
Pulmonology
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su
Infectious Disease
http://www.aappublications.org/cgi/collection/hospital_medicine_sub
Hospital Medicine
ev_sub
http://www.aappublications.org/cgi/collection/teaching_curriculum_d
Teaching/Curriculum Development
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.102.6.1376
1998;102;1376
Pediatrics
Pediatric Multicenter Pneumococcal Surveillance Study Group (PMPSSG)
Gordon E. Schutze, Ellen R. Wald, Laurence B. Givner, Edward O. Mason and The
John S. Bradley, Sheldon L. Kaplan, Tina Q. Tan, William J. Barson, Moshe Arditi,
Pediatric Pneumococcal Bone and Joint Infections
http://pediatrics.aappublications.org/content/102/6/1376
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.