Introduction. The first feasibility evaluation of the GemTax IV study using the novel therapeu-tic agent cetuximab, a chimaeric monoclonal antibody, which specifically targets the epidermal growth factor receptor and binds to the extracellular domain of the EGFR, preventing ligand binding and activation of the receptor was carried out. The objective was to assess the feasibility of cetuximab in combination with two common chemotherapeutic regimens in patients with locally advanced or metastatic non-small cell lung cancer. Early phase II results and updated results of the second interim analysis are presented in this article.
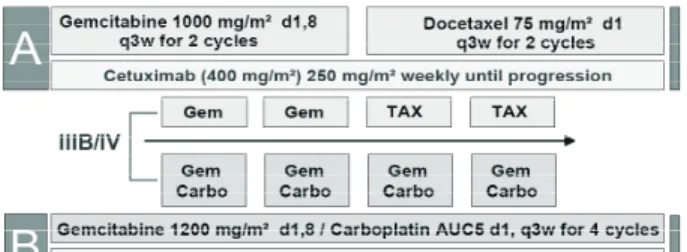
Materials and methods. In the period 2006–2008, 328 patients were enrolled at 23 centres in Germany and 1 centre (Institute of Oncology, Vilnius University) in Lithuania. 236 patients with histologically confirmed stage IIIB or IV non-small cell lung cancer, WHO performance status 0–2, and with no prior chemotherapy received cetuximab 400 mg/m2 as an initial dose,
then 250 mg/m² weekly either in combination with gemcitabine 1000 mg/m² on days 1 and 8 for two 3-weekly cycles followed by docetaxel 75 mg/m² on day 1 for 2 cycles (q3w) or gemcit-abine 1200 mg/m² on days 1 and 8 and carboplatin AUC5 on day 1 for a maximum of 4 cycles (q3w). Cetuximab was administered beyond these four cycles as maintenance therapy until dis-ease progression or unacceptable toxicity.
Results.142 patients assessable for toxicity received 404 cycles of cetuximab (1119 infu-sions) in combination with chemotherapy and 285 cycles (797 infuinfu-sions) of single-agent cetuxi-mab (maintenance phase). Clinically relevant toxicity is more common in the combinational treatment arm but in total not extraordinary. If therapeutic intervention was needed, there were 17 patients (14.5%) of 117 patients in Arm A and 30 patients (25.2%) of 119 patients in Arm B, respectively, resulting in a reduction to 60% of clinically relevant toxicity in Arm A in relation to Arm B. The haematological toxicities of CTC grade 3/4 indicate the treatment: the action of chemotherapy can be especially seen on day 8 and day 15. Serious adverse events (SAE’s) were officially reported, however, serious adverse events were more common in combination therapy. There were 209 SAE’s in this trial (the corresponding number of patients up to this date is 291): 98 in Arm A with some 4 duplicates: 94 SAE’s with a corresponding number of patients, 147 (study population) and 111 calls in Arm B with 2 duplicates → 109 calls with a corresponding patient number of 144 pts (study population), respectively. There were single agent cetuximab 177 cycles in arm A (33 patients), median 4 cycles per patient and mean 5.4 cycles per patient, 230 cycles in arm B (47 patients), median 3 cycles per patient and mean 4.9 cycles per patient. Overall survival is early for judgment.
Conclusion. Cetuximab does not add significantly to learn chemotherapy toxicity in the induction phase and is well tolerated in the maintenance phase.
Key words:advanced non-small cell lung cancer, chemotherapy, toxicity, feasibility
© lietuvos mokslų akademijos leidykla, 2008 © Vilniaus universitetas, 2008
Advanced non-small cell lung cancer treatment:
cetuximab treatment in a randomized phase II / III trial
in combination with gemcitabine or docetaxel or with
carboplatin / gemcitabine (GemTax IV).
A preliminary feasibility report on the first data
Saulius Cicėnas
1, 21 Institute of Oncology, Vilnius University,
Lithuania
2 Institute of Rehabilitation, Sport Medicine
and Nursing, Vilnius, Lithuania
correspondence to: Prof. Saulius cicėnas, department of Thoracic Surgery and Oncology, institute of Oncology, Vilnius university, Santariškių 1, lt-08660 Vilnius, lithuania. e-mail. [email protected]
INTRODUCTION
Lung cancer is the leading cause of cancer mortality with an-nual death rate of more than 1.1 million people worldwide (1). Globally, there are 850.000 lung cancer deaths in men per year (age standardized rate (ASR: 31.2) and 330.000 lung cancer deaths in women (ASR: 10.3). Lung cancer is the number one cause of cancer deaths causing approximately 18% of the total number of deaths. 8% of all the lung cancers at the time of di-agnosis are in advanced stage. A 5-year survival makes up5% of all the cases. Treatment of locally advanced and metastatic lung cancer is very difficult, and results are unsatisfactory.
For the treatment of patients with advanced non-small cell lung cancer (NSCLC) traditionally platinum-based doublet regimens are used for the first-line chemotherapy, as a stand-ard. But not all the patients – particularly those with stage IV disease and a performance status (PS) of 2 – will benefit (2). Docetaxel (D) and gemcitabine (G) are active, with relatively fa-vourable toxicity profiles as the first- or second-line treatment of advanced NSCLC (3–10), and are useful agents for treating patients who are unable to tolerate more toxic regimens (11). The novel therapeutic agent cetuximab, a chimaeric mono-clonal antibody, that specifically targets the epidermal growth factor receptor, is currently registered for colorectal and head and neck cancers and is undergoing broad clinical investiga-tions in advanced NSCLC. Table 1 shows the results of using Cetuximab in the first-line NSCLC treatment.
Before we started trial with GemTax IV, results of GemTax I, II and III were evaluated and conclusion was drawn that se-quencing of single agent chemotherapy is effective and well tolerated in patients with advanced NSCLC, weekly regiments with docetaxel (D) and gemcitabine (G) to be less feasible than 3-weekly regiments (GemTax II). Sequential chemotherapy with D and G is better tolerated than a standard combination regimen (G + D), with lower clinically relevant haematological toxicity. A phase II / III study to compare sequential single-agent therapy to a platinum based doublet has been initiated in GemTax IV trial.
In this randomized trial the feasibility of cetuximab in combination with two common chemotherapeutic regimens in patients with locally advanced or metastatic NSCLC is assessed
and phase II results are reported. The primary objectives were clinically relevant haematological toxicity (CRHT) and skin toxicity. The secondary objectives were overall survival (OS); time to progression (TTP); overall response rate (ORR); quality of life (QoL); additional medical resource requirements. MATERIALS AND METHODS
Between April 17, 2006 and September 9, 2008, 328 patients were enrolled in 23 centres in Germany and 1 centre (Institute of Oncology Vilnius University) in Lithuania. 236 patients were evaluablefor interim analysis. Patients and treatment: open-labelled randomized phase II / III multicentre study. The main inclusion criteria were:
– Histologically or cytologically proven stage III–IV non-resectable non-small cell lung cancer.
– Age ≥18 years.
– World Health Organization performance status 0–2. – ≥1 uni-dimensional target lesion(s).
– No prior chemotherapy or radiotherapy.
– No symptomatic / uncontrolled brain metastases or pe-ripheral neuropathy grade >2.
– Adequate haematological and biological function. Treatment administration:
CRHT was defined as a combined score of grade 3 / 4 thrombocytopenia + ≥1 platelet transfusion during the treat-ment cycle; or grade 3 / 4 anaemia + ≥1 blood transfusion; or febrile neutropenia + intravenous (IV) antibiotics, plus clini-cally relevant skin reactions (CTC grade 3 or 4 and need to dis-continue cetuximab treatment).
Table 1. Cetuximab: consistent results in the first-line non-small cell lung cancer (NSCLC)
RR (%) PFS (months) OS (months)
CT + Erbitux CT CT + Erbitux CT CT + Erbitux CT
LUCAS n = 86 Rosell et al. (2) Cis / vino 35 28 5 4.6 8.3 7.3 BMS-100 n = 133 Butts et al. (3) Platinum / gem 28 18 5.1 4.2 12 9.3 BMS-099 n = 676 Lynch et al. (4) Carbo / taxane 26 17 4.4* 4.3 4.2* 3.8 9.7 8.4 HR: 0.89 FLEX n = 1125 Pirker et al. (5) Cis / vino 36 29 4.8 4.8 11.3 10.1 HR: 0.87
Note. *PFS by Independent Radiological Review Committee (IRRC) / PFS by Investigator; RR – response rate; PFS – progression free survival; CT – computed tomography; OS – overall survival; HR – hazard ratio.
RESULTS
Tables 2 and 3 show the baseline patients’ characteristics. The clinically relevant toxicity is more common in the com-binational treatment arm but in total not extraordinary. Clini-cally relevant toxicity as defined in the protocol is shown in de-tail in the tables below. In summary, if therapeutic intervention was needed, there were 17 patients of 117 patients in Arm A and 30 patients out of 119 patients in Arm B, respectively, resulting in a reduction to 60% of clinically relevant toxicity in Arm A in relation to Arm B. Table 4 shows clinically relevant haemato-logical and skin toxicity for cycles 1–4.
The haematological toxicities of CTC grade 3 / 4 indicate the treatment: especially on day 8 and day 15 the action of chemo-therapy can be seen, details can be taken from Table 5.
Non-haematological toxicities (adverse events) beside skin toxicity were generally less frequent in Arm A than in Arm B.
Serious adverse events, as to be reported to the official insti-tutions, were more common to the combination therapy. From May 17, 2006 up to June 10, 2008, there were 209 SAE’s in this trial (corresponding patient number up to this date was 291 pa-tients): 98 in Arm A with some 4 duplicates → 94 SAE’s with a corresponding patient number of 147 patients (study popula-tion) and 111 calls in Arm B with 2 duplicates → 109 calls with a corresponding patient number of 144 patients (study popu-lation), respectively. Table 6 shows the proportion of patients: Arm A 48% (70 / 147); Arm B 49% (70 / 144).
Stratification of SEA’s can be seen in Table 7. In relation to the cetuximab treatment there are no differences between the study
Table 2. Baseline characteristics (demographics) Patient characteristics (n = 236) Single with cetuximab (n = 117) Doublet with cetuximab (n = 119) Total Gender Female 35 (30%) 30 (25%) 65 (28%) Male 82 (70%) 89 (75%) 117 (72%) WHO-PS* 0 46 (39%) 56 (47%) 102 (43%) 1 69 (59%) 58 (49%) 127 (54%) 2 2 (2%) 5 (4%) 7 (3%) Age Range 36–77 41–80 36–80 Median 64.0 64.0 64.0
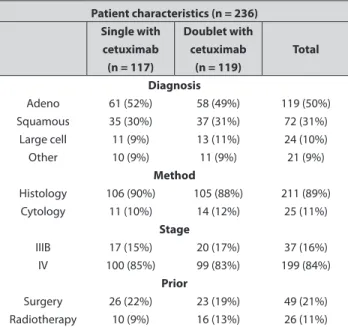
Table 3. Baseline characteristics (diagnosis)
Patient characteristics (n = 236) Single with cetuximab (n = 117) Doublet with cetuximab (n = 119) Total Diagnosis Adeno 61 (52%) 58 (49%) 119 (50%) Squamous 35 (30%) 37 (31%) 72 (31%) Large cell 11 (9%) 13 (11%) 24 (10%) Other 10 (9%) 11 (9%) 21 (9%) Method Histology 106 (90%) 105 (88%) 211 (89%) Cytology 11 (10%) 14 (12%) 25 (11%) Stage IIIB 17 (15%) 20 (17%) 37 (16%) IV 100 (85%) 99 (83%) 199 (84%) Prior Surgery 26 (22%) 23 (19%) 49 (21%) Radiotherapy 10 (9%) 16 (13%) 26 (11%)
Table 4. Clinically relevant haematological and skin toxicity for cycles 1–4 Clinically relevant toxicity cycle 1 (n = 225)
Single with cetuximab (n = 112) Doublet with cetuximab (n = 113) CTC grade 3 CTC grade4 CTC grade 3 CTC grade 4 Anaemia 1 – 2 1 Thrombocytopenia 1 – 3* 8 Febrile neutropenia 1 – 1 1
Skin rush acne 7 – 6 –
Patients 9 21
* one patient Grade 2
Clinically relevant toxicity cycle 2 (n = 172) Single with cetuximab (n = 82) Doublet with cetuximab (n = 90) CTC grade 3 CTC grade 4 CTC grade 3 CTC grade 4 Anaemia – – – – Thrombocytopenia – – – 4 Febrile neutropenia – – – –
Skin rush acne 1 – 3 –
Patients 1 6
Clinically relevant toxicity cycle 1 (n = 133) Single with cetuximab (n = 60) Doublet with cetuximab (n = 73) CTC grade 3 CTC grade 4 CTC grade 3 CTC grade 4 Anaemia – – 4 – Thrombocytopenia – – – 5 Febrile neutropenia 3 – – –
Skin rush acne 3 – 2 –
Patients 6 11
Clinically relevant toxicity cycle 1 (n = 111) Single with cetuximab (n = 45) Doublet with cetuximab (n = 66) CTC grade 3 CTC grade 4 CTC grade 3 CTC grade 4 Anaemia – – 3 – Thrombocytopenia – – – 4 Febrile neutropenia – – – –
Skin rush acne 3* – 2 –
Patients 3 8
arms, while in relation to chemotherapy a probable or certain re-lationship is more often seen in the combination treatment arm.
The number of single agent cetuximab cycles (3 applica-tions; weekly) following the chemotherapy phase in Arm A was 177 cycles for 33 patients with a median 4 cycles per patient and a mean of 5.4 cycles per patient. In Arm B the numbers were
230 cycles for 47 patients with a median of 3 cycles per patient and a mean of 4.9 cycles per patient (see Table 8).
Preliminary overall survival data show no statistically sig-nificant differences and are too early for judgment.
DISCUSSION
Over-expression of the EGFR is common in NSCLC. It occurs in up to 80% of tumours (12, 13), and has been shown to play a key role in processes linked to tumour growth and progression (13).
The EGFR antibody Erbitux (cetuximab) is the first tar-geted therapy to demonstrate a survival benefit in the 1st line treatment with NSCLC regardless of histology, when added to a standard platinum-based chemotherapy regimen. The recently presented pivotal phase III FLEX study assessed the efficacy and safety of Erbitux in combination with cisplatin and vinor-elbine (CT) in patients with advanced NSCLC (15). Overall sur-vival (OS) was significantly improved in the CT-Erbitux arm compared with CT (median 11.3 vs 10.1 months; hazard ratio (HR) 0.87, p = 0.044). Pre-specified analyses showed the sur-vival benefit across all the major subgroups including ECOG performance status, smoking status, histology, gender, age, and tumour stage. The major treatment group (84% of the intent-to-Table 5.Haematological toxicity for cycles 1–4
Haematological toxicities CTC grade 3 / 4; cycle 1 (n = 225) A: Single with Cetuximab (n = 112); B: Doublet with Cetuximab (n = 113)
Day 8 Day 15 Before next cycle
A: CTC 3/4 B: CTC 3/4 A: CTC 3/4 B: CTC 3/4 A: CTC 3/4 B: CTC 3/4
Haemoglobin – / – – / – – / – – / – – / 1 – / –
Leucocytes – / – 7 / – 1 / – 19 / 4 – / – 1 / –
Neutrophils – / – 5 / – 1 / – 15 / 6 – / – – / –
Platelets – / – – / – 3 / 1 16 / 14 – / – – / –
Haematological toxicities CTC grade 3 / 4; cycle 2 (n = 172) A: Single with Cetuximab (n = 82); B: Doublet with Cetuximab (n = 90)
Day 8 Day 15 Before next cycle
A: CTC 3/4 B: CTC 3/4 A: CTC 3/4 B: CTC 3/4 A: CTC 3/4 B: CTC 3/4
Haemoglobin – / – – / – 1 / – – / – – / – 1 / –
Leucocytes – / – 7 / – – / – 7 / – – / – – / –
Neutrophils – / – 6 / 1 – / – 11 / – – / – 1 / –
Platelets – / 1 – / – – / – 6 / 5 – / – – / –
Haematological toxicities CTC grade 3 / 4; cycle 3 (n = 133) A: Single with Cetuximab (n = 60); B: Doublet with Cetuximab (n = 73)
Day 8 Day 15 Before next cycle
A: CTC 3/4 B: CTC 3/4 A: CTC 3/4 B: CTC 3/4 A: CTC 3/4 B: CTC 3/4
Haemoglobin – / – 1 / – 1 / – 2 / – – / – – / –
Leucocytes 10 / 1 5 / – – / – 8 / 1 – / – – / –
Neutrophils 9 / 4 7 / – 1 / – 9 / 1 – / – 1 / –
Platelets – / – 2 / 1 – / – 12 / 6 – / – – / –
Haematological toxicities CTC grade 3 / 4; cycle 4 (n = 111) A: Single with Cetuximab (n = 45); B: Doublet with Cetuximab (n = 66)
Day 8 Day 15 Before next cycle
A: CTC 3/4 B: CTC 3/4 A: CTC 3/4 B: CTC 3/4 A: CTC 3/4 B: CTC 3/4
Haemoglobin – / – 1 / – – / – 5 / – – / – 1 / –
Leucocytes 6 / 1 4 / – – / – 5 / – – / – 1 / –
Neutrophils 4 / 7 5 / – 2 / – 5 / 2 – / – 3 / –
Platelets – / – – / 1 – / – 11 / 8 – / – 1 / 1
Table 6. Number of serious adverse events as to be reported to the official institutions SAE’s (patient n = 291) Single with Cetuximab (n = 144) Doublet with Cetuximab (n = 147) Total Number of
re-ports per patient
Total: 94 reports Total: 109 reports 203 1 52 44 96 2 13 16 29 3 4 8 12 4 1 1 2 5 0 1 1
treat population, n = 946) was Caucasian. This patient popula-tion showed a significant benefit in OS of 1.4 months (10.5 vs 9.1 months, HR 0.80, p = 0.003). Given the latest interest in ad-enocarcinoma, an analysis based on histology demonstrated a 1.7 months survival benefit for the Erbitux combination (12 vs 10.3 months, HR 0.81). A survival benefit was also seen in all additional histology findings.
The addition of Erbitux to standard chemotherapy regi-mens in the 1st line treatment of NSCLC has led to consistently improved efficacy. For example, in a recent phase II study, Butts et al. compared the addition of Erbitux to gemcitabine with cis-platin or carbocis-platin (16). Response rates (28% vs 18%), median progression-free survival (5.1 vs 4.2 months), and OS (12.0 vs 9.3 months) all favoured Erbitux plus chemotherapy vs chemo-therapy alone.
Erbitux in combination with standard platinum-based chemotherapy was well tolerated, with expected and manage-able side effects (14–17).
Cox regression analysis based on 789 patients from three randomized phase IItrials showed, that gender significantly influenced OS (overall survival) in the uni-varied analysis (p = 0.0085), but had less influence in the multivariate analysis (p = 0.07). Age, histology, tumour stage, extra-thoracic metastas-es, co-morbidities surgical and radiotherapy treatment were not prognostic of OS. Serum Hgb and LDH, WHO PS (performance status) and QoL (EORTC LC13) have prognostic value of OS in retrospective analysis of the GemTax I–III studies. In GemTax IV trial cetuximab does not add chemotherapy toxicity in the induc-tion phase and is well tolerated in the maintenance phase. Hae-matological toxicities of CTC grade ¾ appears especially on day 8 and day 15. Non-haematological toxicities beside skin toxicity were generally less frequent in Arm A than in Arm B.
CONCLUSION
Cetuximab does not add significantly to the known chemother-apy toxicity in the induction phase and is well tolerated in the maintenance phase.
GEMTAX – NSCLC – Cooperative Study Group: Lothar R. Pilz (Department of Biostatistics, German Cancer Research Centre, Heidelberg, Germany), Monika Serke (Lung Clinic of Hemer, Germany), Corinna Eschbach (Asklepios Clinic Harburg, Germany), Jürgen Fischer (Clinic Löwenstein, Lö-wenstein, Germany), Cornelius Kortsik (Sankt Hildegardis Hospital, Mainz, Germany), Christian Schumann (University Medical Centre, Ulm, Germany), Martin Steins (Thoraxklinik, Heidelberg, Germany), Christian Manegold (Heidelberg Uni-versity Medical Centre, Mannheim, Germany).
Received 20 november 2008 accepted 28 november 2008
References
1. Jemal a, Siegel R, Ward em, Thun mJ. cancer statistics, 2006. ca cancer J clin 2006; 56: 106–30.
2. Buccheri G, Ferrigno d. Prognostic factors in lung can-cer: tables and comments. eur Respir J 1994; 7: 1350–64. 3. Pfister dG, Johnson dH, azzoli cG et al. american
Soci-ety of clinical Oncology treatment of unresectable non-small-cell lung cancer guideline: update 2003. J clin On-col 2004; 22: 330–53.
Table 7. Specific serious adverse events as to be reported to the official institutions SAE’s (patient n = 291) Single with Cetuximab (n = 144) Doublet with Cetuximab (n = 147) Total Description and number of outcomes Total: 94 reports Total: 109 reports 203 Pneumonia 12 7 19 Fever 8 9 17 Thrombopenia – 15 15 Allergic reaction 3 9 12 Dyspnoea 7 3 10 Pain 7 3 10 Cardial 5 4 9 Hemopthysis 1 7 8 Death 3 4 7 Renal failure 4 3 7 Infection 3 3 6 Anaemia 1 4 5 Diarrhoea 4 1 5 Febrile neutropenia 5 – 5 Thrombosis 4 1 5 Others 27 36 63
Table 8.Number of single agent cetuximab cycles (3 applications; weekly) following chemotherapy, starting with the 5th cycle
Continuation therapy: cetuximab cycles Cetuximab following single therapy Cetuximab following combination therapy Total
Cycle number Number of
patients Number of patients
5 4 12 16 6 7 4 11 7 3 8 11 8 4 7 11 9 5 1 6 10 1 5 6 11 – 1 1 12 2 1 3 13 1 1 2 14 1 1 2 15 1 3 4 16 1 – 1 18 – 1 1 19 3 – 3 24 – 1 1 26 – 1 1 Total 33 47 80
4. anderson H, Hopwood P, Stephens RJet al. Gemcitabine plus best supportive care (BSc) versus BSc in inoperable non-small cell lung cancer in a randomised trial with quality of life as the primary outcome. Br J cancer 2000; 83: 447–53.
5. Fossella FV, deVore R, Kerr Rn et al. Randomized phase iii trial of docetaxel versus vinorelbine or ifosfamide in patients with advanced non-small-cell lung cancer pre-viously treated with platinum-containing chemotherapy regimens: the taX 320 non-Small cell lung cancer Study Group. J clin Oncol 2000; 18: 2354–62.
6. Georgoulias V, Papadakis e, alexopoulos a et al. Plati-num-based and non-platiPlati-num-based chemotherapy in advanced non-small-cell lung cancer: a randomised mul-ticentre trial. lancet 2001; 357: 1478–84.
7. Roszkowski K, Pluzanska a, Krzakowski m et al. a multi-center, randomized phase iii study of docetaxel plus best supportive care versus best supportive care in chemo-na-ive patients with metastatic or non-resectable localised non-small cell lung cancer (nSclc). lung cancer 2000; 27: 145–57.
8. manegold c, Pilz lR, Koschel G et al. Randomized mul-ticenter phase ii study of gemcitabine versus docetaxel as first-line therapy with second-line crossover in advanced-stage non-small-cell lung cancer. clin lung cancer 2005; 7: 208–14.
9. Shepherd Fa, dancey J, Ramlau Ret al. Prospective ran-domized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J clin Oncol 2000; 18: 2095–103.
10. Shepherd Fa, abratt RP, anderson H, Gatzemeier u, an-glin G, iglesias J. Gemcitabine in the treatment of elderly patients with advanced non-small cell lung cancer. Semin Oncol 1997; 24(Suppl 4): S50–S55.
11. manegold c, Thatcher n, Kortsik cet al.a phase ii / iii randomized study in advanced non-small cell lung can-cer (nSclc) with first line combination versus sequential gemcitabine (G) and docetaxel (d): update on quality of life (Qol), toxicity, and costs.J clin Oncol 2005; 23(16S): 7057.
12. Hirsch FR, Varella-Garcia m et al. epidermal Growth Factor Receptor in non–Small-cell lung carcinomas: correlation Between Gene copy number and Protein expression and impact on Prognosis. J clin Oncol 2003; 21: 3798–807.
13. Herbst RS, Shin dm.monoclonal antibodies to target epidermal growth factor receptor-positive tumors. a new paradigm for cancer therapy. cancer 2002; 94: 1593–611. 14. Pirker R, Szczesna a, von Pawel J et al. FleX: a
rand-omized, multicenter, phase iii study of cetuximab in combination with cisplatin / vinorelbine (cV) versus cV alone in the first-line treatment of patients with advanced non-small cell lung cancer (nSclc). J clin Oncol 2008; 26(15S): 3.
15. Butts ca, Bodkin d, middleman el et al. Randomized phase ii study of gemcitabine plus cisplatin or carboplatin [corrected], with or without cetuximab, as first-line
thera-py for patients with advanced or metastatic non small-cell lung cancer.J clin Oncol 2007; 25(36): 5777–84.
16. Rosell R, Robinet G, Szczesna a et al.Randomized phase ii study of cetuximab plus cisplatin / vinorelbine com-pared with cisplatin / vinorelbine alone as first-line ther-apy in eGFR-expressing advanced non-small-cell lung cancer. ann Oncol 2008; 19: 362–9.
17. lynch tJ, Patel t, dreisbach l et al. a randomised multicenter phase iii study of cetuximab (erbitux®) in comination with taxane / carboplatin versus tax-ane / carboplatin alone as first-line treatment for patients with advanced / metastatic non-small cell lung cancer (nSclc). J Thorac Oncol 2007; 2 (Suppl 4): S340–1. Saulius Cicėnas
IšpLITUSIO NESMULkIALąSTELINIO pLAUčIų vėžIO gyDyMAS:
RANDOMIzUOTAS II / III fAzėS TyRIMAS, kAI gyDyMAS
CETUkSIMAbU DERINAMAS SU gEMCITAbINU AR DOCETAkSELIU, ARbA SU kARbOpLATINA / gEMCITAbINU (gEMTAx Iv). TyRIMO TAIkyMO gALIMybėS IR ANkSTyvIEjI gyDyMO REzULTATAI S a n t r a u k a
Chimerinis monokloninis antikūnis cetuksimabas veikia epidermio augimo receptorių bei jungiasi su ekstraceliuliniu epidermio augimo domenu (baze), trukdydamas prisijungti ligandą ir aktyvindamas epidermio augimą.
Darbo tikslas. Įvertinti cetuksimabo, derinamo su dviem įprastais chemoterapijos preparatais, klinikinio taikymo galimybes ligoniams, sergantiems vietiškai išplitusiu ar metastaziniu nesmulkialąsteliniu plaučių vėžiu. Šiame straipsnyje pateikti atnaujinti ankstyvieji II fa-zės tyrimo rezultatai po tarpinės duomenų analifa-zės.
Tyrimo medžiaga ir metodai. Į šį tyrimą 2006–2008 m. buvo įtraukti 328 ligoniai, gydyti 23 centruose Vokietijoje ir Vilniaus uni-versiteto Onkologijos institute Lietuvoje. Anksčiau negydytiems 236 ligoniams, kuriems histologiškai buvo patvirtintas IIIB–IV stadijos nesmulkialąstelinis plaučių vėžys ir kurių būklė atitiko 0–2 balų pagal PSO skalę, iš pradžių skirta 400 mg/m2 cetuksimabo, vėliau
250 mg/m2 vieną savaitę kartu su gemcitabinu (1000 mg/m2) 1–8-ąją
dieną kas 3 savaites bei dviem kursais docetakselio (75 mg/m2) kas
3 savaites arba gemcitabino (1200 mg/m2) 1–8-ąją dieną ir
karbopla-tinos (AUC = 5) 1-ąją dieną (iki 4 kursų) kas 3 savaites. Po keturių chemoterapijos kursų cetuksimabas buvo lašinamas vienu ar kitu režimu kaip palaikomoji chemoterapija iki ligos progresavimo arba netoleruojamo toksiškumo.
Rezultatai. Chemoterapijos toksiškumas tirtas 142 ligoniams. Jiems buvo sulašinta 404 kursai cetuksimabo (1 119 infuzijų) kartu su 285 kursais chemoterapijos (797 infuzijos) ir palaikomąja cetuk-simabo doze. Kompleksinio gydymo grupės ligoniai pasižymėjo di-desniu kliniškai svarbiu toksiškumu, bet jie šį toksiškumą toleravo. Papildomo gydymo prireikė 17 asmenų (14,5%) iš 117 A grupės ligo-nių ir 30 asmenų (25,2%) iš 119 B grupės ligoligo-nių. Po gydymo A gru-pėje toksiškumas sumažėjo 60% atvejų, lyginant su B grupe. Dėl III° ir IV° (pagal CTC skalę) hematologinio toksiškumo papildomo gydymo ypač prireikė 8-ąją ir 15-ąją chemoterapijos dieną. Sunkūs nepageidaujami reiškiniai dažniausiai užregistruoti kompleksinio gydymo grupėje. 291 ligoniui nustatyti 209 reiškiniai: 98 A grupėje, iš jų 4 pakartotinai. Kiti 94 reiškiniai buvo užregistruoti 147
ligo-niams – 111 B grupėje, iš kurių 2 pakartotinai. 144 ligoligo-niams buvo registruoti 109 nepageidaujami reiškiniai. Palaikomasis gydymas cetuksimabu taikytas 33 A grupės ligoniams, iš viso – 177 kursai, vidutiniškai – 4 kursai vienam ligoniui (vidurkis – 5,4 kurso ligoniui); 47 B grupės ligoniams, iš viso – 230 kursai, vidutiniškai – 3 kursai ligoniui (vidurkis – 4,9 kurso ligoniui). Bendrojo išgyvenamumo re-zultatai bus paskelbti vėliau.
Išvada. Įvairiais chemoterapijos režimais skiriamas cetuksima-bas nedidina jau žinomo chemoterapinio toksiškumo ir gerai toleruo-jamas palaikomojo gydymo metu.
Raktažodžiai:išplitęs nesmulkialąstelinis plaučių vėžys, chemote-rapija, toksiškumas, tyrimo taikymo galimybės