Scoping exercise with Black and
minority ethnic groups on perceptions
of mental wellbeing in Scotland
Final Report
August 2008
Karen Newbigging
Dr. Manjit Bola
Professor Ajit Shah
Institute for Philosophy, Diversity and Mental
Health, Centre for Ethnicity and Health
Published by NHS Health Scotland,
The opinions expressed in this publication are those of the author/s and do not necessarily reflect those of Health Scotland.
Contents
Acknowledgements ...vi
Abbreviations ...vii
Executive Summary...viii
1. Introduction ...1
1.1 A note on terminology ...1
2. Background ...2
2.1 Policy background ...2
2.2 Background to the development of the project...4
2.3 Chinese and Pakistani communities in Scotland...4
2.3.1 Chinese communities in Scotland ...5
2.3.2 Pakistani communities in Scotland...6
3. Conceptualising mental wellbeing ...7
3.1 The relationship between mental wellbeing and mental illness ...7
3.2 Elements of mental wellbeing ...8
3.3 Enhancing mental wellbeing ...9
3.4 Cultural and ethnic differences in the conceptualisation of mental wellbeing...9
4. Method ...10
4.1 Aims and objectives of the scoping excercise...10
4.2 Involving stakeholders ...10
4.3 Methodology...11
4.3.1 Literature review ...11
4.3.2 Consultation with community informants...14
4.3.3 Synthesis ...17
4.3.4 Ethical considerations ...17
4.4 Exploration of the relevant methodology literature ...17
4.5 Limitations ...18
5. Review of the literature...19
5.1 Overview of the material identified ...19
5.1.1 Breakdown by country ...19
5.1.2 Participants ...20
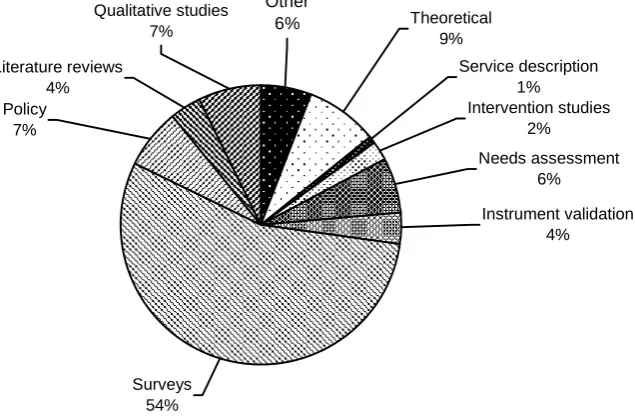
5.1.3 Type of material ...21
5.2 UK material ...22
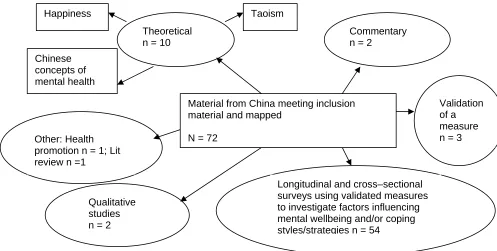
5.3 Material from China...25
5.4 Material from Pakistan ...26
5.5 Non-UK English speaking countries ...26
5.5.1 United States and Canada ...26
5.5.2 Australia and New Zealand ...26
5.6 Other European countries ...27
5.7 Cross-cultural comparisons...27
5. 8 Qualitative studies ...29
6. Chinese communities ...30
6.1 Language and key terms used to describe mental wellbeing ...30
6.1.1 Findings from the literature review ...30
6.1.2 Findings from interviews with community informants ...30
6.2 Conceptualisations of mental wellbeing ...30
6.2.1 Findings from the literature review ...30
6.2.2 Findings from interviews with community informants ...35
6.3 Factors influencing conceptualisations of mental wellbeing...36
6.3.1 Findings from the literature review ...36
6.3.2 Findings from interviews with community informants ...37
6.4 Factors influencing mental wellbeing ...39
6.4.1 Findings from the literature review ...39
6.4.2 Findings from interviews with community informants ...40
6.5 Improving mental wellbeing ...42
6.5.1 Findings from the literature review ...42
6.5.2 Findings from interviews with community informants ...42
7. Pakistani communities ...44
7.1 Language and key terms used to describe mental wellbeing ...44
7.1.1 Findings from the literature review ...44
7.1.2 Findings from interviews with community informants ...45
7.2 Conceptualisations of mental wellbeing ...46
7.2.1 Findings from the literature review ...46
7.2.2 Findings from the interviews with community informants ...46
7.3 Factors influencing conceptualisations of mental wellbeing...48
7.3.1 Findings from the literature review ...48
7.3.2 Findings from interviews with community informants ...48
7.4 Factors influencing mental wellbeing ...48
7.4.1 Findings from the literature review ...48
7.4.2 Findings from interviews with community informants ...49
7.5 Improving mental wellbeing ...51
7.5.1 Findings from the literature review ...51
7.5.2 Findings from interviews with community informants ...53
8. Comparison with the majority populations living in Scotland ...55
8.1 Literature review ...55
8.2 Findings from interviews with community informants ...56
9. Synthesis ...57
9.1 Conceptualisations of mental wellbeing ...57
9.2 Factors influencing conceptualisations of mental wellbeing...58
9.3 Promoting mental wellbeing ...59
10. Methods for future research...60
10.1 Methodological issues in relation to this review...60
10.1.1 Issues arising from the literature review...60
10.1.2 Issues arising from the fieldwork...61
10.2 Methods identified from the literature review...63
10.3 Rapid appraisal of methods literature ...65
11. Discussion ...67
11.1 Theoretical implications ...67
11.1.1 Relationship between mental wellbeing and mental health problems/illness ...67
11.1.2 Cultural beliefs and wellbeing ...67
11.1.3 Conceptual equivalence...68
11.1.4 Diversity of Chinese and Pakistani communities...69
11.2 Methodological implications ...69
11.3 Implications for policy and practice ...70
12. Implications for Phase 2 ...71
13. Conclusion...72
References ...73
Appendix 1: Technical appendix for literature review ...80
Appendix 2: Briefing Sheet ...90
Appendix 3: Topic guide for individual and group interviews ...92
Appendix 4: Overview of search results...94
Appendix 5: Bibliography of results of literature review...95
Appendix 6: Summary of UK material- systematic inquiry ...103
Appendix 7: Language and terms used ...111
Appendix 8: Annotated bibliography of methodological literature ...112
Acknowledgements
We would like to thank all those who participated in this research and gave of their time freely to share their views and help organise aspects of the research. We are grateful to Joanna Teuton, NHS Health Scotland, Dale Meller at the National Resource Centre for Ethnic Minority Health (NRCEMH) for their ongoing support and to Stuart Anderson and Margaret Didcock, from NHS Health Scotland Library for help in accessing additional research material. We would also like to thank members of the Steering Group, as below, for their guidance and helpful insights. As always our work has been supported by colleagues in the Centre for Ethnicity and Health and we would particularly like to thank Ravi Bola, Pam Howard, Samena Rashid and Marian Lawrenson.
Steering Group Membership
vi
Name Organisation Role
Joanna Teuton /Wendy Hearty (Chair)
NHS Health Scotland Public Health Advisor (Mental Health and Wellbeing)
Emma Hogg NHS Health Scotland Programme Manager (Mental Health
Improvement ) Dale Meller NHS Health Scotland
Formerly National Resource Centre for Ethnic Minority Health
Programme Manager (Mental Health & Race Equality)
Formerly Mental Health Project Manager
Jane Parkinson NHS Health Scotland Public Health Advisor (Mental Health Indicators) Trevor Lakey Greater Glasgow and
Clyde NHS Board
Head of Inequalities and Health Improvement Mental Health Partnership Lee Knifton Mental Health Foundation
Formerly Greater Glasgow and Clyde NHS Board
Associate Head of
Programmes for Scotland Formerly Senior Health Improvement Officer Akin Fatunmbi Health in Mind Service Manager, Men in
Mind
Abbreviations
BME Black and minority ethnic CHI Chinese Happiness Inventory GHQ General Health Questionnaire NHS National Health Service
NIMHE National Institute for Mental Health England
NRCEMH National Resource Centre for Ethnic Minority Health NSF National Service Framework
OHI Oxford Happiness Inventory PAR Participatory Action Research SCIE Social Care Institute for Excellence
SWB Subjective Wellbeing
UCLan University of Central Lancashire
UK United Kingdom
US and USA United States of America
WEMWBS Warwick-Edinburgh Mental Wellbeing Scale WHO World Health Organisation
Executive Summary
Background
1. The Scottish Government has made a commitment to improving public mental health as part of a wider agenda on health improvement. This includes work on promoting mental wellbeing in addition to work on the prevention of mental health problems and recovery.
2. This project was commissioned by NHS Health Scotland to add to the knowledge base in relation to the conceptualisations of mental wellbeing by Black and minority ethnic communities (BME) in order, ultimately, to provide mental health improvement guidance in relation to BME communities. The project has focused on Chinese and Pakistani communities, the largest BME communities in Scotland
3. This report provides an overview of the method and the main findings of this scoping exercise, which forms phase one of a project. The theoretical, methodological, policy and practice implications are explored and recommendations are made for future work in this area.
Method
4. The broad research question that guided this project asked how do Chinese and Pakistani communities living in Scotland conceptualise mental wellbeing and what are the implications of this for mental health promotion strategies?
5. The scoping exercise involved:
• reviewing the literature on mental wellbeing and Chinese and Pakistani communities
• interviews with key informants from community organisations working with Chinese and Pakistani communities in Scotland. Nearly all the people interviewed were also from these communities
• a brief review of the literature to identify the methods for undertaking research in this area of inquiry with Chinese and Pakistani
communities.
Findings
6. In total over 5,000 papers were initially identified for the literature review but only 140 were found to be relevant to this area of inquiry. This included 32 from the UK and 108 from China, Pakistan, USA, Canada, Australia, New Zealand and Europe. Just over half of the non-UK papers came from China and the majority of the material from non-UK English speaking countries related to Chinese communities, with only 5% from Pakistan. However there were more papers relating to Pakistani communities in the UK and they made up 50% of the total UK papers compared with 28% for
Chinese communities; the remainder relating to Asian or BME communities in general but inclusive of Chinese and Pakistani communities.
7. None of the UK papers directly answered the research question in any depth. By contrast the wealth of material from China provided rich insights into conceptualisations of mental wellbeing in different parts of China. This material included cross-sectional and longitudinal surveys that explored a broad range of factors and their relationship to mental wellbeing. These studies used measures of mental wellbeing, often validated on US populations and developed for use with Chinese populations. A small number of theoretical papers provided a useful exploration of philosophical influences, particularly Confucianism and Taoism, on conceptualisations of mental wellbeing and happiness. Papers relating to Pakistani Muslim communities, mainly from the UK, highlighted the central role of Islam in understanding and contributing to maintaining mental wellbeing.
8. From the interviews and the literature review, happiness emerges as the most widely used term to describe mental wellbeing for Chinese communities and the concept of a peaceful mind seemed to be most widely used within Pakistani communities. It was also apparent that these conceptualisations of mental wellbeing are rooted in philosophical and religious values, often described by community informants as cultural values. For Chinese communities, Confucianism and Taoism were identified, particularly in the literature from China, as major and not necessarily complementary influences. For Pakistani communities, the importance of faith was confirmed by community informants.
9. For both communities, conceptualisations of wellbeing have a number of dimensions, which appear to be inextricably linked – family wellbeing, spiritual wellbeing and material wellbeing with both communities placing an emphasis on social roles and connectedness. Further the way in which mental illness was conceptualised by both communities has an influence on how mental wellbeing was conceptualised. In general community informants viewed mental wellbeing as incompatible with mental illness, with mental illness defined in terms of severe mental illness and with more common mental health problems viewed as part of life.
10. Philosophical and religious beliefs emerge as the most significant influence on conceptualisations of mental wellbeing, even for younger people who have received a Western education. However age, generation, ethnic identity, cultural orientation and context were also important. There was a hint from both the literature review and the interviews that people may hold more than one frame of reference for conceptualising mental wellbeing.
11. There were relatively few papers in the literature review that related to specific strategies used by Chinese and Pakistani communities to maintain mental wellbeing and prevent mental illness although a number of papers relating to policy, or good practice in mental health promotion for these
communities were identified. The interviews with the community informants identified the role of religion and faith, activity and social networks and the importance of awareness raising in relation to mental health problems.
12. Whilst no direct comparisons could be drawn between Chinese and Pakistani communities and the majority community in Scotland, it was evident from studies elsewhere that the conceptualisations of mental wellbeing may differ fundamentally from those developed with majority populations. In particular it is suggested that terms and concepts used in mental wellbeing research in the West may not be as relevant or have a profoundly different meaning in these communities.
13. The indication from a rapid review of the literature is that participatory action research using qualitative methods provides the most promising way of developing a richer understanding of the meaning of mental wellbeing for Black and minority ethnic communities. Participatory action research aims to address inequalities between researchers and participants found in a traditional model of research and is well suited to identifying practical action that needs to be taken.
Recommendations
14. A wealth of data has been generated through this scoping exercise and further analysis of the literature and the interview data is recommended. The focus of this should be a more in-depth analysis of the factors influencing conceptualisations of mental wellbeing and the points of convergence and divergence within Chinese and Pakistani and with majority communities in Scotland and other English-speaking countries. 15. As the literature review identified a significant gap in the knowledge base
in terms of qualitative studies exploring meaning of mental wellbeing within Chinese and Pakistani communities it is recommended that this should be a priority for further research. Strategies for sampling and methods for facilitating discussion of the issues are discussed in the report.
16. This scoping phase also identified that tremendous potential exists within Chinese and Pakistani community organisations to build on this initial scoping exercise. The authors recommend investment in Black and minority ethnic organisations in Scotland to support capacity building, providing them with the training and resources to take this agenda forward.
1. Introduction
The strategic emphasis on public mental health forms part of Scottish Government’s wider agenda for a Healthier Scotland, with the “goal of less ill-health and higher levels of wellbeing and fitness across the nation and social spectrum” (Scottish Executive, 1998, Ch 4). There is a clear recognition that if the public mental health agenda is to be thoroughly pursued this needs to include a focus on mental wellbeing. This project has been commissioned by NHS Health Scotland as a means of extending the knowledge base about mental wellbeing in Black and minority ethnic (BME) communities in order, ultimately, to provide mental health improvement guidance in relation to BME communities.
It is self-evident that mental wellbeing is likely to be understood differently by diverse communities. This project has scoped the conceptualisations of mental wellbeing by Chinese and Pakistani communities, i.e. the majority BME communities, living in Scotland. It is intended as Phase 1 of a more comprehensive piece of work and has involved a rapid appraisal of the literature and initial fieldwork with community workers in Scotland undertaken between November 2007 and February 2008. The implications for subsequent research are drawn out in the final section.
The work has been undertaken by the Institute for Philosophy, Diversity and Mental Health in the Centre for Ethnicity and Health at the University of Central Lancashire (UCLan). The Centre has an established national and international reputation for engaging service users, carers and communities as equal partners in research and service development.
1.1 A note on terminology
The concept of mental wellbeing is complex, interpreted differently and continues to be debated (Friedli, 2006) and Section 3 provides a discussion of the term. The term positive mental health is also used to refer to the concept of mental wellbeing by other authors and both terms “encompass more than the absence of mental health problems and cover both experience and functioning” (Parkinson 2007, p.15). The starting point for this review has been a broad and inclusive approach to definition so as not to preclude important aspects of the concept. The term mental wellbeing is therefore used within this report to refer to a subjective sense of emotional, psychological, social and/or spiritual wellbeing and includes life satisfaction, positive relationships with others and a purpose in life (Parkinson, 2007). As well as positive mental health, the terms subjective wellbeing, psychological wellbeing and emotional wellbeing are also used but tend to be used to refer to specific elements of the overall concept of mental wellbeing, as discussed in Section 3. The term mental health is used in this report as an umbrella term to refer to mental health problems, diagnosable mental illness and mental wellbeing (i.e. positive mental health) whilst the term wellbeing is also used as an umbrella term to refer to physical wellbeing and mental wellbeing.
The term mental health improvement is used to refer to any action to increase mental health amongst individuals and populations. This includes action to strengthen mental wellbeing and/or action to prevent mental illness. A fuller exploration of the terms mental health, mental wellbeing, mental health improvement and mental illness is provided by Friedli (2006).
The other terminology that is debated and can be misleading relates to the definition of ethnicity. Where possible the descriptors Chinese or Pakistani have been used and generic terms avoided. However this had not always been possible and it is therefore worth noting that the term Asian is used differently in US and Australian contexts (likely to refer to people from China or East Asia) and the UK where it is used to refer to people from Pakistan, India or Bangladesh (i.e. South Asia). The terms Western and Eastern have been used, again reflecting their use in the literature and in particular used to distinguish belief systems and values and their origin.
2. Background
2.1 Policy background
The current strategic direction for mental health improvement or public mental health has evolved from a number of policy areas including: mental health, public health, social justice and social inclusion, education, enterprise and life long learning and arts, sports and culture. Public health policy in Scotland has increasingly identified mental health as an integral part of the wider agenda for health improvement (Scottish Executive, 1998). It forms part of the Scottish Government’s ambitions for wider health and wellbeing and is integral to addressing health and social inequalities (Scottish Government, 2008a). Forty-five national indicators have been developed to enable the Government to identify the extent to which its overall strategic objectives are being achieved. One of these indicators is concerned with improving the mental wellbeing of the Scottish population by 2011 (Scottish Government, 2008b).
Scottish Government policy on mental health integrates mental health improvement (i.e. promotion, prevention and support) and care and treatment (i.e. implementation of mental health legislation and mental health services) within the Scottish Government Health and Wellbeing portfolio. In 2000 a framework for further improvements in health and health services was established and included a commitment to a national anti-stigma campaign, the promotion of positive mental health and a national framework to reduce suicides in Scotland (Scottish Executive, 2000a). Further emphasis on the importance of continuing efforts in these areas was given in 2003 (Scottish Executive, 2003a) and a subsequent framework for action for health improvement in Scotland included a commitment to establishing a 3 year action plan for the National Programme for Improving Mental Health and Well-being between 2003-2006 (Scottish Executive, 2003b). This was extended into a second phase (2006-2008) with underpinning resources from the Scottish Executive Health Improvement Fund. Further information on the Scottish Government’s mental health improvement work can be found at www.wellscotland.info.
The discussion document, Towards a Mentally Flourishing Scotland, was published for consultation in October 2007, outlining a proposed future direction for mental health improvement and population mental health for 2008-2011 (Scottish Government, 2007). This discussion document draws attention to the debate about defining mental health and wellbeing, the underlying causes of mental health problems and the best ways of maintaining and improving mental health and wellbeing. It frames mental wellbeing in terms of three dimensions - emotional, social and psychological wellbeing, which includes:
“our ability to cope with life’s problems and make the most of life’s opportunities, to cope in the face of adversity and to flourish in all our environments; to feel good and function well, both individually and
collectively.”
(Scottish Government, 2007, p.2) The model underpinning this and outlined in the discussion document is the dual continua model, discussed in Section 3 of the current report. The document proposes taking forward action on three themes:
• promoting and improving mental health through a focus on increasing key protective factors and reducing key risk factors
• preventing mental health problems, mental illness, co-morbidity and suicide with a focus on key risk factors and protective factors
• supporting improvements in the quality of life, social inclusion, health, equality and recovery of people who experience mental illness.
It proposes that targeted groups for local and national action could include amongst others, people without access to key assets and resources and people and groups who experience discrimination, including racism. This is a clear reference to people from Scotland’s diverse BME communities and the analysis of the consultation responses confirms the need for a targeted approach to mental health improvement with these communities (Griesback, 2008).
In Scotland, the framework for race equality across health services is driven by the Race Relations Amendment Act of 2000, the Equalities Strategy (Scottish Executive, 2000) and the subsequent Fair for All policy driver (Scottish Executive, 2001) and subsequent guidance (Scottish Executive, 2002) directing the NHS in Scotland. The legislation and policy provides a baseline on race equality practice and clear guidance to NHS boards on mainstreaming race equality. These policies directly led to the establishment of the National Resource Centre for Ethnic Minority Health (NRCEMH) in 20021. The National Programme for the Improvement of Mental Health and
1
In April 2008 NRCEMH along with the other organisations representing the equality ‘strands’ identified by the Fair for All policy driver joined together to form a single Equalities and Planning Directorate within NHS Health Scotland. The mental health and race equality programme formerly hosted by NRCEMH is now also part of the Equalities and Planning Directorate.
Wellbeing funded a specific mental health programme within NRCEMH which sought to strategically influence and improve the mental health and wellbeing of BME communities (Meller, 2007). This research brief clearly relates to this programme of work as part of a broader portfolio of mental health improvement work within NHS Health Scotland.
2.2 Background to the development of the project
The development of this scoping exercise looking at perceptions of mental wellbeing in Black and minority ethnic (BME) communities developed in response to a number of key issues.
There is growing international recognition of the benefits of addressing mental wellbeing and its role in protecting and promoting mental health as part of a comprehensive approach to mental health improvement, as evidenced in The Helsinki Declaration signed by member states in Europe in 2005 (WHO, 2005). In line with this, national policy in mental health improvement in Scotland places a strong emphasis on promoting mental wellbeing in addition to the work on prevention of mental health problems and recovery.
The national work on mental health amongst BME communities in Scotland, developed by NRCEMH has a strong focus on service delivery and recovery and recognised that there was a gap in the research and practice in relation to mental wellbeing. NHS Health Scotland also identified a clear need for guidance for practitioners on promoting mental wellbeing within BME communities.
Given the lack of research on perceptions of mental wellbeing amongst BME communities generally and more specifically in Scotland, NHS Health Scotland’s NRCEMH and Mental Health improvement Programme, agreed that there was a need to develop a research programme to increase the knowledge base in this area. Due to the complexity of the area, any research needed to generate a good quality, meaningful output which was of practical value to stakeholders.
The first stage in the process was commissioning a scoping project which would provide an overview of the current level of knowledge and understanding about mental wellbeing in BME communities in Scotland. This research project forms part of a portfolio of mental health improvement work. It was anticipated that this scoping exercise would help inform the development of more substantive research addressing relevant questions around mental wellbeing amongst BME communities in Scotland and ultimately informing culturally sensitive mental health improvement work to be carried out in Scotland.
2.3 Chinese and Pakistani communities in Scotland
Analysis of the 2001 census data indicates that the minority ethnic population compromises just over 100,000, or 2% of the population (Scottish Executive, 2004). This is likely to be an underestimate as there has since been continued
arrival of refugees, asylum seekers and migrant workers from the European Union. Based on the 2001 Census figures, the Pakistani community is the largest BME group in Scotland, followed by Chinese, Indians and those of mixed backgrounds. In 2001, 31% of the Scottish BME population lived in Glasgow making up 5.5% of Glasgow’s total population, 4% in Edinburgh, 3.9% in Renfrewshire, 3.5% in Dundee and just fewer than 3 % in Aberdeen and East Dunbartonshire. In general, BME communities have a younger population profile than the majority community with 60% of Pakistani communities and 52% of Chinese communities under the age of 29 compared with 12% and 15% over the age of 50 respectively (Scottish Executive, 2004). Information from the Census also indicates that in most urban areas the largest ethnic minority is Pakistani, but that in rural areas such as Ayrshire and Arran, the Borders, Grampian and Dumfries and Galloway, the Chinese community is larger. The majority of people from Pakistani communities were either born in Scotland (47.4%) or Pakistan (36.7%) whilst the majority of people from Chinese communities were born in the Far East, excluding China (44.9%) or Scotland (29.7%) compared with 18% born in China.
2.3.1 Chinese communities in Scotland
Chinese people living In Scotland are a heterogeneous community and include people born in Britain (British Born Chinese-BBC), Hong Kong, Taiwan and mainland China and speak different languages including Cantonese, Mandarin and Hakka (Dobbie & Lee, 2004). The first Chinese people arrived in Scotland as a result of Scotland’s colonial activities in China. Chinese seamen hired as cheap labour became stranded in Scottish ports and they became part of the Lascar communities, which developed in dock areas throughout Scotland.2 Dorothy Neoh (2005) provides a useful overview of the migration of Chinese people to Scotland and their experience. The first settled Chinese community developed in Glasgow in 1960. The collapse of the agricultural economy in the People’s Republic in China in 1949, coupled with economic prosperity in Britain in the 1950s led to the first major wave of immigration from Hong Kong and the rural New Territories. The catering business developed and expanded and people from urban areas of Hong Kong and the nearby island of Apu Chau followed. Further migration occurred in the 1990s as Hong Kong reverted to Chinese control in 1997. Education has also been a driver for migration, particularly as China’s market economy has expanded and created a need for education and training overseas. There has also been migration from Taiwan with the opening of the Taiwanese manufacturing plants in Renfrewshire, South Lanarkshire and West Lothian. Marriage to Scottish men has been part of the pattern of settlement for Chinese women. The asylum dispersal system has led to Chinese men from Canton and Fijian seeking employment in the catering and retail sectors in Glasgow and Edinburgh.
Neoh (2005) describes how the notion of ‘family’ supported the survival of Chinese migrants in their chosen place of settlement. Family reunion and business opportunities, which were mainly family run, have led to Chinese communities being spread across Scotland. The lack of concentration of
2
http://www.scotlandagainstracism.com/onescotland/61.1.21.html
these communities, particularly in rural areas has contributed to social incohesion and exclusion (Neoh, 2005). Social exclusion has further been compounded by language, culture, racism and social isolation. This is particularly the case for early migrants who came from rural areas such as the New Territories compared with later migrants who had a better education and therefore found it easier to integrate and learn about the host community (Neoh, 2005). Neoh writes that the process of integration is not an easy one and identifies the conflict between Chinese values of family, respect for authority, harmony, dependency and conservatism and those derived from a Western education, including individuality, independent thinking, equality, justice and liberalism as a source of intergenerational conflict and confusion in terms of identity for Scottish-born Chinese people. She goes on to describe the multi-layered and evolving identity for Chinese people in Scotland, particularly second and third generations who face challenges associated with experience of tensions between majority and minority cultures.
In contrast with the Pakistani community, Chinese people in Scotland do not have a single shared religion but do ascribe to Confucian ideals and principles, which Neoh indicates could be seen as part of the Chinese cultural identity. As well as Confucianism, Taoism and Buddhism are followed by Chinese people and there is a revival of interest in religious practices among the older generation following the establishment of small Buddhist and Taoist temples that have connections with religious communities in Manchester and London (Neoh, 2005). Furthermore, Christianity is also followed and there are now several Chinese Christian churches in Scotland, which are attended by Chinese people of different generations.
2.3.2 Pakistani communities in Scotland
The majority of people from Pakistan migrated to Scotland after 1945. However migration from India to Scotland began during the 18th century also as a consequence of Scotland’s colonial involvement. These early migrants formed the Lascar colonies and went on to develop the social structures that subsequently assisted later migrants.3 By 1920, people had begun to settle and small communities developed initially in Glasgow and Edinburgh, with the majority of these people coming from the area of India that formed Pakistan in 19484. These communities developed further in the 1950s and 60s, particularly as industries faced labour shortages and Pakistani migrants were employed often in low paid jobs in factories, mills and in public transport. However the experience of racism in the labour force led many to establish small scale retail businesses, particularly small shops involving working long hours5.
Pakistani people are predominantly Muslim and form the largest Muslim community in Scotland. The first Muslim organisation was established in Glasgow in 19406. For Muslims, their faith is a way of life; it provides the main
3
www.scotlandagainstracism
4
ibid
5
ibid
6
www.ltscotland.org.uk/antisectarian/whatIsSectarianism/aboutsectarianism/Islam/ muslimsinscotlandtoday.asp
basis for group cohesiveness; it sustains and advances their ethnic identity and helps establish social networks (Anwar, 1994). Muslims in general face significant educational and economic disadvantage and experience racism and Islamophobia, which has heightened since 9/11 and the London bombings. Racism has been identified as a major issue affecting mental health and wellbeing for Muslims in Scotland and police data indicates that it has increased (Grant, 2007). The experience of conflict between cultural values, issues in relation to citizenship and defining identity have been identified as key issues for Pakistani Muslims with two main influences on identity being faith and national identity as Scottish7.
3. Conceptualising mental wellbeing
There are many different and debated definitions of mental wellbeing8 leading Ryan and Deci (2001) to conclude that mental wellbeing is a multidimensional and complex concept. Three key ideas emerge from the general literature on the concept of mental wellbeing. First the relationship between mental wellbeing and mental illness; second the elements of mental wellbeing and in particular the distinction between hedonic (subjective) and eudaimonic (psychological) wellbeing. Third the idea that mental wellbeing can be enhanced and is therefore an appropriate focus for understanding and intervention and consequently measurement.
3.1 The relationship between mental wellbeing and mental illness
Mental health is a confusing term and can be merely seen as a euphemism for mental illness as observed by Herron & Mortimer, 1999. They go on to identify two models for the relationship between positive mental health, i.e. mental wellbeing and mental illness. The bipolar or single continuum model reflects the view that mental wellbeing (positive mental health) exists at the opposing end of the same continuum as mental illness. The existence or degree of one is dependent on the existence, absence or degree of the other and mental wellbeing is therefore seen in terms of the absence or reduction of mental illness (Herron & Trent, 2000). Mental wellbeing has therefore been described as a secondary concept to mental illness; requiring prior knowledge of mental illness to be understood and inevitably viewed through ‘the lens of mental illness’ (Herron & Trent, 2000, p.30).
The alternative model is the two or dual continua model, which suggest that mental health consists of two dimensions; mental health problems or mental illness and mental wellbeing (positive mental health) (Tudor, 1996; Keyes 2007). Separating the definition of mental wellbeing from mental illness means that it is possible to focus on strengths rather than deficiencies; capacity rather than loss and growth rather than remediation (Herron & Trent, 2000). Mental wellbeing is thus more than the absence of mental illness and is a state “in which the individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community” (WHO, 2004, p.12 as
7
ibid
8
http://www.healthscotland.com/mental-health-background.aspx
cited in Keyes, 2007). There is emerging evidence to support the dual continua model – for example the data drawn from the Midlife in the United States (MIDUS) Survey, undertaken with English-speaking populations only. This model is increasingly being used to underpin public mental health in Scotland (Scottish Government, 2007) and the Scottish Indicators of Mental Health programme has established mental health indicators to encompass both mental health problems and positive mental health (Parkinson, 2007).
3.2 Elements of mental wellbeing
From a review of research on mental wellbeing, Ryan and Deci (2001) identify two broad traditions - hedonic wellbeing and eudaimonic wellbeing. Hedonic wellbeing often refers to the subjective sense of wellbeing, notably happiness and life satisfaction and is most usually termed subjective wellbeing (SWB). Eudaimonic wellbeing relates to the realisation of human potential and includes meaning, self-realisation and functioning in life and is usually referred to as psychological wellbeing. Although these two concepts overlap, they are derived from two distinct traditions, both arising from Western philosophy - hedonism and eudaimonism. They differ fundamentally in terms of their views of what constitutes a good society and a good life (Ryan & Deci, 2001). This has had implications for the questions asked about how developmental and social processes relate to wellbeing and to the approach to undertaking research and Ryan & Deci’s review outlines this in some detail. They describe how research within the hedonic paradigm has used the assessment of subjective wellbeing as its focus. SWB includes three components life satisfaction, positive mood and the absence of negative mood, which together are often summarised as happiness. Ryan & Deci argue that much of the research on SWB fits with the expectancy-value approach; in other words, that wellbeing is a function of expecting to attain (and ultimately attaining) the outcomes or values, whatever these might be. The goals through which SWB is enhanced can therefore be highly idiosyncratic and culturally specific.
Eudaimonic wellbeing, also referred to as psychological wellbeing, positive mental health or positive functioning consists of an individual’s evaluation of their psychological wellbeing (Keyes, 2006), It has been operationalised by Ryff who identified six aspects of functioning – autonomy, environmental mastery, personal growth, positive relations with others, purpose in life and self-acceptance (Ryff, 1989). Ryff has developed these into various scales of psychological wellbeing, which have been predominantly tested on US populations.
Keyes (2006) has commented on the relative lack of focus on the social dimensions of an individual’s functioning in life within the eudaimonic tradition of research. He has thus developed the concept of social well-being and proposed five dimensions - social coherence (whether a social life is seen as meaningful); social actualization (whether society is seen as possessing potential for growth; social integration (a sense of belonging and acceptance by their communities; social acceptance (feel they accept other people) and social contribution (sense of having something worthwhile to contribute) (Keyes 2006, p.5).
3.3 Enhancing mental wellbeing
Keyes (2006) contends that mental wellbeing9 (hedonic and eudaimonic) is a valuable asset at both an individual and a social level. In a conference presentation in Glasgow in autumn 200710, he thus argued that governments needed to focus on enhancing mental wellbeing as well as reducing mental illness. This emphasis is increasingly reflected in national government policy not just in Scotland but across the UK (DH, 2005) and internationally. The development of national mental health indicators in Scotland will enable changes in Scotland’s mental health (both mental wellbeing/positive mental health and mental health problems) to be monitored (Parkinson, 2007) and could provide a mechanism for evaluating the impact of public policy on the mental wellbeing of Scotland’s population.
3.4 Cultural and ethnic differences in the conceptualisation of mental wellbeing
The importance of cultural context in shaping health beliefs (Gervais & Jochelovitdh, 1998) and in wellbeing research is recognised (Keyes, Schmotkin & Ryff, 2002). In particular attention has been drawn to the integration of physical, spiritual and emotional aspects of health and illness in sharp contrast with mind-body dualism of Western philosophies impacting upon how mental distress is perceived Belippa (1991). In drawing comparisons between subjective and psychological wellbeing (Keyes, Schmotkin & Ryff, 2002) suggest that both traditions may reflect Western, and possibly middle and upper-class definitions of what it means to live a full and satisfying life. They suggest that Eastern perspectives may emphasise connection to others; meeting obligations and achieving fulfillment through carefully managed social ties.
This points to the importance of exploring mental wellbeing in different cultural contexts. However the discussion above raises a fundamental methodological issue about whether the constructs are equally applicable across different populations. Cheng & Chan (2004) note that this issue has been relatively unexplored. Two key concepts have thus influenced our thinking and approach, both derived from cross-cultural work in relation to the meaning of mental illness and stigma (Glasgow Anti-stigma Partnership, 2007). The first is the concept of categorical fallacy from Kleinman (1977) who sounds a note of caution in the search for conceptual equivalence in relation to the definition of mental illness. Kleinman uses the term to refer to the adoption of a disease classification developed for a particular cultural group and then applying it to another cultural group for whom it lacks coherence and for whom its validity has not been established (Kleinman, 1987, p. 452). The second related concept is the distinction drawn between etic and emic approaches, Again these concepts have been developed in the context of cross-cultural research with etic referring to the outsider view to research developed in the positivist tradition that emphasises independence, objectivity and universalism and
9 Although Keyes typically uses the term mental health to refer to mental wellbeing.
10
http://www.wellscotland.info/mentally-flourishing-scotland-interactive.html.
emic referring to the insider view, and to research in the constructionist tradition that is qualitative and focuses on developing an understanding and meaning from the communities’ perspective, often involving narrative accounts of individual experience.
4. Method
4.1 Aims and objectives of the scoping exercise
This scoping exercise forms phase one of a project, whose ultimate aims are to increase the understanding of: conceptualisations of mental health and wellbeing among BME groups; strategies used to promote mental wellbeing and prevent the development of mental health problems; and the extent to which these conceptualisations and strategies complement or diverge from current mental health improvement strategies. This scoping exercise is being undertaken to inform the scope, aims, methodology and focus of the subsequent research phase.
The aim of the scoping exercise is therefore to develop recommendations to inform the next research phase, focusing on the two largest established BME communities in Scotland, the Pakistani and Chinese communities11. It is important to understand that these communities are not homogenous and that there is considerable diversity in terms of age, generation of migration, gender, religious beliefs and geographical location. Specific objectives for this scoping exercise are:
• to scope and explore existing literature relating to the conceptualisations of mental wellbeing amongst Chinese and Pakistani communities and the strategies used by these communities to promote wellbeing within these communities and prevent mental health problems
• to gather expert opinion within Scotland regarding the extent that these conceptualisations and strategies are used by these two communities and the degree to which they complement or diverge from the majority population
• to explore priorities for further research in relation to promoting mental wellbeing and preventing mental health problems within the two communities
• to explore methodology literature in order to identify appropriate methodology for the subsequent research phase, with consideration of issues such as skills and experience required of researchers carrying out the project.
4.2 Involving stakeholders
It was recognised by NHS Health Scotland early on in the development process that the project required external expertise in the form of a steering
11
http://www.gro-scotland.gov.uk/census/censushm/index.html
group. NRCEMH made use of its national contacts across the BME mental health sector to approach individuals who would bring such expertise to the steering group. Many of the individuals approached were already part of NRCEMH’s Mental Health Strategic Advisory Panel. Although ultimately the steering group was small it did achieve representation from the BME mental health voluntary sector, mental health improvement specialists (with experience in BME work), specialist research and NRCEMH’s race equality and mental health programme.
The Steering Group has been directly involved in developing the research brief, monitoring and reviewing the progress of the work, informing the search strategy and defining the search terms for the literature review, identifying individuals and organisations to be interviewed and finalising this report.
4.3 Methodology
There are three elements to the scoping exercise – a literature review of conceptualisations and strategies for mental wellbeing; consultation with community informants to explore the use of these conceptualisations within a Scottish context; and, an exploration of the methodology literature, to identify the key issues for the subsequent phase of research.
4.3.1 Literature review
The literature review provides an appraisal of a diverse and wide range of literature to identify conceptualisations of mental wellbeing and strategies to promote mental wellbeing and prevent mental health problems within Chinese and Pakistani communities living within the UK and their parent countries. It is not a systematic review but is a scoping exercise and therefore deliberately wide ranging in order to establish the breadth of the literature. It has been undertaken in accordance with Social Care Institute for Excellence (SCIE) guidelines (Coren & Fisher, 2006). A protocol was developed for the review, and circulated for comment to the Project Steering Group. This protocol outlined in full the review question, search strategies, parameters for the review, analysis and quality appraisal methods. The technical detail is available in Appendix 1.
Review questions
• What are the main ways of conceptualising mental wellbeing by Chinese and Pakistani communities?
• What strategies do Chinese and Pakistani communities living in Scotland use to maintain their mental wellbeing?
• What strategies do Chinese and Pakistani communities living in Scotland use to prevent mental health problems?
• To what extent do these conceptualisations and strategies differ from majority populations living in Scotland?
• What methodologies have been used to ascertain conceptualisations of mental wellbeing In Chinese and Pakistani communities?
• What are the implications of this for further research to inform mental health improvement?
Searching
This review aimed to establish the extent of the literature and identify the implications for further searching for the next phase of the research. The materials were identified by using bibliographic databases and web-based sources, communication with experts in the field and contacting relevant organisations in the UK. A full list is provided in Appendix 1. The search terms used were mental wellbeing; emotional wellbeing; psychological wellbeing; subjective wellbeing; happiness; positive mental health; self-esteem; psychological resilience or adaptation or mental health beliefs or mental health concepts or mental health promotion or mental illness prevention and Chinese or Pakistani or Muslim or Asian or Black and minority ethnic (BME). The material searched for was limited to that published in English between 1988 an 2007, as an earlier review in relation to stigma and BME communities in Scotland had identified little material before this date.
Criteria for inclusion and exclusion
The criteria for inclusion was material concerned with knowledge, attitudes, concepts and beliefs of Chinese and Pakistani communities in relation to mental wellbeing and mental health and strategies for mental health promotion and/or prevention of mental illness. Both UK and international papers were included and non-English material was excluded, as it was not possible within the timescale and resources of the review to undertake translation.
Inclusion criteria
Papers were included if they met criteria in the following areas:
• Participants: Pakistani, Chinese; Asian; South Asian; Muslim of all ages and both men and women. Material that covered Muslim or South Asian or Asian communities was only included if there was clear reference to Chinese or Pakistani communities and it was possible to extract relevant data.
• Definition of mental wellbeing: As this is the focus of the review and given the conceptual issues raised earlier, the definition aimed to be as inclusive as possible and included beliefs, attitudes, personal experiences, self-expression, social relationships and behaviours that convey a positive sense of wellbeing and/or freedom from mental illness. The search terms used included mental wellbeing12, emotional wellbeing, psychological wellbeing, subjective wellbeing, resilience, happiness and self-esteem.
• Interventions: Material relating to mental health promotion activities used by Chinese and Pakistani communities was searched for using the terms mental health promotion, positive mental health and prevention of mental illness.
• Contexts: Scotland; UK; China; Pakistan; English-speaking non-UK countries, Europe.
12
And various spellings of wellbeing i.e. well being and well-being
• Literature. The search was limited to literature published from 1988 to the present day. The search was limited to material published in English.
Exclusion criteria
Papers were excluded if:
• published in languages other than English • relating to other BME communities
• solely concerned with substance abuse, drug misuse and alcohol abuse, or learning disabilities
• published on or before 31.12.1987.
Two reviewers applied the inclusion and exclusion criteria to all titles and abstracts and then to the majority of hard copies. Papers identified were coded for inclusion, and all relevant or potentially relevant papers were retrieved, within an 8 week period. Theses, although details were kept were not retrieved at this stage.
Analysis
The analysis that was undertaken was as follows: Mapping of available material
All the material that met the inclusion criteria was systematically mapped in order to describe the extent of the available material, identify gaps in the knowledge base and to identify areas for future work. A keywording strategy for classifying the material was used (see Appendix 1) with the following categories:
• participants (i.e. Chinese or Pakistani, age, generation, gender)
• location (China, Pakistan, US and Canada, Australia and New Zealand, Other European)
• type of material (theoretical, study and type of study, instrument design, policy, commentary)
• focus (mental wellbeing, quality of life, subjective wellbeing, happiness, mental health symptomatology, mental health improvement, prevention of mental illness).
In depth analysis of the material
The material was organised into four categories, reflecting the country that the material related to: UK, considered primary data; China or Pakistan, English speaking Non-UK countries and Europe, which were all considered as secondary data sources.
1. Material from the UK
An in-depth analysis, including a quality appraisal, was undertaken on this material as this was considered to be primary data. The categories for data extraction of content were:
• participants (Chinese or Pakistani, age, generation, gender)
• location (Scotland; rest of UK)
• language and key terms used to describe mental wellbeing • conceptualisation of mental wellbeing
• factors identified influencing conceptualisations of mental wellbeing • details of strategies to promote mental wellbeing and/or prevent
mental health problems
• outcomes of strategies used, including service user views • comparisons with other populations.
In addition, details were extracted relating to the evidence:
• evidence type and main details of design e.g. aim, sample, data collection method
• quality criteria relevant to the evidence type/study design.
There was limited but consistent quality appraisal of included material using a brief version of TAPUPAS (Pawson, Boaz, Grayson et al., 2003). The form for this is included in Appendix 1 and the criteria include strength of design, centrality of perspectives of Chinese and Pakistani communities; transparency; quality and reporting of analysis; utility; propriety; accessibility and generalisability. No material was excluded from the review on the basis of quality, but quality issues influencing the interpretation of results and the strength of the evidence are included in Section 5.2.
2. Secondary data
A thematic analysis was undertaken on the material from China and Pakistan, defined by participants’ location, rather than author location. A more limited analysis was undertaken and the following categories for data extraction were used:
• language and key terms used to describe mental wellbeing • conceptualisation of mental wellbeing
• factors identified influencing conceptualisations of mental wellbeing • details of strategies to promote mental wellbeing and/or prevent
mental health problems
• outcomes of strategies used, including service user views • comparisons with other populations.
This material from English speaking, non-UK countries or Europe was read and the key theoretical points extracted.
The results from the mapping the literature is are provided in Section 5, the more detailed analysis in Sections 6 and 7, where it is considered in relation to Chinese and Pakistani communities respectively, and an overview of the search results and details of the papers and data extracted available in Appendices 4-7.
4.3.2 Consultation with community informants
A qualitative approach was used to collect in-depth data using either one to one or group interviews with 47 community development workers with
Chinese and Pakistani communities in Scotland. The aim of these interviews was to explore:
• conceptualisations and strategies used by Chinese and Pakistani communities within the Scottish context
• the similarities and differences for these communities and the majority populations
• priorities for future work in relation to mental health promotion and/or the prevention of mental illness in Chinese and Pakistani communities; • key issues in relation to the methodology for the next phase.
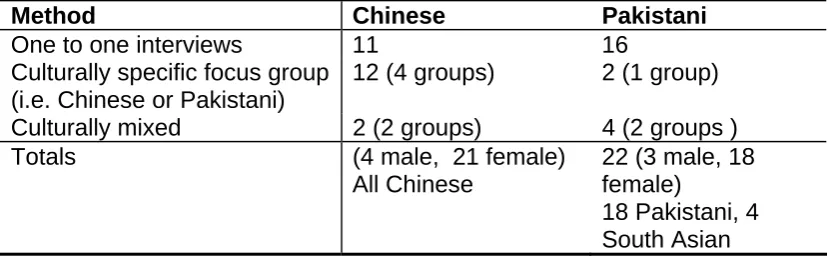
The individuals were selected for this initial stage because of their roles, which gave them a working knowledge and overview of the issues in relation to these communities. Individuals were only interviewed as a group when more than one member of the community worked in the same organisation and hence the participants would have an existing working relationship. Table 1 details the total number of participants (N = 47) together with the breakdown of participants and method used.
Sampling and recruitment strategies
As the timescale for this first phase was tight, it was necessary to adopt a degree of pragmatism to recruit participants. Nineteen key organisations or individuals were identified by NRCEMH. Four initial scoping interviews were undertaken with this sample to identify other potential interviewees and snowballing was subsequently used to identify other key informants. Information about the research was sent to the identified individuals and groups (see Appendix 2). This was followed by a personal approach by telephone to provide further information, answer questions and arrange a date either for an individual interview or focus group discussion.
Participants
[image:25.595.90.507.642.771.2]Forty-seven interviews were undertaken with people who had relevant knowledge of either Chinese or Pakistani communities in Scotland. The majority were community workers mainly in the voluntary sector with a small number in professional roles e.g. social work, health promotion. All of the people working with Chinese communities were Chinese and 81% of those working with the Pakistani community were Pakistani with the remainder being South Asian.
Table 1: Details of participants and methods used
Method Chinese Pakistani
One to one interviews 11 16
Culturally specific focus group (i.e. Chinese or Pakistani)
12 (4 groups) 2 (1 group) Culturally mixed 2 (2 groups) 4 (2 groups )
Totals (4 male, 21 female)
All Chinese
22 (3 male, 18 female)
18 Pakistani, 4 South Asian
The majority of interviewees were drawn from the urban belt between the main centres of population and interviews were undertaken in Edinburgh or Glasgow. The number of men in the final sample was relatively small (15%) and this is likely to reflect the recruitment strategy of targeting community workers in the voluntary sector, which is female dominated.
In addition, four telephone interviews were undertaken with key informants who could provide a national picture of developments in relation to mental health policy, mental wellbeing and/or BME communities in Scotland.
Data collection
Data was collected through interviews or small group interview as appropriate. The majority (96%) of interviews with the key community informants were face to face with the remainder being telephone interviews. All but one of the interviews were undertaken mainly in English, with the other being conducted in Urdu. However the language skills of the researcher enabled definitions or terms to be explored in Urdu or Punjabi as appropriate.
Lines of inquiry
The topic guide used to ascertain the views of the participants is provided in Appendix 3. These interviews were in-depth and open ended to encourage interviewees to explore the issues from their perspective. The areas covered were:
• language and terms used to describe mental wellbeing, mental health and mental illness
• preferred conceptualisations of mental wellbeing
• factors influencing the conceptualisation of mental wellbeing including spirituality, family and community factors etc
• perceived differences between the conceptualisation of wellbeing and that of the majority population
• the range of strategies for promoting and maintaining mental wellbeing and frequency of use by different community members • the range of strategies for preventing mental health problems and
frequency of use by different community members
• priorities for future research on promoting and preventing mental health problems in Chinese and Pakistani communities
• key issues in relation to the methodology for the next phase e.g. preferred methods for community engagement.
The topic guide was only that – a guide. It showed what needed to be covered and expected responses to vary according to the individual. The language on the guide – formal academic language was substituted with everyday wording during the interview. The questions were not asked in any particular order and the questions were supplemented with follow on questions to answers given by participants. In a way the guide was a checklist and used as a prompt for information. All interviews with community informants were tape recorded and 60% transcribed for analysis reflecting the available time and resource constraints of the project, although saturation was reached fairly early on. The remaining tapes were all listened to and coded.
Analysis
The review questions were used as the main focal points of analysis for the data and the interview data was analysed using a systematic thematic analysis method. An initial coding frame was developed from the categories used for the literature review to enable comparison and synthesis of the interview data with that from the review. Each interview transcript was coded and summary notes and memos made in the margins. This was carried out for all the transcribed data (60% of total data set). The remaining taped data was then listened to and data extracted in relation to the identified codes and themes.
4.3.3 Synthesis
Findings from the literature review and the consultation with community informants were drawn together to provide a description of the language and terms used to describe mental wellbeing by Chinese and Pakistani communities, the conceptualisations of mental wellbeing, the factors influencing these conceptualisations, the strategies used by these communities to maintain and promote mental wellbeing or prevent mental illness, comparisons with the majority population and the implications for further research. The information has been organised to answer the review questions above (see Sections 6 and 7). A glossary of terms used by informants can be found in Appendix 7).
4.3.4 Ethical considerations
As the project involved consultation with community workers rather than NHS patients, it was not necessary to obtain NHS Ethical Committee Approval but approval was applied for and given by the University’s Faculty of Health Ethics Committee. Information about the study was given or sent to key informants and community organisations and this laid out:
• the aims of the study and purpose of the interview
• the areas that the consultation group or interview will cover • consent and the right to refuse
• confidentiality
• what will happen to the information that is collected.
Participants were asked if they have any questions about their involvement before the interview commenced and were asked to give written consent at the beginning of the interview for the interview to be recorded.
Confidentiality was stressed both in the written information circulated prior to and at the beginning of the interview. All information given during the course of the interviews will be treated confidentially and the anonymity of all participants in the study was assured.
4.4 Exploration of the relevant methodology literature
A rapid review was undertaken to identify key publications and reviews of methodologies for research with Black and minority ethnic communities from 1990. The search strategy focused on web-based sources that were known to
the authors to have specific expertise in this area or be undertaking research on BME communities and included:
• Scottish Government, Department of Health, Department of Communities and Local Government and Care Services Improvement Partnership (CSIP), non-government organisations such as the Civis Trust, the Mental Health Foundation and the Scottish Development Centre and Universities known to be undertaking relevant mental health-related research with Black and minority ethnic communities
• Examination of national databases specifically the Kings Fund; the CSIP library database, CRE, Joseph Rowntree Foundation, Social Care Online .
In addition a basic search of two bibliographic databases (Medline and Cambridge Web of Knowledge) was also undertaken. The search terms used were research methods, participatory research, community engagement and Black and minority ethnic and the search was not restricted to health or mental health. Strict inclusion criteria were not applied as this was essentially an exploratory exercise to scope what was readily accessible.
The results of the rapid appraisal and from the methodology literature review have been used to build an annotated bibliography for use in the second phase of the study (Appendix 8). The results of this are included in Section 9 together with the methodological issues identified during the course of the review and observations from interviewees about methods for future research. Information about methods for undertaking research on mental wellbeing with Chinese and Pakistani communities was extracted from the material that had met the study inclusion criteria for the literature review on conceptualisations of mental wellbeing and from interview data, where interviewees had explored methodological issues. The results of this have been combined and are reported in Section 10.
4.5 Limitations
There are five main limitations to this scoping exercise, the first two reflecting that this is a scoping review. First, the search for grey literature was limited and given the relative shortage of published material it is important to extend the search in the next phase. Whether this will lead to the identification of a significant amount of additional material may be unlikely, given the feedback from experts in this area. Second, the depth of the analysis in all elements is limited as the aim has been to provide an overview of the key issues. However data capture, particularly in the fieldwork element has been good and consideration should be paid to undertaking further analysis of existing data as part of the next phase of this project. Third the majority of fieldwork was undertaken by an English-speaking researcher who was also fluent in Urdu and Punjabi and supported in the analysis by a colleague, also fluent in both languages. However, the research team did not have the same capacity in relation to Chinese languages and this is a major weakness as English was the second language for a number of participants. Fourth there was a significant gender imbalance in the sample with the ratio of women: men being 5.6:1. This reflected the sampling strategy of recruiting via community organisations where there are more women workers in community worker
roles. This is a potential source of bias and will be taken into account in the interpretation of the results from the fieldwork data.
Finally, the extent of involvement of people from Chinese and Pakistani communities in the research design and process has been limited. Involvement of people from these communities has the potential to increase the validity and quality of research (Beresford, 2005) and therefore needs consideration in any subsequent work.
5. Review of the literature
This section provides the results from the literature review element of the scoping exercise. 5.1 provides an overview of the material that was identified and the following sub-sections a summary by country of origin. The main themes from this material are summarised in Sections 6, 7 and 8 together with the findings from the interviews with the community informants.
5.1 Overview of the material identified
A total of 5,264 papers were identified, with a significant number of duplicates. Once these were removed 4006 papers were filtered and those that did not meet the inclusion criteria were excluded either on the basis of date, the paper’s scope, the population considered or if it was clear that it was not available in English. This left 508 papers and of these it was possible to retrieve 461 papers (90.7%). These were subsequently filtered again and 140 papers that met the criteria for inclusion as either a primary or secondary source were left. Appendix 4 provides an overview of the results from each stage of the review and Appendix 5 a bibliography of papers classified by country.
5.1.1 Breakdown by country
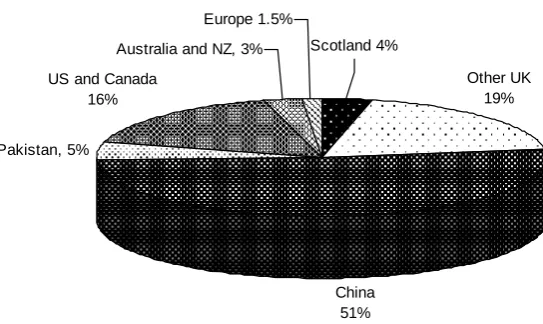
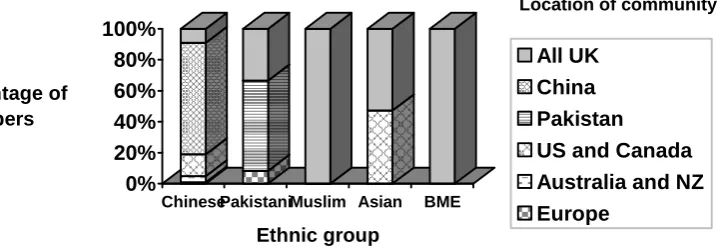
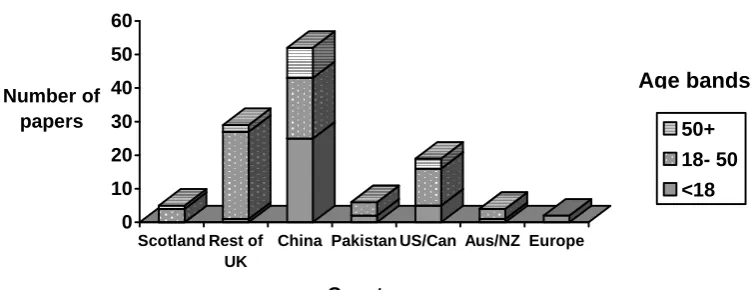
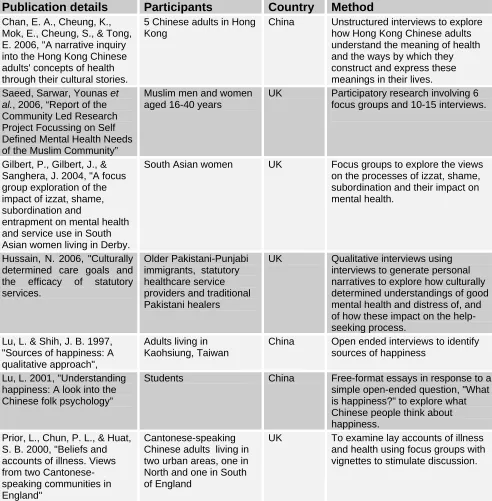
[image:29.595.186.458.561.723.2]The majority of the material identified that met the inclusion criteria related to Chinese populations, with the majority coming from China. Figure 1 provides an overview of the material identified by country and Figure 2 a breakdown by country and ethnicity.
Figure 1: Analysis of material by country (N =140)
Pakistan, 5%
Australia and NZ, 3%
China 51%
Other UK 19% Scotland 4%
Europe 1.5%
US and Canada 16%