EuropeanAnnalsofOtorhinolaryngology,HeadandNeckdiseases(2014)131,159—166
Availableonlineat
ScienceDirect
www.sciencedirect.com
ORIGINAL
ARTICLE
Malignant
head/neck
paragangliomas.
Comparative
Study
A.
Mediouni
a,
S.
Ammari
a,
M.
Wassef
b,f,
A.-P.
Gimenez-Roqueplo
c,
J.-D.
Laredo
d,f,
M.
Duet
a,f,
P.
Tran
Ba
Huy
g,
N.
Oker
e,f,∗aServicedemédecinenucléaire,hôpitalLariboisière(AssistancePublique—HôpitauxdeParis),2,rue
Ambroise-Paré,75010Paris,France
bServicedecytologieetd’anatomiepathologique,hôpitalLariboisière(AssistancePublique—Hôpitauxde
Paris),2,rueAmbroise-Paré,75010Paris,France
cServicedegénétique,hôpitaleuropéenGeorges-Pompidou(AssistancePublique—HôpitauxdeParis),20,
rueLeblanc,75015Paris,France
dServicederadiologie,hôpitalLariboisière(AssistancePublique—HôpitauxdeParis),2,rue
Ambroise-Paré,75010Paris,France
eServiced’otorhinolaryngologie,hôpitalLariboisière(AssistancePublique—HôpitauxdeParis),2,rue
Ambroise-Paré,75010Paris,France
fUniversitéParis-DiderotParis-7,75205Pariscedex13,France g2,rueSaint-Petersbourg,75008Paris,France
KEYWORDS
Malignantheadand neckparaganglioma; Metastases; SDHxmutation; Octreoscan; 18FDG-PET Summary
Background: The objectiveofthisstudy wastoreport11 casesofmalignantheadandneck paragangliomaandtocomparetheirepidemiological,clinical,andgeneticcharacteristics,their naturalhistoryandtheirtreatmentwiththoseofaseriesof131benignparagangliomas. Patientsandmethods: Retrospectiveanalysisof142patientswithheadandneckparaganglioma managedbetween2001and2008.Ageatthetimeofdiagnosis,gender,primarytumoursite, presenceofothernon-head/neckparagangliomasand/ormetastasesdiagnosedbyimaging(CT, MRI,Octreoscanor18F-FDGPET),histology,urinarycatecholamineandmetanephrinelevels,
familyhistory,andgenetictestresultswererecorded.
Results: Thisseriescomprised131benignheadandneckparagangliomas,mostlyobservedin womenwithameanageatdiagnosisof45yearsandapredominanceoftympanojugularsites (followedbycarotidandvagalsites)with5%ofsecretingtumoursand20%ofmultifocaltumours. Elevenpatients(7.7%)witha1:1sex ratiopresentedcriteriaofmalignancy.Thesepatients, withalowermeanage(38years),predominantlypresentedcarotidlesionswithahigherrate ofsecretingandmultifocaltumours,27%and46%respectively.Themainsitesofmetastases wereboneandlymphnodes.Notympanicparagangliomaswereobserved.
∗Correspondingauthor.Serviced’otorhinolaryngologie,hôpitalLariboisière(AssistancePublique—HôpitauxdeParis),2,rueAmbroise-Paré,
75010Paris,France.
E-mailaddress:[email protected](N.Oker).
1879-7296/$–seefrontmatter©2013ElsevierMassonSAS.Allrightsreserved. http://dx.doi.org/10.1016/j.anorl.2013.05.003
Conclusions: Malignantparagangliomasaremainlyobservedinyoungpatientswithmultifocal tumours,particularlycarotidtumours,andarepredominantlyrelatedtosubunitSDH-B muta-tion.Thework-upinthesehigh-riskpatientsmustincludewholebodyscintigraphyandspine MRI.Malignancyisnotnecessarilyassociatedwithapoorshort-termprognosisduetotheslow courseofthedisease.
©2013ElsevierMassonSAS.Allrightsreserved.
Introduction
The WorldHealthOrganisation[1] definesparagangliomas (PG) asneuroendocrine tumoursarisingfrom paraganglia, collectionsofneuralcrest-derivedparaganglionic neuroec-todermalcellspresentthroughoutthebody.
However, malignant paragangliomas are rare and no consensus has been reached concerning the histological criteria of malignancy, although multiple mitotic figures, nuclearpolymorphismandcapsulareffractionmayindicate thepresenceofmalignancy.According toLack [2],twoof thefollowingthreecriteriaarerequired toconfirm malig-nancy:centralnecrosis,vascularandlymphaticinvasionand mitotic abnormalities. There is a general consensus that malignancyischaracterisedbythepresenceofmetastases, i.e.paraganglionictissueinorgansotherthanparaganglia. Thisdefinitioncantherefore beusedtodistinguish malig-nanttumoursfrommultifocaltumoursarisinginparaganglia
[3].
Limiteddata areavailable in theliterature concerning malignantheadandneckparagangliomasandtheirnatural historyispoorlydefined.However,itisgenerallyaccepted that6%to24%ofnon-adrenalparagangliaaremalignant[4]. Recentprogressinmoleculargeneticssince2000[5]hasalso revealedthatSDHxgenemutationisinvolvedinhereditary paragangliaandthatmalignantformsareoftenassociated withmutationoftheBsubunit[6].
Thisstudyreports11casesofmalignantheadandneck PGandcomparestheirepidemiological,clinicalandgenetic characteristics,naturalhistoryandtreatmentwiththoseof aseriesof131benignPGmanagedoverthesameperiodin ourinstitution.
Patients
and
methods
This retrospective studyconcerned allpatients consulting foraprimarydiagnosisorreferredforheadandneckPGin ouruniversityhospitalbetween2001and2008.
Age at the time of diagnosis, gender, primary tumour site,presenceof othernon-head/neck PGsand/or metas-tasesdiagnosedbyimaging,includingCT,MRIorfunctional whole body imaging (somatostatin scintigraphy, 18FDG or 123I-MIBG PET), sometimes confirmed by histology, urinary
metanephrinelevels,familyhistory,andgenetictestresults wererecorded.PatientswerefolloweduntilSeptember2012 oruntildeath.
Results
This series comprised 142 patients, including 11 (7.7%) patientspresentingcriteriaofmalignancy.
PatientswithbenignPG(group1)
This group comprised 131 patients (87 females; M:F sex ratio: 1:1.98). The main characteristics of these patients areshowninTable1.
Mean age at diagnosis of the primary head and neck PGwas45.3years (range:15—76). Onehundredand thir-teen(86.3%)patientspresentedanisolatedheadandneck lesion and 18 (13.7%) patients presented multiple lesions (synchronous lesions). Isolated lesions involved tympanic (n=32),tympanojugular(n=37),vagal(n=18),andcarotid (n=26)sites.Sixpatients(4.6%)hadsecretingtumours.
Another head and neck paraganglioma (metachronous lesions) was observed during follow-up in 8 of the 113 patients with a single primary tumour and 1 para-aortic PG was detected by 111In-pentetreotide scintigraphy. The
globalmultifocalrate(includingheadandneckand thoraco-abdominopelvicPG)wastherefore20.6%ingroup1.
The mean interval between diagnosis of the primary lesionandrecurrenceaftersurgery(n=13)ordiagnosis of anewPG(n=9)was9.9years(range:4—20)and13years (range:2—39),respectively.
Genetictesting(when availableand whenaccepted by the patient) was performed in 43 patients: 24 patients (55.8%)presentedamutationoftheDsubunitofthe succi-natedehydrogenasecomplex(SDH-D)and4(9.3%)presented amutationof theSDH-Bsubunit; 15patients (34.9%) pre-sentednomutation.
PatientswithmalignantPG(group2)
Paraganglionicdisease
This group consisted of 11 patients (6 females; male to femaleratio: 1:1.2).The main patientcharacteristics are summarized inTable1. Meanageat thetimeofdiagnosis was 37.8 years (range: 17—65). At the time of diagno-sis, paragangliomas were isolated in 9 cases (82%) and multiple in two cases. Isolated tumours involved carotid (n=5),vagal(n=2),tympanojugular(n=1)andnasalcavity (n=1)sites. The twocases ofmultiple PGwere tympano-jugular and carotid. No pure tympanic site was observed in this series. Three patients (27.3%) presented secreting tumours.
Among the 9 patients with an isolated lesion, metachronous PG were diagnosed during follow-up in 3 cases.Inthesethreepatients,someofthesemetachronous tumoursweresituatedin regionsotherthan theheadand neck:thoracic (n=1),retroperitoneal(n=1),thoracic and retroperitoneal(n=1).Theoverallmultifocalrate (includ-ing multiple head and neck and thoraco-abdominopelvic PGs)was45.5%.
Malignanthead/neckparagangliomas.ComparativeStudy 161
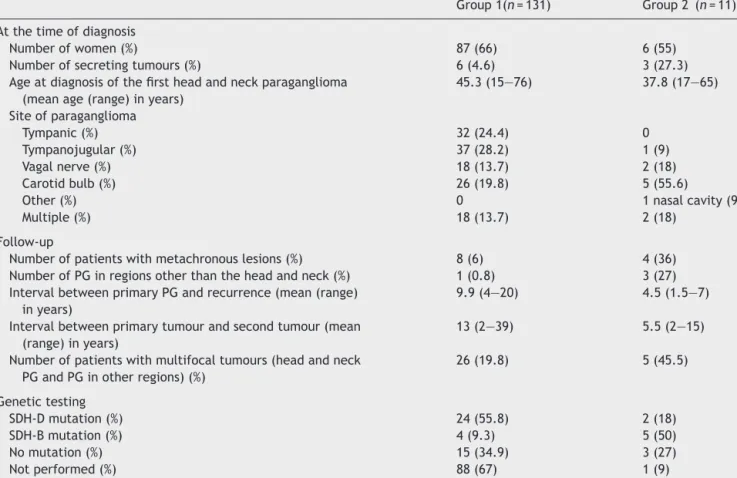
Table1 Characteristicsofthetwogroups.
Group1(n=131) Group2 (n=11) Atthetimeofdiagnosis
Numberofwomen(%) 87(66) 6(55)
Numberofsecretingtumours(%) 6(4.6) 3(27.3)
Ageatdiagnosisofthefirstheadandneckparaganglioma (meanage(range)inyears)
45.3(15—76) 37.8(17—65) Siteofparaganglioma Tympanic(%) 32(24.4) 0 Tympanojugular(%) 37(28.2) 1(9) Vagalnerve(%) 18(13.7) 2(18) Carotidbulb(%) 26(19.8) 5(55.6)
Other(%) 0 1nasalcavity(9)
Multiple(%) 18(13.7) 2(18)
Follow-up
Numberofpatientswithmetachronouslesions(%) 8(6) 4(36) NumberofPGinregionsotherthantheheadandneck(%) 1(0.8) 3(27) IntervalbetweenprimaryPGandrecurrence(mean(range)
inyears)
9.9(4—20) 4.5(1.5—7)
Intervalbetweenprimarytumourandsecondtumour(mean (range)inyears)
13(2—39) 5.5(2—15)
Numberofpatientswithmultifocaltumours(headandneck PGandPGinotherregions)(%)
26(19.8) 5(45.5) Genetictesting SDH-Dmutation(%) 24(55.8) 2(18) SDH-Bmutation(%) 4(9.3) 5(50) Nomutation(%) 15(34.9) 3(27) Notperformed(%) 88(67) 1(9)
The mean interval between diagnosis of the primary lesionandrecurrenceaftersurgery(n=4)ordiagnosisofa secondPG(n=4)was4.5years(range:1.5—7)and5.5years (range:2—15),respectively.
Genetictestingwasperformedin10patients:2patients presentedamutationoftheDsubunit(SDH-D),5patients presentedamutationoftheBsubunit(SDH-B)and3patients hadnomutation.
Metastases
Metastases were present at the time of diagnosis of the primary lesion in 3 patients and were diagnosed during follow-up in another 8 patients, witha mean metastasis-freeintervalof8years(1—25).Thesemetastasesinvolved bone(n=7),cervicallymphnodes(n=7),liver(n=2),lung (n=1),andthyroid(n=1)(Table2).
Bone metastases were symptomatic in four cases and detected bysystematic imaging inthreecases. They pre-dominantlyinvolvedthespine,butalsotheiliacbone,ribs, sternumorcalvarium.
MRI demonstrated two types of lesions: nodular and expanding. Nodular lesions presented a specific radiolog-ical appearance, as we have previously described [7], consisting of a central low-intensity signal surrounded by a single fat-like halo or a double halo with a fat-density inner circle and an outer circle suggestive of oedema(Fig.1a,b).Insomepatients,theselesions coex-isted with expanding lesions characterized by cortical
destruction and soft tissue involvement, especially bone marrow.
111In-pentetreotide (Octreoscan) scintigraphy revealed
onlysomeofthesebonelesions(Table2).123Iodine-labelled
metaiodobenzylguanidine(123I-MIBG)scintigraphywas
per-formed in 4 patients and revealed only slight contrast enhancementof the spine in one patient. 18FDG-PET was
performedintwopatientsandwasnegativeinonecaseand stronglypositiveintheothercase.
Cervical lymph node metastases were detected in 7 cases,eitheronneckpalpationorbyimagingshowingamass situatedinazoneclearlydistinctfromthecarotidbulbor subdigastricregion.
Twopatients hadnodularliver metastasesandanother patient had lung metastases. One patient had a thy-roidmetastasis, incorrectlydiagnosed aspapillarythyroid tumourandtreatedbysurgeryand131Iodinetherapy.Three
yearslater,thispatientdevelopedvertebralmetastasesand retrospective analysis of the thyroid operative specimen establishedthecorrectdiagnosis.
Follow-up
Meanfollow-upwas4.25years(range:1—10.5years).One foreignpatientdiedinhiscountryoforigin56monthsafter managementinourinstitution,apparentlyfrommetastatic cachexia.Twopatientswerelosttofollow-up,oneafter1 monthandtheotherafter5years.
A.
Mediouni
et
al.
Table2 Characteristicsofmetastasesin11casesofmalignantparaganglioma.
Patient SDHmutation Site Modeof
discovery
111In-pentetreotide
scintigraphy (Octreoscan)
18FDG-PET 123I-MIBG SpineMRI Follow-up
(months)
1 B Bone,lymph
nodes
Imaging Ribs,sternum Notdone Metastasesnot
visualized
Multiplelesionsof cervical,thoracic andlumbarspine
96
2 B Bone Dorsalpain Multiplelesionsof
cervical,thoracicand lumbarspine,sacrum, occipitalbone
Notdone Metastasesnot visualized
Multiplelesionsof cervical,thoracic andlumbarspine
Dead(56)
3 Nomutation Bone Weaknessof
lower
limbs+pyramidal syndrome
L3+rightclavicle Notdone Metastasesnot visualized
Multiplelesionsof cervical,thoracic andlumbarspine
303
4 D Bone Imaging Metastasesnotvisualized Metastasesnot
visualized
Notdone Multiplelesionsof cervical,thoracic andlumbarspine
348
5 B Lymphnode
bone
Lowbackpain Palpation
Metastasesnotvisualized Metastasesnot visualized
Notdone Lesionsoflumbar spine Lostto follow-upat1 month 6 Nomutation Bone Liver Thyroid Bonepain Imaging Palpation
Vertebralcolumn,ribs, pelvis,liver Vertebrae, sternum, sacrum,pelvis, ribs Lesionof thoracicspine Multiplelesionsof cervical,thoracic andlumbarspine
247
7 B Lymphnodes Palpation Metastasesnotvisualized Notdone Notdone Metastasesnot
visualized
250
8 Nottested Lymphnodes Palpation Metastasesnotvisualized Notdone Notdone Metastasesnot visualized Lostto follow-upat 144months 9 B Lymphnodes Bone Liver Palpation Imaging
Thoracicspine+liver Notdone Notdone Notdone 21
10 Nomutation Lymphnodes Palpation Metastasesnotvisualized Notdone Notdone Metastasesnot visualized 14 11 D Lymphnodes Lung Palpation Imaging
Metastasesnotvisualized Notdone Notdone Metastasesnot visualized
Malignanthead/neckparagangliomas.ComparativeStudy 163
Figure1 MRIofthelumbarspine,sagittalsection,T1-(a)and gadolinium-enhancedT1-weighted(b)sequences:presenceof nodularbonemetastaseswithadoublehalo.
Onepatient(patient3)requiredsurgicalcurettageofa lumbarvertebraduetoprogressivelowerlimbparaparesis. In five patients (patients 2, 4, 5, 6 and 9), MRI after 4 years did not reveal any new lesions or any change in the size of the metastases. However,detailed analysisof signalintensityonT1-andT2-weightedsequencesshowed decreasedoedemaoftheouterhalooftwovertebrallesions intwopatients.
The lastpatient(patient1)wasoperatedfor leftvagal PG in 2001 and, two years later presented a very large lefttemporallesionwithintracranialextensionand multi-plemetastasesofthecervicothoracicvertebrae,calvarium andonerib.Radiotherapyatadoseof45Gywasdelivered tothetemporallesionbutbonemetastasesdidnotrequire anytreatment,astheyremainedasymptomatic.Afteralong periodof apparent stabilization, the patientconsulted in November2012 following theappearance oftwoleft cer-vicalmasses.CTandscintigraphyconfirmedthemetastatic natureofthesemasses,butalsorevealedmarked progres-sionoftheC6andC7lesions(thatinitiallyhadanosteolytic appearance)associatedwithepiduritis(Fig.2).The riskof short-termspinalcordlesionsjustifiedradiotherapyofthe vertebrallesion.Cervicallymphnodedissectionconfirmed thepresenceof metastases.Thiscase illustratesthe rela-tivelyslowrateofprogressionofmetastaticdisease.
The7patientswithlymphnodemetastasesweretreated byneckdissectionconcomitantwithsurgicaltreatmentof thetympanojugularorcarotidtumourin6cases(patients5, 7,8,9,10and11),whiletheseventhpatientcorresponded topatient1describedabove.Twoofthese6patientswere
lost to follow-up, one at 1 month, and the other at 5 years.Threepatients havenotdevelopedanylocal recur-renceandarecurrently alivewithnosignsof progression oftheirparaganglioma.The lastpatient(patient10),who initially presented a vagal PG with cervical lymph node metastasestreatedbysurgeryandexternalbeam radiothe-rapy,developedmultipleboneandlivermetastasesduring thefollowingyearandiscurrentlyinpalliativecare.
Of the twocases of liver metastases diagnosed at the time of diagnosis of the primary tumour (patient 6 and 9), one alsopresented lung metastasis and died after 56 months.Theotherpatientisalivewithnoapparentsignsof progression.
Discussion
Thisretrospective,comparativestudyofoneofthelargest seriespublishedtodatedefinescertainaspectsofthe nat-uralhistoryofmalignantheadandneckparaganglioma.
Inlinewiththeliterature,patientswithbenignheadand neck PG were predominantly females (66%) and tumours were predominantly located in tympanojugular sites (fol-lowedby vagal andcarotid sites),with amean ageof 45 yearsat thetimeofdiagnosis, withlowrates ofsecreting andmultifocaltumours:5%and20%,respectively.
Incontrast,patients withmalignanthead andneck PG (7.7% of the population of this series, i.e. a comparable ratetothatreportedintheliterature[8])didnotpresent anygenderpredominance, mainlypresentedcarotidsites, hadayoungermeanageatthetimeofdiagnosis(38years), andpresentedhighratesofsecreting(27%)andmultifocal tumours(46%). These characteristics appeartoconstitute riskfactorsformalignancy.
No purelytympanic lesion wasobserved in this series. These forms are classically not multifocal, occur in the absenceofafamilyhistoryandtreatmentisbasedon sur-gicalresection,whichisusuallystraightforward.Thisseries confirmsthatpuretympaniclesionsareneveraccompanied bymetastases[9]andthereforedonotrequiregenetic test-ingorstagingassessment.
Metastaticspreadmay behaematogenousor lymphatic andmainly involvebone and lymph nodes[4,7,10]. Liver andlung metastasesareobservedmorerarely.Metastases maybeeithersynchronous,atthetimeofdiagnosisofPG,or metachronous,inwhichcasetheyappeartobeassociated withabetterprognosis[11].
Bone metastases may remain asymptomatic or may present clinically in the form of neurological deficits or pain,or radiologically according totwo modalities: oste-olyticand expandingor nodularsurrounded bya singleor doublefat-densityandwater-densityhalo.Reductionofthe water-density zone and increase of the fat-density zone wereobservedduringfollow-up, suggestingpossible spon-taneous involution. The results of our seriesindicate the generally slow rate of progression of PG. However, two patients developed signs of extension tothe spinal cord, requiringsurgeryinonecaseandradiotherapyintheother case.
Lymph node metastases are usually detected by neck palpation or by X-rays or scintigraphy. Tumours situated too inferiorly or too anteriorly to correspond to carotid
Figure2 a:neckMRI,gadolinium-enhancedT1-weightedsequence,axialsection:twoleftcervicallymphnodemetastases;b: spineMRI,T2-weightedsequence,sagittal section: spinal cordcompression overC7;c: octreoscan,coronalsection: increased uptakeinalymphnode:d,e:octreoscan,axialandcoronalsections:increaseduptakeofC7vertebra.
orvagaltumoursmustbeconsideredtobepossiblelymph nodemetastases.Theyaresometimesdiscoveredonsurgical explorationandareconfirmedbyhistologicalexamination. Theyappeartobeassociatedwitharelatively favourable prognosis,aslymphnoderecurrencesappeartoberare.
Functional imaging does not appear to be a reliable modality for the detection of bone metastases. Although functionalimagingcandetectprimaryPGoftheheadand neckorothersiteswithsensitivitycloseto100%[12],111
In-pentetreotidescintigraphyfailedtovisualizeallmetastases inthepresentseries.Thispoorperformancehasalsobeen reportedbyTimmersetal.[13],whodescribedpooruptake of123/131I-MIBG[14] bynon-adrenalPG.123I-MIBGrevealed
bonemetastasisinonlyoneofthefourcasesofourseries. PET-CThasbeenproposedintheliteratureforthe assess-ment of phaeochromocytomas and PG. 18F-FDG is more
reliable for the detection of PG than their metastases
[13,15].18F-DOPAhasahighsensitivityforthedetectionof
benignheadandneckPG[16],butalowsensitivityforthe detectionofmetastases,particularlyinsubjectswithSDH-B
mutation.Thelowperformanceofthesespecificagentscan beexplainedbylossofdifferentiationofmetastasesrelated toSDH-Bmutation.
A recent study demonstrated that plasma levels of a metabolite of dopamine, methoxytyramine, higher than 0.2nmol/L constituted a useful biomarker to detect the presenceofmetastases[17].
InfamilialformsofbenignheadandneckPG,amutation oftheDsubunitoftheSDHgeneisidentifiedin50%to94% ofcases,whileamutationoftheBsubunitisidentifiedin 10%to20%ofcases[18,19].Insporadicforms,aSDHgene mutation,mainlyinvolvingtheDsubunit,isreportedin11% to29%ofcases[18].However,SDH-Bmutationsaremainly reportedin malignant headand neck PG[6,8,18,20].The resultsofthepresentseriesconfirmthesepublishedresults, withapredominanceofSDH-Dmutation(56%)inthebenign PGgroupandSDH-Bmutation(5ofthe10patientstested, i.e.50%)inthemalignantPGgroup.However,twopatients ofthemalignantPGgrouppresentedaSDH-Dmutation,as previouslyreportedbyotherauthors[21,22].Nomutation
Malignanthead/neckparagangliomas.ComparativeStudy 165
wasidentifiedinthe remaining3patients. Notethat four patientsofthebenignPGgrouppresentedSDH-Bmutation withnosignsmalignancyduringfollow-up.
Demonstration of an SDH-Bgenemutation ina patient withheadandneckPGthereforeappearstoconstitutethe mostrelevantriskfactorformalignancy,justifying radiologi-calwork-up,especiallywhentheotherriskfactorsdescribed abovearealsopresent:youngsubject,multiplesites, par-ticularlycarotid,possiblysecreting,withafamilyhistoryof PG.
The free interval between diagnosis of the primary tumour and metastases can be long and therefore justi-fieslong-term follow-up, especiallyfor high-risk patients. Althoughthe5-yearoverallsurvivalreportedinthe litera-tureforphaeochromocytomasandmalignantPGrangesfrom 40%to74%[5,7,9],theindividualprognosisisunpredictable. Inourstudy,allpatientsofthemalignantPGgroup(group 2)werealiveatlastfollow-up(withafollow-upofupto29 years),exceptforonepatient(with SDH-Bmutation). Ina seriesof5patients,Havekesetal.[14]describedthecase of a patient whodied after a follow-up of 32 years: this woman with SDH-D mutation developed multiple cervical lymphnodeandbonemetastases.
Surgery is theoretically the only curative treatment for metastases of malignant PG. However, the treatment optionsformetastasesdepend ontheirsiteandtheir ope-rability.Surgeryisclearlyindicatedinthecaseofisolated or multiple lymph node metastases, in the neck, chest or abdomen, especiallyas surgeryalso allowshistological confirmationofmalignancy.Similarly,isolatedliver metas-tases can be treated by resection, sometimes allowing long-termsurvival.
However,two-thirdsofmetastasesinvolveboneandare usuallyvertebraland thereforeunresectable. Acombined medicalandsurgicalapproachisindicated inthesecases: analgesicsandanti-inflammatorydrugstocontrolpainand nervecompression,butalsobisphosphonatesandlocalized radiotherapyorsometimesembolizationandradiofrequency ablation[23,24].Surgicaldecompressionfollowedby verte-broplastycanbeproposedinthepresenceofsignsofspinal cordcompression.
Anotherattractivetreatmentoptionismetabolic radio-therapy based on the property of paraganglionic cells to express somatostatinreceptors ontheir cell surface.This modalityusesa markerlabelled withahighly radioactive agent such as131I-MIBG or 90Ytrium- or 111Indium-labelled
octreotide.However,inpractice,thistypeoftreatmentis limitedbythefactthatalmostone-halfofPGmetastasesdo nottakeupthetracerandone-thirdofpotentialcandidates forthistherapyfailtorespond[25].Thistreatmentisalso veryexpensiveandtheresultsofmetabolicradiotherapyfor metastasesof tympanojugularPGhave notbeen reported todate. Theonlypublishedstudiesconcernmetastasesof phaeochromocytomas[7,25—27].
Randomized trials of chemotherapy are methodologi-callydifficulttoperform,buttheadditionofchemotherapy appearedtoprovideimprovementofsymptomsand short-termremissionsinsomestudiesbasedonsmallsamplesizes
[26,27].
Targeted molecular therapy remains a promising approach, basedonthe principleofthemolecular effects of SDH-B gene mutations, resulting in activation (or
deregulation) of genes targeted by hypoxia-induced fac-tors.Targetedmoleculartherapies arethereforedesigned to inhibit these genes. Sunitinib, an oral multi-target tyrosinekinasereceptorinhibitorwithanti-angiogenicand antitumouractivity,hasbeen recentlyusedin somecases withpromisingresults[28].
Conclusion
Thisretrospectivestudyindicatesthefollowingconclusions:
• malignantparagangliomas areobservedmorefrequently among young patients with multifocal and secreting tumours,particularly,incarotidsites;
• malignantheadandneckparagangliomasaremainly asso-ciatedwithmutationoftheBsubunitoftheSDHgene,but amutationoftheDsubunitissometimesobserved;
• stagingof high-risk patients must include spine MRI, as Octreoscanfailstodetectallmetastases;
• puretympanicformsarenevermalignantanddonot jus-tifygenetictestingorstaging;
• metastases generally present a low rate of progression andarecompatiblewithoftenprolongedsurvival;
• treatmentofmetastasesmustbeadaptedtosymptoms.
Disclosure
of
interest
Theauthorsdeclarethattheyhavenoconflictsofinterest concerningthisarticle.
References
[1]DelellisRLR,HeitzP,EngC,editors.WorldHealthOrganization ClassificationofTumors.Pathologyandgeneticsoftumorsof endocrineorgans.Lyon,France:JARCPress;2004.
[2]LackE.Tumorsoftheadrenalglandsandextraadrenal para-ganglia.In:PressSSA,editor.AFIPAtlasoftumorpathology. 2007.
[3]DelellisR,LloydR,HeitzP,etal.WorldHealthOrganization ClassificationofTumors.In:Pathologyangeneticsoftumorsof endocrineorgans.Lyon,France:JARCPress;2004.
[4]LeeJH,BarichF,KarnellLH,etal.NationalCancerDataBase report onmalignant paragangliomas of the headand neck. Cancer2002;94:730—7.
[5]BaysalBE,FerrellRE,Willett-BrozickJE, etal.Mutationsin SDHD,amitochondrialcomplexIIgene,inhereditary paragan-glioma.Science2000;287:848—51.
[6]Gimenez-Roqueplo AP, Burnichon N, Amar L, et al. Recent advances in the genetics of phaeochromocytoma and functional paraganglioma. Clin Exp Pharmacol Physiol 2008;35:376—9.
[7]Chrisoulidou A, Kaltsas G, Ilias I, et al. The diagnosis and managementofmalignantphaeochromocytomaand paragan-glioma.EndocrRelatCancer2007;14:569—85.
[8]AmarL,BaudinE,BurnichonN,etal.Succinatedehydrogenase B gene mutations predict survival in patients with malig-nantpheochromocytomasorparagangliomas.JClinEndocrinol Metab2007;92:3822—8.
[9]ManolidisS,ShohetJA,JacksonCG,etal.Malignantglomus tumors.Laryngoscope1999;109:30—4.
[10]Zelinka T, Timmers HJ, Kozupa A, et al. Role of positron emissiontomographyandbonescintigraphyintheevaluation of bone involvement in metastatic pheochromocytoma and
paraganglioma:specificimplicationsforsuccinate dehydroge-naseenzymesubunitBgenemutations.EndocrRelatCancer 2008;15:311—23.
[11]Ayala-Ramirez M, Feng L, Johnson MM, et al. Clinical risk factors for malignancy and overallsurvival inpatients with pheochromocytomasandsympatheticparagangliomas:primary tumorsizeandprimarytumorlocationasprognosticindicators. JClinEndocrinolMetab2011;96:717—25.
[12]Duet M, Sauvaget E, Petelle B, et al. Clinical impact of somatostatinreceptorscintigraphyinthemanagementof para-gangliomasoftheheadandneck.JNuclMed2003;44:1767—74. [13]Timmers HJ, Kozupa A, Chen CC, et al. Superiority of fluorodeoxyglucose positron emission tomography to other functionalimagingtechniquesintheevaluationofmetastatic SDHB-associatedpheochromocytomaandparaganglioma.JClin Oncol2007;25:2262—9.
[14]HavekesB,LaiEW,CorssmitEP,etal.Detectionandtreatment ofpheochromocytomasandparagangliomas:currentstanding ofMIBGscintigraphyandfutureroleofPETimaging.QJNucl MedMolImaging2008;52:419—29.
[15]Mamede M, Carrasquillo JA, Chen CC, et al. Discord-ant localization of 2-[18F]-fluoro-2-deoxy-D-glucose in 6-[18F]-fluorodopamine-and [(123)I]-metaiodobenzylguanidine-negative metastatic pheochromocytoma sites. Nucl Med Commun2006;27:31—6.
[16]HoegerleS,GhanemN,AltehoeferC,etal.18F-DOPApositron emissiontomographyforthedetectionofglomustumours.Eur JNuclMedMolImaging2003;30:689—94.
[17]EisenhoferG,LendersJW,SiegertG,etal.Plasma methoxy-tyramine:anovelbiomarkerofmetastaticpheochromocytoma and paraganglioma in relationto establishedrisk factorsof tumoursize,locationandSDHBmutationstatus.EurJCancer 2012;48:1739—49.
[18]BaysalBE.Clinicalandmolecularprogressinhereditary para-ganglioma.JMedGenet2008;45:689—94.
[19]Burnichon N, Rohmer V, Amar L, et al. The succinate dehydrogenase genetictesting ina large prospective series of patients with paragangliomas. J Clin Endocrinol Metab 2009;94:2817—27.
[20]Timmers HJ, Kozupa A, Eisenhofer G, et al. Clinical pre-sentations,biochemicalphenotypes,andgenotype-phenotype correlationsinpatientswithsuccinatedehydrogenasesubunit B-associatedpheochromocytomasandparagangliomas.JClin EndocrinolMetab2007;92:779—86.
[21]HavekesB,CorssmitEP,JansenJC,etal.Malignant paragan-gliomasassociatedwithmutationsinthesuccinate dehydroge-naseDgene.JClinEndocrinolMetab2007;92:1245—8. [22]TimmersHJ,PacakK,BertheratJ,etal.Mutationsassociated
withsuccinatedehydrogenase D-relatedmalignant paragan-gliomas.ClinEndocrinol2008;68:561—6.
[23]WhiteBD, StirlingAJ,PatersonE,etal.Diagnosisand man-agement of patients at risk of or with metastatic spinal cordcompression:summaryofNICEguidance.BMJ2008;337: a2538.
[24]WilkinsonAN,ViolaR,BrundageMD.Managingskeletalrelated eventsresultingfrombonemetastases.BMJ2008;337:a2041. [25]PlouinPF,FitzgeraldP,RichT,etal.Metastatic
pheochromocy-tomaandparaganglioma:focusontherapeutics.HormMetab Res2012;44:390—9.
[26]HuangH,AbrahamJ,HungE,etal.Treatmentofmalignant pheochromocytoma/paraganglioma with cyclophosphamide, vincristine,anddacarbazine:recommendationfroma22-year follow-upof18patients.Cancer2008;113:2020—8.
[27]ScholzT,EisenhoferG,PacakK,etal.Clinicalreview:Current treatmentofmalignantpheochromocytoma.JClinEndocrinol Metab2007;92:1217—25.
[28]Joshua AM, Ezzat S, Asa SL, et al. Rationale and evi-dence for sunitinib in the treatment of malignant para-ganglioma/pheochromocytoma. J Clin Endocrinol Metab 2009;94:5—9.