Treating Co-Occurring Axis I Disorders in Recurrently Suicidal Women
With Borderline Personality Disorder: A 2-Year Randomized Trial of
Dialectical Behavior Therapy Versus Community Treatment by Experts
Melanie S. Harned
University of WashingtonAlexander L. Chapman
Simon Fraser UniversityElizabeth T. Dexter-Mazza, Angela Murray, Katherine A. Comtois, and Marsha M. Linehan
University of WashingtonThis study evaluated whether dialectical behavior therapy (DBT) was more efficacious than treatment by nonbehavioral psychotherapy experts in reducing co-occurring Axis I disorders among suicidal individ-uals with borderline personality disorder (BPD). Women with BPD and recent and repeated suicidal
and/or self-injurious behavior (n ⫽101) were randomly assigned to 1 year of DBT or community
treatment by experts (CTBE), plus 1 year of follow-up assessment. For substance dependence disorders (SDD), DBT patients were more likely to achieve full remission, spent more time in partial remission, spent less time meeting full criteria, and reported more drug- and alcohol-abstinent days than did CTBE patients. These findings suggest that improvements in co-occurring SDD among suicidal BPD patients are specific to DBT and cannot be attributed to general factors associated with nonbehavioral expert psychotherapy. Further, group differences in SDD remission were not explained by either psychotropic medication usage or changes in BPD criterion behaviors. DBT and CTBE did not significantly differ in the reduction of anxiety disorders, eating disorders, or major depressive disorder.
Keywords:dialectical behavior therapy, borderline personality disorder, suicidal behavior, comorbidity
Numerous studies have documented high rates of co-occurring Axis I disorders among individuals who meet criteria for border-line personality disorder (BPD), particularly for major depressive disorder (MDD; 61%– 87%), substance use disorders (SUD; 14%– 62%), posttraumatic stress disorder (PTSD; 36%–58%), panic disorder (29%– 45%), and eating disorders (ED; 17%–54%; Line-han et al., 2006; Zanarini, Frankenburg, Hennen, Reich, & Silk, 2004; Zimmerman & Mattia, 1999). Patients with BPD also have more co-occurring Axis I disorders than do other diagnostic groups (e.g., Zimmerman & Mattia, 1999), and these disorders are chronic and persistent (Zanarini et al., 2004). Furthermore, the presence of
co-occurring Axis I disorders, particularly SUD and PTSD, de-creases the likelihood of attaining remission from BPD (Zanarini et al., 2004).
Given these findings, treatments for BPD must not only address the behaviors considered central to the disorder (e.g., suicide attempts and nonsuicidal self-injury [NSSI]) but must manage the difficulties associated with multiple Axis I disorders. Dialectical behavior therapy (DBT; Linehan, 1993) is a comprehensive cognitive– behavioral treatment with considerable evidence for its efficacy in treating BPD (for a review, see Lynch, Trost, Salsman, & Linehan, 2007). Although several studies have found that DBT decreases behaviors associated with Axis I disorders, such as substance use (Linehan et al., 1999, 2002), bingeing/purging (Safer, Telch, & Agras, 2001; Telch, Agras, & Linehan, 2001), depression (Koons et al., 2001; Linehan, Armstrong, Suarez, Allmon, & Heard, 1991; Linehan et al., 2006), and anxiety (Koons et al., 2001), no studies have examined whether DBT leads to remission of co-occurring Axis I disorders among patients with BPD.
The present study is part of a larger program of research com-paring DBT with a rigorous control condition (community treat-ment by experts, or CTBE) designed to control for potential threats to internal validity (e.g., expertise, allegiance). Findings from the main outcome study indicate that DBT has unique effects that extend beyond those of general nonbehavioral expert therapy in reducing suicide attempts, medical severity of suicide attempts and NSSI acts, use of crisis services, inpatient hospitalizations, and treatment dropout (Linehan et al., 2006). In the present study, we Melanie S. Harned, Elizabeth T. Dexter-Mazza, Angela Murray, and
Marsha M. Linehan, Department of Psychology, University of Washing-ton; Katherine A. Comtois, Department of Psychiatry, University of Wash-ington; Alexander L. Chapman, Department of Psychology, Simon Fraser University, Burnaby, British Columbia, Canada.
This study was supported by National Institute of Mental Health Grants MH34486 and MH01593 to Marsha M. Linehan. Portions of this paper were presented at the 40th Annual Convention of the Association for Behavioral and Cognitive Therapies, Chicago, Illinois, November 2006. We thank the clients, therapists, assessors, and staff at the Behavioral Research and Therapy Clinics, without whom this research would not have been possible. We also thank Robert Gallop for providing statistical con-sultation on this article.
Correspondence concerning this article should be addressed to Melanie S. Harned, Behavioral Research and Therapy Clinics, Department of Psy-chology, Box 351525, University of Washington, Seattle, WA 98195-1525. E-mail: [email protected]
used data from the Linehan et al. (2006) study to examine the efficacy of DBT versus CTBE in treating co-occurring Axis I disorders among suicidal BPD patients. Because patients in DBT reported fewer BPD criterion behaviors (i.e., suicide attempts) and less psychotropic medication use during the study than did CTBE patients (Linehan et al., 2006), we also examined whether these variables explained any significant group differences in Axis I disorder remission. Given the exploratory nature of this study, we did not make specific hypotheses.
Method
Participants
Participants were 101 women (age 18 – 45) who met criteria for BPD and reported at least two suicide attempts and/or NSSI acts in the past 5 years, with at least one act in the 8-week prestudy period. Exclusion criteria were (a) schizophrenia, schizoaffective disorder, bipolar disorder, psychotic disorder not otherwise spec-ified, or mental retardation; (b) a seizure disorder requiring med-ication; (c) a mandate to treatment; or (d) the need for primary
treatment for another debilitating condition. All participants pro-vided informed consent, and all protocols were approved by the University of Washington Human Subjects Division. No adverse events occurred.1
Procedures
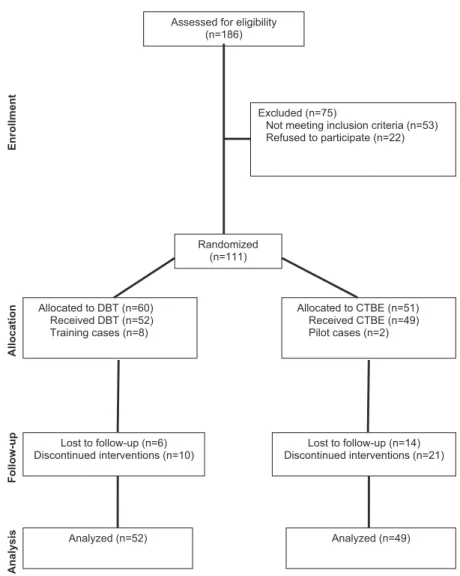
Participants were randomly assigned to condition by the partic-ipant coordinator, who used a computerized adaptive minimization randomization procedure that matched participants on five primary prognostic variables (see Linehan et al., 2006). On the basis of 0.8 power to detect significant differences (p⫽.05, one-sided), 101 participants were randomized to DBT (n⫽52) or CTBE (n⫽49; see Figure 1). The periods of enrollment and follow-up ran from October 1994 through August 2003. Baseline assessments were
1Given the inclusion criteria for this study, suicide attempts and NSSI
were not considered to be unexpected adverse events. All criteria for adverse event reporting were approved by the University of Washington Human Subjects Division.
Assessed for eligibility (n=186)
Excluded (n=75)
Not meeting inclusion criteria (n=53) Refused to participate (n=22) Randomized (n=111) Allocated to DBT (n=60) Received DBT (n=52) Training cases (n=8) Allocated to CTBE (n=51) Received CTBE (n=49) Pilot cases (n=2) Lost to follow-up (n=6) Discontinued interventions (n=10) Lost to follow-up (n=14) Discontinued interventions (n=21) Analyzed (n=52) Analyzed (n=49) Analysis Enrollment Allocation Follow-up
Figure 1. Participant flowchart. DBT ⫽ dialectical behavior therapy; CTBE ⫽community treatment by experts.
made before participants were informed of their treatment assign-ment, and outcome assessments occurred at 4-month intervals through the 1-year treatment and 1-year follow-up period. Assess-ments were conducted by blinded, independent clinical assessors. They were trained on interview measures by the instrument devel-opers or an approved trainer and were then evaluated for reliability (kappa or intraclass correlation coefficient for all diagnostic rat-ings ranged between 0.74 and 1.0).
Treatment Conditions
DBT. DBT is a cognitive– behavioral treatment for suicidal individuals who meet criteria for BPD. DBT targets, in hierarchi-cal order, life-threatening behaviors (e.g., suicide attempts and NSSI), behaviors that interfere with treatment delivery (e.g., non-compliance), and severe quality of life interfering behaviors (e.g., severe Axis I disorders). DBT consists of (a) weekly individual psychotherapy (1 hr/wk); (b) group skills training (2.5 hr/wk); (c)
phone consultation (as needed); and (d) weekly therapist consul-tation team meeting.
CTBE. The CTBE condition was developed to control for expertise, treatment allegiance, availability of a clinical supervi-sion group, prestige, general factors and assistance in finding a therapist, availability of affordable and sufficient treatment hours, and therapist gender, training, and clinical experience. Community mental health leaders nominated CTBE therapists as experts in the treatment of difficult patients. We excluded CTBE therapists who self-identified as cognitive or behavioral in orientation.
Assessment Measures
BPD at pretreatment was diagnosed with the Structured Clinical Interview for DSM–III–RPersonality Disorders (SCID–II; First, Spitzer, Gibbon, & Williams, 1995b) and the International Person-ality Disorders Examination (Loranger, 1995). The SCID–II was readministered at the 24-month point. The SCID–I (First, Spitzer,
Table 1
Pretreatment Demographic and Diagnostic Data for DBT and CTBE
Variable DBT (n⫽52) CTBE (n⫽49) Total
Age (M⫾SD) 29.0⫾7.3 29.6⫾7.8 29.3⫾7.5
Race (%)
African American 3.8 4.1 4.0
Asian American 1.9 2.0 2.0
Native American or Alaskan Native 1.9 0 1.0
Other 5.8 6.1 5.0
White 86.5 87.8 87.0
Single, divorced, or separated (%) 88.4 85.7 87.2
Education (%)
⬍High school 9.6 6.1 7.9
High school graduate or GED 15.4 18.4 16.8
Some college or technical school 50.0 53.1 51.5
College graduate 25.0 22.4 23.8
Annual income (%)
⬍$15,000 75.0 75.5 75.2
$15,000–$30,000 13.4 8.2 10.9
⬎$30,000 9.6 10.2 9.9
Lifetime Axis I psychiatric diagnoses (%)a
MDD 94 98 96
Panic disorder 48 55 52
PTSD 60 51 55
Any other anxiety disorderb 52 51 51
Any SUDc 79 67 73
Any EDd 44 35 40
Current Axis I psychiatric diagnoses (%)a
MDD 71 74 72
Panic disorder 42 39 41
PTSD 50 49 50
Any other anxiety disorderb 42 39 41
Any SUDc 23 37 30
Any EDd 25 22 24
Total no. lifetime Axis I diagnoses (M⫾SD) 4.21⫾1.64 4.26⫾1.83 4.24⫾1.73
Total no. current Axis I diagnoses (M⫾SD) 2.81⫾1.33 3.20⫾1.96 3.00⫾1.67
Note. No between-groups differences were statistically significant. Analyses were conducted with thettest,
Mann–Whitney test, and chi-square test, as appropriate. DBT ⫽ dialectical behavior therapy; CTBE ⫽
community treatment by experts; GED⫽general equivalency diploma; MDD⫽major depressive disorder;
PSTD⫽posttraumatic stress disorder; SUD⫽substance use disorders; ED⫽eating disorders.
aThe first 8 participants who entered the study metDSM–III–R criteria. All other subjects met DSM–IV
criteria. bIncludes generalized anxiety disorder, agoraphobia without panic disorder, social phobia, specific
phobias, and obsessive-compulsive disorder. cIncludes substance abuse disorders and substance dependence
Gibbon, & Williams, 1995a) assessed Axis I diagnoses at pretreat-ment. The Treatment History Interview (Linehan & Heard, 1987) assessed psychotropic medications at each assessment period. The Longitudinal Interval Follow-Up Evaluation (LIFE; Keller et al., 1987) is a semistructured interview that we used to gather retro-spective ratings of Axis I disorders for each week of the study (i.e., 104 weeks). Using a time line follow-back procedure, we assigned weekly psychological status ratings (PSRs) for each disorder iden-tified at pretreatment via the SCID–I. PSRs range from 1 to 6 for MDD (1⫽usual self,2⫽residual,3⫽partial remission,4⫽
marked,5⫽ definite criteria,6⫽definite criteria, severe) and from 1 to 3 for all other diagnoses (1⫽none,2⫽moderate,3⫽
severe). High interviewer– observer reliability has been shown for the change points in diagnostic criteria as well as for the level of psychopathology (Keller et al., 1987).
For substance dependence disorders (SDD), we used the remis-sion criteria from theDiagnostic and Statistical Manual of Mental Disorders(4th ed., text rev.;DSM–IV–TR; American Psychiatric Association, 2000): (a) early partial remission (PSR ⫽ 2 for at least 4 weeks) and (b) early full remission (PSR⫽1 for at least 4 weeks). Given the absence ofDSM–IV–TRremission criteria for mood, anxiety, and ED, we followed conventions for the LIFE and defined full remission as at least 8 consecutive weeks with mini-mal or no symptoms (for MDD, PSRⱕ2; for all others, PSR⫽ 1), and partial remission as at least 8 consecutive weeks with subthreshold symptoms (for MDD, PSR ⫽ 3– 4; for all others,
PSR⫽2). For all disorders, relapse was defined as meeting full criteria for a disorder after having achieved full remission.
Statistical Methods
Group comparisons were conducted on the intent-to-treat sam-ple using t tests for continuous variables and chi-squares and Fisher’s exact tests for categorical variables. Cohen’s d and w
effect sizes (with 95% confidence intervals) were calculated. Kaplan–Meier and Cox regression survival analyses examined the time to first full remission. Because few participants met criteria for certain diagnoses, we created the following combined catego-ries: (a) any anxiety disorder other than PTSD and panic disorder (i.e., generalized anxiety disorder, n ⫽ 3; agoraphobia without panic disorder,n⫽3; social phobia,n⫽16; specific phobia,n⫽
10; obsessive-compulsive disorder,n⫽ 16); (b) any SDD (i.e., alcohol,n⫽8; cannabis,n⫽5; cocaine,n⫽4; stimulants,n⫽
1); and (c) any ED (i.e., bulimia nervosa,n⫽8; anorexia nervosa,
n⫽3; binge disorder,n⫽4).
Results
Sample Characteristics and Baseline Differences
The treatment groups did not differ significantly on any demo-graphic characteristics or in rates of lifetime or current Axis I diagnoses at pretreatment (see Table 1).
Table 3
Group Comparisons of Rates of Full Remission
Group
Full remission No full remission Effect size
DBT (%) CTBE (%) DBT (%) CTBE (%) 2(1) p w 95% CI
MDD (n⫽59) 67.6 48.0 32.4 52.0 2.30 .13 0.20 ⫺0.05, 0.45
Panic disorder (n⫽32) 47.4 53.8 52.6 46.2 0.13 .72 0.06 ⫺0.28, 0.41
PTSD (n⫽40) 34.8 23.5 65.2 76.5 0.59 .44 0.12 ⫺0.18, 0.42
Other anxiety disorders (n⫽35) 38.9 47.1 61.1 52.9 0.24 .62 0.08 ⫺0.25, 0.41
SDD (n⫽17) 87.5 33.3 12.5 66.7 5.13 .02 0.55 0.17, 0.93
ED (n⫽15) 63.6 50.0 36.4 50.0 0.23 .64 0.12 ⫺0.39, 0.63
All disorders combined (n⫽82)a 73.9 66.7 26.1 33.3 0.51 .47 0.08 ⫺0.14, 0.30
Note. For Cohen’sw,small effect⫽0.1, medium effect⫽0.3, large effect⫽0.5. DBT⫽dialectical behavior therapy; CTBE⫽community treatment
by experts; CI⫽confidence interval; MDD⫽major depressive disorder; PSTD⫽posttraumatic stress disorder; SDD⫽substance dependence disorders;
ED⫽eating disorders.
aFor the all disorders combined category, full remission⫽achieved full remission from at least one disorder, no full remission⫽did not achieve full
remission from any disorder. Table 2
Group Comparisons of the Proportion of Total Axis I Disorders per Patient Reaching Full Remission or Relapsing
Outcome
DBT CTBE
M SD M SD t p d(95% CI)
Proportion of Axis I disorders reaching full
remission 0.55 0.41 0.47 0.40 0.84 .40 0.20 (⫺0.24, 0.63)
Proportion of fully remitted Axis I
disorders that later relapsed 0.41 0.45 0.42 0.48 0.02 .98 0.02 (⫺0.50, 0.54)
Note. For Cohen’sd, small effect⫽0.2, medium effect⫽0.5, large effect⫽0.8. DBT⫽dialectical behavior
Remission and Relapse for Co-Occurring Axis I Disorders
Overall, DBT and CTBE patients did not significantly differ in the proportion of Axis I disorders that reached full remission or that subsequently relapsed (see Table 2). For specific Axis I disorders, DBT patients were significantly more likely to achieve full remission from SDD than were CTBE patients (see Table 3). In addition, DBT patients spent significantly more time in partial remission and less time in no remission from SDD than did CTBE patients (see Table 4). No other significant differences in rates of full remission or the proportion of time spent in different levels of remission were found for any other Axis I disorder. Survival analyses of the time to the first full remission did not indicate significant differences between treat-ments for any Axis I disorder (see Table 5). Similarly, DBT patients and CTBE patients did not significantly differ in rates of relapse for any Axis I disorder (see Table 6).
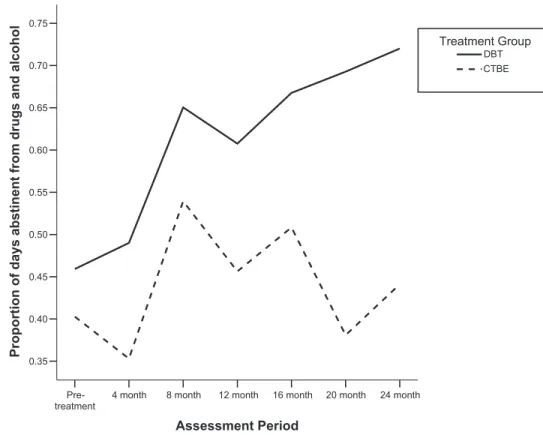
To validate the significant findings for SDD remission, we exam-ined the proportion of days abstinent from drugs and alcohol during treatment and follow-up measured via the time line follow-back procedure (Sobell, Sobell, Klajner, Pavan, & Basian, 1986). DBT patients with SDD reported a significantly greater proportion of drug-and alcohol-abstinent days across time than did CTBE patients with SDD (see Figure 2). Also, DBT and CTBE patients with SDD did not significantly differ in the number of BPD criteria met or in use of psychotropic medication (see Table 7).
Discussion
The present study indicates that DBT is superior to CTBE in treating co-occurring SDD among suicidal BPD patients. These findings are particularly important, given that SDD is the only Axis I disorder associated with an increased risk of completed suicide in patients with BPD (McGirr, Paris, Lesage, Renaud, & Turecki, 2007). Compared with CTBE patients, DBT patients were more than two and half times as likely to achieve full remission from SDD (87.5% vs. 33.3%) and spent proportionally more time in partial remission and less time in meeting full criteria for SDD. DBT patients with SDD also reported more drug- and alcohol-abstinent days across time than did CTBE patients with SDD.
The superiority of DBT in decreasing SDD among patients with BPD does not appear to be attributable to differences in BPD criterion behaviors or to psychotropic medication usage between treatment groups.2Several aspects of DBT may account for these findings: (a) DBT targets substance use directly (via self-monitoring, behavioral analyses, and problem-solving strategies) rather than indirectly (via other, related problems); (b) several DBT skills (e.g., mindfulness) are similar to those used in evidence-based SUD treatments (e.g., Marlatt & Donovan, 2005); and (c) specific attention has been paid to adapt-ing DBT to treat co-occurradapt-ing SUD in patients with BPD (Linehan & Dimeff, 1997). The present findings are consistent with those of studies indicating that DBT is an efficacious treatment for substance use behaviors among patients with BPD (Linehan et al., 1999, 2002). They add to this literature by showing that these outcomes extend to include remission from SDD, are generalizable to recurrently suicidal
2Although DBT and CTBE patients with SDD did not significantly
differ in their use of psychotropic medications across time, there was a
notable trend (d⫽0.79) indicating that DBT patients with SDD were less
likely to use psychotropic medication than were CTBE patients with SDD.
Table 4 Group Comparisons of the Proportion of Time Spent at Different Levels of Remission Group Full remission Partial remission No remission DBT M( SD ) CTBE M( SD ) td (95% CI) DBT M( SD ) CTBE M( SD ) td (95% CI) DBT M( SD ) CTBE M( SD ) td (95% CI) MDD ( n ⫽ 59) 0.24 (0.25) 0.16 (0.23) 1.29 0.33 ( ⫺ 0.19, 0.85) 0.22 (0.20) 0.20 (0.18) 0.52 0.10 ( ⫺ 0.41, 0.62) 0.54 (0.29) 0.65 (0.29) 1.43 0.38 ( ⫺ 0.15, 0.89) Panic disorder ( n ⫽ 32) 0.12 (0.21) 0.17 (0.24) 0.58 0.22 ( ⫺ 0.49, 0.93) 0.22 (0.22) 0.18 (0.19) 0.43 0.19 ( ⫺ 0.52, 0.89) 0.66 (0.31) 0.64 (0.30) 0.13 0.07 ( ⫺ 0.64, 0.77) PTSD ( n ⫽ 40) 0.12 (0.21) 0.13 (0.26) 0.08 0.04 ( ⫺ 0.58, 0.67) 0.25 (0.26) 0.13 (0.16) 1.68 0.54 ( ⫺ 0.11, 1.16) 0.63 (0.31) 0.74 (0.29) 1.18 0.36 ( ⫺ 0.27, 0.99) Other anxiety disorders ( n ⫽ 35) 0.21 (0.30) 0.12 (0.17) 1.12 0.37 ( ⫺ 0.31, 1.03) 0.22 (0.28) 0.21 (0.27) 0.08 0.04 ( ⫺ 0.63, 0.70) 0.57 (0.34) 0.67 (0.36) 0.85 0.29 ( ⫺ 0.39, 0.95) SDD ( n ⫽ 17) 0.41 (0.31) 0.18 (0.32) 1.48 0.73 ( ⫺ 0.29, 1.67) 0.18 (0.22) 0.02 (0.06) 2.08 ⴱ 1.02 ( ⫺ 0.04, 1.98) 0.41 (0.36) 0.80 (0.32) 2.36 ⴱ 1.15 (0.07, 2.11) ED ( n ⫽ 15) 0.27 (0.23) 0.27 (0.34) 0.02 0.00 ( ⫺ 1.14, 1.14) 0.20 (0.18) 0.10 (0.08) 1.04 0.62 ( ⫺ 0.58, 1.74) 0.53 (0.32) 0.63 (0.40) 0.48 0.29 ( ⫺ 0.87, 1.43) All disorders combined ( n ⫽ 82) 0.21 (0.20) 0.17 (0.20) 0.89 0.20 ( ⫺ 0.24, 0.64) 0.24 (0.20) 0.18 (0.16) 1.47 0.33 ( ⫺ 0.12, 0.76) 0.55 (0.25) 0.65 (0.27) 1.69 0.39 ( ⫺ 0.06, 0.82) Note. For Cohen’s d, small effect ⫽ 0.2, medium effect ⫽ 0.5, large effect ⫽ 0.8. DBT ⫽ dialectical behavior therapy; CTBE ⫽ community treatment by experts; CI ⫽ confidence interval; MDD ⫽ major depressive disorder; PSTD ⫽ posttraumatic stress disorder; SDD ⫽ substance dependence disorders; ED ⫽ eating disorders. ⴱp ⬍ .05.
BPD patients, and are not attributable to general nonbehavioral expert therapy.
The lack of significant differences between DBT and CTBE for other Axis I disorders suggests that general factors associated with expert therapy may account for reductions in these disorders. This explanation is consistent with previous studies that have indicated DBT is comparable with control conditions in reducing the severity of depression and anxiety among patients with BPD (Koons et al., 2001; Linehan et al., 1991, 2006). Alternatively, given that many of the comparisons yielded moderate-to-large effect sizes generally in favor of DBT, the lack of significant differences may be due to inadequate power. This possibility is consistent with previous studies that have found DBT to be superior to control conditions in reducing depression (Koons et al., 2001) and ED behaviors (Safer et al., 2001; Telch et al., 2001).
Overall, 74% of DBT patients and 67% of CTBE patients achieved full remission from at least one Axis I disorder, and patients in both treatments fully remitted from approximately 50%
of their co-occurring Axis I disorders. These overall remission rates are notably high, particularly given the severity of the patient population. Although comparisons with other treatments are difficult due to varying definitions of remission, these rates, particularly for DBT, are at least comparable with, if not higher than, those com-monly found in psychological treatments for SDD (54%–71%; Crits-Christoph et al., 1999), MDD (47%–56%; de Mello, Mari, Ba-caltchuk, Verdeli, & Neugebauer, 2005), and ED (50%; Fairburn & Brownell, 2001). Our findings are especially noteworthy, given that BPD typically predicts worse outcome in treatments for these disor-ders (e.g., Darke, Ross, Williamson, & Teeson, 2005; Shea et al., 1990; Wilfley et al., 2000).
In contrast, both DBT and CTBE achieved lower rates of remission from anxiety disorders than treatments for these disorders more gen-erally (e.g., panic disorder⫽80%–100%, Barlow, 2001; PTSD⫽ 56%, Bradley, Greene, Russ, Dutra, & Westen, 2005). Our lower remission rates support previous findings that anxiety disorder treat-ments are less efficacious among individuals with BPD (e.g., Weert-Table 5
Survival Analyses of Treatment Group as a Predictor of Time to First Full Remission
Group
Estimated means for survival time
Hazard ratio 95% CI Wald’s2(1) p
DBTM (SE) CTBEM (SE)
MDD (n⫽59) 63.47 (5.55) 75.37 (6.75) 0.59 0.29, 1.20 2.13 .14
Panic disorder (n⫽32) 78.02 (7.94) 68.88 (10.11) 1.30 0.48, 3.50 0.27 .61
PTSD (n⫽40) 89.13 (4.93) 87.57 (7.62) 0.80 0.24, 2.66 0.13 .72
Other anxiety disorders (n⫽35) 77.87 (8.03) 81.99 (6.12) 1.04 0.38, 2.88 0.01 .94
SDD (n⫽17) 40.75 (10.75) 73.17 (14.15) 0.33 0.08, 1.29 2.52 .11
ED (n⫽15) 69.27 (8.99) 61.75 (21.16) 0.99 0.20, 4.79 0.00 .99
All disorders combined (n⫽82) 71.21 (3.88) 70.86 (4.99) 0.95 0.57, 1.61 0.03 .86
Note. Treatment group (0⫽DBT, 1⫽CTBE) was entered as a predictor of time to first full remission for each Axis I disorder while we controlled for censoring effects. Data from patients who remitted were censored at the week of their first full remission. Data from patients who did not remit were censored at the last week at which
they provided follow-up data. Hazard ratios are interpreted as a measure of effect size as follows: small effect⫽
⬎0.66, medium effect⫽0.40 – 0.66, large effect⫽ ⬍0.40. DBT⫽dialectical behavior therapy; CTBE ⫽
community treatment by experts; CI⫽confidence interval; MDD⫽ major depressive disorder; PSTD ⫽
posttraumatic stress disorder; SDD⫽substance dependence disorders; ED⫽eating disorders.
Table 6
Group Comparisons of Rates of Relapse
Group
Rate of relapse Effect size
DBT (%) CTBE (%) p w 95% CI
MDD (n⫽35) 60.9 41.7 0.28 0.18 ⫺0.14, 0.51
Panic disorder (n⫽16) 22.2 42.9 0.60 0.22 ⫺0.26, 0.70
PTSD (n⫽12) 12.5 25.0 1.00 0.16 ⫺0.44, 0.75
Other anxiety disorders (n⫽15) 14.3 12.5 1.00 0.03 ⫺0.48, 0.53
SDD (n⫽10) 28.6 66.7 0.50 0.36 ⫺0.24, 0.95
ED (n⫽9) 28.6 50.0 1.00 0.19 ⫺0.49, 0.87
All disorders combined (n⫽58)a 52.9 45.8 0.59 0.07 ⫺0.19, 0.33
Note. Only those participants who achieved full remission from the relevant Axis I disorder were included in
these analyses. For Cohen’sw,small effect⫽0.1, medium effect⫽0.3, large effect⫽0.5. Analyses were
conducted with the chi-square test and Fisher’s exact test, as appropriate. DBT⫽dialectical behavior therapy;
CTBE⫽community treatment by experts; CI⫽confidence interval; MDD ⫽major depressive disorder;
PSTD⫽posttraumatic stress disorder; SDD⫽substance dependence disorders; ED⫽eating disorders.
aFor the all disorders combined category, all participants who achieved full remission from any disorder were
man, Arntz, Schouten, & Dreessen, 2005). With severe, multiproblem patients, anxiety disorders may have been a lower treatment priority than suicidal behaviors or other quality of life problems. Indeed, in DBT, PTSD related to childhood abuse is not targeted until the second
stage of treatment (Linehan, 1993). Alternatively, anxiety disorders may be particularly intractable among patients with BPD. One study found that high rates of anxiety disorders persist across time in a largely treatment-seeking BPD sample (Zanarini et al., 2004). Thus,
24 month 20 month 16 month 12 month 8 month 4 month Pre-treatment Assessment Period 0.75 0.70 0.65 0.60 0.55 0.50 0.45 0.40 0.35
Proportion of days abstinent
from drugs and alcohol
CTBE DBT Treatment Group
Figure 2. Proportion of days abstinent from drugs and alcohol among patients with co-occurring substance
dependence disorder (n⫽17). A hierarchical linear model indicated a significant between-groups difference in
the rate of change in drug- and alcohol-abstinent days across time,F(1, 87)⫽7.33,p⫽.008. DBT patients
reported a significant increase in drug- and alcohol-abstinent days across time (slope⫽0.05,SE⫽0.01),t(85)⫽
3.62,p⬍.001, whereas CTBE patients did not improve on this measure (slope⫽ ⫺0.004,SE⫽0.01),t(88)⫽
⫺0.31,p⫽.75. DBT⫽dialectical behavior therapy; CTBE⫽community treatment by experts.
Table 7
Group Comparisons of the Number of BPD Criteria Met and Use of Psychotropic Medications Among Patients With SDD
Variable DBT with SDD (n⫽8) CTBE with SDD (n⫽9) M SD M SD t p d(95% CI)
No. BPD criteria met
Pretreatment 7.37 1.41 7.55 1.13 0.29 .77 0.14 (⫺0.82, 1.09)
Follow-up yeara 4.86 3.02 5.33 2.94 0.29 .78 0.16 (⫺0.95, 1.24)
Use of psychotropic medications 0.48 0.29 0.72 0.31 1.62 .13 0.79 (⫺0.24, 1.73)
Note. Use of psychotropic medications was calculated as the proportion of assessment periods (pretreatment through 24-month follow-up) at which participants reported using any psychotropic medication in the 2 months
prior to the assessment. For Cohen’sd,small effect⫽0.2, medium effect⫽0.5, large effect⫽0.8.BPD⫽
borderline personality disorder; SDD⫽substance dependence disorder; CBTE⫽community treatment by
experts; CI⫽confidence interval.
aThe between-groups difference during the follow-up year remained nonsignificant when the BPD criterion of
impulsive, self-destructive behaviors that can include substance use was excluded (DBT,M⫽4.29,SD⫽2.69;
anxiety disorder treatments may need to address the unique needs of patients with BPD (e.g., Harned & Linehan, 2008).
The primary limitation of this study is a possible lack of power to detect between-groups differences due to small sample sizes for the specific Axis I disorders and primarily dichotomous outcomes. Future studies with larger samples are needed to replicate these findings. In addition, although we validated all significant findings on the LIFE with a secondary measure of a similar outcome, there is a potential risk of Type I error. Finally, further research on mechanisms of action in reducing Axis I disorders among patients with BPD is needed. Despite these limitations, this is the only major clinical trial to have examined the comparative efficacy of two rigorous treatments in reducing co-occurring Axis I disorders among suicidal BPD patients. These data, therefore, should spark future research and treatment development.
References
American Psychiatric Association. (2000).Diagnostic and statistical
man-ual of mental disorders(4th ed., text rev.). Washington, DC: Author.
Barlow, D. H. (2001). Panic disorder. In D. H. Barlow (Ed.),Clinical
handbook of psychological disorders: A step-by-step treatment manual. New York: Guilford Press.
Bradley, R., Greene, J., Russ, E., Dutra, L., & Westen, D. (2005). A
multidimensional meta-analysis of psychotherapy for PTSD.American
Journal of Psychiatry, 162,214 –227.
Crits-Christoph, P., Siqueland, L., Blaine, J., Frank, A., Luborsky, L., Onken, L. S., et al. (1999). Psychosocial treatments for cocaine depen-dence: National Institute on Drug Abuse Collaborative Cocaine
Treat-ment Study.Archives of General Psychiatry, 56,493–502.
Darke, S., Ross, J., Williamson, A., & Teeson, M. (2005). The impact of borderline personality disorder on 12-month outcomes for the treatment
of heroin dependence.Addiction, 100,1121–1130.
de Mello, M. F., Mari, J. J., Bacaltchuk, J., Verdeli, H., & Neugebauer, R. (2005). A systematic review of research findings on the efficacy of
interpersonal therapy for depressive disorders.European Archives of
Psychiatry and Clinical Neuroscience, 255,75– 82.
Fairburn, C. G., & Brownell, K. D. (Eds.) (2001).Eating disorders and
obesity(2nd ed.). New York: Guilford Press.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1995a). Structured Clinical Interview for Axis IDSM–IVDisorders—Patient Edition (SCID–I/P).New York: Biometrics Research Department, New York State Psychiatric Institute.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1995b). The
Structured Clinical Interview for DSM–III–R Personality Disorders
(SCID–II): II. Multisite test–retest reliability study.Journal of
Person-ality Disorders, 9,92–104.
Harned, M. S., & Linehan, M. M. (2008). Integrating dialectical behavior therapy and prolonged exposure to treat co-occurring borderline
person-ality disorder and PTSD: Two case studies.Cognitive and Behavioral
Practice, 15,263–276.
Keller, M. B., Lavori, P. W., Friedman, B., Nielsen, E., Endicott, J., McDonald-Scott, P., & Andreasen, N. C. (1987). The Longitudinal Interval Follow-up Evaluation: A comprehensive method for assessing
outcome in prospective longitudinal studies.Archives of General
Psy-chiatry, 44,540 –548.
Koons, C. R., Robins, C. J., Tweed, J. L., Lynch, T. R., Gonzalez, A. M., Morse, J. Q., et al. (2001). Efficacy of dialectical behavior therapy in women veterans
with borderline personality disorder.Behavior Therapy, 32,371–390.
Linehan, M. M. (1993). Cognitive– behavioral treatment of borderline
personality disorder.New York: Guilford Press.
Linehan, M. M., Armstrong, H. E., Suarez, A., Allmon, D., & Heard, H. L.
(1991). Cognitive– behavioral treatment of chronically parasuicidal
bor-derline clients.Archives of General Psychiatry, 48,1060 –1064.
Linehan, M. M., Comtois, K. A., Murray, A. M., Brown, M. Z., Gallop, R. J., Heard, H. L., et al. (2006). Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs. therapy by experts for
suicidal behaviors and borderline personality disorder.Archives of
Gen-eral Psychiatry, 63,757–766.
Linehan, M. M., & Dimeff, L. A. (1997).Dialectical behavior therapy for
substance abuse treatment manual.Unpublished manuscript, University of Washington, Seattle.
Linehan, M. M., Dimeff, L. A., Reynolds, S. K., Comtois, K. A., Welch, S. S., Heagerty, P., & Kivlahan, D. R. (2002). Dialectical behavior therapy versus comprehensive validation therapy plus 12-step for the treatment of opioid dependent women meeting criteria for borderline
personality disorder.Drug and Alcohol Dependence, 67,13–26.
Linehan, M. M., & Heard, H. L. (1987). Treatment History Interview
(THI).Unpublished manuscript, University of Washington, Seattle. Linehan, M. M., Schmidt, H. I., Dimeff, L. A., Craft, J. C., Kanter, J., &
Comtois, K. A. (1999). Dialectical behavior therapy for patients with
borderline personality disorder and drug dependence.American Journal
on Addictions, 8,279 –292.
Loranger, A. W. (1995).International Personality Disorder Examination
(IPDE) manual.White Plains, NY: Cornell Medical Center.
Lynch, T. R., Trost, W. T., Salsman, N., & Linehan, M. M. (2007).
Dialectical behavior therapy for borderline personality disorder.Annual
Review of Clinical Psychology, 3,181–205.
Marlatt, G. A., & Donovan, D. M. (2005).Relapse prevention:
Mainte-nance strategies in the treatment of addictive behaviors(2nd ed.). New York: Guilford Press.
McGirr, A., Paris, J., Lesage, A., Renaud, J., & Turecki, G. (2007). Risk factors for suicide completion in borderline personality disorder: A case-control study of cluster B comorbidity and impulsive aggression. Journal of Clinical Psychiatry, 68,721–729.
Safer, D. L., Telch, C. F., & Agras, W. S. (2001). Dialectical behavior
therapy for bulimia nervosa. American Journal of Psychiatry, 158,
632– 634.
Shea, M. T., Pilkonis, P. A., Beckham, E., Collins, J. F., Elkin, I., Sotsky, S. M., & Docherty, J. P. (1990). Personality disorders and treatment outcome in the NIMH Treatment of Depression Collaborative Research
Program.American Journal of Psychiatry, 147,711–718.
Sobell, M. B., Sobell, L. C., Klajner, F., Pavan, D., & Basian, E. (1986). The reliability of a timeline method for assessing normal drinker college
students’ recent drinking history: Utility for alcohol research.Addictive
Behaviors, 11,149 –161.
Telch, C. F., Agras, W. S., & Linehan, M. M. (2001). Dialectical behavior
therapy for binge eating disorder.Journal of Consulting and Clinical
Psychology, 69,1061–1065.
Weertman, A., Arntz, A., Schouten, E., & Dreessen, L. (2005). Influences of beliefs and personality disorders on treatment outcome in anxiety
patients.Journal of Consulting and Clinical Psychology, 73,936 –944.
Wilfley, D. E., Friedman, M. A., Douchis, J. Z., Stein, R. I., Welch, R. R., & Ball, S. A. (2000). Comorbid psychopathology in binge-eating disor-der: Relation to eating disorder severity at baseline and following
treatment.Journal of Consulting and Clinical Psychology, 4,641– 649.
Zanarini, M. C., Frankenburg, F. R., Hennen, J., Reich, D. B., & Silk, K. R. (2004). Axis I comorbidity in patients with borderline personality
dis-order: 6-year follow-up and prediction of time to remission.American
Journal of Psychiatry, 161,2108 –2114.
Zimmerman, M., & Mattia, J. L. (1999). Axis I diagnostic comorbidity and
borderline personality disorder.Comprehensive Psychiatry, 40,245–252.
Received August 3, 2007 Revision received July 28, 2008