ORIGINAL ARTICLES
RENAL DISEASE IN MULTIPLE MYELOMA
Andia Banu-Bradu
1, Hortensia Ionita
2, Ioana Ionita
2, Corina Vernic
3,
Claudiu Macarie
4REZUMAT
Introducere: Boala cronică de rinichi (BCR) poate apare la aproximativ jumătate din cazurile de mielom multiplu, 20% dezvoltând insuficiență renală. Aceasta poate reprezenta forma de debut a bolii hematologice sau poate apare în cursul evoluției hemopatiei maligne. Obiectiv: Evaluarea BCR la pacienții cu mielom multiplu aflați sub chimioterapie, internați în Clinica de Hematologie a Spitalului Municipal Timișoara pe parcursul a șapte ani, respectiv în perioada ianuarie 2002 – martie 2009. Material și metode: In urma unei analize retro- și prospective, au fost studiați 97 pacienți cu mielom multiplu. Pentru stabilirea gradului de afectare renală s-au urmărit indicii antropometrici, parametrii biologici sangvini și urinari precum și evaluarea factorilor de risc asociați. Rezultate: La debutul hemopatiei, 40,2% din cazuri au prezentat afectare renală, iar dintre aceștia, la 10,25% s-a identificat creșterea stadiului BCR pe parcursul evoluției hemopatiei. Dintre pacienții cu mielom multiplu cu funcție renală inițială bună aflați sub chimioterapie, 12,37% au dezvoltat o boală cronică de rinichi pe perioada urmărită, astfel încât incidența BCR la finalul studiului a fost de 52.58% (p=0.08405). Complicațiile infecțioase urinare cu efect direct renal nu au fost de neglijat, ele fiind prezente la 42,26% din pacienți. Majoritatea celor care au dezvoltat insuficiență renală cronică (83,33%) au primit scheme chimioterapice complexe. Concluzie: Mielomul multiplu reprezintă una din cauzele de afectare renală atât prin acțiune directă la nivel tubular cât și datorită asocierii factorilor de risc (de tipul proteinuriei, hipercalcemiei, hiperuricemiei, deshidratării, complicațiilor infecțioase, hipervâscozității) și a comorbiditățiilor (în special HTA și factorul obstructiv), peste care se suprapune terapia antineoplazică cu potențial nefrotoxic cert.
Cuvinte cheie: boala cronică de rinichi, mielom multiplu, rinichi mielomatos, chimioterapie
ABSTRACT
Introduction: The chronic renal disease (CRD) can occur in approximately half of the multiple myeloma cases, with 20% of them developing renal failure. It may represent the onset of the haematological disease, or may appear during the progress of the malignant haemopathy. Objective: To evaluate the chronic renal disease in multiple myeloma patients undergoing chemotherapy, admitted in the Haematology Clinic of the Timisoara Municipal Hospital over a period of seven years, from January 2002 to March 2009. Material and methods: Following retrospective and prospective evaluation, we examined 97 multiple myeloma patients. We established the level of renal impairment based on anthropometric indices, blood and urine biological parameters, and the evaluation of associated risk factors. Results: At the onset of the haemopathy, 40.2% of the cases displayed renal impairment, with the stage of the chronic renal disease advancing in 10.25% of these cases. Among multiple myeloma patients undergoing chemotherapy and having good initial renal function, 12.37% developed chronic renal disease over the period we monitored; thus, the incidence rate of the CRD at the end of the study was 52.58% (p = 0.08405). Urinary infectious complications with direct renal effect were also quite significant, occurring in 42.26% of patients. The majority of patients who developed chronic renal failure (83.33%) received complex schemes of cytostatic therapy. Conclusion: Multiple myeloma is one of the causes of renal impairment, both through direct action at tubular level, and due to an association of risk factors (such as proteinuria, hypercalcemia, hyperuricemia, dehydration, infectious complications, hyperviscosity) and co-existing pathologies (especially HBP and obstructive factor), combined with antineoplastic therapy having an established nephrotoxic potential.
Key Words: chronic renal disease, multiple myeloma, myelomatous kidney, chemotherapy
1 Clinic of Internal Medicine I, Municipal Hospital, Timisoara 2 Clinic of
Haematology, Municipal Hospital, Timisoara 3 Victor Babes University of
Medicine and Pharmacy, Timisoara, 4 Clinic of Intensive Care, Clinical
County Emergency Hospital, Timisoara Correspondence to:
Andia Banu-Bradu, Clinic of Internal Medicine I, Municipal Hospital, 5 Gheorghe Dima Str., Timisoara, Tel. +40-722-663454.
Email: [email protected]
INTRODUCTION
Multiple myeloma is a malignant monoclonal gammopahty characterized by proliferation of a myelomatous clone that is responsible for the
production of osteolytic lesions, infiltration of
the hematogenic bone marrow with plasmocytes, production of abnormal monoclonal proteins and, subsequently, occurrence of renal lesions, amyloidosis and hyper-viscosity syndrome, along
with immune deficiency.
It is relatively frequent and represents 1% of all malignancies and 10% of the haematological neoplasms;
it affects the elderly in general. Incidence rates in Europe are 5.72/100,000 population, with approximately 27,500
new cases discovered every year.1
The myeloma-associated nephropathy is
poly-morphous. The chronic renal disease is seen in approximately half of the multiple myeloma cases, with 20% of the cases developing renal failure. Up to
50% of the newly diagnosed patients display decreased
creatinine clearance, and approximately 9% require dialysis due to severe deterioration of the renal function.
Renal failure can be a form of onset of the haematological disease, or it can develop during the
evolution of the malignant haemopathy. In general,
renal impairment is the result of tubular obstruction by hyaline cylinders made of protein material, atrophy
and consecutive interstitial fibrosis (myelomatous
kidney).2 Proteinuria is characteristic, but usually does
not exceed 3 grams/24 hours. Approximately 10% of patients develop nephrotic syndrome.
Renal amyloidosis is present in 15-30% of the multiple myeloma patients, with proteinuria being the
most frequent renal manifestation at onset, identified in ~80% of the patients. Nephrotic syndrome is
found in 30-50% of the renal amyloidosis cases, while
chronic renal failure occurs in 70% of the patients. Goldschmidt and Lannert claim that approximately
20% of the multiple myeloma patients have renal failure at the onset of the haematological disease, but the condition is reversible in half of the cases, by elimination
or diminution of some of the aggravating factors.3
Thus, the pathogenesis of the chronic renal disease in multiple myeloma occurs through a number of
mechanisms.4,5 The precipitation of light chains (that
are produced in excess in patients with this haemopathy,
compared to levels in healthy people) at the level of the renal tubes, resulting in formation of obstructive cylinders, leads to breaking of the basement membrane
and consecutive interstitial fibrosis. Thus, urine tests
point out a monoclonal proteinuria with Bence Jones
light chains. When in large amounts, these chains disturb
the renal function, either by massive precipitation in
the tubes, leading to cylinder formation (myeloma cast nephropathy), or by direct toxic action on the proximal tubes. The nephrotoxic potential of the Bence Jones protein was outlined in experimental studies conducted
on mice.6,7 The myelomatous kidney was the object of
research in studies conducted by many authors.8-19 It is a
specific renal impairment, characterized by the presence
of intra-tubular cylinders with a protein structure made
of light monoclonal chains, glomerular ultra-filtrates and the Tamm-Horsfall protein.
In 25% of the cases, the chronic renal disease in multiple myeloma can also be induced by sedimentation
of monoclonal immunoglobulins, with subsequent thickening of the renal tubes’ basement membrane,
leading to glomerulosclerotic lesions. Cases of
rapidly progressive and membranoproliferative
glomerulonephritis were also reported.5,20-22
The cellular and humoral immune dysfunction results in increased susceptibility to infections - a factor with negative impact on the already impaired renal function; at the same time, the immune suppression from the corticotherapy and cytostatic
therapy increases the risk of infections.23 These can
lead to the occurrence of acute renal failure episodes that can aggravate the chronic renal disease and
implicitly deteriorate the body. Thus, some authors
recommend prophylactic antibiotic treatment to
prevent infections in multiple myeloma.24
Chemotherapy used in treating malignant haemopathies can have a nephrotoxic effect. Antineoplastic therapy can be nephrotoxic and lead
to renal failure by impairment at tissue, interstitial and - rarely - glomerular level, as well as through mechanisms that affect circulation at kidney
level. The presence of the chronic renal disease in a multiple myeloma patient can favor the toxic
action of cytostatic medication.25-27 Methotrexate
- an antagonistic anti-metabolite of folic acid
- has a nephrotoxic effect, as it precipitates at
the level of the distal tube, already impaired in the multiple myeloma and the consecutive renal
failure. Nephrotoxicity depends on the dose
and duration of the treatment and is favored by
dehydration.20,28,29 Cyclophosphamide can determine
severe haemorrhagic cystitis and – in rare cases –
renal tubular necrosis. The literature mentions cases
of renal failure after administration of melphalane, which more frequently induces cystitis and
urination perturbations. Carmustine (a derivate of nitrosourea) is potentially nephrotoxic, as it induces complex renal lesions, such as tube atrophy and interstitial fibrosis. Evolution to chronic stages may
generate glomerulosclerotic lesions.26-28,30-32
Most patients require treatment for chemotherapy
in various schemes: CVP (cyclophosphamide, vincristine and prednisone) and VAD (vincristine, doxorubicin and dexamethazone). Some studies underline the beneficial role of VAD on kidney
damage in multiple myeloma.33
MATERIAL AND METHODS
Following retrospective and prospective
evaluation, we identified 97 multiple myeloma patients admitted at the Haematology Clinic of
These patients received complex cytostatic therapy with nephrotoxic potential: CVP (cyclophosphamide, vincristine and prednisone) associated with melphalane.
The remaining patients with initial proteinuria received
varying therapy schemes.
Increased susceptibility to infections showed
in the high percent of cases with urinary infections.
Infectious episodes at the level of the urinary tract
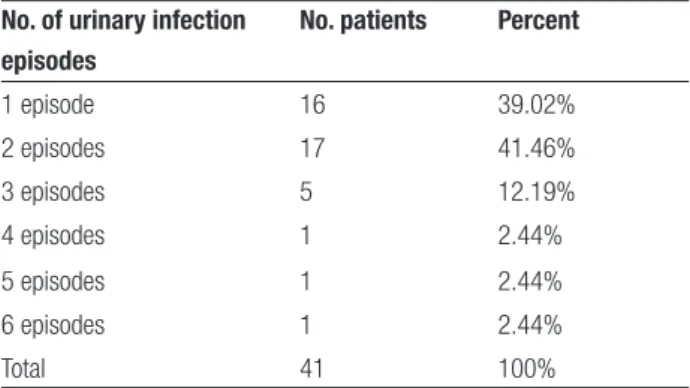
were seen in 41 patients (42.26%), with more than half of them (25 patients) having recurrent urinary infections. We ascertained that in 60% of the cases these recurrences happened in the context of a pre-existing renal condition, in patients with GFR<60 ml/
min/1.73m2, while in 5 patients (20%) these infectious
episodes played a significant part in the subsequent development of chronic renal disease. The distribution
of multiple myeloma patients per number of urinary
infection episodes is given in Table 1.
Table 1. Distribution of MM patients per number of UTI episodes. No. of urinary infection
episodes
No. patients Percent
1 episode 16 39.02% 2 episodes 17 41.46% 3 episodes 5 12.19% 4 episodes 1 2.44% 5 episodes 1 2.44% 6 episodes 1 2.44% Total 41 100%
In terms of the pathogen triggering the urinary tract infections, E. Coli was the most frequent (87.8%);
Kleb. Pneumoniae was identified in urine culture in 3
patients (7.31%), and Proteus mirabilis and Ps. aeruginosa
shared the same incidence rate (2.44%).
Figure 1 shows the distribution of the presence of E. Coli in urine cultures in patients with multiple myeloma and urinary tract infections, compared to
other pathogens.
Fig.1. Incidence of pathogens involved in generating UTI in the MM group.
the Timisoara Municipal Hospital over seven years,
January 2002 to March 2009, undergoing various schemes of cytostatic therapy.
During the mentioned period, we monitored
the patients' dynamics, each of them having at least
4 admissions. We established the level of kidney
impairment based on anthropometric indices, blood
(urea, creatinine, uric acid) and urine (urine analysis,
proteinuria, urine culture) biological parameters, and
paraclinical investigations (ECG, pulmonary x-Ray, abdominal echography). Proteinuria was determined using dipsticks. The glomerular filtration rate (GFR)
was calculated depending on the four variables: age, gender, race, and blood creatinine rates, from the
formula in the guide developed by The Kidney Disease
Outcomes Quality Initiative (K/DOQI).34,35
At the same time, we looked at the presence of
risk factors for chronic renal disease: senescence, anaemic syndrome, HBP, diabetes mellitus, hyperuricemia, recurrent urinary infections, other
co-existing malignant conditions, cytostatic therapy and corticotherapy.
RESULTS
The 97 multiple myeloma patients examined from January 2002 to March 2009 displayed the following distribution per age and gender: 50 patients (51.54%) were female, aged 34 – 79 (with the average age being 60.64 +/- 11.88 years) and 47 patients were male (48.45%), aged 42 – 82 (with the average age being 65.43+/- 9.17 years).
Among them, 73.19% (71 cases) had various co-existing pathologies: 31 patients had high blood pressure, 4 were diabetics, 5 cases had high blood pressure and diabetes, 4 had another associated
neoplasm, 6 patients were known with chronic viral hepatitis, 3 men were diagnosed with prostate
adenoma, and the others had coronary disease. 7.21% (7 patients) were known with unilateral or bilateral kidney lithiasis.
Hyperuricemia was detected in 24 cases (24.74%) at first admission, but none of them displayed associated lithiasis.
When the haematological disease was diagnosed, proteinuria was present in 44.32% of the myeloma patients (43 cases), out of which 32 were known with
renal impairment, GFR<60 ml/min/1.73m2. Two
patients with initial proteinuria and no previous renal impairment developed the chronic renal disease during
the monitored period. Both patients were hypertensive
and repeatedly developed infectious complications –
In terms of the chronic renal disease, 39 cases (40.2%) had renal impairment at the onset of the
haemopathy, with GFR<60 ml/min/1.73m2. A
number of 24 patients (61.53%) were found with chronic renal disease stage III; 11 patients (28.2%) were in stage IV, and 4 cases in stage V. (Table 2) Table 2. Distribution of patients with MM and renal impairment per stages of the CRD. Stage of CRD Number of patients Percent Stage III 24 61.53% Stage IV 11 28.2% Stage V 4 10.25% Total 39 100%
The following observations were made regarding these multiple myeloma patients with chronic renal disease already formed at the time when they came to
the Haematology Clinic: 3 patients were diagnosed with chronic glomerulopathy. Renal biopsy has revealed one case of renal amyloidosis with significant proteinuria,
consecutive nephrotic syndrome and chronic renal
failure. In two other situations, renal biopsy has revealed membranoproliferative glomerulonephritic lesions (in one patient) and myeloma cast nephropathy (in the second case).
The patients’ dynamics showed that most of them
remained at the initial stage of the CRD; only in 4 cases (10.25%) there was a permanent decrease of the glomerular filtration rate – with implicit advancement of the chronic renal disease stage. We noticed that none of
these patients displayed any obstructive factors; half of them were diagnosed with recurrent urinary infections
and all of them had aggravations of the pre-existing renal disease in the context of existing infections, which led to an aggravation of the renal impairment.
In terms of chemotherapy schemes these patients were following, they were all on cyclophosphamide,
vincristine, melphalane and prednisone.
Among multiple myeloma patients under chemotherapy who previously had GFR>60 ml/
min/1.73m2, 12 cases (12.37%) developed chronic renal
disease during the monitored period. While evaluating
the presence of risk factors in these patients and of the infectious complications they developed, as well as the chemotherapy scheme applied, we noticed the following: 5 patients had high blood pressure and one
had another co-existing neoplasm, and the obstructive factor (renal lithiasis) was present in 3 patients. We also
noted that only two patients had proteinuria at the moment of receiving the multiple myeloma diagnosis,
and hyperuricemia was present in 5 cases. Regarding urinary infection episodes in these patients, 7 had
recurrent urinary tract infections, with consecutive
acute renal failure in almost half of the cases (3 patients – 42.85%). In terms of therapy, 2 patients were on melphalane, 7 were treated with complex
schemes including melphalane, cyclophosphamide, vincristine and prednisone, one was on carmustine in
a VBAP scheme (vincristine, carmustine, adriamycin and prednisone), and 2 were on the VAD scheme (vincristine, adriamycin and dexamethazone).
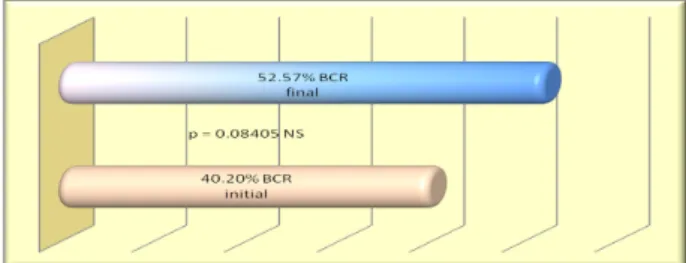
At the end of the study, the chronic renal disease was present in 52.57% of the cases (51 patients).
Figure 2 shows a graphic comparison between the incidence rates of the chronic renal disease in this lot at the beginning and at the end of the study; the
difference is not statistically significant (p=0.08405).
Figure 2. CRD incidence rates in the MM group at the beginning and at the end of study.
Out of the 97 multiple myeloma patients examined, 7 (7.21%) died during the study period.
This was due to infectious complications occurred in 3 patients with good renal function, but who developed episodes of irreversible acute renal
failure, and in 4 cases with previously impaired renal function (1 case was in stage III of the chronic renal disease, 2 cases were in stage IV and one in stage V) and aggravation of the chronic renal failure.
DISCUSSIONS
Unlike in some studies claiming that the renal
chronic disease is seen in 20% of the cases at the
onset of the haematological disease (Goldschmidt and
Lannert), in this study renal impairment was present
in 40.2% of the patients at the time the patients were diagnosed with multiple myeloma.
Compared to previous studies regarding the
incidence of chronic renal disease in multiple myeloma,
claiming that CRD is found in approximately half of
the patients, the incidence rates of renal impairment we
found at the end of our study were similar (52.57%). Within the lot we studied, we identified one case
of membranoproliferative glomerulonephritis, one case of myeloma cast nephropathy and one case of renal amyloidosis with nephrotic syndrome that had
an unfavorable development.
Urinary infectious complications with direct effect
on the renal function by induction of acute renal failure episodes, subsequently recovered through adequate
therapeutic behavior, were quite significant. As much as 42.26% of the myeloma patients were diagnosed
with urinary tract infections, and more than half of
these (60.97%) had recurrent urinary infections.
The majority of patients who developed
chronic renal failure (83.33%) were under complex
cytostatic therapy schemes including melphalane, cyclophosphamide, vincristine, carmustine, adriamycin
and prednisone.
CONCLUSION
From the data presented above, multiple myeloma is revealed to be one of the cases of renal impairment, both through a direct action following the organic changes induced at tube level, and through association
of risk factors (such as proteinuria, hypercalcemia,
hyperuricemia, dehydration, infectious complications,
hyperviscosity), co-existing pathologies (especially
high blood pressure and obstructive factor) and
antineoplastic therapy with established nephrotoxic potential.
REFERENCES
1. Rodriguez-Abreu D, Bordoni A, Zucca E. Epidemiology of hematological malignancies Ann Onc. 2007;18(1): i3-i8.
2. Mut Popescu D. Hematologie clinica. Editia a II-a, Ed. Medicala, Bucuresti, 2003.
3. Goldschmidt H, Lannert H, Bommer J. Renal failure in multiple myeloma. “The myeloma kidney”: state of the art. Saudi J Kidney Dis Transpl 2001;12(2):145-50.
4. Jourde-Chiche N, Dussol B, Daniel L. Kidney involvement in malignant hematologic malignancies. Diagnostic approach. Rev Med Interne 2010 May 17.
5. Clarkson MR, Brenner BM. Pocket companion to Brenner and Rector’s. The Kidney 7-th ed. Ed Saunders, Philadelphia 2005, 223-4. 6. Solomon A, Weiss DT, Kattine AA. Nephrotoxic potential of Bence
Jones proteins. N Engl J Med 1991 Jun 27; 324(26):1889-90. 7. Koss MN, Pirani CL, Osserman EF. Experimental Bence Jones cast
nephropathy. Lab Invest 1976 Jun;34(6): 579-91.
8. Ivanyi B. Renal complications in multiple myeloma. Acta Morphol Hung 1989;37(3-4):235-43.
9. Ivanyi B. Frequency of light chain deposition nephropathy relative to
renal amyloidosis and Bence Jones cast nephropathy in a necropsy
study of patients with myeloma. Arch Pathol Lab Med 1990 Sep;114(9):986-7.
10. Batuman V. Proximal tubular injury in myeloma. Contrib Nephrol 2007;153:87-104.
11. Taparia BN, Bahel B, Shah BV, et al. Renal involvement in multiple myeloma. J Assoc Physicians India 1996 Apr; 44(4):240-2. 12. Spicka I, Merta M, Cieslar P, et al. Renal impairment in monoclonal
gammapathies. Clinical study. Cas Lek Cesk 1995 Aug 2;134(15):478-81.
13. Hill GS, Morel-Maroger L, Mery JP, et al. Renal lesions in multiple myeloma: their relationship to associated protein abnormalities. Am J Kidney Dis 1983 Jan; 2(4):423-38.
14. Pasquali S, Zuchelli P, Casanova S, et al. Renal histological lesions and clinical syndromes in multiple myeloma. Renal Immunopathology Group. Clin Nephrol 1987 May; 27(5):222-8.
15. Nakayama N, Fujigaki Y, Tsuji T, et al. Rapid deterioration of renal
function in a patient with multiple myeloma associated with amyloid
and light chain depositions. Clin Exp Nephrol 2009 Dec;13(6):671-6. 16. Alexanian R et al. Renal failure in multiple myeloma: pathogenesis and
prognostic implications. Arch Intern Med 1990, 150, I 693. 17. Bataille R, Harousseau JL. Multiple myeloma. N Engl J Med 1997;336:23-30. 18. Tubbs RR, Gephardt GN, McMahon JT, et al. Light chain nephropathy.
Am J Med 1981 Aug;71(2):263-9.
19. Gherasim L – Medicina Interna, vol IV, Ed Medicala, Bucuresti 2002. 20. Gluhovschi G, Petrica L, Velciov S. Manual de nefrologie clinica, Vol I,
Ed Mirton, Timisoara 2008, p 251-3.
21. Appel GB, Radhakrishnan J, D’Agati V. Secondary glomerular disease, Brenner BM, Brenner and Rector’s. The Kidney 7-th ed. Ed Saunders, vol I 2004, p 1381-481.
22. Ronco PM, Aucouturier P, Mougenot B. Monoclonal gammapathies: multiple myeloma, amyloidosis and related disorders. In Schrier RW, Diseases of the kidney and urinary tract. 8-th ed. Ed Lippincot. Williams and Wilkins 2007, vol 3, p 1941-85.
23. Kalambokis GN, Christou L, Tsianos EV. Multiple myeloma presenting with an acute bacterial infection. Int J Lab Hematol 2009 Aug;31(4):375-83.
24. Oken MM, Pomeroy C, Weisdorf D, et al. Prophylactic antibiotics for the prevention of early infection in multiple myeloma. Am J Med 1996 Jun; 100(6):624-8.
25. Kintzel PE, Dorr RT. Anticancer drug renal toxicity and elimination: dosing guidelines for altered renal function. Cancer Treat Rev 1995;21:33. 26. Aronoff GM, Berns JS, Brier ME, et al. Drug prescribing in renal
failure: dosing guidelines for adults, 4th Edition, American College of Physicians, Palm version 2002.
27. Aronoff GM, Bennett WM, Berns JS, et al. Drug prescribing in renal failure: dosing guidelines for adults and children, 5th Edition, American College of Physicians, 2007.
28. Velciov SM. Nefrotoxicitatea medicamentoasa. Ed Mirton, Timisoara 2007. 29. Methotrexate: Drug Information. In: Rose BD, editor. UpToDate.
Wellesley, MA, UpToDate; 2006.
30. Cyclophosphamide: Drug Information. In: Rose BD, editor. UpToDate. Wellesley, MA, UpToDate; 2005.
31. Dede F, Ayili D, Sahiner S. Effective treatment administration of cyclophosphamide in membranous nephropathy. J Nephrol 2008 Jul-Aug; 21(4):560-5.
32. Perry MC. The Chemotherapy Source Book. Fourth Edition, 2008; p 224-31. 33. Matsuda M, Gono T, Katoh N, et al. Nephrotic syndrome due to
primary systemic AL amyloidosis successfully treated with VAD (vincristine, doxorubicin, dexamethazone) alone. Intern Med 2008; 47(6):543-9.
34. National Kidney Foundation - K/DOQI kidney disease outcome quality initiative. Am J Kidney Dis. 2002;39: (Suppl. 1):S1–S266. 35. National Kidney Foundation - Clinical practice guidelines for chronic
kidney disease evaluation, classification and stratification. Am J Kidney Dis, 2002.