IDENTIFYING OPPORTUNITIES TO IMPROVE PARENT INVOLVEMENT IN CHILDREN’S PHYSICAL ACTIVITY
Cody Dalton Neshteruk
A dissertation submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department
of Nutrition in the Gillings School of Global Public Health.
Chapel Hill 2019
ii © 2019
iii ABSTRACT
Cody Dalton Neshteruk: Identifying Opportunities to Improve Parent Involvement in Children’s Physical Activity
(Under the direction of Dianne S. Ward)
Over one third of children in the United States have overweight or obesity. Physical
activity is a key component of maintaining a healthy weight, while also benefiting children’s
growth and development. However, many children do not meet the recommended amount of
physical activity needed to achieve these health benefits. Parents are one of the primary sources
of child socialization, but despite the known influence of parents, there are still gaps in our
understanding of how parents impact children’s physical activity, specifically around the use of
multiple parent physical activity practices and the role of fathers.
To learn more about how parents use multiple physical activity practices, secondary data
analyses were conducted using a sample of 319 parent-child dyads enrolled in an obesity
prevention trial. Latent profile analyses identified three distinct patterns of parenting including
Rewarders, Activity Supporters, and Screen Time Permissive parents. There were statistically
significant demographic differences among the groups, but no differences were observed in child
physical activity, sedentary behavior or adiposity.
To understand more about the role of fathers in children’s physical activity,
semi-structured interviews were conducted with 24 fathers of 3 to 11-year-old children exploring their
interactions with children around physical activity. Findings showed that fathers use a variety of
iv
their children in order to bond and develop shared interests, and fathers perceived their role in children’s physical activity to be greater compared to mothers.
Because fathers are typically not included in family-based interventions, a mixed methods design was used to identify barriers and facilitators to father involvement in a physical activity focused, community-based pediatric weight management program. Time and
responsibilities were the primary barriers preventing fathers from participating, while key facilitators included an inviting program staff, desire to spend time with children, and concern for children’s weight.
v
vi
ACKNOWLEDGEMENTS
I have a great deal of gratitude for all of the people who supported me during my training at UNC and throughout the dissertation process. First and foremost, I would like to thank my advisor and mentor, Dr. Dianne Ward. Through your guidance and wisdom, you have shaped me into the researcher that I am today. Words cannot express how grateful I am for your unwavering support and for providing me with countless opportunities to succeed. I would also like to
express my appreciation to each of my committee members – Drs. Alice Ammerman, Deborah Jones, Asheley Skinner, and Deb Tate, for their valuable advice, insight and pushing me to think critically. Additionally, I would like to thank Dr. Sarah Armstrong for her willingness to include me in the Bull City Fit team.
Outside of my committee, I would like to acknowledge all of the members of the
Children’s Healthy Weight Research Group. I’m honored to have been part of this team and am thankful for everything that I’ve learned while working with all of you. I appreciate all the support and words of encouragement I’ve received. I would also like to thank the students and teachers in the Department of Nutrition for your motivation, support and friendship.
vii
viii
TABLE OF CONTENTS
LIST OF TABLES ... xiii
LIST OF FIGURES ... xiv
LIST OF ABBREVIATIONS AND SYMBOLS ... xv
CHAPTER 1: INTRODUCTION ... 1
Background ... 1
Specific aims... 3
CHAPTER 2: LITERATURE REVIEW ... 4
Pediatric obesity and overweight are a public health problem ... 4
Physical activity is key for children’s health and weight ... 5
Parents play a key role in influencing children’s physical activity behaviors ... 7
Limited research on fathers suggests that dads may be influential in promoting child PA... 10
Identifying barriers and facilitators to father engagement in children’s health promotion ... 13
CHAPTER 3: METHODS ... 15
Study population and protocols ... 15
Aim 1 ... 15
Aim 2 ... 16
Aim 3 ... 17
Measures ... 20
Parent physical activity and screen time practices ... 20
ix
Child and parent anthropometrics ... 22
Sample demographics ... 22
Semi-structured interviews ... 23
Theoretical model constructs ... 24
Role Construction ... 24
Self-efficacy for Managing Child’s Weight ... 24
Invitation to Participate... 25
Analyses ... 25
Aim 1 ... 25
Aim 2 ... 27
Aim 3 ... 28
CHAPTER 4: IDENTIFYING PATTERNS OF PARENT PHYSICAL ACTIVITY AND SCREEN TIME PRACTICES AND ASSOCIATION WITH CHILD PHYSICAL ACTIVITY AND ADIPOSITY ... 30
Overview ... 30
Background ... 31
Methods... 32
Recruitment... 33
Data collection ... 33
Measures ... 34
Demographics... 34
Physical activity and screen time practices ... 34
Parent and child physical activity and sedentary behavior ... 35
Parent and child anthropometrics ... 35
Data analysis ... 36
x
Latent profiles ... 38
Association with child outcomes ... 39
Discussion ... 40
Conclusion ... 45
CHAPTER 5: UNDERSTANDING THE ROLE OF FATHERS IN CHILDREN’S PHYSICAL ACTIVITY: A QUALITATIVE STUDY... 52
Overview ... 52
Background ... 53
Methods... 54
Recruitment... 54
Semi-structured interview guide development ... 55
Data collection ... 56
Data analysis ... 56
Results ... 57
Fathers use of physical activity practices ... 58
Co-participation... 58
Facilitation ... 59
Modeling ... 59
Involvement ... 60
Encouragement ... 60
Physical activity in the father-child relationship ... 61
Parental roles in children’s physical activity ... 62
Discussion ... 63
xi
CHAPTER 6: IDENTIFYING BARRIERS AND FACILITATORS TO FATHER
PARTICIPATION IN A COMMUNITY-BASED PEDIATRIC WEIGHT MANAGEMENT
PROGRAM ... 72
Overview ... 72
Background ... 73
Methods... 75
Bull City Fit ... 75
Recruitment... 76
Theoretical framework ... 76
Data collection ... 77
Measures ... 78
Semi-structured interviews ... 78
Demographics... 78
Physical activity ... 78
Theoretical model constructs... 79
Role construction ... 79
Self-efficacy for managing child’s weight ... 80
Invitation to participate ... 80
Data analysis ... 81
Results ... 82
Barriers ... 82
Time and responsibilities ... 82
Other barriers ... 83
Facilitators ... 84
Invitation to participate ... 84
xii
Concern for child’s weight ... 85
Discussion ... 86
Conclusion ... 90
CHAPTER 7: SYNTHESIS ... 96
Overview of findings ... 96
Limitation and strengths ... 99
Limitations ... 99
Strengths ... 101
Future directions ... 102
Public health impact and summary ... 107
APPENDIX 1: PARENTING SOS PHYSICAL ACTIVITY AND SCREEN TIME PARENTING QUESTIONNAIRE ... 109
APPENDIX 2: SCORING FOR PARENTING SOS PHYSICAL ACTIVITY AND SCREEN TIME PRACTICES ... 123
APPENDIX 3: SELF-REPORT PHYSICAL ACTIVITY QUESTIONNAIRE ... 125
APPENDIX 4: AIM 2 INTERVIEW GUIDE ... 127
APPENDIX 5: AIM 3 INTERVIEW GUIDE ... 131
APPENDIX 6: INTERVIEW DEBRIEF FORM ... 133
APPENDIX 7: MEASURES OF THEORETICAL CONSTRUCTS IN MODEL OF PARENT INVOLVEMENT ... 134
xiii
LIST OF TABLES
Table 1. Physical activity and screen time practice indicator variables ... 46
Table 2. Parent demographic characteristics (n = 319) ... 47
Table 3. Fit indices for 2-6 class model solutions ... 48
Table 4. Estimated means (SE) for parenting practices by class ... 49
Table 5. Parent demographic characteristics by class ... 50
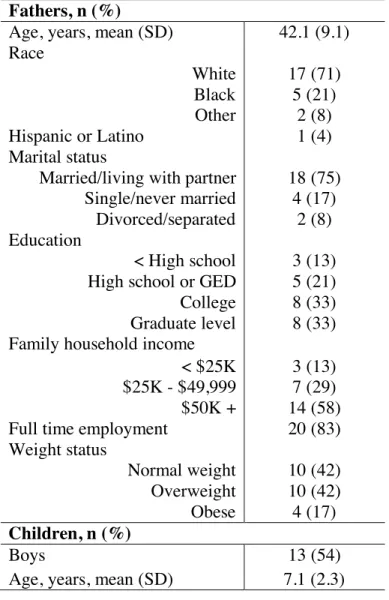
Table 6. Demographic characteristics of fathers participating in interviews (n = 24) ... 68
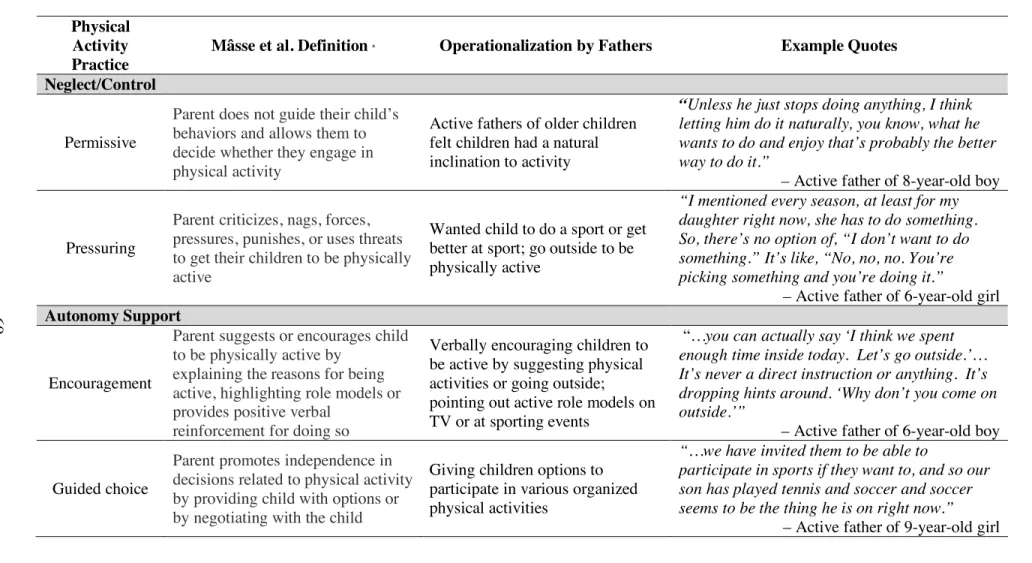
Table 7. Operationalization of defined physical activity practices by fathers ... 69
Table 8. Demographic characteristics of participating fathers (n = 8) ... 93
xiv
LIST OF FIGURES
Figure 1. Davison et al.'s Integrated Model of Physical Activity Parenting ... 8
Figure 2. Mâsse et al.'s conceptual model of physical activity parenting ... 9
Figure 3. Children’s physical activity and sedentary behavior per 10 hours ... 51
Figure 4. Flow of participant recruitment for Bull City Fit fathers ... 91
Figure 5. Adapted version of Hoover-Dempsey & Sadler’s model of parent engagement ... 92
xv
LIST OF ABBREVIATIONS AND SYMBOLS
ANOVA Analysis of variance BCF Bull City Fit
BIC Bayesian Information Criterion BLRT Bootstrap Likelihood Ratio Test BMI Body mass index
BRFSS Behavioral risk factor surveillance survey CDC Centers for Disease Control and Prevention DADEE Dads and Daughters Exercising and Empowering EFA Exploratory factor analysis
HDHK Healthy Dads Healthy Kids
IPAQ International physical activity questionnaire LMR LRT Lo-Mendell-Rubin adjusted likelihood ratio test LTPA Leisure time physical activity
MVPA Moderate-to-vigorous physical activity
NHANES National Health and Nutrition Examination Survey PA Physical activity
SAS Statistical analysis software
SD Standard deviation
SE Standard error
SNAP Supplemental Nutrition Assistance Program
ST Screen time
xvi
US United States
1
CHAPTER 1: INTRODUCTION
Background
In the United States, more than one in three children are classified as having overweight or obesity. These children experience a number of physical and emotional consequences and most importantly, are at risk for continuing to have overweight or obesity into adulthood. Physical activity has been recognized as an important component of obesity prevention and treatment efforts in young children, while also benefiting children in a variety of developmental domains. However, many children do not meet current physical activity recommendations and there are clear disparities by sex, age, and weight status. Effective strategies are needed to improve children’s physical activity in order to help establish healthy lifelong behaviors.
Leveraging the role of parents is one potential strategy to promote healthy physical activity behaviors in children. Parents shape children’s physical activity preferences and habits through how they choose to structure the home environment, their own physical activity
2
Relatively little empirical attention has been devoted to the role of fathers in children’s health research and fathers are largely underrepresented in family-based programming. Despite the dearth of research, there are observational and a few intervention studies that have shown fathers can impact children’s physical activity. However, to gain a better understanding of how exactly fathers influence children’s physical activity, we need to know more about how they interact with their children around physical activity, and more specifically, their physical activity parenting behaviors. Furthermore, it is necessary to understand the barriers and facilitators to their involvement in order to design programs that effectively engage fathers. To address these gaps in the physical activity parenting literature, a series of studies was undertaken.
3
project will add to the physical activity parenting literature by identifying potential
intervention targets, ways to engage fathers in children’s physical activity and key barriers
and facilitators to father involvement in physical activity promotion programs.
Specific aims
Aim 1: Identify patterns of physical activity parenting using latent profile analysis and examine associations with children’s physical activity, sedentary behavior and adiposity.
Aim 2: Characterize fathers’ involvement in children’s physical activity and identify the physical activity practices commonly used by fathers.
4
CHAPTER 2: LITERATURE REVIEW
Pediatric obesity and overweight are a public health problem
Over the past 30 to 40 years, the rates of pediatric overweight and obesity have risen dramatically in the United States (US).1 Some evidence suggests that the levels of pediatric overweight and obesity may be plateauing and even decreasing in certain age groups,2,3 but the most recent estimates indicate the prevalence has continued to increase. A study using data from the National Health and Nutrition Examination Survey (NHANES) collected between 1999 – 2016 found that 35.1% of children ages 2 to 19 years had overweight or obesity (BMI ³ 85th percentile for sex and age) with higher rates observed among older children and African American and Hispanic children. Additionally, the study found a rise in severe obesity (BMI ³ 120% of the 95th percentile).4
5
The consequences of overweight and obesity in children are pervasive. Children with obesity are more likely to develop risk factors for cardiovascular disease such as high blood pressure, high LDL cholesterol, and insulin resistance.15–17 Children with obesity also suffer emotional and social effects such as stigmatization by their peers,18 lower self-esteem,19 and decreased quality of life.20–22 Most importantly, children with overweight or obesity are more likely to have overweight or obesity as adults, putting them at risk for health complications including type 2 diabetes, heart disease and several types of cancer.23–26 The numerous
consequences make it critical that effective prevention and treatment programs are available to help children develop healthy behaviors and put them on healthy weight trajectories to improve lifetime health.
Physical activity is key for children’s health and weight
Physical activity contributes to children’s healthy growth and development in a variety of domains. Higher levels of physical activity have been associated with reductions in cardio- metabolic risk factors, including lower blood pressure, serum triglycerides, and LDL cholesterol.27–29 Furthermore, increased physical activity is associated with children’s motor development, bone health, cardiovascular fitness, cognitive development, and academic
6
Furthermore, physical activity is recognized as an integral part of pediatric obesity treatment programs,39 highlighting the importance of physical activity in weight management.
Despite the numerous benefits of physical activity to children’s health and weight, many children do not participate in sufficient amounts of physical activity to obtain these benefits. The 2018 Physical Activity Guidelines for Americans recommend that children ages 3 to 5 years should be active throughout the day, obtaining at least 180 minutes of activity at any intensity, while older children ages 6 to 17 years should engage in 60 minutes of moderate to vigorous physical activity (MVPA) per day.40 Objective estimates of children’s physical activity suggest that many are not meeting these recommendations. It is estimated that only about half of preschool children ages 2 to 5 years meet current guidelines,41–45 with even fewer older children meeting recommendations. A study using accelerometer data from NHANES showed that only 43% of children 6 to 11 years old obtained at least 60 minutes of MVPA per day, while less than 10% of children 12 to 19 years old met this recommendation.46 Not surprisingly, the US Report Card on Physical Activity for Children and Youth currently ranks children’s overall participation in physical activity at dismal D minus grade.47
Furthermore, certain subgroups tend to be at higher risk for obtaining lower amounts of physical activity. At the population level, there are clear age-related declines in physical activity. Physical activity tends to peak during the preschool and early elementary years and then begins to decline steadily through childhood and adolescence.48 When examining sex differences in physical activity, girls are consistently less active than boys.49 Finally, children with overweight and obesity tend to be less active than their normal weight peers. Surveillance data from
7
children with obesity spent 16 fewer minutes per day engaged in MVPA compared to their normal weight counterparts.51
With many children not meeting physical activity recommendations and clear subgroup differences, physical activity promotion strategies are needed to ensure the development of healthy physical activity habits in children. Evidence shows that physical activity behaviors early in life can track into adolescence and adulthood, suggesting that early childhood is a critical period for intervention.52 Identifying effective strategies to promote children’s physical activity are needed to help prevent aged-related declines in physical activity as well as sex and weight-related disparities.
Parents play a key role in influencing children’s physical activity behaviors
Parents are the primary agents of child socialization, influencing children through their own behaviors, attitudes, and beliefs.53 As such, the familial environment plays an important role in shaping and supporting children’s physical activity behaviors and is considered an important target for promoting healthy physical activity habits. Parents influence children’s physical activity through how they structure the physical activity environment children are exposed to (e.g., availability of active toys),54 their own physical activity behaviors and attitudes (e.g., importance placed on physical activity),55 and the physical activity related parenting behaviors used, specifically their physical activity practices.56,57
8
verbal reinforcement or encouragement, and facilitation of physical activity (i.e., logistic
support) through enrolling children in sports/classes, providing transportation or opportunities to be active, and purchasing equipment or active toys, have all been linked to positive
improvements in children’s physical activity.66–70 While parent physical activity practices are recognized as important sources of support for children’s physical activity, there has been little agreement on the measurement and conceptualization of these practices. The physical activity parenting literature is in its infancy compared to the extensively developed food parenting literature within which it is rooted. As such, reviews have highlighted inconsistent terminology and operationalization of practices across studies and a lack of comprehensive, psychometrically tested measures as current challenges in measuring parent physical activity practices.71,72
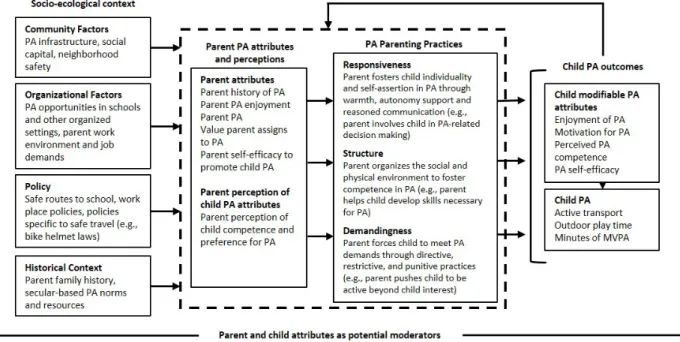
In order to begin addressing these challenges, there have been efforts to organize physical activity practice constructs into parenting dimensions or domains, similar to the food parenting and general parenting literature.65,73,74 A conceptual model by Davison et al. shown in Figure 1
9
represents one of the first efforts to organize parent physical activity practices and create a common terminology. Practices are organized into three parenting dimensions: responsiveness, structure, and control or demandingness. Responsive practices are child focused, with the parent providing warmth and autonomy support as well as openly communicating with the child (e.g., encouragement or praise), while controlling
or demanding practices are parent focused, with the parent using practices that are directive, restrictive or punitive (e.g., pressure). Structure based practices are the ways that parents organize the social and physical activity environment to support children’s physical activity (e.g.,
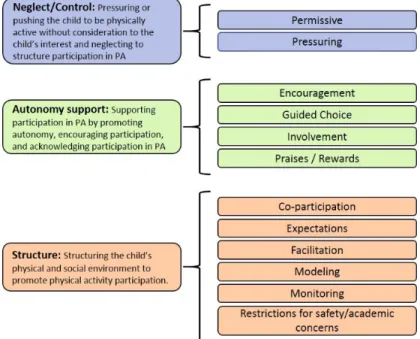
modeling).65 More recently, Mâsse et al., published a conceptual model of physical
activity parenting shown in Figure 2.73 Twelve parenting practice constructs were identified using expert informed concept mapping analysis and then organized into three domains similar to those identified by Davison et al: neglect/control, autonomy support, and structure, with the main difference being the inclusion of neglect/permissiveness within the control or
demandingness dimension. Although these conceptualizations of physical activity parenting provide the field with a consistent terminology and structure, there is still much to be learned about the influence of parents on children’s physical activity.
Most research has studied the impact of individual parent physical activity practices on children’s physical activity, but we know that parents use a variety of different parenting
10
practices to influence their children’s behavior.75,76 Furthermore, evidence from the food parenting literature shows that parenting practices fluctuate on a day to day and situational basis. For instance, a study using ecological momentary assessment to examine the variability of parent feeding practices showed that the practices parents used varied across the week and were often context-specific (e.g., number of people at meals, foods served, meal setting).77 Currently, there are no studies that have examined how parents use physical activity practices in combination. Examining how practices work in conjunction can potentially help identify patterns of physical activity parenting that would give a more generalized picture of parents’ approaches to parenting in the domain of physical activity. Additionally, this research will provide an opportunity to understand more about the current conceptualization of physical activity parenting and how practices from the proposed parenting dimensions interact with one another. By identifying patterns of physical activity parenting, this can provide potential targets for family-based physical activity promotion interventions.
Limited research on fathers suggests that dads may be influential in promoting child PA
11
only 1% focused exclusively on fathers and only 37% included both mothers and fathers, of which half included 10 or fewer fathers. Across all interventions, fathers represented only 6% of parent participants.79 Similarly, Morgan et al. reviewed 213 behavioral interventions designed to prevent or treat pediatric obesity, finding that of the 80 trials focusing on one parent, fathers represented 6% of parents and of the 133 trials in which both parents could participate, 92% did not report father involvement.80 These reviews show that inclusion of fathers in children’s weight related research is limited. Given the high prevalence of pediatric overweight and obesity and importance of physical activity in maintaining a healthy weight, it is essential that we better understand the role that fathers play in their children’s health behaviors. This can inform the design of effective strategies to increase father engagement both in research and in real world settings.
12
and child physical activity, while there was limited evidence for an association between mother and child physical activity.84
Few interventions have exclusively targeted fathers for health promotion, with only two published interventions involving only fathers and their children. Healthy Dads Healthy Kids (HDHK) is an 8-week program designed to promote positive weight-related behaviors in fathers and their children. HDHK has been extensively tested and showed positive improvements in both father and child physical activity and weight in each of the efficacy,85 effectiveness,86 and
dissemination randomized controlled trials.87 The second intervention, Dads and Daughters Exercising and Empowering (DADEE), is a program designed to engage fathers with their daughters through physical activity. In a randomized controlled trial, DADEE produced an increase in both fathers’ and girls’ physical activity as well as positive improvements in the father-daughter relationship compared to a wait-list control 88,89 The success of these interventions shows that engaging fathers in physical activity promotion is a promising strategy for improving children’s physical activity.
13
Identifying barriers and facilitators to father engagement in children’s health promotion
Family-based interventions have been identified as an effective strategy for promoting children’s physical activity and managing children’s weight.90,91 For instance, a classic study by Epstein and colleagues showed that when parents are involved in pediatric obesity treatment compared to child only treatment, there are greater long-term benefits. At both 5- and 10-year follow-ups, children treated along with their parents maintained relative weight loss, while children who were treated alone gained weight.92,93 Despite the known benefits of including parents, current family-based obesity treatment and physical activity promotion programs have had modest success at reducing weight and promoting physical activity.90,94–96 One possible explanation is that family-based interventions tend to not be truly family based, predominantly focusing on the mother-child dyad.79,80,97,98 This could create a disconnect between parents when it comes to making healthy lifestyle changes. Engaging fathers in family-based interventions may provide an opportunity to ensure that both parents are on the same page and provide consistent reinforcement of healthy behaviors through their conversations with children, parenting practices, and own behaviors. However, very little is known about the inclusion of fathers in parenting programs, making it critical to understand barriers to father engagement as well as facilitators for their involvement in programming.
Very little is known about what factors inhibit or facilitate the inclusion of fathers in parenting research and programs. Studies examining father involvement in general parenting interventions have shown that time (i.e., work and family commitments) is one of the primary barriers to father participation.99–101 Other barriers that have been cited include: lack of interest or relevance, program cost, perception that interventions are mother focused, and lack of
14
15
CHAPTER 3: METHODS
Study population and protocols
Aim 1
This study used baseline data from the Parenting SOS trial, a randomized controlled trial designed to test the efficacy of a 35-week parent focused childhood obesity prevention
intervention (Clinical Trials ID: NCT00998348). 103 Families were randomized to either the My Parenting SOS intervention or a child book club control group. My Parenting SOS consisted of 12 in-person sessions focused on building general parenting skills (e.g., stress management, co-parenting, and child behavior management) and then applying these skills to promote healthier diet and physical activity behaviors in children. All study protocols were reviewed and approved by the University of North Carolina at Chapel Hill Institutional Review Board.
A convenience sample of families with preschool aged children was recruited from central North Carolina in three waves from 2009 to 2012. Recruitment methods included direct mailings, listserv announcements, advertisements and flyers in the community, and interceptions at child care centers. Interested families were screened by phone. To be eligible, families had to have at least one child between the ages of 2 to 5 years, at least one parent with a self-reported BMI ³ 25 (i.e., classified as having overweight or obesity), willingness to complete intervention activities, and the ability to speak and read English.
16
accelerometers. Children then participated in child activities while parents completed study questionnaires. Informed consent was obtained from all participants prior to baseline data collection. Parents consented on behalf of children.
Aim 2
Data for this study comes from a formative study designed to better understand fathers’ physical activity views, beliefs, and behaviors, how fathers are involved in their children’s physical activity, and intervention preferences for physical activity promotion. Due to the large amount of qualitative data, this study focused on father-child interactions around physical activity and fathers’ physical activity parenting behaviors. A total of 24 fathers were recruited to complete semi-structured interviews. To ensure that there was adequate representation of active and low active fathers, the sample was stratified such that we recruited both active fathers (n = 12) and low-active fathers (n = 12). All study protocols were reviewed and considered exempt by the University of North Carolina at Chapel Hill Institutional Review Board.
17
chosen as the referent child. During screening, fathers were asked to self-report their own vigorous leisure-time physical activity (LTPA) using a screener question. 104 Fathers were classified as active if they indicated they met physical activity recommendations via vigorous LTPA. Vigorous LTPA was used to classify fathers’ activity level because this type of activity is typically intentional, easier to quantify in a reported recall, and has demonstrated better self-report reliability and validity compared to moderate physical activity. 105 Following screening, eligible fathers were scheduled to complete an in-person interview.
All interviews were conducted by an interviewer trained in qualitative research methods. Interviews occurred in a private space (e.g., conference room or office) and informed consent was obtained prior to the start of the interview. Each interview was audio recorded and interviews lasted an average of an hour (mean 59.4 minutes). Following the interview, participants completed a brief demographic survey and a physical activity self-report
questionnaire. Participants received $35 cash for completing the interview and questionnaires.
Aim 3
This study used a cross sectional mixed methods design where fathers were asked to complete an in-person interview and a series of questionnaires. A convergent approach was used where both qualitative and quantitative data were collected simultaneously. Equal weights were given to both components (QUAN + QUAL). 106 Data were collected from March to June 2019. All study protocols were reviewed and approved by the University of North Carolina at Chapel Hill Institutional Review Board.
18
management clinic at Duke University and the Durham Department of Parks and Recreation. 107,108 The program is designed to provide children 5 to 18 years old and their families with the
necessary resources to make healthy lifestyle changes around diet and physical activity in order to help reduce children’s weight. Patients receiving clinical care at the Healthy Lifestyles clinic are referred to Bull City Fit, which gives families an opportunity to practice and reinforce clinical recommendations in a supportive context. Bull City Fit is offered Monday through Thursday from 6 to 8 pm and Saturday and Sunday from 1 to 3 pm at a local community center. Each session offers opportunities for physical activity through free play and structured activities. On weekends, activities are held in the community center pool. Sessions are guided by the program coordinator with assistance provided by volunteers, who are mostly undergraduate students from Duke and other local universities. Bull City Fit also offers a weekly cooking and nutrition education class for parents and children. Family involvement is welcomed and
encouraged, with parent(s) and siblings able to participate in all activities.
Fathers, which included father figures (e.g., grandparent, step-father), were recruited through advertisements in the weekly Bull City Fit e-newsletter and direct phone calls. A list of fathers and their contact information (n = 42) was provided by the Bull City Fit program
coordinator to facilitate phone calls. To ensure that fathers were most familiar with the current iteration of Bull City Fit, this list included fathers with a child currently participating in Bull City Fit or who had participated in the past year. To be eligible, fathers had to be comfortable
19
Data collection for this Aim was guided by Hoover-Dempsey & Sadler’s model of parent involvement. 109 This model of parent involvement has empirically demonstrated the ability to explain parent involvement in children’s education. 110,111 Many of the constructs are applicable to general parent involvement and as such, we adapted the model to explain parent involvement within a pediatric obesity treatment program. There are three key constructs in the model that contribute to parent involvement: parents’ motivational beliefs, parents’ perception of invitation for involvement from others, and parents’ perceived life context. Parents’ motivational beliefs are further broken down into parental role construction (i.e., how parents view their role in children’s weight management) and parental self-efficacy (i.e., how confident parents are that they can help their children manage their weight). In this context, parents’ perception of
invitation includes how welcome they feel they are to participate in Bull City Fit from different sources including the child and program staff/volunteers. Finally, parents’ perceived life context provides important contextual information that may influence the ability of parents to be actively involved including time and energy as well as skills and knowledge related to the program and children’s weight management.
20
interviews and underwent a two-hour training to become familiar with Bull City Fit and the interview guide. Interviews lasted between 15 to 30 minutes and were audio recorded. Following the interview, participants completed a series of questionnaires that included demographics, self-report physical activity, and scales to assess constructs in the theoretical model. After completing the interview and questionnaires, participants received $20 cash as incentive.
Measures
Parent physical activity and screen time practices
In Aim 1, parents self-reported their physical activity and screen time parenting behaviors using a 147-item questionnaire (Appendix 1). A comprehensive literature review was
21
child preference for physical activity and support/reinforcement from other adults) and all four screen time practices were used in this study. To calculate subscale scores, all items in the subscale are averaged (Appendix 2). The initial EFA analyses showed that the identified subscales demonstrated acceptable reliability and construct validity. 58
Child and parent physical activity and sedentary behavior
Parent and child physical activity and sedentary behavior were assessed using ActiGraph GT3X accelerometers (ActiGraph, Pensacola, FL) in Aim 1. Monitors were worn on an
adjustable belt on the participant’s right hip for seven consecutive days, except while sleeping or in water. For parents, data were captured in 60-second epochs, while child data were captured in 15-second epochs to account for short bursts of activity typical of children’s active play. Data were downloaded and processed using the NHANES SAS code. Non-wear time was identified by isolating periods of at least 60 minutes with zero counts. 112 For parents and children to have valid accelerometer data, they must have worn the monitor for six or more hours on at least four of the days. Sedentary behavior, light activity, and MVPA were identified by applying
established, age-specific cut points to the data, with NHANES cut points applied to parent data and Evenson cut-points applied to child data. 46,113 To account for differences in wear time,
estimates of sedentary behavior and physical activity were standardized to a 10-hour day for both parents and children.
22
over the past week using closed ended response options ranging from 5 minutes or less to 90 minutes for vigorous activity and 10 minutes or less to 180 minutes for moderate activity. These four items were adapted from the International Physical Activity Questionnaire and Behavioral Risk Factor Surveillance System questionnaire. 114,115 These instruments have demonstrated acceptable validity and reliability in prior studies. 114,116
Child and parent anthropometrics
Parent and child anthropometrics where captured using standard procedures by trained data collectors in Aim 1. Parent and children’s standing height was measured to the nearest 1/8 inch using Shorr or Seca infant/child/adult stadiometers (Shorr Productions, Olney, MD; Seca Corporation, Columbia, MD) and weight to the nearest 0.1 pound with a Seca model 770 portable electronic scale (Seca Corporation, Columbia, MD). All measures were taken at least twice. Height and weight were used to calculate parent BMI and child BMI z-score. The Centers for Disease Control (CDC) SAS code was used to derive child BMI z-score. 117
Participants in Aims 2 and 3 self-reported their height and weight, which were then used to calculate BMI.
Sample demographics
23 Semi-structured interviews
Semi-structured interviews were conducted in Aims 2 and 3. To guide interviews, a semi-structured interview guide was developed for each Aim. The interview guide used in Aim 2 was developed by members of the research team (CN, DJ, and DSW) with expertise in parenting, psychology, physical activity, child development, and qualitative research methods. The
Integrative Model of Physical Activity Parenting was used as the guiding theoretical framework for the interview guide. The model integrates evidence regarding the impact of physical activity parenting on children’s physical activity, embedded within the larger socio-ecological context in which families operate. The parent components of the model were the primary focus of the interview guide and included parent physical activity attributes, perceptions, and practices. Questions focused on exploring fathers’ own physical activity behaviors, views, and attitudes as well as their interactions with their children and parenting practices around physical activity (Appendix 4).
The interview guide used in Aim 3 was developed by members of the research team (CN, AS, DSW) with expertise in parenting, child development, weight management, and qualitative research methods. Hoover-Dempsey & Sadler’s model of parent involvement (previously described) was used to inform the interview guide. Questions in the semi-structured interview guide were designed to assess constructs in the theoretical model as well as gain knowledge about fathers’ experiences with the program and challenges they faced in participating
24 Theoretical model constructs
Subscales measuring role construction, self-efficacy, and invitation to participate were adapted from existing measures specifically for Aim 3 (Appendix 7). 111 All items were scored on a Likert scale from one to six. To create subscale scores for each construct, all items within that subscale are averaged together to create a total score, with higher scores indicating greater perception of that particular construct (e.g., higher scores on role construction indicated greater perceived role in children’s weight management). Due to the small sample size, we were unable to assess the psychometric properties of these newly developed scales.
Role Construction
Participants self-reported their role in children’s weight management using a 12-item scale. Items were anchored by the statement “I believe it is my responsibility to…”. For each item, fathers were asked rate to their agreement (e.g., “disagree very strongly” to “agree very strongly”). Items were designed to measure parents’ role in general weight management (4-items; e.g. “help my child manage his/her weight”), physical activity (3-(4-items; e.g., “play and exercise with my child”), nutrition (3-items; e.g. “talk with my child about eating healthy foods”), and parents’ own behavior (2 items; e.g., “set a good example for my child”).
Self-efficacy for Managing Child’s Weight
Participants self-reported their self-efficacy for helping their children manage their
25
agreement with each item (i.e., “disagree very strongly” to “agree very strongly”). Three items were reverse coded.
Invitation to Participate
Participants self-reported their perceived invitation using three scales measuring general invitation (6-items), child invitation (6-items) and staff invitation (6-items). For general
invitation, participants were asked to respond with their agreement to each statement (i.e., “disagree very strongly” to “agree very strongly”) These items assessed Bull City Fit on a broad level (e.g., “I feel welcome at Bull City Fit”; “Bull City Fit lets me know about activities and special events”). For the staff and child invitation scales, participants were asked to indicate how often they experienced each statement (i.e., “never” to “daily”). Staff items (e.g., “Bull City Fit staff asked me to participate in Bull City Fit”) assessed how welcoming Bull City Fit staff and volunteers were, while child items (e.g. “my child wanted me at Bull City Fit”; “my child asked me to attend Bull City Fit”) assessed invitation from the child for the father to participate in Bull City Fit.
Analyses
Aim 1
26
individual’s most likely class membership. There are several advantages to using latent profile analysis over other statistical approaches such as cluster analysis: 1) groups can be separated even if they overlap, 2) includes cases with missing data through the use of Maximum
Likelihood estimation, 3) both categorical and continuous variables can be included and 4) latent profile analysis allows for the statistical testing of different model solutions, which provides a more rigorous basis for final model selection. 120
Indicator variables for these analyses include parent physical activity and screen time practices previously identified through EFA. One observation was excluded because data were missing for all indicator variables. We estimated five different latent profile models, varying the number of classes from two to six. To identify the best fitting model, we used a combination of model fit statistics and interpretability including 1) Bayesian Information Criterion (BIC), 2) Lo-Mendell-Rubin adjusted Likelihood Ratio Test (LMR LRT), 3) Bootstrap Likelihood Ratio Test (BLRT), 4) number of individuals assigned to each class and 5) interpretability of the classes based on existing literature. Because there was no variation in the indicator variable “rules around active play indoors,” another set of models were constructed excluding this variable. Following the identification of the best fitting model, individuals were assigned to the class with the highest probability of membership. Estimated means and standard errors for indicator
variables from the best fitting model are presented.
Remaining analyses were conducted using SAS 9.4. Descriptive statistics (means,
standard deviations, and frequencies) were calculated to describe the demographic characteristics of the total sample and each identified class. Analysis of variance (ANOVA), chi square tests, and Fisher’s exact tests were used to determine if classes differed by demographic
27
behavior per 10 hours, as well as BMI z-score, were examined by parent class membership using a series of generalized linear models. Models included parent class membership as a categorical predictor variable of each child level outcome. A contrast statement was used to compare groups (i.e., class 1 to class 2). A significance level of a=0.05 was used. Following this initial test, additional demographic covariates known to be associated with the outcomes, including child sex and age, parent BMI, parent race and education, and annual family income, were added to the models.
Aim 2
Interviews were transcribed verbatim, reviewed for accuracy and then imported into QSR NVivo 12 (QSR International, Melbourne, Australia) for analysis using a deductive thematic analysis approach. 121 A deductive approach was most appropriate given the guidance by an existing framework. Briefly, thematic analysis involves six steps: 1) becoming familiar with the data, 2) generating initial codes, 3) searching for themes, 4) reviewing themes, 5) defining and naming themes, 6) producing a manuscript reporting identified themes.
Two coders (the principal investigator and a research assistant) read each transcript to become familiar with the content. To ensure consistent coding, a codebook was developed using the semi-structured interview guide as well as relevant papers from the physical activity
28
how each code should be operationalized and applied. The two coders then pilot tested the codebook on one transcript, discussing disagreements and refining the codebook as necessary. Coding was an iterative process and the codebook was refined as needed throughout the analysis. Each transcript was coded independently by the two coders and then compared to identify
disagreements. The two coders met periodically to resolve disagreements and ensure that
adherence to the codebook was maintained. Themes were identified and then additional analyses examined these themes to determine if there were differences in the operationalization of the theme by father activity level.
Aim 3
29
For the quantitative data, descriptive statistics including means, standard deviations, and frequencies were calculated to describe the participant demographics and weekly physical activity. Next, scores were calculated for role construction, self-efficacy for managing child’s weight, and each invitation to participate construct by averaging the responses to each item within the subscale. Means and standard deviations were calculated for each subscale score. Additionally, frequencies were calculated at the item level to further explore participants’ responses. All quantitative analyses were conducted in SAS v. 9.4.
Once the qualitative and quantitative data were analyzed separately, the two datasets were merged by importing the quantitative data for each participant into QSR NVivo 12. This allowed for the triangulation of themes, to ensure consistency or identify potential discordance within the data. An initial set of themes describing fathers’ barriers and facilitators to
participating in Bull City Fit was developed and then further explored by participant
30
CHAPTER 4: IDENTIFYING PATTERNS OF PARENT PHYSICAL ACTIVITY AND SCREEN TIME PRACTICES AND ASSOCIATION WITH CHILD PHYSICAL
ACTIVITY AND ADIPOSITY
Overview
Parent physical activity and screen time practices impact children’s behaviors. However, studies have not examined how these practices work in combination. The purpose of this study was to identify patterns of physical activity and screen time parenting, as well as to examine differences in children’s physical activity, sedentary behavior, and adiposity among the identified patterns.
Data were collected from 319 parent-child dyads enrolled in a randomized controlled trial testing a parent-focused obesity prevention intervention in 2 to 5-year-old children. Parent
physical activity and screen practices were assessed using a validated self-report survey at baseline. Children’s physical activity and sedentary behavior were measured using
accelerometers and child anthropometrics were objectively measured. Latent profile analyses identified patterns of parent physical activity and screen time practices. Differences in child outcomes were tested among the groups.
31
screen time. There were no differences in the mean child MVPA, sedentary behavior or BMI z-score among the three classes.
Findings from this study identified three distinct classes of parents. More work is needed examining the influence of parent physical activity and screen time practice patterns
longitudinally and in different populations. Understanding more about these patterns may provide modifiable targets for family-based physical activity promotion.
Background
Increased physical activity and reduced sedentary behavior have been linked to children’s healthy growth and development, including positive benefits on children’s adiposity, cardio-metabolic fitness, gross motor development, academic performance, and social and emotional health.30,32,33,35 However, many young children do not obtain enough physical activity and engage in excessive amounts of sedentary behavior, particularly in the form of screen time. Estimates suggest that preschool aged children spent only about 47 minutes engaged in MVPA per day, while spending an average of 10 hours/day engaged in sedentary behavior.127 Furthermore, many young children greatly exceed the recommended one hour of screen time per day,128,129 indicating the need to identify effective strategies to promote physical activity and reduce sedentary behavior in young children.
The familial environment plays an important role in shaping children’s physical activity and sedentary behaviors, in particular through parents’ physical activity and screen time
32
physical activity, facilitation of activity through logistic support (e.g., providing transportation or equipment), and co-participation in activity have been associated with increased child physical activity,66,67,69 while setting rules and limits around screen time has been associated with reduced screen time.130 Leveraging these parenting practices may be an effective way to promote children’s physical activity and reduce sedentary behavior.
Research on parent physical activity and screen time practices has focused on the impact of individual practices on child behavior, but parents typically employ a variety of practices.75 Furthermore, evidence from the food parenting literature shows that parent practices fluctuate day-to-day and based on the situation.77 To date, no studies have tested how physical activity and screen time practices work in conjunction. Although parent practices related to physical activity and screen time may evolve fairly separately, they each have the potential to impact children’s physical activity and sedentary behavior. Identifying patterns of parent physical activity and screen time practices combined may elucidate how these practices work together, while also providing a broader understanding of how parents influence their children’s physical activity and sedentary behavior. Therefore, the aims of this study were to 1) identify patterns of parent physical activity and screen time practices using latent profile analysis and 2) examine if identified patterns were associated with differences in children’s physical activity, sedentary behavior, and adiposity.
Methods
This study uses baseline data from the Parenting SOS trial, a randomized controlled trial designed to test the efficacy of a 35-week parent-focused childhood obesity prevention
33
Parenting SOS intervention consisting of 12 in-person group sessions or a child book club control group. All protocols were approved by the University of North Carolina at Chapel Hill Institutional Review Board.
Recruitment
Recruitment has been described in detail in the protocol paper.103 Briefly, families with preschool aged children were recruited from central North Carolina. Recruitment methods included direct mailings, listserv announcements, advertisements and flyers in the community, and interceptions at child care centers. To be eligible, families had to have at least one child between the ages of 2 to 5 years, at least one parent with a self-reported BMI greater than 25, willingness to complete intervention activities, and the ability to speak and read English.
Data collection
34 Measures
Demographics
Parents completed a self-report demographic questionnaire at baseline that captured parent age, sex, race/ethnicity, marital status, education, employment status, and annual family income. Parents also self-reported their child’s sex and date of birth.
Physical activity and screen time practices
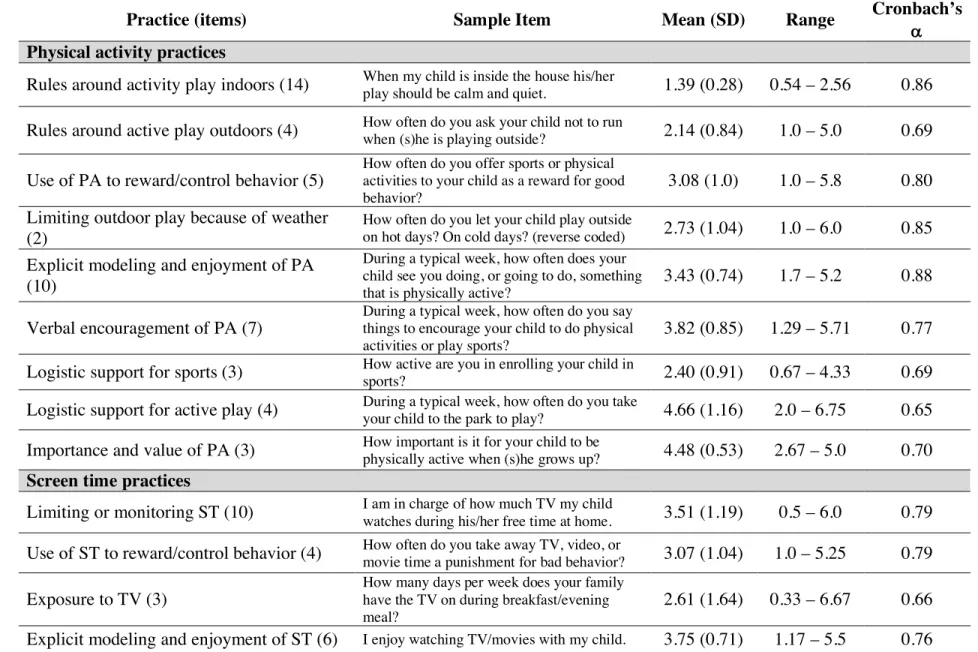
Parents self-reported their physical activity and screen time parenting behaviors using a 147-item questionnaire developed specifically for Parenting SOS.58 A comprehensive literature review was undertaken to identify relevant parenting constructs and existing instruments in order to develop a content map around physical activity and screen time parenting. Items from existing measures were matched to each construct on the content map and new items were developed to ensure that each construct was adequately measured. Items assessed parent behaviors using Likert responses (e.g., “never” to “very often”; “strongly disagree” to “strongly agree”) and open-ended questions (e.g., “During the last month, how many times have you taken your child to play at a park?”). Appropriate items were reverse coded and open-ended responses
categorized such that higher scores indicate more frequent use of the practice. Previously, we used exploratory factor analyses with the baseline sample to identify relevant physical activity and screen time practice subscales. Of the original 147 items, 83 were retained to form 11 physical activity practice subscales and four screen time practice subscales. Subscales
35
subscale scores, all items in the subscale are averaged. Information on each subscale including number of items, sample items, and reliability are shown in Table 1. The initial analyses showed that subscales demonstrated acceptable reliability and construct validity.58
Parent and child physical activity and sedentary behavior
Parent and child physical activity and sedentary behavior were assessed using ActiGraph GT3X accelerometers (ActiGraph, Pensacola, FL). Monitors were worn on an adjustable belt on the participant’s right hip for seven consecutive days, except while sleeping or in water. For parents, data were captured in 60-second epochs, while child data were captured in 15-second epochs to account for short bursts of activity typical of children’s active play. Data were downloaded and processed using the National Health and Nutrition Examination Survey
(NHANES) SAS code. Non-wear time was identified by isolating periods of at least 60 minutes with zero counts.112 For parents and children to have valid data, they must have worn the monitor for six or more hours on at least four of the days. Valid data were available for 282 children and 299 parents. Sedentary behavior, light, and moderate or vigorous physical activity (MVPA) were identified by applying established, age-specific cut points to the data, with NHANES cut points applied to parent data and Evenson cut-points applied to child data.46,113 To account for differences in wear time, estimates of sedentary behavior and physical activity were standardized to a 10-hour day for both parents and children.
Parent and child anthropometrics
36
Shorr or Seca infant/child/adult stadiometers (Shorr Productions, Olney, MD; Seca Corporation, Columbia, MD) and weight to the nearest 0.1 pound with a Seca model 770 portable electronic scale (Seca Corporation, Columbia, MD). All measures were taken at least twice. Height and weight were used to calculate parent BMI and child BMI z-score was calculated using the Centers for Disease Control SAS code.117
Data analysis
Latent profile analysis using Mplus7 was used to identify patterns of parent physical activity and screen time practices.118 Latent profile analysis is a type of mixture modeling used to identify underlying homogenous groups (i.e., classes) within a population based on a set of indicator variables, which can be either categorical or continuous.119 Latent profile analysis estimates the probability of membership in each identified class in order to determine the individual’s most likely class membership.
37
the highest probability of membership. Estimated means and standard errors for indicator variables from the best fitting model are presented.
Remaining analyses were conducted using SAS 9.4. Descriptive statistics (means,
standard deviations, and frequencies) were calculated to describe the demographic characteristics of the total sample and each identified class. Analysis of variance (ANOVA), chi square tests, and Fisher’s exact tests were used to determine if classes differed by demographic
characteristics. Group differences in children’s minutes of physical activity and sedentary
behavior per 10 hours, as well as BMI z-score, were examined by parent class membership using a series of generalized linear models. Models included parent class membership as a categorical predictor variable of each child level outcome. A contrast statement was used to compare groups (i.e., class 1 to class 2). A significance level of a = 0.05 was used. Following this initial test, additional demographic covariates known to be associated with the outcomes, including child sex and age, parent BMI, parent race and education, and annual family income, were added to the models.
Results
38 Latent profiles
Model fit statistics for the 2-6 class solutions are shown in Table 3. The LMR LRT indicated that the 2-class model was the best fitting model, while the BIC indicated either the 3-class or 4-3-class model. There was a minimal change in the BIC between the 3-3-class and 4-3-class models (9841 vs 9821) and both produced classes with at least 10% of the sample assigned to each class. The 3-class model yielded three interpretable classes, which were generally
reproduced in the 4-class model, but with less clarity. Therefore, the 3-class model was chosen as the best fitting model.
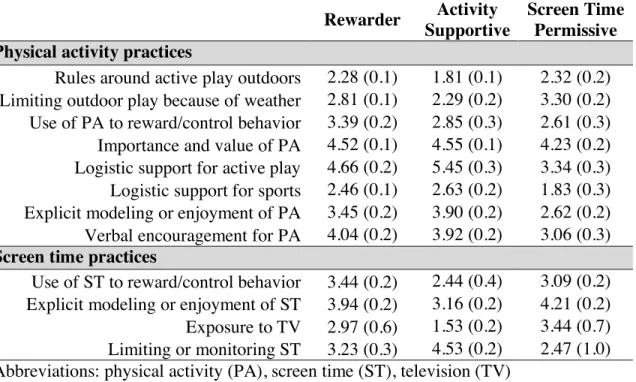
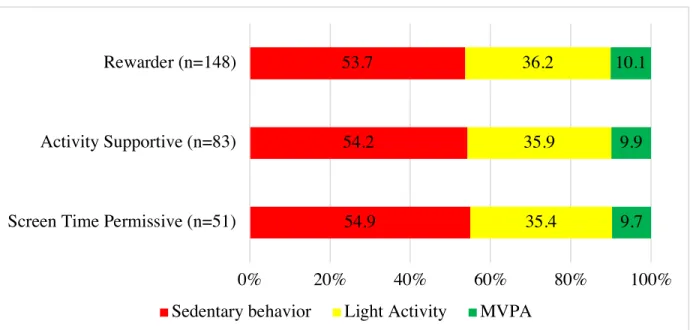
Estimated means for the indicator variables for each of the three identified classes are shown in Table 4. The largest class, Rewarders (n =165; 52%), was characterized by parents who exhibited the highest scores for using physical activity and screen time as a reward or to control children’s behavior. Rewarder parent scores for the other practices generally fell in between the scores of the remaining two classes. Activity Supportive parents (n = 98; 31%) made up the second largest group. This group was characterized by parents with the highest scores on practices supportive of physical activity (e.g., providing logistic support, modeling active behavior, limiting or monitoring screen time) and lowest scores on practices that may promote screen time (e.g., rules or limits on physical activity, modeling/enjoyment of screen time). The third and smallest class, Screen Time Permissive (n = 56; 18%), was characterized by parents with the lowest scores on limiting or monitoring screen time and highest scores on practices that promote screen time (e.g., exposure to TV, modeling/enjoyment of screen time). In general, Screen Time Permissive parents scored lowest on practices supportive of physical activity.
39
education, annual family income, and employment status. Compared to Rewarder and Screen Time Permissive parents, Activity Supportive parents had a lower mean BMI, were more frequently fathers, and tended to be White, married or living with a partner, well educated, and higher income. Fewer Activity Supportive parents worked full time, but there was a greater percentage of parents who worked at home or who were stay at home parents. Rewarder and Screen Time Permissive parents tended to have similar demographic characteristics, with the exception of annual household income, where more Rewarder parents were considered high income.
There were significant group differences among the classes in parent physical activity and sedentary behavior (per 10 hours). Activity Supportive parents had the most MVPA (mean = 24.2 minutes), followed by Rewarder parents (mean = 22.6 minutes). Both groups had similar amounts of light activity (mean = 164.2 vs. 164.5 minutes) and sedentary behavior (mean = 407.5 vs. 409.6 minutes). Screen Time Permissive parents, however, had the lowest MVPA (mean = 18.0 minutes) and light activity (mean = 149.0), as well as the most sedentary behavior (mean = 429.7).
Association with child outcomes
The percent of time that children engaged in physical activity and sedentary behavior over a standardized 10-hour period is shown in Figure 3 by parent class membership. There were no significant differences in children’s mean MVPA or sedentary behavior among the parent classes. Children of Rewarder parents spent the most time engaged in MVPA over the 10-hour period (mean = 60.1 minutes), while spending the least amount of time in sedentary
40
time engaged in MVPA (mean = 59.0 minutes) and second least in sedentary behavior (mean = 323.7 minutes). Children of Screen Time permissive parents engaged in the least amount of MVPA (mean = 58.1 minutes) and most sedentary behavior (mean = 327.8 minutes).
A significant difference was found between the mean BMI z-scores of children of Rewarder and Activity Supportive parents (mean = 0.42 vs. 0.17, p = 0.05); however, this association was no longer significant when controlling for parent and family demographic characteristics. There were no significant differences in the mean child BMI z-scores between children of Rewarder and Screen Time Permissive parents (mean = 0.42 vs. 0.40; p = 0.90) or between children of Screen Time Permissive and Activity Supportive parents (mean = 0.40 vs. 0.17; p = 0.18).
Discussion
41
Current conceptualizations of physical activity and screen time parenting have separately organized practices into dimensions or domains.65,73,131 Because there are many parallels between these two literatures, Vaughn and colleagues integrated these models to develop an integrated conceptual model of parent physical activity and screen media practices (under review). In the model, there are four distinct parenting dimensions (i.e., control/demandingness, permissiveness, responsiveness/autonomy support, and structure) within which parent practices are categorized. Findings from this study show that there were distinct patterns in how parents used physical activity and screen time practices, utilizing practices from across the parenting dimensions. For instance, Activity Supportive parents had high scores on practices in both the autonomy support and structure dimensions. The identified patterns emphasize the need to assess a variety of physical activity and screen time practices in order to understand how parents use these practices to influence children’s behavior.
The Rewarder class had the largest membership, accounting for 50% of parents. Interestingly, the defining characteristic of this class was the highest scores for using both physical activity and screen time as a reward or to control children’s behavior, suggesting that this controlling practice may be a general strategy often employed by parents. This is consistent with standard approaches to child behavior management and evidence-based treatment
42
important considerations for parents should be the type of behavior parents use as a reward (e.g., healthy vs. unhealthy) and if parents make children aware in advance of this contingency, as well as if parents use it judiciously (e.g., 10-minutes versus 1 hour) and consistently.
Previous literature has often focused on understanding the impact of supportive physical activity practices,61 and the identification of the Activity Supportive class in this study shows that these practices group together. Conversely, the Screen Time Permissive pattern is a unique finding, although permissive parenting is a well-established parenting style demonstrated early on by the seminal work of Baumrind.134 A question then is whether permissiveness for these families is limited to screen time, in which case one could envision fairly targeted interventions teaching other parenting strategies that promote greater engagement with and monitoring of young children. Alternatively, the permissiveness around screen time may be reflective of a broader parenting style that reflects an overall lack of engagement with the child, which may require more intensive intervention with parents. As such, these patterns may have value as a screening tool to help tailor intervention targets and approaches within physical activity promotion interventions.
43
able to devote more time and resources to their children’s physical activity. We also observed differences in parent race among the groups, which is consistent with previous literature showing that parents from different racial and ethnic groups use different physical activity practices.138,139 These findings suggest that parent demographic characteristics are important considerations when attempting to understand the influence of parenting practices on child behaviors.
Based on the identified classes, it could be hypothesized that children of Activity Supportive parents would have higher levels of physical activity and less sedentary behavior. However, children of Rewarder parents had the most MVPA and least sedentary behavior, although the difference was not statistically significant. One explanation for the lack of difference in child physical activity and sedentary behavior among the parent classes could be the homogeneity of the sample. Overall, this was a sample of active children. The 2018 Physical Activity Guidelines recommend 3 to 5-year-old children should be active for 180 minutes per day at any intensity.40 Children in this study obtained an average of 273.9 minutes of total of physical activity per day, of which 59.3 minutes were MVPA. This indicates a need to understand how patterns of physical activity and screen time practices may impact child behaviors in higher risk populations where children are less likely to be meeting
recommendations.
44
may be that factors related to children’s diet, including dietary intake or parent feeding practices, may have a stronger influence on adiposity.
Despite finding no differences in child outcomes among the parent classes, this study provides a foundation for future research to better understand the effect of physical activity and screen time parenting on children’s behaviors. Future studies can build on the identified patterns to understand the influence on child behaviors in other populations. Additionally, it will be important to explore other intermediary outcomes (e.g., child enjoy of physical activity, parent child relationship). For instance, a physical activity intervention targeting fathers and daughters showed an improvement in the father-daughter relationship.89 Finally, it will be important to examine how these parenting patterns change over time and the predictive value of these patterns on children’s later behaviors. It may be that differences in child behaviors may be more
pronounced later in childhood when children’s physical activity declines and sedentary behavior and adiposity increase. For example, the Activity Supportive pattern may mitigate declines in children’s physical activity over time compared to the other parenting patterns.
Although this study had a number of strengths including measurement of an array of parenting practices, objectively measured physical activity and sedentary behavior, and the use of latent profile analysis, there were several limitations. First, there may be additional indicator variables that would better predict class membership, as indicated by the low entropy value. Additionally, we did not use the 2-class model specified by the LMR-LRT, but rather relied on the BIC and interpretability as the defining factors for model selection. However, simulation studies have suggested that entropy is a poor indicator of model fit and that the BIC is one of the best predictors.141,142 Additionally, although we were able to measure a number of different
45
to measure a wide range of practices representing the four proposed parenting dimensions. Furthermore, the sample was predominantly mothers, limiting the generalizability to all parents. Research has shown that mothers and fathers parent differently around physical activity,83 so future work should seek to identify patterns of fathers’ physical activity practices. Finally, the sample was comprised of primarily well-educated and affluent families. It could be that parents with lower income may not have the time and resources to support children’s activity compared to parents in this sample, so more research is needed to understand the practices and patterns of more diverse families.
Conclusion