Abstract
Objective: The primary objectives are to implement the pharmacy consult program with
sustainable pharmacy student involvement in the dental school clinic and to demonstrate an improvement in patient health behaviors.
Design: This was a prospective pilot study with pre-post intervention evaluation
performed at the UNC School of Dentistry clinic from August 2016 through May 2017. Pre- and post-intervention surveys were administered to collect the students’
demographics, knowledge and confidence of each discipline’s scope of practice, and perceptions of inter-professional communication and teamwork.
Conclusions: Our prospective pilot program demonstrated the success of a pharmacy
Introduction
In the United States, chronic diseases including hypertension, hyperlipidemia, and diabetes continue to remain uncontrolled and impose a significant burden on the
population and the public health infrastructure in terms of economic cost, disability, and death.1,2 However, there is a lack of primary care providers to appropriately manage this burden alone, especially in rural and underserved areas. Team-based care in practice is needed to optimize patient outcomes and to help alleviate the shortage, it’s important to effectively utilize other members of the healthcare workforce. Pharmacists are well positioned within primary care and community pharmacy settings to assess patients with complex medication regimens and help manage chronic diseases by providing education on lifestyle changes, monitoring, and medication use. Prior studies have shown that pharmacist involvement in disease state management improves clinical outcomes and reduces healthcare costs.3-7 For decades, dental practices have also been involved in helping patients modify lifestyle habits to improve poor oral hygiene.8,9
In order for healthcare providers to provide safe team-based, patient-centered care, they must be trained to work collaboratively. The World Health Organization defines inter-professional education (IPE) as two or more professions
learning about, from, and with each other to enable effective collaboration and improve health outcomes.10 Of the existing healthcare collaborations, few studies have evaluated the impact of pharmacy and dental students’ interaction within the classroom
The Accreditation Council for Pharmacy Education Standard 11 details the need to prepare all pharmacy students to provide patient-centered care in a variety of practice settings as a contributing member of an inter-professional team with competency in team expectations, education, and practice.15 Commission on Dental Accreditation Standard 2-19 emphasizes that dental graduates must be competent in communicating and
collaborating with other members of the healthcare team.16 However, barriers to implementation of these standards exist and the call for intentional programs of team education and practice with a robust assessment platform is now.Thus, in order for learners of different disciplines to be ready for collaborative practice, they must
have intentional programs within their curricula to foster these relationships and acquire the Interprofessional Collaborative Practice Competencies.17
Training dentists and pharmacists early in their education and promoting collaboration has the potential to provide a lasting impact on patient care. Working together, the pharmacist and dentist will not only obtain an understanding of each other’s scope of practice, but will work as a team to help patients set goals in
overcoming psychosocial barriers and improving self-monitoring to improve chronic disease management. Therefore, pharmacists’ integration into a dental clinic setting to improve patient care while enhancing IPE through a consult model is a solution.
Methods Study Design
This was a prospective pilot study with pre-post intervention evaluation
clinic and pharmacy consult intervention model in August 2016. For the intervention, Doctor of Dental Surgery and Dental Hygiene students were asked to self-identify a patient that qualifies for an advance pharmacotherapy consult. Consult services included conducting medication histories, providing medication and/or chronic disease state counseling, answering medication-related inquiries, or conducting a patient profile review. Participants were expected to obtain at least one pharmacotherapy consult “intervention” during the academic year ending in May 2017.
Study Population
As part of their clinic requirements, eighty UNC School of Dentistry Doctor of Dental Surgery (DDS) third-year students and thirty-five UNC School of Dentistry Dental Hygiene (DH) second-year students obtained a pharmacotherapy consult for at least one of their patients. Twenty UNC Eshelman School of Pharmacy Doctor of Pharmacy students assisted in completing the pharmacotherapy consults as part of their experiential education. This study focused on the experiences of DDS and DH students. Data Collection
Pre- and post-intervention surveys were administered to collect the students’ demographics, knowledge and confidence of each discipline’s scope of practice, and perceptions of inter-professional communication and teamwork. These surveys included the modified Knowledge of Scope of Practice and Readiness for Interprofessional
Analysis
Descriptive statistics were used to analyze the collected demographic data. Paired t-test was used for the pre-post comparison of confidence in knowledge and RIPLS scores. These results were verified with non-parametric Wilcoxon signed rank test due to the small study population size.
Results Demographics
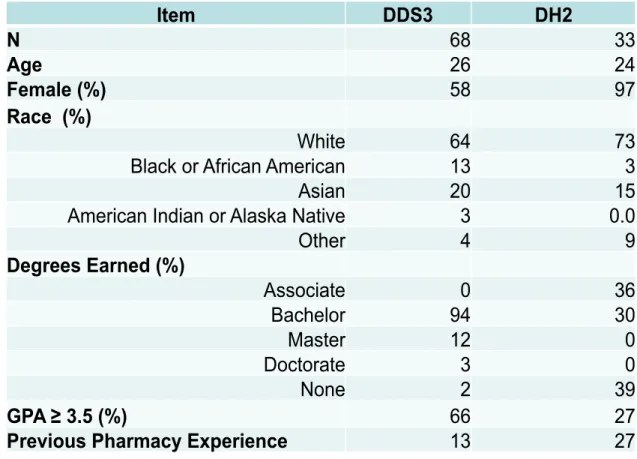
In total, sixty-eight DDS third-year students and thirty-three DH second-year students completed both the pre- and post- intervention surveys and were included in data analysis. Baseline characteristics of the participants are included in Table 1. Of note, DDS students tended to be older and to already possess a bachelor’s degree. This is to be expected as the DDS degree is a doctorate program, whereas a DH degree can be
Table 1. Baseline characteristics
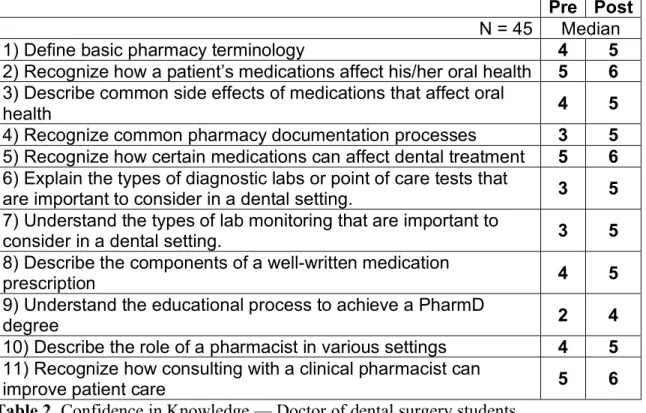
Confidence in Knowledge
We assessed DDS (Table 2) and DH (Table 3) students in the confidence in knowledge relating to pharmacy scope of practice and related topics. All DDS students who completed both surveys indicated that their pharmacy knowledge had improved as a result of the intervention program. Similar, DH students reported an increase in pharmacy knowledge in most areas, expect for basic pharmacy terminology and components of an appropriate written medication prescription.
Item
DDS3
DH2
N
68
33
Age
26
24
Female (%)
58
97
Race (%)
White
64
73
Black or African American
13
3
Asian
20
15
American Indian or Alaska Native
3
0.0
Other
4
9
Degrees Earned (%)
Associate
0
36
Bachelor
94
30
Master
12
0
Doctorate
3
0
None
2
39
GPA ≥ 3.5 (%)
66
27
Pre Post
N = 45 Median 1) Define basic pharmacy terminology 4 5
2) Recognize how a patient’s medications affect his/her oral health 5 6
3) Describe common side effects of medications that affect oral
health 4 5
4) Recognize common pharmacy documentation processes 3 5
5) Recognize how certain medications can affect dental treatment 5 6
6) Explain the types of diagnostic labs or point of care tests that
are important to consider in a dental setting. 3 5 7) Understand the types of lab monitoring that are important to
consider in a dental setting. 3 5
8) Describe the components of a well-written medication
prescription 4 5
9) Understand the educational process to achieve a PharmD
degree 2 4
10) Describe the role of a pharmacist in various settings 4 5
11) Recognize how consulting with a clinical pharmacist can
improve patient care 5 6
Table 2. Confidence in Knowledge — Doctor of dental surgery students Bolded values are significantly different.
Pre Post
N = 24 Median 1) Define basic pharmacy terminology 4 5 2) Recognize how a patient’s medications affect his/her oral health 5 6
3) Describe common side effects of medications that affect oral
health 5 6
4) Recognize common pharmacy documentation processes 2 5
5) Recognize how certain medications can affect dental treatment 4 6
6) Explain the types of diagnostic labs or point of care tests that
are important to consider in a dental setting. 2 4 7) Understand the types of lab monitoring that are important to
consider in a dental setting. 2 4
8) Describe the components of a well-written medication
prescription 3 4.5
9) Understand the educational process to achieve a PharmD
degree 2 4
10) Describe the role of a pharmacist in various settings 3 5
11) Recognize how consulting with a clinical pharmacist can
improve patient care 5 6
Readiness for Interprofessional Learning Scale
The modified RIPLS tool was used to assess dental students’ willingness to work and learn in an inter-professional environment. From the beginning of the experience, dental students indicated a general openness to collaborating with the pharmacy team for both learning and patient care purposes (Table 4). Post-test RIPLS results are not
reported, as there were no significant differences for any of the surveyed items.
RIPLS DDS3 Range DH2 Range
Learning with other dental (DDS), dental hygiene (DH), and pharmacy (PHARM) students will help me to become a more effective member of an inter-professional health care team
5 3-5 5 3-5
Patients will ultimately benefit if DDS/DH and PHARM students worked together to solve
patient problems 5 3-5 5 4-5
Shared learning with DDS/DH and PHARM students will increase my ability to understand clinical problems
5 3-5 5 3-5
Communication skills relevant for patient care should be learned with DDS/DH and PHARM students
4 3-5 5 3-5
For small group learning to work, DDS/DH and PHARM students need to trust and respect each other
5 3-5 5 4-5
Teambuilding skills are essential for DDS/DH
and PHARM students to learn 4 2-5 5 2-5 I don’t want to spend time learning with
DDS/DH and PHARM students 2 1-4 1 1-4 It is not necessary for DDS/DH and PHARM
students to learn together 2 1-4 1 1-3 The function of allied health members is
mainly to provide support for dentists and pharmacists
3 1-5 2 1-5
I have to acquire much more knowledge and
skills than other health care disciplines 3 1-5 3 1-5 Table 4. RIPLS Pre-test for DDS and DH students.
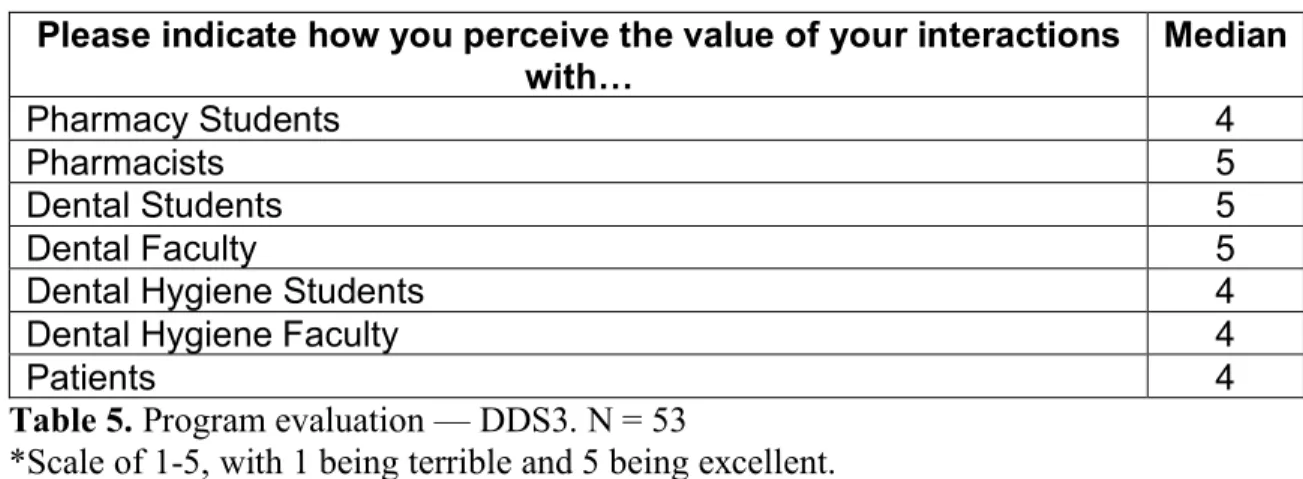
A total of fifty-three DDS3 students completed the final program evaluation (Table 5). Of note, twenty of the surveyed DDS3 students (38%) were able to obtain at least one advance pharmacotherapy consult, and the average number of inter-professional interactions experienced was 5.4 interactions. Forty-one of the DDS3 students who responded rated the pharmacy consult model experience as excellent or good.
Please indicate how you perceive the value of your interactions with…
Median
Pharmacy Students 4
Pharmacists 5
Dental Students 5
Dental Faculty 5
Dental Hygiene Students 4
Dental Hygiene Faculty 4
Patients 4
Table 5. Program evaluation — DDS3. N = 53
*Scale of 1-5, with 1 being terrible and 5 being excellent.
Overall, dental students had a positive experience with the pharmacy consult model at the dental clinic. From collaborating with pharmacy faculty, dental students stated they learned the importance of obtaining a complete medication history; how to counsel on proper diabetes care, medications, and symptoms and treatment of
hypoglycemia; and how to recognize common oral side effects of certain medications. By working with pharmacy students, dental students felt more comfortable asking
Dental students were also given the opportunity to provide feedback on their overall experience with the consult model. One strength was that dental students noticed how interdisciplinary collaboration better allowed them to provide holistic care to patients, and that benefitted the dental clinic patients overall. Dental students also stated that they felt the program was well organized and close interaction with pharmacy students allowed them to expand their understanding of another health discipline. A final common theme identified was that dental students expressed they had a better
understanding of how medications impact dental care.
Discussion
There are several ways to improve the pharmacy consult model for future iterations of the program. Dental students were expected to obtain at least one advance pharmacotherapy consult as part of their clinical experience requirements. However, not every dental student was able to meet this requirement. Potential reasons included
Some limitations with this pilot program was the limited study population, especially among dental hygiene students. One-third of dental students who completed the initial survey did not complete the post-survey. While all students were required to attend orientation at the beginning of the academic year where the pre-survey was administered, the post-survey was to be completed towards the end of the year once students had completed the intervention. As common with many students, the end of the semester is often overrun with many project deadlines and examinations, so it is possible that these students did not view it as urgent to complete the post-survey and program evaluation. Additionally, it is unclear how sensitive the RIPLS tool is for this specific population. From the pre- and post-data we were able to obtain, there was no significant difference in the RIPLS scores for either group of dental students. It is possible that the dental students at UNC are already exposed to other disciplines throughout the course of the undergraduate and graduate education or that our study population at baseline felt that they personally understood what inter-professional collaboration was. Both of these factors may have influenced why students’ mindset towards inter-professional learning was not significantly impacted by this experience.
Conclusions
References
1. Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States, 2014. Atlanta, GA: US Department of Health and Human Services; 2014.
2. Nwankwo T, Yoon SS, Burt V, et al. Hypertension among adults in the US: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief, No. 133. Hyattsville, MD: National Center for Health Statistics, Centers for Disease Control and Prevention, US Dept of Health and Human Services, 2013. 3. Snyder ME, Earl TR, Gilchrist S, et al. Collaborative drug therapy management:
case studies of three community-based models of care. Prev Chronic Dis 2015;12:140504
4. Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US pharmacists’ effect as team members on patient care: systematic review and meta-analyses. Med Care 2010;48:923–33
5. Chiquette E, Amato MG, Bussey HI. Comparison of an anticoagulation clinic with usual medical care: anticoagulation control, patient outcomes, and healthcare costs. Arch Intern Med 1998;158:1641–7.
6. Davidson MB, Karlan VJ, Hair TL. Effect of a pharmacist-managed diabetes care program in a free medical clinic. Am J Med Qual 2000;15:137–42.
7. Luder HR, Frede SM, Kirby JA, et al. TransitionRx: Impact of community
pharmacy postdischarge medication therapy management on hospital readmission rate. J Am Pharm Assoc 2015;55:246-54.
8. Lamster IB, Wolf DL. Primary healthcare assessment and intervention in the dental office. J Periodontol 2008; 79:1825-1832.
9. Elangovan S, Hertzman-Miller R, Karimbux N, et al. A framework for physician-dentist collaboration in diabetes and periodontitis. Clin Diabetes 2014;32:188– 192.
10.WHO, 2010. Framework for Action on Interprofessional Education & Collaborative Practice. Geneva: World Health Organization
11.Conway SE, Smith WJ, Truong TH, et al. Interprofessional pharmacy observation activity for third-year dental students. J Dent Educ 2014;78:1313-1318.
12.Formicola AJ, Andrieu SC, Buchanan JA, et al. Interprofessional education in U.S. and Canadian dental schools: an ADEA team study group report. J Dent Educ 2012;76:1250-1268.
13.Wilhelm M, Poirier T, Otsuka A, et al. Interprofessional ethics learning between schools of pharmacy and dental medicine. J Interprof Care 2014;28:478-480. 14.Palatta A, Cook BJ, Anderson EL, et al. 20 years beyond the crossroads: the path
to interprofessional education at U.S. dental schools. J Dent Educ 2015;79:982-996.
15.Accreditation Council for Pharmacy Education Standards 2016 16.Commission on Dental Accreditation Standards 2016
17.Interprofessional Education Collaborative Expert Panel. (2011). Core
18.American Pharmacists Association, National Association of Chain Drug Stores Foundation. Medication therapy management in community pharmacy practice: core elements of an MTM service (version 2.0). J Am Pharm Assoc 2008;48:341-353.
19.Exploring Pharmacists’ Role in a Changing Healthcare Environment.
Washington, DC: Avalere Health; May 2014. http://avalere.com/expertise/life-