Refereed papers
The role of the electronic medical record
(EMR) in care delivery development in
developing countries: a systematic review
Faustine Williams MS
Researcher, Health Management and Informatics
Suzanne Austin Boren PhD MHA
Assistant Professor, Health Management and Informatics
School of Medicine, University of Missouri, Columbia, USA
Introduction
Most countries in Europe and the USA are increasingly using an electronic medical record (EMR) due to the belief that it can help improve healthcare quality. Especially after Hurricane Katrina in 2005 the importance
of EMRs has been re-emphasised, since the hurricane destroyed or left inaccessible the medical records of an untold number of people. This focused new attention on the need for computerised medical records – health
ABSTRACT
Objective Most countries in Europe and the USA are increasingly using an electronic medical record (EMR) to help improve healthcare quality. Unfortunately, most developing countries face many challenges ranging from epidemics and civil wars to disasters: they also lack a robust healthcare infrastructure in the form of information and com-munications technology (ICT) to ensure continuity of patient health which many research studies con-sider a lifesaving resource. The aim of this system-atic review is to examine the benefits of an EMR and its contribution to the development of healthcare delivery in developing countries.
Methods We searched MEDLINE, PubMed, CINAHL, COMPENDEX and Academic Search Premier as well as systematically searching the reference lists of included studies and relevant reviews. Inclusion criteria were that studies should relate to the importance and challenges of an EMR system, paper-based medical records, development and implementation of an EMR system in devel-oping countries or EMR impact on care delivery in developing countries.
Results A total of 23 articles were identified that met the eligibility criteria. Articles identified were grouped into five non-exclusive areas: EMR benefits (n=4), challenges (n=6), transition from paper-based to EMR (n=5), EMR in developing countries (n=8) and pilot projects (n=5). Nine articles were excluded because three were not published in English and six were studies on EMR in developed countries.
Conclusions The potential of EMR systems to transform medical care practice has been recognised over the past decades, including the enhancement of healthcare delivery and facilitation of decision-making processes. Some benefits of an EMR system include accurate medication lists, legible notes and prescriptions and immediately available charts. In spite of challenges facing the developing world such as lack of human expertise and financial resource, most studies have shown how feasible it could be with support from developed nations to design and implement an EMR system that fits into this en-vironment.
records that follow patients, even if their doctors’ offices no longer exist. A disaster does not mean re-starting care from scratch. Unfortunately, most developing countries faced with challenges such as epidemics, civil wars and disasters, also lack robust healthcare infrastructure in the form of information and communications technology (ICT) to ensure the continuity of patient health which many research studies consider a lifesaving resource.
Good health is not only important for individuals, but also for governments because it plays a central role in achieving sustainable economic development and growth as well as effective use of resources.1 Un-fortunately, we live in a world where two thirds of the population lives in so-called ‘developing coun-tries’ under conditions grossly different from those in the richer industrialised countries.2The Okinawa Charter on the Global Information Society, adopted by leaders of the G8 countries at their summit in 2000, re-emphasised the importance of ICTs in the global development agenda.3 To ensure the Millennium Development Goals (MDGs) are achieved by 2015, the Socialist International has challenged the Organ-ization for Economic Cooperation and Development (OECD) countries to focus first on delivering Goal 8 – i.e. with additional and more effective aid, directed mainly to poor countries, and also more sustainable debt relief and more trade and technology oppor-tunities for these countries. The Socialist International has pointed out that for poor countries to realise the MDGs, an additional US$50 billion is needed in aid from OECD countries. Further urgent measures must be taken to fix the problems in the international trade systems that continue to prevent the world’s poor countries from trading themselves out of poverty.4
In spite of the importance of ICT and EMR systems in developing clinical care and policy in developed countries, there are still some problems or challenges that must be overcome. Among them are hardware and software compatibility, training, lack of quality control and antiquated infrastructure.5Some researchers also believe data collected in developing countries are incomplete, inaccurate, unreliable and not timely, therefore the potentials of EMRs may not be realised.6 There is the fear that the use of an EMR system might expedite the dissemination of wrong or poor data which does not represent the truth, hence the slow pace of development.6Irrespective of these challenges the aim of this study is to examine EMR benefits to the patients, physicians and other care providers as well as its ultimate contribution to development of health-care delivery in developing countries.
Methods
Data sources
Medline (1966–2007), CINAHL (1982–2007), COMPENDEX (1980–2007) and Academic Search Premier (1984–2007) were searched using combin-ations of the following search terms: electronic medical records OR informatics computerised OR informa-tion storage and retrieval OR medical informatics OR computer-assisted decision making OR information systems OR hospital information systems AND devel-oping countries. We also systematically searched the reference lists of articles retrieved. There was no limit-ation of publiclimit-ation date in the search; however, the earliest eligible article was published in 1995.
Inclusion and exclusion criteria
Our inclusion criteria were studies relating to the importance and challenges of an EMR system, medical records, development and implementation of an EMR system in developing countries, and EMR impact on care delivery in developing countries. We excluded studies that were not published in English as well as those that were not on developing countries.
Results
While there have been many papers on EMRs or computer-based patient records, there exists only a few articles significant to this research area in devel-oping countries. In all, 32 articles were identified, but based on the aforementioned selection criteria 23 articles were considered eligible.2,5–26
Benefits of EMR systems
is that care givers never have to worry about finding a chart, since information concerning the patient is already input into the computer.
Another important element of an EMR is legibility of clinical notes.7–9An EMR provides documentation in a computerised format that allows for data or records to be printed in text form rather than hand written. Also the computer makes spelling, validity and range checks which prompt users when data entry error is detected. An EMR also increases efficiency of healthcare providers’ workflow. Thus, data entered into the hospital information system (HIS) can be used to refer a patient to a specialist. Also, epidemiologists, researchers, physicians and other clinicians can extract information from HISs to protect and promote the health of the population through efficient surveil-lance, investigation, prevention and control of com-municable diseases of public health importance. Further, an EMR allows care providers an opportunity to be abreast of patient health status. For instance, by creating shortcuts to documents warning about abnormal laboratory examination results, prescriptions and drug administration, physicians are able to quickly provide feedback to patients without any difficulties. Other benefits of EMRs include data accessibility by multiple users and continuous data processing as well as auto-matic data back up and stored at different locations outside the hospital or clinics so that in case of disaster access to the record will not be denied.7,9
Challenges of EMR systems
Despite EMRs’ importance there are some challenges that must be considered when designing and imple-menting EMR systems. One limitation is lack of hard-ware and softhard-ware standardisation. Although standards reduce development costs, increase integration and facilitate the collection of meaningful aggregate data for quality improvement and health policy develop-ment,5due to the complexity and different needs of each of the units/departments within the healthcare industry, maintaining technological standards is always difficult. As a result, each department usually imple-ments its own technology pertaining to the needs of that unit, which makes it impossible for all systems within the hospital system to communicate. Further, lack of such standardisation makes it harder to auto-matically generate the alerts which are necessary for decision making.10Similarly, a survey of US primary care physicians identified 264 different EMRs in use.7 Consequently, EMR systems development has had problems of proprietary and incompatibility.
Other limitations include too many data sources, privacy, confidentiality and security issues and cost.5,10–14,27Security is a very important issue, but it is essential that the appropriate users are not denied
access when the information is needed. It is true that hospitals need robust ICT infrastructures, particularly in terms of hardware and software, but the cost of such technology is highly capital intensive, therefore small hospitals and developing countries especially find it difficult to embark on. Also, due to the heavy cost involved, any decision to implement an EMR should be a strategic one involving all leaders from every segment of the healthcare institution to facilitate the design, implementation and maintenance of the sys-tem. Further, due to fear, change is often considered a threat. Yet without adequate involvement of the users of the system, the project can never be developed, implemented and maintained successfully.28
Transition from paper-based to EMR
systems
Converting from a paper-based to an EMR system is complex and difficult because it represents a paradigm shift for the work of physicians and other staff. The transition requires a systematic activity and must be managed from many aspects ‘clinically, administrat-ively, culturally, and organisationally. The transition must include not only the process changes inherent in the use of a new tool, but also the technical and procedural training, and the resultant changes to physician and staff roles within the office.’15 Subse-quently, it requires a strong management commit-ment and motivation.16Secondly, involvement of all stakeholders, care providers and other users of the system right from the beginning is necessary for survival and sustenance of the project. Involving the stakeholders will help them to have a clear understand-ing of why the organisation is makunderstand-ing the change. Involvement and understanding also helps users (care providers) to identify themselves with activities that will make the transition very smooth to achieve desir-able outcomes.
During this process, care must be taken not to impact the patient–physician relationship or the in-tegrity of the clinical processes covered. Some factors to be considered during the process include: (i) cost of training, hardware and software; (ii) type of hardware and software; (iii) security of patient information; (iv) maintenance of patient privacy and confidentiality; (v) maintenance and integrity of medical record con-tent and (vi) continuity and quality of care must be maintained through the transition period.15
EMR systems in developing countries
resources vital for strategic policy making to either acquire, train, or accommodate informatics profes-sionals to handle the design and implementation of systems to meet their needs.17–19Again due to lack of funds and high costs of repair, developing countries are not able to draw up maintenance plans to sustain the few computers and other equipment donated by philanthropists.
Some researchers believe data collected in devel-oping countries are incomplete, inaccurate, unreliable and not timely, therefore the potential of EMR systems may not be realised.6It is also suggested that the use of an EMR might expedite the dissemination of wrong or poor data which does not represent the truth, hence the slow pace of development.6Further, it is assumed that technology architectures designed for developed countries are appropriate and can easily fit into devel-oping countries’ environments. However, considering the differing cultural, organisational and environmental factors, it is essential for systems analysts and designers to research into these areas to design equipment per-taining to the needs of these countries. Finally, EMR implementation in developing countries requires human resources, funds, systematic collection of data and effective monitoring of the existing system. Gov-ernments, health managers and administrators have to exercise strong commitment, and invest in HISs to improve the health delivery status of their citizens. To bridge the digital divide between the north and south, it is essential for international agencies and corpor-ations to assist developing countries in the areas of technology and manpower developments in order to meet the demand of 21st century healthcare delivery.
Implementation of EMR systems in
developing countries
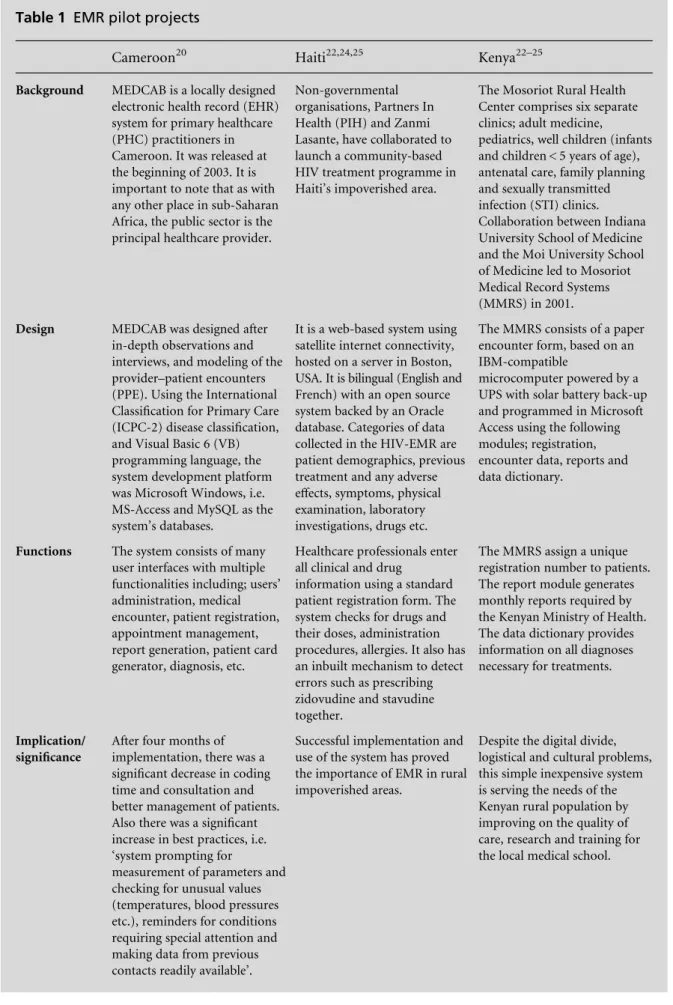
Availability of good quality data for continuity of care, decision making and allocation of limited resources in most developing countries, and especially sub-Saharan Africa, remains a mirage. Table 1 provides an overview of the design and implementation of three EMR projects. These projects illustrated the potentials of imple-menting EMR systems in developing countries despite the challenges. To facilitate effective and efficient data collection for policy making, evaluation, disease man-agement and quality care delivery, collaboration and involvement between developing countries and the developed world is required.
EMR impact on care delivery in
developing countries
EMR systems have been shown to be feasible and important in developing countries in spite of some
challenges. Some immediate benefits on care delivery development are as follows:
Patient care An EMR promotes effective and ap-propriate management of cases leading to quicker recovery without undue hospitalisation. The econ-omic impact can be seen in terms of speedy storage and retrieval of patient records thus reducing un-necessary costs of repeating diagnostic examinations over and over.14,18
Planning and management Incomplete and incor-rect information is leading to defective health plan-ning and management in most developing countries. Healthcare programs are failing because inaccurate data is used for planning. Access to accurate, correct and timely information could be a good source of data to plan and prepare for epidemics or disasters to prevent undue loss of life.7,18
Research ‘An effective HIS is indispensable in furthering medical research’.16Availability of quality data enhances identification of problems in treatment and finds solutions to prevent extra costs due to ineffec-tive treatment, thus making care delivery less expensive.
Discussion and conclusion
The potential of EMR systems to transform medical care practice has been recognised over the past decades including their ability to enhance healthcare delivery and facilitate decision-making processes. Consequently, EMR systems and other clinical decision support tools are currently used in both primary and secondary healthcare facilities in most developed nations. How-ever, implementing an EMR system or any HIS in a clinical practice is a daunting task. It requires good planning, strong management, clinical leadership and supportive staff. The most immediate benefits of EMR systems include accurate medication lists, legible notes and prescriptions, immediately available charts, de-creased chart pulls, lower transcription costs, medical errors reduction and improvement in quality care and standards in patient safety. Unfortunately, most devel-oping nations lack the experts, funds and ICT infra-structure necessary for the implementation of such modern healthcare technology to ensure continuity of care.
Table 1 EMR pilot projects
Cameroon20 Haiti22,24,25 Kenya22–25
Background MEDCAB is a locally designed electronic health record (EHR) system for primary healthcare (PHC) practitioners in Cameroon. It was released at the beginning of 2003. It is important to note that as with any other place in sub-Saharan Africa, the public sector is the principal healthcare provider.
Non-governmental organisations, Partners In Health (PIH) and Zanmi Lasante, have collaborated to launch a community-based HIV treatment programme in Haiti’s impoverished area.
The Mosoriot Rural Health Center comprises six separate clinics; adult medicine, pediatrics, well children (infants and children < 5 years of age), antenatal care, family planning and sexually transmitted infection (STI) clinics. Collaboration between Indiana University School of Medicine and the Moi University School of Medicine led to Mosoriot Medical Record Systems (MMRS) in 2001.
Design MEDCAB was designed after in-depth observations and interviews, and modeling of the provider–patient encounters (PPE). Using the International Classification for Primary Care (ICPC-2) disease classification, and Visual Basic 6 (VB) programming language, the system development platform was Microsoft Windows, i.e. MS-Access and MySQL as the system’s databases.
It is a web-based system using satellite internet connectivity, hosted on a server in Boston, USA. It is bilingual (English and French) with an open source system backed by an Oracle database. Categories of data collected in the HIV-EMR are patient demographics, previous treatment and any adverse effects, symptoms, physical examination, laboratory investigations, drugs etc.
The MMRS consists of a paper encounter form, based on an IBM-compatible
microcomputer powered by a UPS with solar battery back-up and programmed in Microsoft Access using the following modules; registration, encounter data, reports and data dictionary.
Functions The system consists of many user interfaces with multiple functionalities including; users’ administration, medical encounter, patient registration, appointment management, report generation, patient card generator, diagnosis, etc.
Healthcare professionals enter all clinical and drug
information using a standard patient registration form. The system checks for drugs and their doses, administration procedures, allergies. It also has an inbuilt mechanism to detect errors such as prescribing zidovudine and stavudine together.
The MMRS assign a unique registration number to patients. The report module generates monthly reports required by the Kenyan Ministry of Health. The data dictionary provides information on all diagnoses necessary for treatments.
Implication/ significance
After four months of implementation, there was a significant decrease in coding time and consultation and better management of patients. Also there was a significant increase in best practices, i.e. ‘system prompting for
measurement of parameters and checking for unusual values (temperatures, blood pressures etc.), reminders for conditions requiring special attention and making data from previous contacts readily available’.
Successful implementation and use of the system has proved the importance of EMR in rural impoverished areas.
to power rationing.23–25,29 Meanwhile, without reli-able and relevant HIS, healthcare providers cannot effectively plan, assess health needs of populations and groups, make decisions to allocate scarce resources to implement programmes, improve the quality of health, or address the numerous health issues facing them especially HIV–AIDS, tuberculosis, malaria and civil wars.
In spite of these challenges, implementation of computer-based medical record systems in Haiti, Kenya, Rwanda and Cameroon, using web-based systems with satellite internet connectivity and IBM compat-ible microcomputers powered by an uninterrupted power supply with solar battery back up, have shown how feasible it could be with support from developed nations to design and implement systems that fit into the developing world environment.20,22–25Finally, to avoid problems with inefficiencies and tie-in to ex-pensive software vendors regarding intellectual property rights and maintenance, developing countries can take advantage of various open source software (OSS) solutions that are available. Free and open-source software is not only ‘a useful and significant tool for the developing countries’, but clearly has the potential to help reduce the costs associated with IT investment because these codes are freely available for public use. They can easily be modified and tailored towards the needs of less developed countries, hence helping find solutions to the most pressing problems faced by the populations in these countries.24–26,30,31
REFERENCES
1 Godal T. Do we have the architecture for health aid right? Increasing global aid effectiveness.Nature Reviews Microbiology2005;3:899–903.
2 Tolmie CJ and Plessis JP. The use of knowledge-based systems in medicine in developing countries: a luxury or a necessity?Methods of Information in Medicine1997; 36:154–9.
3 United Nations ICT Task Force.Tools for Development: using information and communications technology to achieve the Millennium Development Goals. 2003. 4 Socialist International.Declaration on the Millennium
Development Goals. 2005. www.socialistinternational. org
5 Shortliffe EH and Perreault LE (eds). Medical Informatics: computer applications in health care and biomedicine(2e). New York: Springer, 2001.
6 Simba DO. Application of ICT in strengthening health information systems in developing countries in the wake of globalization.African Health Sciences2004;4:195–9. 7 Fraser HSF, Biodich P, Moodley D, Choi S, Mamlin BW
and Szolovits P. Implementing electronic medical rec-ord systems in developing countries. Informatics in Primary Care2005;14:83–95.
8 Levesque Y.Going Paperless with Minimal Pain. 2001. www.chmonline.ca/issue/article.jsp?content=20010201_ 270128_9928
9 Powsner SM, Wyatt JC and Wright P. Opportunities for and challenges of computerization.The Lancet 1998; 352:1617–22.
10 Tomasi E, Facchini LA and Maia MFS. Health infor-mation technology in primary health care in developing countries: a literature review. Bulletin of the World Health Organization2004;82:867–74.
11 McDonald CJ. The barriers to electronic medical record systems and how to overcome them. Journal of the American Medical Informatics Association1997;4:213– 21.
12 Bates DW, Ebell M, Gotlieb E, Zapp J and Mullins HC. A proposal for electronic medical records in the US pri-mary care.Journal of the American Medical Informatics Association2003;10:1–10.
13 Dick RS and Steen EB (eds).The Computer-based Patient Record: an essential technology for health care. Washington, DC: National Academy Press, 1991.
14 Miller RH and Sim I. Physicians’ use of electronic medical records: barriers and solutions.Health Affairs
2004;23:116–26.
15 College of Physicians and Surgeons of Alberta Guideline. Transition to electronic medical records. 2005. www. cpsa.ab.ca.publicationsresources/attachements_policies/ Transition%20t0%20Electronic%20Medical%20Records. pdf
16 Ginneken AM. The computerized patient record: bal-ancing effort and benefit.International Journal of Medical Informatics2002;65:97–119.
17 Jayasuriya R. Health information from theory to prac-tice: lessons from a case study in a developing country.
Medinfo Proceedings1995;8:1603–7.
18 Osunlaja AA and Olabode JA. Role of an effective Hospital Information System in a depressed economy.
Methods of Information in Medicine1997;36:141–3. 19 Azubuike MC and Ehiri JE. Health information systems
in developing countries: benefits, problems, and pros-pects.The Journal of the Royal Society for the Promotion of Health1999;9:180–4.
20 Kamadjeu R, Tapang EM and Moluh RN. Designing and implementing an electronic health record system in primary care practice in sub-Saharan Africa: a case study from Cameroon.Informatics in Primary Care2005;13: 179–86.
21 Fraser HSF, Jazayeri D, Nevil Pet al. An information system and medical record to support HIV treatment in rural Haiti.British Medical Journal2004;329:1142–6. 22 Tierney WM, Rotich JK, Smith FE, Nii J, Einterz RM and
Hannan TJ. Crossing the ‘digital divide’: implementing an electronic medical record system in a rural Kenyan health center to support clinical and research. Proceed-ings of the AMIA Annual Symposium2002;792–5. 23 Rotich JK, Hannan TJ, Smith FE et al. Installing and
implementing a computer-based patient record system in sub-Saharan Africa: the Mosoriot Medical Record System. Journal of the American Medical Informatics Association2003;10:295–303.
25 Allen C, Jazayeri D and Miranda J. Experience in implementing the OpenMRS medical record system to support HIV treatment in Rwanda. Medinfo2007;12: 382–6.
26 Bergsjø P, Mlay J, Lie RT, Lie-Nielsen E and Shao JF. A medical birth registry at Kilimanjaro Christian Medical Centre.East African Journal of Public Health2007;4:1–4. 27 Goedert J. Finding the HIPAA mix.Health Data
Man-agement2005;12:48.
28 Leonard KJ. The role of patients in designing health information systems: the case of applying simulation techniques to design an electronic patient record inter-face.Health Care Management Science2004;7:275–84. 29 Davidson O, Kitiyi E, Nkomo J, Turner C and Sebitosi B.
Sustainable energy in sub-Saharan Africa. 2007. www. icsu-africa.org/sustainable_energy_rep_2007.pdf 30 Jayasuriya R. Managing information systems for health
services in a developing country: a case study using a contextualist framework.International Journal of Infor-mation Management1999;19:335–49.
31 Noronha F.Developing Countries from Free/Open Source Software. 2003. www.linusjournal.com/article/6884
CONFLICTS OF INTEREST
None.
ADDRESS FOR CORRESPONDENCE
Faustine Williams School of Medicine University of Missouri Columbia
MO 65211 USA
Tel: +1 (573) 7710 346 Email: [email protected]