PROFILING FOR KSHV AND OTHER HERPESVIRUSES IN VIVO IN CLINICAL SPECIMENS
Kristen Marie Tamburro
A dissertation submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of
Philosophy in the Curriculum in Genetics and Molecular Biology.
Chapel Hill 2013
Approved by:
Dirk Dittmer, PhD
Charles van der Horst, MD
Blossom Damania, PhD
Mark Heise, PhD
ABSTRACT
KRISTEN MARIE TAMBURRO: Profiling for KSHV and Other Herpesviruses In Vivo In Clinical Specimens
(Under the direction of Dirk Dittmer)
The 1994 discovery of Kaposi Sarcoma-associated herpesvirus (KSHV)
was an important finding, especially as the sharp rise in HIV infections in the
early 1990’s led to an explosive Kaposi Sarcoma (KS) epidemic in men who have
sex with men. This cancer-causing herpesvirus is the causative agent of three
diseases in addition to KS: Multicentric Castlemen Disease (MCD), Primary
Effusion Lymphoma (PEL), and the newly described condition KSHV
Inflammatory Cytokine Syndrome (KICS). By understanding viral gene
expression in human patients, we hope to better understand KSHV infection and
its diseases, with the hope to shed light on novel therapeutic techniques.
In order to quantify KSHV viral gene expression, I devised methods to
profile human clinical specimens using high-throughput qPCR. This technique
was used to profile microRNA expression and was published as a methods video
journal in the Journal of Visualized Experiments (Chugh, Tamburro, and Dittmer,
2010). The accompanying manuscript is found in the Appendix chapter. This
same high-throughput technique was employed in Chapter II to determine KSHV
In Chapter II, we hypothesized that HIV patients with newly diagnosed KS
in Malawi could potentially benefit from treatment with the antiherpesviral drug
Ganciclovir (GCV). This was addressed through a pilot study with the AIDS
Malignancy Consortium (AMC). By using qPCR to assess gene expression of
two viral kinases critical to drug responsiveness, we found evidence that 78% of
patients express aviral kinase and would potentially benefit from this therapy.
This finding is important, as it indicates that patients can be stratified for
treatment based on kinase expression in a tumor biopsy, which will maximize
potential effectiveness and limit waste of drugs in a resource limited setting. This
work will lead to upcoming treatment studies in this population.
Next, we used whole-genome KSHV transcriptome profiling to understand
whether all KS patients from the Malawian cohort express similar gene
expression profiles or if subgroups can be distinguished. Our results indicate the
gene expression profiles vary significantly between patients. Specifically, two
subpopulations were discovered- those with and those without high levels of
genome-wide transcription. Patients with high transcription levels demonstrated
significantly higher CD4 counts and KSHV viremia in plasma, although HIV
viremia, number of tumors, or size of biopsied lesion were not significantly
associated with KSHV transcription. This work is described in Chapter III.
In Chapter IV, we employed high-throughput DNA sequencing as a
method to diagnose co-infections in an end-stage AIDS patient. This was
published in the Journal Virology (Tamburro et al. 2012). The patient had minimal
the diagnosis of the newly described condition KSHV Inflammatory Cytokine
Syndrome (KICS). Additionally, sequencing uncovered a co-infection with
HHV6a, which may have accounted for Systemic Inflammatory Response
Syndrome (SIRS) that ultimately led to the patient’s death. Notable to the
research community, this work resulted in the first complete sequence of KSHV
using direct methods, rather than relying on pre-sequencing cloning or cell
ACKNOWLEDGEMENTS
The work that is presented here would not have been possible without
help and support from several people whom I would like to acknowledge.
First, I would like to thank my mentor Dirk Dittmer for accepting me as a
student in his lab, and for his guidance over the years. Despite my initial lack of
knowledge in the field of Virology upon joining the lab, Dirk was patient and
supportive. He allowed me to find my niche in the lab, supporting my decision to
apply for the Translational Medicine Training Grant program, and helping to aim
my project to make the most out of this program.
Additionally, I would like to thank the rest of my thesis committee-
Blossom Damania, Mark Heise, Ronald Swanstrom, and Charles van der Horst- I
appreciate all of your help in preparing me over the years and getting me to this
point in my career. I would especially like to thank my clinical co-mentor Charlie
van der Horst for helping me achieve my certificate in translational medicine and
for exposing me to the clinical aspect of research.
I would like to thank my lab members and members of the Damania lab for
their support and helpful conversations throughout the years. I am grateful for all
of their helpful comments in lab meetings and on a day-to-day basis. In
particular I would like to thank my lab roommate and friend Pauline Chugh for
I would like to thank my amazing friends from college and those that I met
along the way in graduate school. You know who you are- and I couldn’t have
gotten here without all of your support and friendship.
I would like to thank my incredible family for always supporting me and
helping me to succeed. Throughout my life, my parents have always been there
to support me and to celebrate every (even small) victory, and I am so grateful
for all that they have given me.
Lastly, I would like to thank my husband, Daniel Sweet. Dan has always
been in my corner and I am so grateful to have him to share my life with.
He is always there to listen and help me, both in life and in science. Dan is one
of the smartest and more optimistic person that I know, and I am lucky to have
his love and support.
TABLE OF CONTENTS
LIST OF FIGURES AND TABLES ... xii
LIST OF ABBREVIATIONS AND SYMBOLS ... xiv
I. INTRODUCTION ... 1
KAPOSI SARCOMA (KS) ... 1
CLASSIC KS ... 2
ENDEMIC KS ... 3
POTENTIAL COFACTORS IN CLASSIC AND AFRICAN ENDEMIC KS ... 3
IATROGENIC KS ... 4
AIDS-ASSOCIATED KS ... 6
KSHV ... 7
THE DISCOVERY OF AN INFECTIOUS CAUSE OF KS: KSHV ... 7
KSHV GENES AND GENOME ... 8
TRANSMISSION OF KSHV ... 9
OTHER KSHV-ASSOCIATED DISEASES ... 11
KSHV INFLAMMATORY CYTOKINE
SYNDROME (KICS) ... 13
TABLES AND FIGURES ... 15
REFERENCES ... 18
II. ART NAÏVE KAPOSI SARCOMA (KS) PATIENTS EXPRESS KSHV ORF21 AND ORF36 AND MAY BENEFIT FROM GANCICLOVIR THERAPY– AN AIDS MALIGNANCY CONSORTIUM STUDY (AMC-S001) ... 33
PREFACE ... 33
INTRODUCTION ... 34
METHODS ... 36
Study Setting ... 36
Design ... 36
Participants ... 36
Clinical Procedures ... 36
Laboratory Procedures ... 37
Statistical Analysis ... 38
Ethics ... 39
RESULTS ... 39
Population Structure ... 39
KSHV Viral Load does not Correlate with CD4 Count or HIV Viral Load ... 40
DISCUSSION ... 44
SUMMARY ... 48
TABLES AND FIGURES ... 49
REFERENCES ... 54
III. VARIATION IN GENE EXPRESSION PROFILE DISTINGUISHES SUBTYPES OF KAPOSI SARCOMA TUMORS ... 59
PREFACE ... 59
INTRODUCTION ... 60
METHODS ... 62
RESULTS ... 64
DISCUSSION ... 71
TABLES AND FIGURES ... 75
REFERENCES ... 85
APPENDIX ... 89
Appendix 3.1: PEA.R- Code to Calculate CT’ values ... 89
Appendix 3.2: R Code using PEA.R to Calculate CT’ ... 92
Appendix 3.3: R code to Determine Correlation Between Cluster Assignment and Clinical Characteristics ... 95
IV. VIRONOME OF KAPOSI SARCOMA-ASSOCIATED HERPESVIRUS-INFLAMMATORY CYTOKINE SYNDROME IN AN AIDS PATIENT REVEALS CO-INFECTION OF HUMAN HERPESVIRUS 8
AND HUMAN HERPESVIRUS 6A ... 102
PREFACE ... 102
INTRODUCTION ... 103
METHODS ... 105
DNA Extraction ... 105
Illumina Sequencing ... 105
Phylogenetic Comparison ... 106
Immunohistochemistry ... 107
RESULTS ... 107
DISCUSSION ... 114
CONCLUSIONS ... 116
TABLES AND FIGURES ... 117
REFERENCES ... 121
V. OVERVIEW OF FINDINGS AND FUTURE DIRECTIONS ... 124
CHAPTER II- ART NAÏVE KAPOSI SARCOMA (KS) PATIENTS EXPRESS KSHV ORF21 AND ORF36 AND MAY BENEFIT FROM GANCICLOVIR THERAPY– AN AIDS MALIGNANCY CONSORTIUM STUDY (AMC-S001) ... 124
CYTOKINE SYNDROME IN AN AIDS PATIENT
REVEALS CO-INFECTION OF HUMAN HERPESVIRUS
8 AND HUMAN HERPESVIRUS 6A ... 128
REFERENCES ... 130
APPENDIX I. PROFILING OF PRE-MICRO RNAS AND MICRO RNAS USING QUANTITATIVE REAL-TIME PCR (QPCR) ARRAYS ... 131
PREFACE ... 131
INTRODUCTION ... 132
METHODS ... 133
A.Setup Of Pre-miRNA Assay Using The Freedom Tecan Evo Robot ... 134
B.Setup Of Pre-miRNA Assay Using The Matrix Electronic Multichannel Pipette ... 135
SECRETS TO SUCCESS ... 137
REPRESENTATIVE RESULTS ... 138
DISCUSSION ... 140
TABLES AND FIGURES ... 143
FIGURES AND TABLES
Figure 1.1 Kaposi Sarcoma lesions and histology ... 15
Figure 1.2 KS Belt in Africa ... 16
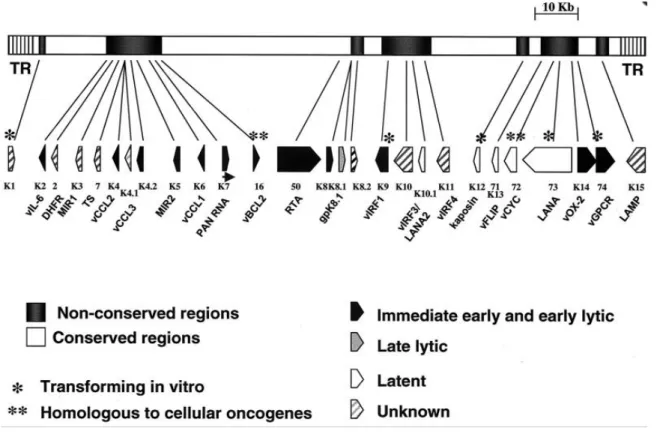
Figure 1.3 KSHV genome ... 17
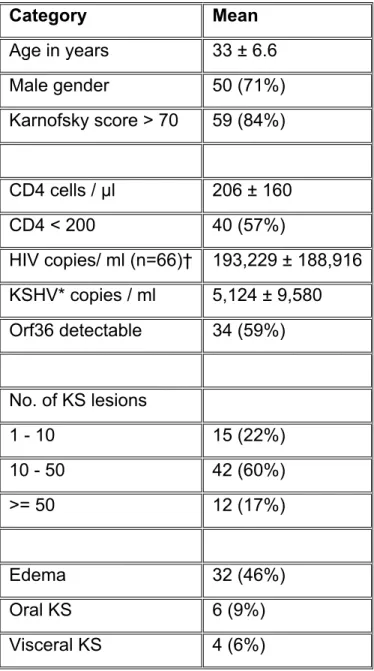
Table 2.1 Cohort characteristics (N=70, unless noted) of Kaposi sarcoma patients evaluated at Lighthouse ART clinic ... 49
Figure 2.1 Lack of correlations between KSHV viral load, CD4 count and HIV viral load in ART naïve patients presenting with HIV-associated KS in an endemic KSHV area ... 50
Figure 2.2 Evidence for different types of KS ... 52
Table 3.1 Cohort demographics for 66 therapy-naïve KS HIV+ patients in Lilongwe, Malawi ... 75
Figure 3.1 Sample and data analysis work flow chart ... 76
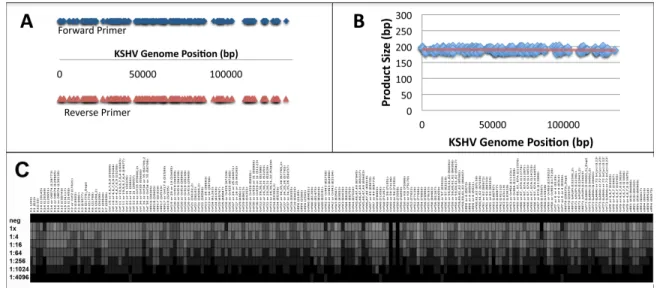
Figure 3.2 KSHV array characteristics and its validation ... 78
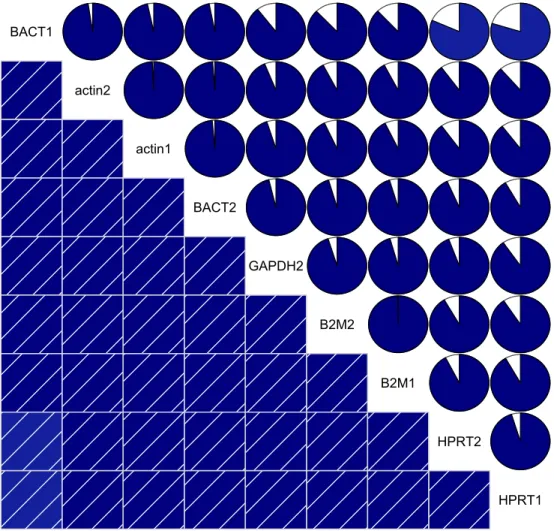
Figure 3.3 Correlation of reference genes ... 79
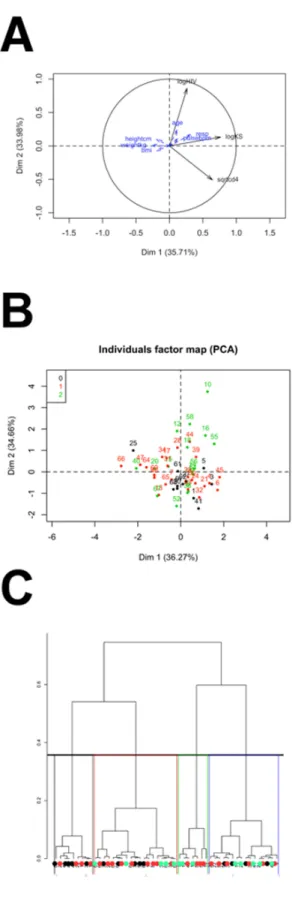
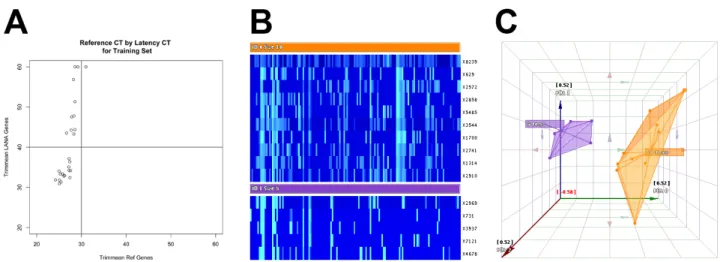
Figure 3.4 Gene expression profiling of training subset of samples indicate two distinct clusters of samples exist ... 80
Table 3.2 Significant primers (p<0.1) were identified from training data set ... 81
Figure 3.5 Gene expression analysis of 33 additional samples confirm two clusters of biopsies are distinguishable ... 82
Figure 3.6 There are significant differences in CD4 count between the two groups, but no difference in HIV or KSHV viremia ... 83
Figure 4.1 Patient was positive for Kaposi Sarcoma, as confirmed by autopsy, immunohistochemistry,
and PCR ... 117
Table 4.1 Comparison of viral loads for KSHV-associated
diseases, as compared to this case ... 118
Figure 4.2 Nextgen sequencing analysis reveals KSHV
and HHV6a coinfection ... 119
Table A1 Specific reagents and equipment ... 143
Figure A1 Pre-microRNA signatures emerge through
profiling using a novel qPCR-based array ... 144
Figure A2 Inclusion of internal controls in the
qPCR-based pre-microRNA array ... 146
Figure A3 Melting peak analysis of pre-microRNA primers
LIST OF ABBREVIATIONS AND SYMBOLS
ACTG AIDS Clinical Trials Group
AIDS Acquired Immune Deficiency Syndrome
AMC AIDS Malignancy Consortium
BAC Bacterial Artificial Chromosome
BCBL Body Cavity-Based Lymphoma
BP base pair
CD Castleman Disease
cDNA Complementary DNA
Cp/mL copies per mL
DNA Deoxyribonucleic acid
DR direct repeat
EBV Epstein-Barr virus
ELISA Enzyme-Linked Immunofluorescence Antibody
FLICE FADD-like IL-1B-converting enzyme
FLIP FLICE-like inhibitory domain
GAPDH Glyceraldehyde-3-Phosphate Dehydrogenase
HCMV Human Cytomegalovirus
HHV Human Herpesvirus
HIV Human Immunodeficiency Virus
HSV Herpes Simplex Virus
KS Kaposi Sarcoma
KSHV Kaposi Sarcoma-associated Herpesvirus
LANA Latency Associated Nuclear Antigen
MCD Multicentric Castleman Disease
miRNA microRNA
NTC No Template Control
ORF Open Reading Frame
PBMC Peripheral Blood Mononuclear Cell
PCR Polymerase Chain Reaction
PEL Primary Effusion Lymphoma
Pre-miRNA Precursor microRNA
Pri-miRNA Primary microRNA
RNA Ribonucleic Acid
RRE RTA Responsive Element
RTA Replication Transcription Activator
SIRS Systemic Inflammatory Response Syndrome
SNP Single Nucleotide Polymorphism
TPA 12-O-tetradecanoyl phorbol-13-acetate
TR Terminal Repeat
vFLIP viral FLICE-like inhibitory domain
vGPCR viral G-protein Coupled Receptor
CHAPTER I.
INTRODUCTION
Kaposi Sarcoma (KS)
The hungarian dermatologistMoritz Kaposi first described Kaposi
Sarcoma (KS) in 1872 as “an idiopathic multiple pigmented sarcoma of the
skin”(Kaposi, 1872). These red, vascular skin lesions were described in a
population of elderly men of Mediterranean descent, now known as the Classic
form of KS. Since the discovery of classic KS, three additional types of KS have
been designated, and named based on the population of patients that they
typically occur in: African endemic, transplant-associated iatrogenic, and
AIDS-associated (epidemic).
KS is a mesenchymal tumor that typically begins with multifocal patch
lesions on the skin or in the oral cavity (FIGURE 1.1 A, B). Lesions typically
either merge to form ulcerated plaques, or become hard solid nodular lesions
(Ganem, 2010). Edema surrounding the lesion and potentially involving the
entire foot, leg, or other regions is common. Aside from the skin, lesions of the
oral cavity and gastrointestinal tract can occur in approximately 10% of patients
(reviewed in (Iscovich et al., 2000)). Involvement of organs such as spleen, liver,
lung, and lymph node are less common in classic KS but observed in Acquired
At the histological level, KS is very complex and is identified by long
spindle cells forming slit-like vessels, extravasated red blood cells, and
inflammatory infiltrate (Boshoff and Weiss, 2001) (FIGURE 1.1 C, D). The cell
type that spindle cells originate from is debated, as they express markers for
endothelial cells including lymphatic markers and vascular endothelial cell
markers, as well as that of dendritic cells, smooth muscle cells, and
macrophages (Beckstead, Wood, and Fletcher, 1985) (Dupin et al., 1999) (Wang
et al., 2004) (Sturzl et al., 1992). KS tumorigenesis has been described as
consisting of three concurrent processes- proliferation, inflammation, and
angiogenesis (Ganem, 2010).
Classic KS
Classic KS, also known as sporadic KS, is the initially described form of
the disease defined by Moritz Kaposi (Kaposi, 1872). Classic KS is benign and
slow progressing, and typically begins with patch lesions on the lower limbs. It
occurs most commonly in elderly men of Mediterranean and Eastern European
Ashkenazi descent (Ross et al., 1985; Rothman, 1962) (Franceschi and Geddes,
1995). Other risk factors include geographic location, being over 65 years of
age, and being of male gender. The highest rates have been observed in the
Italian islands of Sicily and Sardinia (Cottoni, De Marco, and Montesu, 1996)
(Geddes et al., 1994) as well as in Greece (Touloumi et al., 1997). Low rates of
classic KS are reported in England, Wales, and Denmark (Grulich, Beral, and
caused by the herpesvirus Kaposi Sarcoma-associated herpesvirus (KSHV), and
it is likely that immune dysregulation plays a role in disease pathogenesis.
Endemic KS
While classic KS is a more moderate disease mostly limited to the
extremities, endemic of KS that occurs in Africa is highly aggressive. Both
adults and children suffer from KS (Ziegler and Katongole-Mbidde, 1996), and
the prognosis is poor if untreated. This is particularly true of the
lymphadenopathic form of the disease, which occurs in children and involves the
lymph nodes. It is typically fatal within 1 year of onset (reviewed in (Iscovich et
al., 2000)).
KS is the most common malignancy in East African men and the third
most common in women (Jemal et al., 2011). Importantly, high rates of KS
predated the AIDS epidemic in sub-Saharan Africa (Cook-Mozaffari et al., 1998).
For this reason, the region of Africa surrounding the equator is referred to as the
“KS Belt” (FIGURE 1.2).
Potential Cofactors in Classic and African Endemic KS
It is unclear whether geographic or genetic factors might be responsible
for the predisposition of KS in the HIV-negative population. Previous studies
have indicated that there is a higher incidence of KS in areas of Italy with more
for example on the island of Sardinia which has one of the highest rates of KS in
Europe (Cottoni, De Marco, and Montesu, 1996). Depletion of insects due to
DDT and other vector-control acts resulted in a decrease in KS (Coluzzi et al.,
2003) although it is unclear if this is an effect of the decrease in malaria or in
insect bites directly.
Additionally, volcanic clay salts have been proposed as a potential
cofactor for KS (reviewed in (Simonart, 2006)). In Africa as well as in the
volcanic region of the Mediterranean, iron bi-products are found in wet clay and
can enter the skin through sweat glands, possibly from the feet (Price and Plant,
1990) (Montella et al., 1996; Simonart et al., 1999). Poverty-stricken peasants
tend to walk barefoot and are also more likely to have KS, particularly in the
lower extremities (Ziegler et al., 2003; Ziegler, 1993; Ziegler et al., 1997). Iron
also increases the risk for many cancers (Weinberg, 1996) (Huang, 2003), and it
is possible that consuming foods and water containing high levels of iron could
also be playing a role in the predisposition to KS in these regions (Simonart,
2006).
Iatrogenic KS
Iatrogenic KS occurs in transplant recipients on immunosuppressant
therapy, such as steroids (Penn, 1997; Trattner et al., 1993). Unlike classic KS,
males and females have approximately equal rates of iatrogenic KS (reviewed in
(Hardy et al., 1976); Penn, 1988). Transplant patients in the US have
population (Penn, 1988). Additionally, iatrogenic KS is more common in regions
where KS is more prevalent, such as Jewish transplant recipients. In Saudi
Arabia, KS is the most common transplant-associated cancer (Qunibi et al.,
1988).
Iatrogenic KS is commonly seen in renal transplant patients, and is rare in
heart, liver, lung, or bone marrow transplant recipients (reviewed in (Iscovich et
al., 2000)) (Gentile et al., 2005). Lesions typically occur approximately 2 years
after pre-transplant therapy, and the average age of onset is 42 years (Penn,
1979) (Penn, 1988). Although both host and donor KSHV infection has been
proposed as the underlying cause for KS, it seems that reactivation of an
underlying host KSHV infection in the immune suppressed setting is likely
responsible (Becuwe et al., 2005). High KSHV viremia in renal transplant
patients is associated with a greater risk for developing KS (Weigert et al., 2004),
supporting the idea that host KSHV is an important factor in developing KS.
Tumors can regress with reduction of immune suppressants and
restoration of the immune system (Penn, 1988) (Trattner et al., 1993) (Frances,
1998). Additionally, treatment with an mTOR inhibitor Rapamycin (also known as
Sirolimus) has anti-angiogenic function (Guba et al., 2004) and has been
effective in regression of KS (Campistol, Gutierrez-Dalmau, and Torregrosa,
AIDS-Associated KS
The last but possibly most important population of people with KS is in
AIDS patients. 15-20% of AIDS patients develop KS, and it is the most common
cancer in this population (Beral et al., 1990; Nguyen et al., 2008) as AIDS
patients have an approximate 3000 to 5000-fold increased risk for developing KS
over the general population (Grulich et al., 2007; Mesri, Cesarman, and Boshoff,
2010).
In the 1980’s, rare diseases including KS and Pneumocystis carinii
pneumonia (Gottlieb et al., 1981; Hymes et al., 1981), were diagnosed at an
increased frequency in men who have sex with men (MSM) in the metropolitan
areas of New York and San Francisco. This led to the discovery of Human
Immunodeficiency Virus (HIV) and AIDS. It is now understood that HIV causes a
progressive loss of CD4+ T cells resulting in a deficient immune system that is
unable to fight infections (Friedman-Kien, 1981; Gottlieb et al., 1981) (Masur et
al., 1981) (reviewed in (Mildvan et al., 1982)). KS was described as
AIDS-defining (Longo et al., 1984), and was commonly the first sign of an underlying
HIV infection or progression to AIDS (reviewed in (Martin et al., 1998)). Today,
KS is still observed more frequently in AIDS patients despite being rare in the
general population, and remains among the leading cause of death of AIDS
patients today. In up to a third of HIV+ patients that carry KSHV, KS may reoccur
despite successful antiretroviral therapy (ART) (Krown, Lee, and Dittmer, 2008;
my work and justification for the continual search for novel methods of treating
KSHV-associated disease.
KSHV
The Discovery of an Infectious Cause of KS: KSHV
In 1994, Chang and Moore began the search for an infectious cause of
KS, on the premise that an infectious etiology would explain the epidemic in
immunocompromised patients, as a latent infection is able to flourish in this
setting (Chang et al., 1994). They used Representational Difference Analysis to
compare DNA from a KS biopsy and normal skin of the same AIDS patient, and
discovered the herpesvirus that they named Kaposi Sarcoma-associated
Herpesvirus (KSHV) (Chang et al., 1994) also known as Human Herpesvirus 8
(HHV8) (Levy, 1995).
Since its discovery, KSHV has been demonstrated to be in monocytes in
KS biopsies by immunohistochemistry (Blasig et al., 1997), and detected in
PBMCs, saliva, and plasma of KS patients (Carvalho et al., 2010; Humphrey et
al., 1996; Koelle et al., 1997; Miller et al., 2006; Vieira et al., 1997), as well as in
semen, albeit to a lesser extent (Pellett et al., 1999). Antibodies to KSHV have
been detected in blood via enzyme-linked immunofluorescence antibody (ELISA)
assays, western blots, and immunohistochemistry (Edelman, 2005; Tedeschi,
Dillner, and De Paoli, 2002). Because it is identifiable in every lesion (IARC,
1999), and cause disease in healthy individuals (Moore et al., 1996; Whitby et al.,
1995), KSHV is widely accepted as the causative agent of KS (Koch, 1884).
KSHV Genes and Genome
In every case where it has been examined, 100% of KS tumors are
positive for Kaposi Sarcoma-associated Herpesvirus (KSHV, HHV8) (Chang et
al., 1994). The KSHV genome is a linear double-stranded DNA genome of
approximately 165kb in length. 140kb comprise approximately 87 open reading
frames (ORFs), while the additional sequence makes up the terminal repeat
regions that flank both ends of the viral genome (Ganem, 2010). KSHV-specific
ORFs have been named K1 through K15, based on their location in the viral
genome, while the remaining genes have homology to related alpha and beta
herpesviruses.
KSHV belongs to the subgroup gammaherpesvirus, with its closest
human-tropic relative being Epstein-Barr Virus (EBV). As a member of the
herpesviridae family of viruses, KSHV can undergo both lytic and latent life
cycles or infections. During latency, few viral genes are expressed (FIGURE
1.3). The latency genes include the Latency Associated Nuclear Antigen (LANA,
Orf73), viral cyclin homolog (v-cyclin, Orf72), viral FLICE inhibitory protein
(vFLIP, Orf71), kaposin (K12) (Dittmer et al., 1998), and the KSHV miRNA’s (Cai
et al., 2005; Marshall et al., 2007; Pfeffer et al., 2005). The LANA protein
maintains the viral episome in an inactive state, tethered to the host
function to replicate the virus and modulate the host immune response (reviewed
in (West and Damania, 2010)). Reactivation begins with the transcription of
KSHV immediate early genes. Viral
Replication Transcriptional Activator gene
(RTA, Orf50) is known as the “lytic switch” and is critical in initiation of the
lytic cycle or viral replication. RTA and other early genes can in turn
control the expression of RTA Responsive Elements (RRE’s), either
through directly binding the promoter or through interactions with other
transcription factors. RREs include the immediate early and early genes
polyadenylated
nuclear RNA (PAN RNA), ORF6, ORF21, ORF57, ORF59,
ORF74, K1, K5, K8, K9, K12, K14, K15, and viral interleukin-6 (vIL-6)
(Hong et al., 2011). Expression of KSHV late genes includes viral
structural and capsid proteins necessary for the formation of new virions.
Transmission of KSHV
The mechanism of KSHV transmission is still debated. The discovery of
high levels of infectious viral particles in saliva (LaDuca et al., 1998; Lampinen et
al., 2000; Lucht et al., 1998; Vieira et al., 1997) suggests that oral shedding may
be important in person-to-person transmission. Related herpesviruses CMV,
EBV, and HSV-1 can be contracted through oral transmission. Although
mother-to-child vertical transmission may occur rarely (Brayfield et al., 2003;
mothers as well as other children, particularly in regions where KSHV is endemic
or HIV is epidemic (Bourboulia et al., 1998; Malope et al., 2007; Minhas et al.,
2008). In Africa and regions of Europe where classic KS is observed, saliva is
likely an important method of transmission (Gessain et al., 1999; Kasolo,
Mpabalwani, and Gompels, 1997; Ziegler and Katongole-Mbidde, 1996).
Sexual transmission of KSHV is controversial. KSHV can be detected in
semen and in the female genital tract (Gupta et al., 1996; LaDuca et al., 1998;
Whitby et al., 1999). Studies have indicated sexual transmission is likely in MSM
(Beral et al., 1990; Martin et al., 1998; Smith et al., 1999), but possibly less likely
in heterosexuals (Engels et al., 2007; Smith et al., 1999) (de Sanjose et al.,
2009).
Transfusions and blood exchange as a result of drug use also serve as
potential means for transmission (Dodd, 2005) (Blackbourn et al., 1997) (Dollard
et al., 2005), although the low viremia and low prevalence in the healthy adult
population make this less of a threat than initially proposed (Engels et al., 1999;
Pica and Volpi, 2007). Similarly, although it is well known that transplant
recipients often develop KS lesions, it is unclear whether this is due to
reactivated host virus or virus from the donor organ, and both are likely (Becuwe
Other KSHV-associated Diseases
Primary Effusion Lymphoma (PEL)
Primary Effusion Lymphoma (PEL) is a body cavity-based lymphoma
(BCBL) defined by effusion in the pleural, pericardial, or peritoneal cavities
(Cesarman et al., 1995; Cesarman et al., 1996). This lymphoproliferative
disease is rare, and occurs mostly in AIDS patients but can occur in HIV-negative
persons as well (Klepfish et al., 2001). PEL is caused by KSHV and can occur
with or without EBV co-infection (Arvanitakis et al., 1996) (Komanduri et al.,
1996). Typically, PEL in HIV-negative patients is also EBV negative (Nador et
al., 1996) (Hamoudi et al., 2004). PEL progresses rapidly, and prognosis is
typically poor, with median survival of 2-6 months (Komanduri et al., 1996).
Similar to iatrogenic KS, PEL can occur in transplant recipients either alongside
KS or alone (Dotti et al., 1999; Jones et al., 1998). Unlike KS, PEL is monoclonal
and derived from B cells (Reviewed in (Wen and Damania, 2010)).
PEL cell lines have been established, and are a useful tool in studying
KSHV in vitro (Arvanitakis et al., 1996; Boshoff et al., 1998; Drexler et al., 1998;
Renne et al., 1996). PEL cell lines have high copy numbers of latent KSHV,
typically around 40-80 copies per cell (Ablashi et al., 2002). KSHV can be
reactivated by treating cells with sodium butyrate (Yu et al., 1999), a protein
kinase C-activator 12-O-tetradecanoyl phorbol-13-acetate (TPA) (Renne et al.,
1996), or the KSHV “lytic switch” gene RTA (Orf50) (Guito and Lukac, 2012;
Multicentric Castleman Disease (MCD)
The plasma cell variant of Castleman Disease (CD), known as multicentric
Castleman Disease (MCD) due to its presence in several lymph nodes, is
associated with KSHV (Soulier et al., 1995). Notably, the idiopathic localized
hyaline vascular form of CD is more common and has not been associated with
KSHV infection (Ablashi et al., 2002; Cronin and Warnke, 2009). MCD is a rare
condition that arises mostly in HIV-positive immune suppressed patients, and
less commonly in HIV-negative persons who are immunocompromised
(Polizzotto et al., 2012b). The prognosis for MCD patients is poor, and median
survival is approximately 2 years (reviewed in (Stebbing et al., 2008))
(Oksenhendler et al., 2000). MCD is characterized by severe flares of symptoms
including fever, night sweats, malaise, splenomegaly, anemia, thrombocytopenia,
fatigue, edema, high KSHV viral loads and elevated inflammatory markers
(Polizzotto et al., 2012a) (Oksenhendler et al., 1996) (Menke, Camoriano, and
Banks, 1992).
Diagnosis of MCD is dependent on immunohistochemical staining of a
lymph node biopsy (Oksenhendler et al., 1996) (Du et al., 2001). MCD is also
called multicentric angiofollicular hyperplasia due to its characteristic
immunohistochemical appearance of germinal center vascular proliferation. The
lymph node architecture is generally maintained, however the germinal center is
typically hypocellular and the interfollicular region is proliferated (Chadburn et al.,
2008) (Schmidt et al., 2008). KSHV-positive polyclonal IgM lambda cells are
viral interleukin-6 (vIL6) are expressed. Despite sharing molecular similarity of
approximately 25% (Neipel et al., 1997), vIL6 differs from its human homolog in
its ability to bind to the gp130 subunit directly without requiring the high affinity
IL6 receptor gp80 subunit (Molden et al., 1997). This results in an increased
activiy for vIL6, which may contribute to the high levels of inflammation
responsible for symptoms in MCD patients (reviewed in (Sin and Dittmer, 2012)).
KSHV Inflammatory Cytokine Syndrome (KICS)
KSHV Inflammatory Cytokine Syndrome (KICS) is a KSHV-associated
systemic inflammatory disease that has only been recently described (Uldrick et
al., 2010a). To date, only 4 publications exist on KICS- one of which is our case
study described in Chapter 4. The initial report describes a retrospective review
of six HIV-positive, KSHV-positive patients with a disease that symptomatically
mimics MCD, despite no pathological evidence of MCD (Uldrick et al., 2010b).
Symptoms included fevers, wasting, edema, anemia, thrombocytopenia, elevated
inflammatory markers, adenopathy, and splenomegaly, however MCD was
excluded after multiple attempts to confirm with lymph node biopsies. MCD was
not found in follow-up or autopsy, and symptoms were attributed to high levels of
IL6 and vIL6 production. Patients with KICS also had high KSHV load,
comparable to MCD patients, but significantly less than KS patients. Another
study found that KICS patients and MCD patients have more single nucleotide
infection, although it is unknown whether this co-infection is correlated with KICS
or if this was unique to this patient (Tamburro et al., 2012).
A working definition of KICS diagnosis was characterized as having
indicators from at least 2 of these categories- Symptoms, Laboratory
abnormalities, and Radiographic abnormalities- along with elevated C-reactive
protein, elevated KSHV load in PBMCs, and the exclusion of MCD by
pathological evaluation (Polizzotto et al., 2012b).
As this disease is currently poorly understood, treatment options are
unclear, although it is possible that patients may respond to antiviral drugs such
as Ganciclovir alone or in combination with Zidovudine, or Rituximab and
liposomal doxorubicin as these drugs have had some success in treating MCD
and KS (Cianfrocca et al., 2010; Northfelt et al., 1998; Polizzotto et al., 2012a;
TABLES AND FIGURES
FIGURE 1.1: Kaposi Sarcoma lesions and histology
(A) Gross lesions of KS on the palate of a patient with AIDS. (B) Nodular skin lesion seen in KS. (C) Histopathology of a nodular KS lesion, showing fascicles of elongated spindle cells and numerous slit-like neovascular spaces. (D) High-power image of KS spindle cells. All images reproduced from the CDC’s
FIGURE 1.2: KS Belt in Africa
Cumulative incidence from birth to age 64 years of endemic (non-HIV-related)
Kaposi’ sarcoma among men in Africa. Estimates are from Cook-Mozaffari et al.
FIGURE 1.3: KSHV Genome
Structure of the KSHV (HHV-8) genome. The central portion of the genome is
flanked by the terminal repeats, labeled TR. The KSHV genome contains close to
100 open reading frames. Many of these are conserved in most herpesviruses;
these are present in the conserved blocks (white boxes) and are not indicated.
Other open reading frames are unique to rhadinoviruses, gammaherpesviruses,
or KSHV and are present in more divergent areas of the genome (indicated by
gray boxes). ORFs that have homology with herpesvirus saimiri are assigned the
corresponding numbers, and ORFs without recognizable homologues were
REFERENCES
Ablashi, D. V., Chatlynne, L. G., Whitman, J. E., Jr., and Cesarman, E. (2002). Spectrum of Kaposi's sarcoma-associated herpesvirus, or human herpesvirus 8, diseases. Clin Microbiol Rev15(3), 439-64.
Arvanitakis, L., Mesri, E. A., Nador, R. G., Said, J. W., Asch, A. S., Knowles, D. M., and Cesarman, E. (1996). Establishment and characterization of a primary effusion (body cavity-based) lymphoma cell line (BC-3) harboring kaposi's sarcoma-associated herpesvirus (KSHV/HHV-8) in the absence of Epstein-Barr virus. Blood88(7), 2648-54.
Ascoli, V., Zambon, P., Manno, D., Guzzinati, S., Zorzi, M., Arca, B., Costantini, C., and Coluzzi, M. (2003). Variability in the incidence of classic Kaposi's sarcoma in the Veneto region, Northern Italy. Tumori89(2), 122-4.
Beckstead, J. H., Wood, G. S., and Fletcher, V. (1985). Evidence for the origin of Kaposi's sarcoma from lymphatic endothelium. Am J Pathol 119(2), 294-300.
Becuwe, C., Euvrard, S., Bosshard, S., Pouteil-Noble, C., Garnier, J. L., Lefrancois, N., Boillot, O., Kanitakis, J., Touraine, J. L., and Claudy, A. (2005). [Kaposi's sarcoma and organ transplantation: 22 cases]. Ann Dermatol Venereol132(11 Pt 1), 839-43.
Beral, V., Peterman, T. A., Berkelman, R. L., and Jaffe, H. W. (1990). Kaposi's sarcoma among persons with AIDS: a sexually transmitted infection?
Lancet335(8682), 123-8.
Blackbourn, D. J., Ambroziak, J., Lennette, E., Adams, M., Ramachandran, B., and Levy, J. A. (1997). Infectious human herpesvirus 8 in a healthy North American blood donor. Lancet349(9052), 609-11.
Blasig, C., Zietz, C., Haar, B., Neipel, F., Esser, S., Brockmeyer, N. H.,
Tschachler, E., Colombini, S., Ensoli, B., and Sturzl, M. (1997). Monocytes in Kaposi's sarcoma lesions are productively infected by human
herpesvirus 8. J Virol71(10), 7963-8.
Boshoff, C., Gao, S. J., Healy, L. E., Matthews, S., Thomas, A. J., Coignet, L., Warnke, R. A., Strauchen, J. A., Matutes, E., Kamel, O. W., Moore, P. S., Weiss, R. A., and Chang, Y. (1998). Establishing a KSHV+ cell line (BCP-1) from peripheral blood and characterizing its growth in Nod/SCID mice.
Boshoff, C., and Weiss, R. A. (2001). Epidemiology and pathogenesis of Kaposi's sarcoma-associated herpesvirus. Philos Trans R Soc Lond B Biol Sci 356(1408), 517-34.
Bourboulia, D., Whitby, D., Boshoff, C., Newton, R., Beral, V., Carrara, H., Lane, A., and Sitas, F. (1998). Serologic evidence for mother-to-child
transmission of Kaposi sarcoma-associated herpesvirus infection. JAMA 280(1), 31-2.
Brayfield, B. P., Phiri, S., Kankasa, C., Muyanga, J., Mantina, H., Kwenda, G., West, J. T., Bhat, G., Marx, D. B., Klaskala, W., Mitchell, C. D., and Wood, C. (2003). Postnatal human herpesvirus 8 and human immunodeficiency virus type 1 infection in mothers and infants from Zambia. J Infect Dis 187(4), 559-68.
Cai, X., Lu, S., Zhang, Z., Gonzalez, C. M., Damania, B., and Cullen, B. R. (2005). Kaposi's sarcoma-associated herpesvirus expresses an array of viral microRNAs in latently infected cells. Proceedings of the National Academy of Sciences of the United States of America102(15), 5570-5. Campistol, J. M., Gutierrez-Dalmau, A., and Torregrosa, J. V. (2004). Conversion
to sirolimus: a successful treatment for posttransplantation Kaposi's sarcoma. Transplantation77(5), 760-2.
Carvalho, K. S., Silvestre Ede, A., Maciel Sda, S., Lira, H. I., Galvao, R. A., Soares, M. J., Costa, C. H., Malaquias, L. C., and Coelho, L. F. (2010). PCR detection of multiple human herpesvirus DNA in saliva from HIV-infected individuals in Teresina, State of Piaui, Brazil. Rev Soc Bras Med Trop43(6), 620-3.
Cesarman, E., Chang, Y., Moore, P. S., Said, J. W., and Knowles, D. M. (1995). Kaposi's sarcoma-associated herpesvirus-like DNA sequences in AIDS-related body-cavity-based lymphomas. The New England journal of medicine332(18), 1186-91.
Cesarman, E., Nador, R. G., Aozasa, K., Delsol, G., Said, J. W., and Knowles, D. M. (1996). Kaposi's sarcoma-associated herpesvirus in non-AIDS related lymphomas occurring in body cavities. Am J Pathol149(1), 53-7.
Chadburn, A., Hyjek, E. M., Tam, W., Liu, Y., Rengifo, T., Cesarman, E., and Knowles, D. M. (2008). Immunophenotypic analysis of the Kaposi
Chang, Y., Cesarman, E., Pessin, M. S., Lee, F., Culpepper, J., Knowles, D. M., and Moore, P. S. (1994). Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi's sarcoma. Science266(5192), 1865-9.
Cianfrocca, M., Lee, S., Von Roenn, J., Tulpule, A., Dezube, B. J., Aboulafia, D. M., Ambinder, R. F., Lee, J. Y., Krown, S. E., and Sparano, J. A. (2010). Randomized trial of paclitaxel versus pegylated liposomal doxorubicin for advanced human immunodeficiency virus-associated Kaposi sarcoma: evidence of symptom palliation from chemotherapy. Cancer116(16),
3969-77.
Coluzzi, M., Calabro, M. L., Manno, D., Chieco-Bianchi, L., Schulz, T. F., and Ascoli, V. (2003). Reduced seroprevalence of Kaposi's
sarcoma-associated herpesvirus (KSHV), human herpesvirus 8 (HHV8), related to suppression of Anopheles density in Italy. Med Vet Entomol17(4), 461-4. Cook-Mozaffari, P., Newton, R., Beral, V., and Burkitt, D. P. (1998). The
geographical distribution of Kaposi's sarcoma and of lymphomas in Africa before the AIDS epidemic. Br J Cancer78(11), 1521-8.
Cottoni, F., De Marco, R., and Montesu, M. A. (1996). Classical Kaposi's sarcoma in north-east Sardinia: an overview from 1977 to 1991. Br J Cancer73(9), 1132-3.
Cronin, D. M., and Warnke, R. A. (2009). Castleman disease: an update on classification and the spectrum of associated lesions. Adv Anat Pathol 16(4), 236-46.
Dal Maso, L., Polesel, J., Ascoli, V., Zambon, P., Budroni, M., Ferretti, S., Tumino, R., Tagliabue, G., Patriarca, S., Federico, M., Vercelli, M., Giacomin, A., Vicario, G., Bellu, F., Falcini, F., Crocetti, E., De Lisi, V., Vitarelli, S., Piffer, S., Stracci, F., Serraino, D., Rezza, G., and Franceschi, S. (2005). Classic Kaposi's sarcoma in Italy, 1985-1998. Br J Cancer 92(1), 188-93.
de Sanjose, S., Mbisa, G., Perez-Alvarez, S., Benavente, Y., Sukvirach, S., Hieu, N. T., Shin, H. R., Anh, P. T., Thomas, J., Lazcano, E., Matos, E., Herrero, R., Munoz, N., Molano, M., Franceschi, S., and Whitby, D. (2009).
Geographic variation in the prevalence of Kaposi sarcoma-associated herpesvirus and risk factors for transmission. J Infect Dis199(10), 1449-56.
Dodd, R. Y. (2005). Human herpesvirus-8: what (not) to do? Transfusion45(4),
463-5.
Dollard, S. C., Nelson, K. E., Ness, P. M., Stambolis, V., Kuehnert, M. J., Pellett, P. E., and Cannon, M. J. (2005). Possible transmission of human
herpesvirus-8 by blood transfusion in a historical United States cohort.
Transfusion45(4), 500-3.
Dotti, G., Fiocchi, R., Motta, T., Facchinetti, B., Chiodini, B., Borleri, G. M., Gavazzeni, G., Barbui, T., and Rambaldi, A. (1999). Primary effusion lymphoma after heart transplantation: a new entity associated with human herpesvirus-8. Leukemia13(5), 664-70.
Drexler, H. G., Uphoff, C. C., Gaidano, G., and Carbone, A. (1998). Lymphoma cell lines: in vitro models for the study of HHV-8+ primary effusion
lymphomas (body cavity-based lymphomas). Leukemia12(10), 1507-17. Du, M. Q., Liu, H., Diss, T. C., Ye, H., Hamoudi, R. A., Dupin, N., Meignin, V.,
Oksenhendler, E., Boshoff, C., and Isaacson, P. G. (2001). Kaposi sarcoma-associated herpesvirus infects monotypic (IgM lambda) but polyclonal naive B cells in Castleman disease and associated
lymphoproliferative disorders. Blood97(7), 2130-6.
Dupin, N., Fisher, C., Kellam, P., Ariad, S., Tulliez, M., Franck, N., van Marck, E., Salmon, D., Gorin, I., Escande, J. P., Weiss, R. A., Alitalo, K., and
Boshoff, C. (1999). Distribution of human herpesvirus-8 latently infected cells in Kaposi's sarcoma, multicentric Castleman's disease, and primary effusion lymphoma. Proceedings of the National Academy of Sciences of the United States of America96(8), 4546-51.
Edelman, D. C. (2005). Human herpesvirus 8--a novel human pathogen. Virol J 2, 78.
Engels, E. A., Atkinson, J. O., Graubard, B. I., McQuillan, G. M., Gamache, C., Mbisa, G., Cohn, S., Whitby, D., and Goedert, J. J. (2007). Risk factors for human herpesvirus 8 infection among adults in the United States and evidence for sexual transmission. J Infect Dis196(2), 199-207.
Engels, E. A., Eastman, H., Ablashi, D. V., Wilks, R. J., Braham, J., and Manns, A. (1999). Risk of transfusion-associated transmission of human
herpesvirus 8. J Natl Cancer Inst91(20), 1773-5.
Franceschi, S., and Geddes, M. (1995). Epidemiology of classic Kaposi's sarcoma, with special reference to mediterranean population. Tumori 81(5), 308-14.
Friedman-Kien, A. E. (1981). Disseminated Kaposi's sarcoma syndrome in young homosexual men. J Am Acad Dermatol5(4), 468-71.
Ganem, D. (2010). KSHV and the pathogenesis of Kaposi sarcoma: listening to human biology and medicine. The Journal of clinical investigation120(4),
939-49.
Geddes, M., Franceschi, S., Balzi, D., Arniani, S., Gafa, L., and Zanetti, R. (1995). Birthplace and classic Kaposi's sarcoma in Italy. Associazione Italiana Registri Tumori. J Natl Cancer Inst87(13), 1015-7.
Geddes, M., Franceschi, S., Barchielli, A., Falcini, F., Carli, S., Cocconi, G., Conti, E., Crosignani, P., Gafa, L., Giarelli, L., and et al. (1994). Kaposi's sarcoma in Italy before and after the AIDS epidemic. Br J Cancer69(2),
333-6.
Gentile, G., Capobianchi, A., Volpi, A., Palu, G., Pica, F., Calistri, A., Biasolo, M. A., and Martino, P. (2005). Human herpesvirus 8 DNA in serum during seroconversion in allogeneic bone marrow transplant recipients. J Natl Cancer Inst97(13), 1008-11.
Gessain, A., Mauclere, P., van Beveren, M., Plancoulaine, S., Ayouba, A., Essame-Oyono, J. L., Martin, P. M., and de The, G. (1999). Human herpesvirus 8 primary infection occurs during childhood in Cameroon, Central Africa. Int J Cancer81(2), 189-92.
Gottlieb, M. S., Schroff, R., Schanker, H. M., Weisman, J. D., Fan, P. T., Wolf, R. A., and Saxon, A. (1981). Pneumocystis carinii pneumonia and mucosal candidiasis in previously healthy homosexual men: evidence of a new acquired cellular immunodeficiency. N Engl J Med305(24), 1425-31. Grulich, A. E., Beral, V., and Swerdlow, A. J. (1992). Kaposi's sarcoma in
England and Wales before the AIDS epidemic. Br J Cancer66(6), 1135-7. Grulich, A. E., van Leeuwen, M. T., Falster, M. O., and Vajdic, C. M. (2007).
Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet 370(9581), 59-67.
Guba, M., Graeb, C., Jauch, K. W., and Geissler, E. K. (2004). Pro- and anti-cancer effects of immunosuppressive agents used in organ
Guito, J., and Lukac, D. M. (2012). KSHV Rta Promoter Specification and Viral Reactivation. Front Microbiol3, 30.
Gupta, P., Singh, M. K., Rinaldo, C., Ding, M., Farzadegan, H., Saah, A., Hoover, D., Moore, P., and Kingsley, L. (1996). Detection of Kaposi's sarcoma herpesvirus DNA in semen of homosexual men with Kaposi's sarcoma.
AIDS10(13), 1596-8.
Gutierrez-Ortega, P., Hierro-Orozco, S., Sanchez-Cisneros, R., and Montano, L. F. (1989). Kaposi's sarcoma in a 6-day-old infant with human
immunodeficiency virus. Arch Dermatol125(3), 432-3.
Hamoudi, R., Diss, T. C., Oksenhendler, E., Pan, L., Carbone, A., Ascoli, V., Boshoff, C., Isaacson, P., and Du, M. Q. (2004). Distinct cellular origins of primary effusion lymphoma with and without EBV infection. Leuk Res 28(4), 333-8.
Hardy, M. A., Goldfarb, P., Levine, S., Dattner, A., Muggia, F. M., Levitt, S., and Weinstein, E. (1976). De novo Kaposi's sarcoma in renal transplantation. Case report and brief review. Cancer38(1), 144-8.
Hassman, L. M., Ellison, T. J., and Kedes, D. H. (2011). KSHV infects a subset of human tonsillar B cells, driving proliferation and plasmablast
differentiation. J Clin Invest121(2), 752-68.
Hjalgrim, H., Melbye, M., Lecker, S., Frisch, M., Thomsen, H. K., and Larsen, S. O. (1996). Epidemiology of classic Kaposi's sarcoma in Denmark between 1970 and 1992. Cancer77(7), 1373-8.
Hong, Y., Qi, J., Gong, D., Han, C., and Deng, H. (2011). Replication and
transcription activator (RTA) of murine gammaherpesvirus 68 binds to an RTA-responsive element and activates the expression of ORF18. J Virol 85(21), 11338-50.
Huang, X. (2003). Iron overload and its association with cancer risk in humans: evidence for iron as a carcinogenic metal. Mutat Res533(1-2), 153-71. Humphrey, R. W., O'Brien, T. R., Newcomb, F. M., Nishihara, H., Wyvill, K. M.,
Ramos, G. A., Saville, M. W., Goedert, J. J., Straus, S. E., and Yarchoan, R. (1996). Kaposi's sarcoma (KS)-associated herpesvirus-like DNA
Hymes, K. B., Cheung, T., Greene, J. B., Prose, N. S., Marcus, A., Ballard, H., William, D. C., and Laubenstein, L. J. (1981). Kaposi's sarcoma in homosexual men-a report of eight cases. Lancet2(8247), 598-600. Iscovich, J., Boffetta, P., Franceschi, S., Azizi, E., and Sarid, R. (2000). Classic
kaposi sarcoma: epidemiology and risk factors. Cancer88(3), 500-17. Jemal, A., Bray, F., Center, M. M., Ferlay, J., Ward, E., and Forman, D. (2011).
Global cancer statistics. CA: a cancer journal for clinicians61(2), 69-90. Jones, D., Ballestas, M. E., Kaye, K. M., Gulizia, J. M., Winters, G. L., Fletcher,
J., Scadden, D. T., and Aster, J. C. (1998). Primary-effusion lymphoma and Kaposi's sarcoma in a cardiac-transplant recipient. N Engl J Med 339(7), 444-9.
Kaposi, M. (1872). Idiopathisches multiples Pigmentsarkom der haut. Archiv fur Dermatologie und Syphilis4, 265-73.
Kasolo, F. C., Mpabalwani, E., and Gompels, U. A. (1997). Infection with AIDS-related herpesviruses in human immunodeficiency virus-negative infants and endemic childhood Kaposi's sarcoma in Africa. J Gen Virol78 ( Pt 4),
847-55.
Klepfish, A., Sarid, R., Shtalrid, M., Shvidel, L., Berrebi, A., and Schattner, A. (2001). Primary effusion lymphoma (PEL) in HIV-negative patients--a distinct clinical entity. Leuk Lymphoma41(3-4), 439-43.
Koch, R. (1884). An Address on Cholera and its Bacillus. Br Med J2(1236), 453-9.
Koelle, D. M., Huang, M. L., Chandran, B., Vieira, J., Piepkorn, M., and Corey, L. (1997). Frequent detection of Kaposi's sarcoma-associated herpesvirus (human herpesvirus 8) DNA in saliva of human immunodeficiency virus-infected men: clinical and immunologic correlates. J Infect Dis176(1), 94-102.
Komanduri, K. V., Luce, J. A., McGrath, M. S., Herndier, B. G., and Ng, V. L. (1996). The natural history and molecular heterogeneity of HIV-associated primary malignant lymphomatous effusions. J Acquir Immune Defic Syndr Hum Retrovirol13(3), 215-26.
LaDuca, J. R., Love, J. L., Abbott, L. Z., Dube, S., Freidman-Kien, A. E., and Poiesz, B. J. (1998). Detection of human herpesvirus 8 DNA sequences in tissues and bodily fluids. J Infect Dis178(6), 1610-5.
Lampinen, T. M., Kulasingam, S., Min, J., Borok, M., Gwanzura, L., Lamb, J., Mahomed, K., Woelk, G. B., Strand, K. B., Bosch, M. L., Edelman, D. C., Constantine, N. T., Katzenstein, D., and Williams, M. A. (2000). Detection of Kaposi's sarcoma-associated herpesvirus in oral and genital secretions of Zimbabwean women. J Infect Dis181(5), 1785-90.
Levy, J. A. (1995). A new human herpesvirus: KSHV or HHV8? Lancet 346(8978), 786.
Longo, D. L., Steis, R. G., Lane, H. C., Lotze, M. T., Rosenberg, S. A., Preble, O., Masur, H., Rook, A. H., Fauci, A. S., Jacob, J., and et al. (1984).
Malignancies in the AIDS patient: natural history, treatment strategies, and preliminary results. Ann N Y Acad Sci437, 421-30.
Lucht, E., Brytting, M., Bjerregaard, L., Julander, I., and Linde, A. (1998). Shedding of cytomegalovirus and herpesviruses 6, 7, and 8 in saliva of human immunodeficiency virus type 1-infected patients and healthy controls. Clin Infect Dis27(1), 137-41.
Lukac, D. M., Renne, R., Kirshner, J. R., and Ganem, D. (1998). Reactivation of Kaposi's sarcoma-associated herpesvirus infection from latency by
expression of the ORF 50 transactivator, a homolog of the EBV R protein.
Virology252(2), 304-12.
Malope, B. I., Pfeiffer, R. M., Mbisa, G., Stein, L., Ratshikhopha, E. M., O'Connell, D. L., Sitas, F., MacPhail, P., and Whitby, D. (2007). Transmission of Kaposi sarcoma-associated herpesvirus between mothers and children in a South African population. J Acquir Immune Defic Syndr44(3), 351-5.
Marshall, V., Parks, T., Bagni, R., Wang, C. D., Samols, M. A., Hu, J., Wyvil, K. M., Aleman, K., Little, R. F., Yarchoan, R., Renne, R., and Whitby, D. (2007). Conservation of virally encoded microRNAs in Kaposi sarcoma--associated herpesvirus in primary effusion lymphoma cell lines and in patients with Kaposi sarcoma or multicentric Castleman disease. The Journal of infectious diseases195(5), 645-59.
Masur, H., Michelis, M. A., Greene, J. B., Onorato, I., Stouwe, R. A., Holzman, R. S., Wormser, G., Brettman, L., Lange, M., Murray, H. W., and
Cunningham-Rundles, S. (1981). An outbreak of community-acquired Pneumocystis carinii pneumonia: initial manifestation of cellular immune dysfunction. N Engl J Med305(24), 1431-8.
Menke, D. M., Camoriano, J. K., and Banks, P. M. (1992). Angiofollicular lymph node hyperplasia: a comparison of unicentric, multicentric, hyaline
vascular, and plasma cell types of disease by morphometric and clinical analysis. Mod Pathol5(5), 525-30.
Mesri, E. A., Cesarman, E., and Boshoff, C. (2010). Kaposi's sarcoma and its associated herpesvirus. Nat Rev Cancer10(10), 707-19.
Mildvan, D., Mathur, U., Enlow, R. W., Romain, P. L., Winchester, R. J., Colp, C., Singman, H., Adelsberg, B. R., and Spigland, I. (1982). Opportunistic infections and immune deficiency in homosexual men. Ann Intern Med 96(6 Pt 1), 700-4.
Miller, C. S., Berger, J. R., Mootoor, Y., Avdiushko, S. A., Zhu, H., and Kryscio, R. J. (2006). High prevalence of multiple human herpesviruses in saliva from human immunodeficiency virus-infected persons in the era of highly active antiretroviral therapy. J Clin Microbiol44(7), 2409-15.
Minhas, V., Crabtree, K. L., Chao, A., M'Soka T, J., Kankasa, C., Bulterys, M., Mitchell, C. D., and Wood, C. (2008). Early childhood infection by human herpesvirus 8 in Zambia and the role of human immunodeficiency virus type 1 coinfection in a highly endemic area. Am J Epidemiol168(3), 311-20.
Molden, J., Chang, Y., You, Y., Moore, P. S., and Goldsmith, M. A. (1997). A Kaposi's sarcoma-associated herpesvirus-encoded cytokine homolog (vIL-6) activates signaling through the shared gp130 receptor subunit. J Biol Chem272(31), 19625-31.
Montella, M., Franceschi, S., Geddes, M., Arniani, S., and Cocchiarella, G. (1996). Classic Kaposi's sarcoma and volcanic soil in southern Italy.
Lancet347(9005), 905.
Moore, P. S., Kingsley, L. A., Holmberg, S. D., Spira, T., Gupta, P., Hoover, D. R., Parry, J. P., Conley, L. J., Jaffe, H. W., and Chang, Y. (1996). Kaposi's sarcoma-associated herpesvirus infection prior to onset of Kaposi's
sarcoma. AIDS10(2), 175-80.
clinicopathologic entity associated with the Kaposi's sarcoma-associated herpes virus. Blood88(2), 645-56.
Neipel, F., Albrecht, J. C., Ensser, A., Huang, Y. Q., Li, J. J., Friedman-Kien, A. E., and Fleckenstein, B. (1997). Human herpesvirus 8 encodes a homolog of interleukin-6. J Virol71(1), 839-42.
Nguyen, H. Q., Magaret, A. S., Kitahata, M. M., Van Rompaey, S. E., Wald, A., and Casper, C. (2008). Persistent Kaposi sarcoma in the era of highly active antiretroviral therapy: characterizing the predictors of clinical response. AIDS22(8), 937-45.
Northfelt, D. W., Dezube, B. J., Thommes, J. A., Miller, B. J., Fischl, M. A., Friedman-Kien, A., Kaplan, L. D., Du Mond, C., Mamelok, R. D., and Henry, D. H. (1998). Pegylated-liposomal doxorubicin versus doxorubicin, bleomycin, and vincristine in the treatment of AIDS-related Kaposi's sarcoma: results of a randomized phase III clinical trial. J Clin Oncol16(7),
2445-51.
Oksenhendler, E., Carcelain, G., Aoki, Y., Boulanger, E., Maillard, A., Clauvel, J. P., and Agbalika, F. (2000). High levels of human herpesvirus 8 viral load, human interleukin-6, interleukin-10, and C reactive protein correlate with exacerbation of multicentric castleman disease in HIV-infected patients.
Blood96(6), 2069-73.
Oksenhendler, E., Duarte, M., Soulier, J., Cacoub, P., Welker, Y., Cadranel, J., Cazals-Hatem, D., Autran, B., Clauvel, J. P., and Raphael, M. (1996). Multicentric Castleman's disease in HIV infection: a clinical and pathological study of 20 patients. AIDS10(1), 61-7.
Pellett, P. E., Spira, T. J., Bagasra, O., Boshoff, C., Corey, L., de Lellis, L., Huang, M. L., Lin, J. C., Matthews, S., Monini, P., Rimessi, P., Sosa, C., Wood, C., and Stewart, J. A. (1999). Multicenter comparison of PCR assays for detection of human herpesvirus 8 DNA in semen. J Clin Microbiol37(5), 1298-301.
Penn, I. (1979). Kaposi's sarcoma in organ transplant recipients: report of 20 cases. Transplantation27(1), 8-11.
Penn, I. (1988). Tumors of the immunocompromised patient. Annu Rev Med39,
63-73.
Penn, I. (1997). Kaposi's sarcoma in transplant recipients. Transplantation64(5),
Pfeffer, S., Sewer, A., Lagos-Quintana, M., Sheridan, R., Sander, C., Grasser, F. A., van Dyk, L. F., Ho, C. K., Shuman, S., Chien, M., Russo, J. J., Ju, J., Randall, G., Lindenbach, B. D., Rice, C. M., Simon, V., Ho, D. D., Zavolan, M., and Tuschl, T. (2005). Identification of microRNAs of the herpesvirus family. Nat Methods2(4), 269-76.
Pica, F., and Volpi, A. (2007). Transmission of human herpesvirus 8: an update.
Curr Opin Infect Dis20(2), 152-6.
Polizzotto, M. N., Uldrick, T. S., Hu, D., and Yarchoan, R. (2012a). Clinical Manifestations of Kaposi Sarcoma Herpesvirus Lytic Activation:
Multicentric Castleman Disease (KSHV-MCD) and the KSHV Inflammatory Cytokine Syndrome. Front Microbiol3, 73.
Polizzotto, M. N., Uldrick, T. S., Hu, D., and Yarchoan, R. (2012b). Clinical Manifestations of Kaposi Sarcoma Herpesvirus Lytic Activation:
Multicentric Castleman Disease (KSHV-MCD) and the KSHV Inflammatory Cytokine Syndrome. Frontiers in microbiology3, 73.
Price, E. W., and Plant, D. A. (1990). The significance of particle size of soils as a risk factor in the etiology of podoconiosis. Trans R Soc Trop Med Hyg 84(6), 885-6.
Qunibi, W., Akhtar, M., Sheth, K., Ginn, H. E., Al-Furayh, O., DeVol, E. B., and Taher, S. (1988). Kaposi's sarcoma: the most common tumor after renal transplantation in Saudi Arabia. Am J Med84(2), 225-32.
Ray, A., Marshall, V., Uldrick, T., Leighty, R., Labo, N., Wyvill, K., Aleman, K., Polizzotto, M. N., Little, R. F., Yarchoan, R., and Whitby, D. (2012). Sequence analysis of Kaposi sarcoma-associated herpesvirus (KSHV) microRNAs in patients with multicentric Castleman disease and KSHV-associated inflammatory cytokine syndrome. The Journal of infectious diseases205(11), 1665-76.
Razonable, R. R., Brown, R. A., Humar, A., Covington, E., Alecock, E., and Paya, C. V. (2005). Herpesvirus infections in solid organ transplant patients at high risk of primary cytomegalovirus disease. J Infect Dis 192(8), 1331-9.
Renne, R., Zhong, W., Herndier, B., McGrath, M., Abbey, N., Kedes, D., and Ganem, D. (1996). Lytic growth of Kaposi's sarcoma-associated herpesvirus (human herpesvirus 8) in culture. Nat Med2(3), 342-6.
Ross, R. K., Casagrande, J. T., Dworsky, R. L., Levine, A., and Mack, T. (1985). Kaposi's sarcoma in Los Angeles, California. J Natl Cancer Inst 75(6),
Rothman, S. (1962). Some clinical aspects of Kaposi's sarcoma in the European and North American populations. Acta Unio Int Contra Cancrum18, 364-71.
Schmidt, S. M., Raible, A., Kortum, F., Mayer, F., Riessen, R., Adam, P., Gregor, M., and Bissinger, A. L. (2008). Successful treatment of multicentric
Castleman's disease with combined immunochemotherapy in an AIDS patient with multiorgan failure. Leukemia22(9), 1782-5.
Simonart, T. (2006). Role of environmental factors in the pathogenesis of classic and African-endemic Kaposi sarcoma. Cancer Lett244(1), 1-7.
Simonart, T., Van Vooren, J. P., Herbauts, J., and Boelaert, J. R. (1999). High incidence of Kaposi's sarcoma in Iceland and the Faroe Islands. Br J Cancer79(2), 373.
Sin, S. H., and Dittmer, D. P. (2012). Cytokine homologs of human gammaherpesviruses. J Interferon Cytokine Res32(2), 53-9.
Smith, N. A., Sabin, C. A., Gopal, R., Bourboulia, D., Labbet, W., Boshoff, C., Barlow, D., Band, B., Peters, B. S., de Ruiter, A., Brown, D. W., Weiss, R. A., Best, J. M., and Whitby, D. (1999). Serologic evidence of human herpesvirus 8 transmission by homosexual but not heterosexual sex. J Infect Dis180(3), 600-6.
Soulier, J., Grollet, L., Oksenhendler, E., Cacoub, P., Cazals-Hatem, D., Babinet, P., d'Agay, M. F., Clauvel, J. P., Raphael, M., Degos, L., and et al. (1995). Kaposi's sarcoma-associated herpesvirus-like DNA sequences in
multicentric Castleman's disease. Blood86(4), 1276-80.
Stallone, G., Schena, A., Infante, B., Di Paolo, S., Loverre, A., Maggio, G., Ranieri, E., Gesualdo, L., Schena, F. P., and Grandaliano, G. (2005). Sirolimus for Kaposi's sarcoma in renal-transplant recipients. N Engl J Med352(13), 1317-23.
Stebbing, J., Pantanowitz, L., Dayyani, F., Sullivan, R. J., Bower, M., and Dezube, B. J. (2008). HIV-associated multicentric Castleman's disease.
Am J Hematol83(6), 498-503.
Sturzl, M., Roth, W. K., Brockmeyer, N. H., Zietz, C., Speiser, B., and
Hofschneider, P. H. (1992). Expression of platelet-derived growth factor and its receptor in AIDS-related Kaposi sarcoma in vivo suggests
Sturzl, M., Wunderlich, A., Ascherl, G., Hohenadl, C., Monini, P., Zietz, C., Browning, P. J., Neipel, F., Biberfeld, P., and Ensoli, B. (1999). Human herpesvirus-8 (HHV-8) gene expression in Kaposi's sarcoma (KS) primary lesions: an in situ hybridization study. Leukemia13 Suppl 1, S110-2. Tamburro, K. M., Yang, D., Poisson, J., Fedoriw, Y., Roy, D., Lucas, A., Sin, S.
H., Malouf, N., Moylan, V., Damania, B., Moll, S., van der Horst, C., and Dittmer, D. P. (2012). Vironome of Kaposi Sarcoma-associated
herpesvirus-inflammatory cytokine syndrome in an AIDS patient reveals co-infection of human herpesvirus 8 and human herpesvirus 6A. Virology 433(1), 220-5.
Tappero, J. W., Conant, M. A., Wolfe, S. F., and Berger, T. G. (1993). Kaposi's sarcoma. Epidemiology, pathogenesis, histology, clinical spectrum, staging criteria and therapy. J Am Acad Dermatol28(3), 371-95.
Tedeschi, R., Dillner, J., and De Paoli, P. (2002). Laboratory diagnosis of human herpesvirus 8 infection in humans. Eur J Clin Microbiol Infect Dis21(12),
831-44.
Touloumi, G., Kaklamanis, L., Potouridou, I., Katsika-Hatziolou, E., Stratigos, J., Mueller, N., and Hatzakis, A. (1997). The epidemiologic profile of Kaposi's sarcoma in Greece prior to and during the AIDS era. Int J Cancer70(5),
538-41.
Trattner, A., Hodak, E., David, M., and Sandbank, M. (1993). The appearance of Kaposi sarcoma during corticosteroid therapy. Cancer72(5), 1779-83. Uldrick, T. S., Polizzotto, M. N., Aleman, K., O'Mahony, D., Wyvill, K. M., Wang,
V., Marshall, V., Pittaluga, S., Steinberg, S. M., Tosato, G., Whitby, D., Little, R. F., and Yarchoan, R. (2011). High-dose zidovudine plus valganciclovir for Kaposi sarcoma herpesvirus-associated multicentric Castleman disease: a pilot study of virus-activated cytotoxic therapy.
Blood117(26), 6977-86.
Uldrick, T. S., Wang, V., O'Mahony, D., Aleman, K., Wyvill, K. M., Marshall, V., Steinberg, S. M., Pittaluga, S., Maric, I., Whitby, D., Tosato, G., Little, R. F., and Yarchoan, R. (2010a). An interleukin-6-related systemic
inflammatory syndrome in patients co-infected with Kaposi sarcoma-associated herpesvirus and HIV but without Multicentric Castleman disease. Clin Infect Dis51(3), 350-8.
Uldrick, T. S., Wang, V., O'Mahony, D., Aleman, K., Wyvill, K. M., Marshall, V., Steinberg, S. M., Pittaluga, S., Maric, I., Whitby, D., Tosato, G., Little, R. F., and Yarchoan, R. (2010b). An interleukin-6-related systemic
sarcoma-associated herpesvirus and HIV but without Multicentric Castleman disease. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America51(3), 350-8.
Vieira, J., Huang, M. L., Koelle, D. M., and Corey, L. (1997). Transmissible Kaposi's sarcoma-associated herpesvirus (human herpesvirus 8) in saliva of men with a history of Kaposi's sarcoma. J Virol71(9), 7083-7.
Wang, H. W., Trotter, M. W., Lagos, D., Bourboulia, D., Henderson, S., Makinen, T., Elliman, S., Flanagan, A. M., Alitalo, K., and Boshoff, C. (2004). Kaposi sarcoma herpesvirus-induced cellular reprogramming contributes to the lymphatic endothelial gene expression in Kaposi sarcoma. Nat Genet 36(7), 687-93.
Weigert, A. L., Pires, A., Adragao, T., Cardoso, E., Cardoso, C., Sancho, R., Trindade, H., Pimentel, M. S., Casqueiro, A., and Machado, D. (2004). Human herpes virus-8 serology and DNA analysis in recipients of renal allografts showing Kaposi's sarcoma and their respective donors.
Transplant Proc36(4), 902-4.
Weinberg, E. D. (1996). The role of iron in cancer. Eur J Cancer Prev5(1), 19-36.
Wen, K. W., and Damania, B. (2010). Kaposi sarcoma-associated herpesvirus (KSHV): molecular biology and oncogenesis. Cancer Lett289(2), 140-50. West, J. A., and Damania, B. (2010). Kaposi's sarcoma-associated herpesvirus
and innate immunity. Future Virol5(2), 185-196.
Whitby, D., Howard, M. R., Tenant-Flowers, M., Brink, N. S., Copas, A., Boshoff, C., Hatzioannou, T., Suggett, F. E., Aldam, D. M., Denton, A. S., and et al. (1995). Detection of Kaposi Sarcoma-associated herpesvirus in peripheral blood of HIV-infected individuals and progression to Kaposi's sarcoma.
Lancet346(8978), 799-802.
Whitby, D., Smith, N. A., Matthews, S., O'Shea, S., Sabin, C. A., Kulasegaram, R., Boshoff, C., Weiss, R. A., de Ruiter, A., and Best, J. M. (1999). Human herpesvirus 8: seroepidemiology among women and detection in the genital tract of seropositive women. J Infect Dis179(1), 234-6.
Yu, Y., Black, J. B., Goldsmith, C. S., Browning, P. J., Bhalla, K., and Offermann, M. K. (1999). Induction of human herpesvirus-8 DNA replication and transcription by butyrate and TPA in BCBL-1 cells. J Gen Virol80 ( Pt 1),
Ziegler, J., Newton, R., Bourboulia, D., Casabonne, D., Beral, V., Mbidde, E., Carpenter, L., Reeves, G., Parkin, D. M., Wabinga, H., Mbulaiteye, S., Jaffe, H., Weiss, R., and Boshoff, C. (2003). Risk factors for Kaposi's sarcoma: a case-control study of HIV-seronegative people in Uganda. Int J Cancer103(2), 233-40.
Ziegler, J. L. (1993). Endemic Kaposi's sarcoma in Africa and local volcanic soils.
Lancet342(8883), 1348-51.
Ziegler, J. L., and Katongole-Mbidde, E. (1996). Kaposi's sarcoma in childhood: an analysis of 100 cases from Uganda and relationship to HIV infection.
Int J Cancer65(2), 200-3.
CHAPTER II:
ART NAÏVE KAPOSI SARCOMA (KS) PATIENTS EXPRESS KSHV
ORF21 AND ORF36 AND MAY BENEFIT FROM GANCICLOVIR
THERAPY– AN AIDS MALIGNANCY CONSORTIUM STUDY
(AMC-S001)
PREFACE
This work has been submitted to the Journal of Infectious Diseases and is
currently under review 1. Mina Hosseinipour designed the study along with Dirk
Dittmer, Jeanette Lee, and other members of the AIDS Malignancy Consortium
(AMC). I performed all experiments, analyzed the data, and assisted with
making the tables and figures and drafting the manuscript. Dirk performed much
of the statistical analysis, and wrote the manuscript together with Mina and
myself. Jie Xiong assisted with data analysis and statistics. Additional
collaborators on this study include Albert Mwafongo, Loreen Chiwoko, and
Deborah Kamwendo at the UNC Project in Lilongwe, Malawi, Dan Namarika and
Sam Phiri at the Kamuzu Central Hospital, and Michael Nyirenda at the
Lighthouse Trust. Irving Hoffman from UNC Center for Infectious Diseases
(cFAR) and Department of Medicine also assisted in the design and
implementation of this study.
_______________________________________
1 Hosseinipour, M.C., Tamburro, K.M., Xiong, J., Namarika, D., Nyirenda, M.,