Ł
UKASZD
OBREK1, M
ICHAŁN
OWAKOWSKI2, A
NNAS
YGUŁA3, H
ALINAB
ARYLAK3,
R
OMANM
ARIAH
ERMAN2, P
IOTRJ
ANT
HOR1Electrogastrography in Patients with Non−Erosive
Reflux Disease and with Erosive
Reflux Disorder – Preliminary Results
Elektrogastrografia u pacjentów z nieerozyjną chorobą refluksową
oraz z refluksowym zapaleniem przełyku – wstępne wyniki
1Department of Pathophysiology, Medical College, Jagiellonian University, Kraków, Poland 2Third Department of General Surgery, Medical College, Jagiellonian University, Kraków, Poland 3Gastrointestinal Consulting Office “Batorego” in Kraków, Poland
Adv Clin Exp Med 2006, 15, 5, 803–809 ISSN 1230−025X
ORIGINAL PAPERS
© Copyright by Silesian Piasts University of Medicine in Wrocław
Abstract
Background.The GERD pathogenesis is complex, also associated with gastric motility disturbances which are se− condary to the impairment of gastric myoelectrical activity. It can be measured using percutaneous electrogastro− graphy (EGG).
Objectives.Evaluating gastric myoelectrical activity in patients with both GERD forms, i.e. erosive reflux dis−ease (reflux esophagitis, or ERD) or non−erosive reflux disease (NERD), using EGG.
Material and Methods.Ten NERD patients and 10 patients with ERD were studied. The control group contained 20 healthy persons sex− and age−matched to both patient groups. All participants underwent upper gastrointestinal tract endoscopy, esophageal manometry, 24−hour pH−monitoring, and electrogastrography.
Results. All GERD patients had slightly decreased resting lower esophageal sphincter pressure (NERD: 26.1, ERD: 21.0 vs. controls: 27.7 mm Hg, p> 0.05). ERD patients had more stressed acid reflux in pH−metry than both the NERD group and controls (longest reflux episode: ERD: 45.6 vs. NERD: 30.8 and controls: 7.2 min; fraction of time with pH < 4: ERD: 21.2% vs. NERD: 12.4% and controls: 2.3%). Excessive gastric dysrhythmias in the EGG recordings were observed of neither in NERD nor ERD patients, but postprandial drops in dominant power (DP) and the power ratio (PR) were noted in both the patient groups (PR: 0.72 in NERD, 0.36 in ERD, 2.07 in con− trols; p< 0.05).
Conclusions.The EGG results confirm the existence of postprandial gastric myoelectrical activity disturbances in both GERD patients groups, which indirectly reflect the impairment of gastric motility. The presence of these di− sturbances in NERD patients indicates that they may play a role in the development of GERD and are not only a consequence of esophagitis (Adv Clin Exp Med 2006, 15, 5, 803–809).
Key words:gastroesophageal reflux disease (GERD), gastric myoelectrical activity, electrogastrography (EGG).
Streszczenie
Wprowadzenie.Choroba refluksowa przełyku (GERD – gastroesophageal reflux disease) ma złożoną patogene− zę, obejmującą również zaburzenia motoryki żołądka, wtórne do zaburzeń jego czynności mioelektrycznej. Moż− na ją ocenić za pomocą elektrogastrografii (EGG).
Cel pracy.Oszacowanie aktywności mioelektrycznej żołądka u pacjentów z obiema postaciami GERD – erozyjną (ERD) i nieerozyjną (NERD) metodą EGG.
Materiał i metody.W badaniach wzięło udział 10 pacjentów z NERD, 10 pacjentów z ERD oraz 20 zdrowych osób tworzących grupę kontrolną. U wszystkich badanych wykonano badanie endoskopowe, manometryczne, 24−godzinne monitorowanie zmian śródprzełykowego pH oraz elektrogastrograficzny zapis aktywności mioelektrycznej żołądka.
Gastroesophageal reflux disease (GERD) is the most common disorder of the upper part of the gastrointestinal tract. It may proceed with organic esophageal changes (ERD – erosive reflux esophagitis) or without any esophageal damage (NERD – non−erosive reflux disorder). Heartburn, pyrosis, and acid regurgitation are the most com− mon GERD signs, but they can also be atypical, involving cardiac−like chest pain or lung symptoms [1]. The pathogenesis of GERD is complex and is associated with disturbances in many factors, such as resting lower esophageal sphincter pressure, the diaphragm arm functioning as a “gastroesophageal junction external sphincter”, the Hiss angle, and the esophageal clearance phenomenon. All of these create an anti−reflux barrier preventing the backflow of the gastric content into the esophagus [2]. Transient lower esophageal sphincter relax− ations (TLESRs) also play an important role in GERD pathogenesis. There is also a link between TLESRs and delayed gastric motility rate, because gastric distension may trigger an excessive amount of TLESR. That is why an impaired gastric emp− tying (GE) rate contributes to the development of GERD [3]. Gastric motility may be explored in many ways using directly visible methods, such as scintigraphy. There is growing evidence that the registration of gastric myoelectrical activity with electrogastrography (EGG) also indirectly reflects gastric motility [4].
The aim of this study was to establish gastric myoelectrical activity in patients with both GERD forms using percutaneous electrogastrography (EGG). Furthermore, an attempt was made to de− termine whether possible EGG disturbances are primary in character, contributing to the develop− ment of GERD, or secondary, i.e. resulting from esophageal organic changes.
Material and Methods
Twenty patients with GERD symptoms who were being treated in a gastrointestinal practice were investigated. All subjects had typical reflux symptoms, with heartburn as the predominant clinical sign of regurgitation. Persons with co−
existent ischemic heart disease, advanced circula− tory failure, hypertension, cardiac arrhythmia, bronchial asthma, or diabetes, as well as those with contraindications to esophageal catheteriza− tion (coagulopathies, anatomical contraindications e.x. esophagostenosis) were excluded. All the studied patients were untreated or had been with− out treatment for at least three months. The aver− age age in this group was 52.3 ± 9.4 years. The control group consisted of 20 healthy persons without GERD symptoms, in generally good con− dition, and who were sex− and age−matched to the persons in the two patient groups. The healthy par− ticipants were similar in age (49.1 ±8.0 years) to the patient groups and had approximately similar BMI parameters and blood pressure. All of the patients and healthy controls were informed about the aim and method of the study and gave their written consent. The study was approved by the Local Ethics Committee of the Jagiellonian University (KBET/76/B/2004).
Endoscopic assessment of the upper part of the gastrointestinal tract, stationary esophageal mano− metry, 24−hour ambulatory pH−monitoring as the gold standard of GERD diagnosis, and one−chan− nel percutaneous electrogastrography were perfor− med in every subject.
First we carried out endoscopic examination of all the GERD patients to divide them into two groups: those with reflux esophagitis (ERD patients) and those without any esophageal mucosal changes (the NERD group). Of the ERD patients, seven had esophagitis estimated according to the Los Angeles classification as grade “A” and thirteen had grade “B” esophagitis. As a result, the first patient group (ERD) was composed of 10 participants (6 men and 4 women, mean age: 52.7 ±8.0 years) and the se− cond (NERD) group also had 10 patients (5 men and 5 women, mean age: 51.9 ±10.8 years).
In the second step, ambulatory esophageal manometry was done in each group to ascertain the LES position, which is necessary to perform pH− metric monitoring correctly. We used the station−up manometric method [5] and a 4−channel manometric catheter (inserted through the pharynx to the stom− ach and withdrawn into the esophagus) with equip− ment and software (Synectis Medical, Sweden).
trolna – 2,3%. W zapisach EGG w obu grupach pacjentów nie stwierdzono istotnych dysrytmii żołądkowych, ale zaobserwowano spadek mocy dominującej w zapisach poposiłkowych (PR = 0,72 w grupie NERD i PR = 0,36 w ERD przy PR = 2,07 w grupie kontrolnej; p < 0,05).
Wnioski.Uzyskane wyniki potwierdzają zmienioną poposiłkową czynność mioelektryczną u pacjentów z GERD. Za− burzenia takie, obserwowane u pacjentów z NERD, dowodzą, iż nie są one rezultatem rozwijających się zmian zapal− nych w przełyku, ale są jednym z czynników patogenetycznych GERD (Adv Clin Exp Med 2006, 15, 5, 803–809).
Then, 24−hour ambulatory esophageal pH−me− try was conducted in all participants. One−channel pH−metry catheters with standard buffers pH = 1, pH = 7, and a pH−digitrapper Mk III (Synectis Med− ical, Sweden) were used in this procedure. After the calibration process, the pH−metry catheter, ter− minated with an antimony pH electrode, was in− serted through the nasal cavity and pharynx into the esophagus and placed 5 cm above the upper margin of the LES, previously positioned mano− metrically (in accordance with common practice and literature references [6]). During the monito− ring, all the patients maintained their normal life activity. There were neither special dietetic nor da− ily activity limitations during the study except for the prohibition of cigarette smoking and alcohol or acidic meal consumption. Analysis was carried out using EsopHogram Synectics Medical software. The standard parameters were obtained separately for acid and alkaline reflux. The typical acid reflux parameters according to the DeMeester scale were evaluated, accepting a global time of esophageal pH < 4 amounting to at least 4.2% as pH−metric proof of excessive acid reflux.
In the last step, every subject was submitted to percutaneous electrogastrography in supine posi− tion in the morning hours. First was 30 minutes of resting while fasting recordings were collected. Then 250 ml of a standard liquid meal (Ensure Plus; Abbott; 1.5 kcal/ml) was given and the EGG registration was continued for the next 30 minutes in the postprandial period. An EGG digitrapper (Synectics Medical, Sweden) was used and stan− dard ECG Ag/AgCl electrodes, located typically on an abdominal surface according to current gui− delines [7]. The resultant recordings were subjec− ted the spectral analysis using Synectics Medical Sweden software, which produces the typical EGG parameters as results.
Initial statistical analysis was conducted using the parametric Bartlett test of variation analysis and the Fischer−Snedecor test with a significance level of p< 0.05. The changes in pre− and postprandial EGG parameters were analyzed using non−parame− tric tests of differences separately for each group.
Results
All the GERD patients had lower values of the lower esophageal sphincter resting pressure (ERD: 21.0 ± 9.9 and NERD: 26.1 ± 3.7 compared with controls: 27.7 ± 1.6 mm Hg).
pH−metry showed an increase in acid reflux ti− ming in ERD patients. They had the largest num− ber of all the noted acidic episodes. They also had the longest time of esophageal acidification, expressed as the percentage of time when the in− tra−esophageal pH in the distal esophagus was lo− wer than 4. This parameter achieved 21.2% in ERD and 12.4% in the NERD group vs. only 2.3% in the controls. Additionally, the time of the lon− gest reflux episode reached 45.6 min in ERD pa− tients and 30.8 min in NERD, whereas in the con− trol group it lasted only 7.2 min. Analyzing proba− ble alkaline episodes, it was noted that they appeared most often in NERD patients. All the pa− rameters describing this type of regurgitation achieved the largest values in this group. The ma− nometric and 24−hour pH−metric monitoring fin− dings are presented in Table 1.
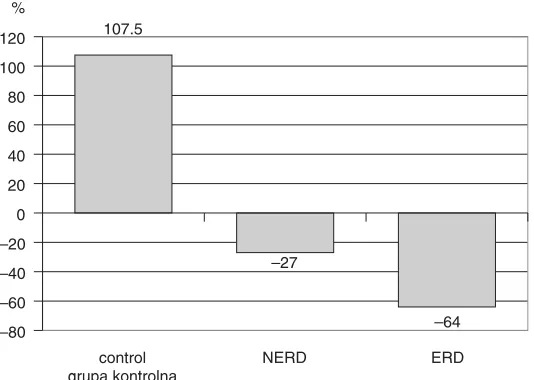
The EGG results in both GERD patient groups differed from the control group’s results, especial− ly in the ranges of the postprandial−preprandial changes in dominant power (DP), i.e. the so−called power ratio (PR). In this study, paradoxical post− prandial decreases in DP in both the patient groups were observed, especially visible in ERD patients.
Table 1. 24−hour esophageal pH−monitoring and stationary manometry results – acid reflux and alkaline reflux Tabela 1.Wyniki 24−godzinnej pH−metrii przełykowej oraz stacjonarnej manometrii – refluks kwaśny oraz alkaliczny
Parameter Reflux Control NERD ERD
(Wskaźnik) (Refluks) (Grupa
kontrolna)
The number of all reflux episodes acid 81.5 ±44.5 267.7 ±246.8 353.4 ±326.8 (Liczba wszystkich epizodów refluksowych) alkaline 61.8 ±103.2 192.6 ±175.8 139.4 ±234.6 Number of reflux episodes lasting > 5 min acid 0.3 ±0.6 3.8 ±5.4 7.5 ±8.0 (Liczba epizodów refluksowych trwających > 5 min) alkaline 8.2 ±14.6 14.7 ±11.9 6.2 ±7.8
Longest reflux episode acid 7.2 ±16.9 30.8 ±62.0 45.6 ±75.2
(Najdłuższy epizod refluksowy) min alkaline 27.7 ±42.8 69.3 ±58.9 35.9 ±48.3 Fraction with pH < 4 or pH > 8 – % acid 2.3 ±1.9 12.4 ±16.7 21.2 ±22.1 (Frakcja czasu zapisu z pH < 4 lub pH > 8 – % alkaline 12.3 ±20.9 26.0 ±20.0 12.1 ±14.3
Resting LESP – 27.7 ± 1.6 26.1 ± 3.7 21.0 ± 9.9
DP values decreased by about 27% (from 1802.3 to 1304.4 µV2) in NERD patients. A considerable
decrease in this parameter of about 64% (from 1843.9 to 661.02 µV2) was particularly observed
in ERD patients. In the control group, DP increa− sed by about 107.5%, from 1668.0 µV2in the pre−
prandial period to 3460.6 µV2in the postprandial.
Thus, the PR in the NERD patients was 0.72 and in ERD patients only 0.36, whereas in the controls it was 2.07. The total amount of gastric dysrhyth− mia in the preprandial period in the NERD group was 16.3% and decreased to 11.4% during the postprandial time, while in the ERD patients it did not change: 20.6% preprandial and 20.0% post− prandial. In the controls, the gastric dysrhythmias were 12.3% and 9.3%, respectively. ERD patients had an increase in the dominant frequency (DF) in the postprandial period (from 1.5 to 2.2). In NERD patients, DF was similar in the pre− and postpran− dial periods (1.3). The DFs in the control group were within the normogastry range in both the pre− and postprandial periods and were 2.8 and 3.1, re− spectively. The electrogastrography results are presented in the Table 2 and in Figure 1 below.
Discussion
Patients with GERD had pathological values of the pH−metric parameters. The general regularity, also confirmed in the literature [8], that there is
a link between acid reflux intensification and the development of inflammatory esophageal changes was observed here. The enormous exposure of the esophageal mucosa to the damaging acid content leads to the development of observed changes. The pH−metry recordings of the ERD patients revealed raised values both in the parameters depicting acid reflux (the total number of reflux episodes, time of the whole pH record with pH < 4 and in those illustrating the phenomenon of esophageal clearance (the number of reflux episodes lasting longer than 5 minutes, the dura− tion of the longest reflux episode).
Considering the pH−monitoring results described above, the manometric resting lower esophageal sphincter pressure (LESP) results were surprising, demonstrating only slightly reduced values in this parameter in NERD patients (26.1 ± 3.7 mm Hg) and in patients with inflammatory changes (21.0 ± 9.9 mm Hg) compared with the control group (27.7 ± 1.6 mm Hg). These differ− ences were not significant statistically. These results also differ from date published in the liter− ature, especially taking into consideration resting LESP in the ERD group. It seems these patients should be distinctly LES hypotensive. This can be difficult to explain, especially when we remember that they had the greatest acid reflux. However, as mentioned in the introduction, LES hypotony is not the only possible cause of reflux. Larger atten− tion is currently given to the mechanism of transi−
Table 2.Electrogastrography results – preprandial and postprandial period Tabela 2.Wyniki elektrogastrografii – okres przedposiłkowy oraz poposiłkowy
Parameter Period Control NERD Esophagitis
(Wskaźnik) (Okres) (Grupa kontrolna) (Zapalenie przełyku)
Bradygastria preprandial 5.3 2.2 11.3
% postprandial 3.6 4.5 9.5
statistical significance p < 0.05 p < 0.05 NS
Normogastria preprandial 87.6 83.7 79.4
% postprandial 90.7 88.7 80.0
statistical significance NS NS NS
Tachygastria preprandial 7.0 14.1 9.3
% postprandial 5.7 6.9 10.5
statistical significance NS p < 0.05 NS
Dominant frequency preprandial 2.8 1.3 1.5
(Częstotliwość postprandial 3.1 1.3 2.2
dominująca) statistical significance NS NS NS
Dominant Power preprandial 1668.0 1802.3 1843.9
(Moc dominująca) postprandial 3460.6 1304.4 661.0
µV2 statistical significance p < 0.05 p < 0.05 p < 0.05
Power Ratio (PR) – 2.07 0.72 0.36
tory LES relaxations (TLESRs) in the pathophysi− ology of GERD. Thus the lack of reduced basal LES pressure does not exclude the possibility of GERD development, even with the existence of esophageal inflammatory changes. The results of the manometric investigations in this study show that both the NERD and the ERD form can occur in the mechanism involving an enlarged number of TLESRs. This means that esophagitis is not only the consequence of LES hypotony.
There are general divergences associated with the results of incidentally performed esophageal manometry published in literature. According to Kraus et al. [9], the average resting LES pressure in all GERD patients (without distinguishing between NERD and ERD) was about 21.4 ± 1.9 mm Hg. Stal [10] reports a similar value. However, when considering LESP in patients with inflammation and in those without separately, larger differences were noticed. Particularly interesting were the observations of Mattioli et al. [11], who studied LES resting pressure in patients with different degrees of esophagitis. According to them, the ERD patients had lower LESP values than NERD patients and there was a progressive drop in LESP together with increased inflammatory state in the esophagus (from E1 to E3). Reflux episodes pre− sent in these patients occurred by the mechanism of free reflux by hypotensive LES. Reflux in the patients of the present study, however, as men− tioned above, was probably associated with the TLESR phenomenon and took place with suffi− cient frequency to conduct the inflammatory changes in the esophagus, in spite of normal, and even enlarged, LESP. However, LES hypotony may be treated as an etiologic GERD factor, but it can also be the result of inflammatory changes in the esophagus (Katz et al. [12], Singh et al. [13]).
The gastric myoelectrical activity results obta− ined in this study are also very interesting. There
are many reports that confirm the concept of distur− bed GE in GERD patients, based mostly on the scintigraphic images, as in the Estevao−Costa et al. study [14]. Herculano et al. [15] also emphasized the role of disturbances in proximal stomach emp− tying in GERD and dyspepsia development. A par− ticularly interesting study was done by Lenglinger et al. [16], who evaluated 71 GERD patients, per− forming esophageal manometry, pH−metry, and scintigraphy. They also discovered, similarly to previous studies, dysfunction in proximal stomach emptying. Freedman et al. [17] showed that GE is more dependent on acid than on alkaline or bile re− flux. Thus the concept of GE disturbances in GERD is not challenged. All of the authors mentio− ned above measured gastric motor function mostly using scintigraphy. In the present study the attempt was made to evaluate gastric motor function indi− rectly by studying gastric myoelectrical activity with electrogastrography (EGG). This is the regi− stration of the gastric slow wave (electrical control activity: ECA and basic electrical rhythm: BER) during the interdigestive time and the electrical res− ponse activity (ERA) especially in the postprandial period. In the light of present knowledge, ECA/ERA frequency and amplitude are connected with the motor activity of the stomach. In the fed state, an increase in the dominant power (DP) is observed in healthy persons compared with the va− lue of this parameter before the meal. Thus gastric motor activity could be seen in an indirect way in this study, interpreting the postprandial increase in DP as a mirror of gastric emptying [4, 7].
It should be noted that patients with either form of GERD had disturbed postprandial stomach my− oelectrical activity. There was a lack of a DP in− crease in postprandial recordings in both groups of patients, more stressed in the ERD patients. Essen− tial gastric dysrhythmias during both registration periods and in both analyzed groups were not
107.5
–27
–64 –80
–60 –40 –20 0 20 40 60 80 100 120
ERD NERD
control grupa kontrolna
% Fig. 1.Percentage of postprandial to prepran−
dial dominant power (DP) changes
Ryc. 1.Procent zmian poposiłkowych w sto− sunku do przedposiłkowych mocy
ascertained. Normogastria was present in at least three fourths of all recordings. The authors of the present study also demonstrated changes in gastric myoelectrical activity during GERD in a previous study (Banach et al. [18]). There, an elevation in postprandial dominant power was also not obse− rved. The presence of gastric dysrhythmia, mostly in the postprandial period, and abnormal DP and PR values were also noted in this patient popula− tion. Chang et al. [19] also demonstrated gastric dysrhythmias in fasting and postprandial recor− dings in GERD patients, but, contrary to previous studies, they noticed increased DP during the post− prandial time in GERD patients compared with controls. Cucchiara et al. [20] had 42 GERD pa− tients in their study, 20 of whom had severe eso− phagitis. They showed the presence of increased gastric dysrhythmias in all of them, contrary to this study. It is the opinion of the authors of the present study that part of these divergences result from the fact that GERD patients in the various studies were taken either as a single group or included only ERD patients. The present study tried to differentiate GERD patients into two basic forms, NERD and ERD, according to present guidelines. The authors consider DP and its changes to be the most impor− tant EGG parameters. It is worth stressing that these gastric myoelectrical activity disturbances were already observed in NERD patients. This allows
one to accept the hypothesis that they are not the results of the development of organic, esophageal changes, but that they can contribute to the patho− genesis of GERD by generating GE disturbances. There is strong evidence that gastric myoelectrical activity organizes the gastric motor function [4, 7], so the present findings confirm again in an indirect way the altered GE in both NERD and ERD. It is also believed that EGG, as the registration of ga− stric myoelectrical activity indirectly reflecting ga− stric motility, should be done more frequently in clinical practice.
In summary, it is concluded that: 1) There are disturbances in postprandial gastric myoelectrical activity in both GERD forms, i.e. with (ERD) and without (NERD) inflammatory esophageal chan− ges. These findings may be related to the general observation of delayed gastric emptying in GERD patients, demonstrated in scintigraphy. 2) The de− monstration of impaired gastric myoelectrical acti− vity in NERD patients may indicate that it is not the consequence of the development of esophage− al inflammatory changes in the course of GERD and that these pathological findings are present in all GERD patients. 3) A relatively small number of NERD and ERD patients was studied, which is why the obtained results may be treated as prelimi− nary. Further studies are required to confirm these findings in more numerous study populations.
References
[1] Sifrim D, Castell D, Dent J, Kahrilas PJ:Gastro−oesophageal reflux monitoring: review and consensus report on detection and definitions of acid, non−acid and gas reflux. Gut 2004, 53, 1024–1031.
[2] Mittal RK, Balaban DH: Mechanisms of disease: the esophagogastric junction. N Engl J Med 1997, 336, 924–932.
[3] Mittal RK, Holloway RH, Penagini R, Blackshaw LA, Dent J:Transient lower esophageal sphincter relaxa− tion. Gastroenterology 1995, 109, 601–610.
[4] Levanon D, Zhang M, Chen JDZ:Efficiency and efficacy of the electrogastrogram. Dig Dis Sci 1998, 43, 1023–1030.
[5] Policy and Position Statement. An American Gastroenterological Association Medical Position Statement on the Clinical Use of Esophageal Manometry. Gastroenterology 1994, 107, 1865–1884.
[6] Price J, Richter JE:The performance and interpretation of ambulatory esophageal pH monitoring in adults. In: Ambulatory Esophageal pH Monitoring: Practical Approach and Clinical Applications. Richter JE, ed., Williams & Wilkins, Baltimore 1997, 2nded., pp. 27–38.
[7] Parkman HP, Hasler WL, Barnett JL, Eaker EY:Electrogastrography: a document prepared by the gastric sec− tion of the American Motility Society Clinical GI Motility Testing Task Force. Neurogastroenterol Motil 2003, 15, 89–102.
[8] Richter JE, Bradley LA, DeMeester TR, Wu WC:Normal 24−hr ambulatory esophageal pH values. Influence of study center, pH electrode, age and gender. Dig Dis Sci 1992, 37, 849–856.
[9] Kraus BB, Wu WC, O.Castell D:Comparison of lower esophageal sphincter manometrics and gastroesophage− al reflux measured by 24−hour pH recording. Am J Gastroenterol 1990, 85, 692–696.
[10] Stal P, Lindberg G, Ost A, Iwarzon M, Seensalu R:Gastroesophageal reflux in healthy subjects. Scand J Ga− stroenterol 1999, 34, 121–128.
[11] Mattioli S, Pilotti V, Spangaro M, Grigioni WF, Zannoli R, Felice V, Conci A, Gozzetti G:Reliability of 24− hour home esophageal pH monitoring in diagnosis of gastroesophageal reflux. Dig Dis Sci 1989, 34, 71–78.
[12] Katz PO, Knuff TE, Benjamin SB, Castell DO:Abnormal esophageal pressures in reflux esophagitis: cause or effect? Am J Gastroenterol 1986, 81, 744–746.
[14] Estevao−Costa J, Campos M, Dias JA, Trindade E, Medina AM, Carvalho JL:Delayed gastric emptying and gastroesophageal reflux: a pathophysiologic relationship. J Pediatr Gastroenterol Nutr 2001, 32, 471–474.
[15] Herculano JR, Troncon LE, Aprile LR, Moraes ER, Secaf M, Onofre PH, Dantas RO, Oliveira RB: Dimi− nished retention of food in the proximal stomach correlates with increased acidic reflux in patients with gastroe− sophageal reflux disease and dyspeptic symptoms. Dig Dis Sci 2004, 49, 750–756.
[16] Lenglinger SG, Bergmann H, Schneider C, Hoffmann M, Wolfl G, Stacher−Janotta G:Gastric emptying: a contributory factor in gastro−oesophageal reflux activity? Gut 2000, 47, 661–666.
[17] Freedman J, Gryback P, Lindqvist M, Granstrom L, Lagergren J, Hellstrom PM, Jacobsson H, Naslund E:
Gastric emptying and duodeno−gastro−oesophageal reflux disease. Dig Liver Dis 2002, 34, 477–483.
[18] Banach T, Ciecko−Michalska I, Cibor D, Szulewski P, Bogdal J, Thor PJ:Myoelectric activity of the stomach and esophageal pH changes in reflux disease. Folia Med Cracov 2001, 42, 53–61.
[19] Chang FY, Lu CL, Chen CY, Luo JC, Jiun KL, Lee SD, Wu HC:Stomach myoelectrical response of patients with gastroesophageal reflux disease receiving omeprazole treatment. Gastroenterol Hepatol 2003, 18, 1399–1406.
[20] Cucchiara S, Salvia G, Borrelli O, Ciccimarra E, Az−Zeqeh N, Rapagiolo S, Minella R, Campanozzi A, Riezzo G: Gastric electrical dysrhythmias and delayed gastric emptying in gastroesophageal reflux disease. Am J Gastroenterol 1997, 92, 1103–1108.
Address for correspondence:
Łukasz DobrekKatedra Patofizjologii Collegium Medicum UJ ul. Czysta 18
31−121 Kraków Poland
e−mail: [email protected]
Conflict of interest: None declared
Received: 4.01.2006 Revised: 10.05.2006 Accepted: 21.09.2006
Praca wpłynęła do Redakcji: 4.01.2006 r. Po recenzji: 10.05.2006 r.